
Abstract
This research uses focus group methodology to examine how a specific subset of family childcare providers—those participating in a voluntary quality rating and improvement system and serving a high percentage of children receiving childcare subsidy—define quality. The study builds on the limited existing research about family childcare quality, especially research focused on understanding quality from the perspective of the childcare provider. A total of 28 family childcare providers participated in three focus groups where they were asked to define quality and to describe high- and low-quality programs. Qualitative analysis revealed four themes: relationships, supporting children’s learning, the physical and temporal environment, and personal professionalism. These results can inform how quality improvement initiatives and professional development systems support and engage family childcare providers.
The importance of high-quality early educational experiences to children’s later development is well established (Campbell et al., 2012; Schweinhart et al., 2005). Because of this, there has been increased investment in improving access to high-quality early care and education (ECE) at the state and national levels in the United States. However, despite this work, there remains a lack of consensus around how to define and measure quality in ECE. This is especially true in home-based childcare settings, where national data suggests that approximately 3.7 million providers serve 7 million children (National Survey of Early Care and Education Project Team, 2015). Home-based childcare in the USA includes any non-custodial childcare that is provided in a residential setting. This is a prevalent form of childcare in the USA—especially for infants and toddlers and for children from low-income families—and in other countries.
One subset of home-based childcare is family childcare (FCC). In the USA, FCC is defined as any non-parental childcare that is provided in a residential setting and is licensed or regulated by the state (Morrissey and Banghart, 2007). Providers in FCC typically receive pay and serve at least one child to whom they are not related (National Survey of Early Care and Education Project Team, 2015). As many as 25% of children from birth to five in the USA spend time in FCC (Morrissey and Banghart, 2007), with children from at-risk families more likely to attend FCC (Laughlin, 2013). However, less is known about the quality of FCC settings and characteristics of high-quality FCC providers compared to the research available on center-based childcare. Gaining a clearer definition of quality in FCC settings is important in supporting quality improvement and ensuring that children have high-quality early experiences that prepare them for later success.
Although this article has a focus on FCC providers in the USA, FCC is a popular form of childcare in other countries as well, including the United Kingdom, Canada, France, Italy, Denmark, the Netherlands, Iceland, and Japan. In these settings, FCC is also known as childminding or home daycare. Families’ use of FCC internationally is expected to continue to increase, as families use FCC to allow more parents to participate in the workforce and to supplement other childcare arrangements (Friendly et al., 2013; Organisation for Economic Co-operation and Development, 2012).
Quality Rating and Improvement Systems (QRIS) have emerged as the primary strategy for states and local communities in the USA to use to operationalize, measure, and improve the quality of ECE settings, including FCC. Unlike the K–12 education system, the ECE system in the USA historically has been largely unregulated and lacking cohesion. QRIS are one strategy to identify and promote higher quality within the complex ECE landscape. Although FCC providers are often able to participate in a QRIS, they tend to join at a much lower rate than center-based programs when QRIS are voluntary (QRIS Compendium, n.d.). Considering how QRIS are defining and measuring quality and ensuring these definitions are aligned with FCC providers’ own definitions of quality may support increased FCC provider participation in these systems. Even though QRIS are largely unique to the USA, findings from research related to QRIS can inform ECE research and the implementation of quality improvement supports beyond a US context. For example, research on QRIS in the USA has informed the evidence base about observational measures of quality, coaching and professional development, and financial incentives. This article focuses specifically on how FCC providers define quality; although the participants are in the USA and participate in a QRIS, the findings related to quality definitions are relevant outside of this context as well.
Defining quality
One common way to conceptualize quality is to separate structural quality and process quality. Process quality includes the aspects of the childcare setting that children directly experience (Cryer, 1999; Kreader et al., 2005), including the child’s interactions with adults, peers, and materials, and their cognitive stimulation. Structural quality includes the factors that create the framework which allows these processes to occur (Cryer, 1999). Some examples of structural quality include a teacher’s level of education, the adult-to-child ratio of the classroom, and group size (Burchinal et al., 2002). Quality improvement initiatives and research have focused on structural quality and process quality both separately and combined (Dowsett et al., 2008). However, measurements of these specific components of quality often have weak associations with child outcomes (Burchinal, 2018). This suggests that more work is needed to determine the most effective way to define and measure ECE quality.
Although not specific to ECE settings, Li and Julian (2012) identified developmental relationships as the foundational active ingredient by which to measure the quality of interventions for children and youth. However, relationships are among the most challenging aspects of quality to measure, and therefore are often left out or measured inadequately in systems like the QRIS. This may be especially problematic in FCC settings, where relationships are identified as one of the primary components of quality (Blasberg et al., 2019).
Moss et al. (2000), along with others, argue that quality in ECE is never an objective or neutral concept. Instead, it is socially constructed based on local and cultural values. However, this view of quality stands in contrast to the growing push to objectively measure quality using standardized tools. They argue for other approaches to evaluating pedagogical work that do not include the measurement of quality. Within the current framework of the QRIS, a movement away from measuring quality seems unlikely.
An additional framework for understanding quality was identified by Lilian Katz. She posited that stakeholders have different perspectives on quality, which she identified as: (1) top-down; (2) bottom-up; (3) outside-inside; (4) outside; and (5) inside (Katz, 1994). In the top-down approach, those who are not directly involved in or impacted by ECE quality, such as researchers and policymakers, define quality. These definitions are then applied to those directly involved in ECE settings. A top-down approach is the most common way in which researchers and policymakers define quality, which has implications for those who teach young children. It is evident in the measures that are often widely used to assess teachers and classrooms, including the Environment Rating Scales and Classroom Assessment Scoring System, and in most research conducted on ECE quality (Ceglowski and Bacigalupa, 2002; Melhuish, 2001).
Alternatively, the bottom-up approach considers how quality is experienced by children (Ceglowski and Bacigalupa, 2007; Einarsdottir, 2005; Kragh-Müller and Isbel, 2010; Wiltz and Klein, 2001). The outside-inside perspective focuses on how quality is perceived by families (Scopelliti and Musatti, 2013; Yamamoto and Li, 2012), and the outside approach examines how quality is conceptualized by the larger society. The final perspective is the inside perspective, where the definition of quality comes from the teachers and caregivers who are working directly with young children (Brownlee et al., 2009; Ceglowski, 2004). Although it has been 25 years since Katz voiced the need for more varied perspectives on ECE quality, research has been slow in seeking out these different perspectives.
Grounded in the inside perspective, several studies have been conducted to examine how practitioners define quality in ECE settings (Barros and Leal, 2015; Ceglowski, 2004; Harrist et al., 2007). Previous research that included teacher or FCC provider perspectives of quality has identified a number of common components of quality, including effective and ongoing provider–parent communication (Ceglowski, 2004; Brownlee et al., 2009; Doherty, 2015; Harrist et al., 2007); a safe and homelike caregiving environment (Ceglowski, 2004; Doherty 2015); enriching play and learning opportunities (Brownlee et al., 2009; Ceglowski, 2004; Doherty, 2015); and provider education and training (Brownlee et al., 2009; Ceglowski, 2004; Harrist et al., 2007). However, some of these studies excluded FCC or included only a small number of FCC providers. More research that includes FCC provider perspectives is needed to more fully understand how they define quality. The current research further explores this inside perspective with FCC providers.
Quality in FCC
There is a growing body of research about measuring and improving quality in FCC settings (Layzer and Goodson, 2006). However, little research has focused specifically on how to define quality in FCC and how quality definitions in this context may differ from those of center-based ECE or programs like Head Start or public pre-kindergarten. Research suggests that the quality of FCC in the USA and internationally varies widely. Large national studies have found that FCC is typically of lower global quality than center-based care when using observational quality measures, most of which were originally designed to be used in center-based settings (Bassok et al., 2016; Coley et al., 2001; Elicker et al., 2005; NICHD, 2004; Whitebook et al., 2004). For example, Kontos et al. (1995) found in their landmark study of FCC that only 10% of FCC providers met thresholds for high-quality care when using one widely used measure of observational quality that prioritizes the structural quality and availability of equipment and materials.
There are several characteristics of FCC that distinguish it from other ECE settings and may be relevant to how quality is defined and measured. For example, FCC providers care for children in their homes. They typically care for children of multiple ages together, often from infants to school age. They are more likely to care for children with whom they have prior personal relationships (Morrissey and Banghart, 2007), and the nature of their relationships with families can be unique (Bromer and Henly, 2009). However, these characteristics are often not included or highlighted in commonly used approaches to defining and measuring quality.
The most frequently used measure of global quality for licensed FCC is the Family Child Care Environment Rating Scale–Revised (FCCERS–R; Harms et al., 2007). The FCCERS–R utilizes a somewhat narrow definition of quality that some have argued may be more appropriate for center-based care (Porter and Kearns, 2005), and therefore may illuminate the less positive aspects of FCC without highlighting the positives (Porter et al., 2010). For example, the philosophical approach of the FCCERS–R is that, in a high-quality setting, children have access to a wide variety of materials for most of the day. Some of these materials need to be organized by type into something similar to learning centers. This may disadvantage FCC providers with more limited materials or childcare space, or those who use more of an adult-controlled approach in selecting which materials children will be able to use, but who may be demonstrating high-quality care in other ways.
Additional quality measures have been developed specifically for FCC or the larger home-based childcare population. Examples include the Quality of Early Childhood Caregiving: Caregiver Rating Scale (Layzer and Goodson, 2006) and the Child Care Assessment Tool for Relatives (Porter et al., 2006). These measures incorporate aspects of home-based childcare that are different from center-based ECE programs, and specifically place a greater emphasis on one-on-one interactions and relationships with children than traditional ECE quality measures. There are also measures that focus on specific domains of quality rather than measuring global quality. For example, the Family Provider/Teacher Relationship Quality measures were developed to measure the quality of the relationships that exist between families and childcare providers (Kim et al., 2014), which is an aspect of quality that is often a strength of FCC (Bromer and Henly, 2009; Coley et al., 2001). However, few QRIS incorporate measures that are specific to home-based childcare or FCC into their systems (QRIS Compendium, n.d.).
In addition to the top-down approach to defining and measuring quality, some studies have utilized one or more of the other approaches to understand FCC quality. One study by Doherty (2015) specifically took an inside approach and explored FCC providers’ definitions of quality. One of the themes uncovered was that providers thought it was pivotal to have affectionate and supportive relationships with each child in their care. However, this study took place in Canada, and the participants were not engaged in a QRIS. Additionally, the participants in this study were primarily Caucasian with high household incomes. Harrist et al. (2007) held focus groups with those vested in FCC using both the inside and outside perspectives. They found that both the parents and the FCC providers in this research valued caregivers who were nurturing.
Subsidy receipt and FCC quality
According to the US Child Care Development Fund’s estimates for 2015, approximately 17% of children receiving subsidy—the financial support offered to low-income families to help them pay for childcare—attend FCC (Child Care Bureau, 2017). Providers have reported that childcare subsidies make it possible for them to care for children (Bromer, 2005). Research suggests that subsidy receipt is related to quality. Raikes et al. (2005) found a negative relationship between the percentage of children receiving subsidy in FCC and quality. This corresponds with the general finding that, across types of childcare settings, low-income children are more likely to be in care that is of a lower quality (Coley et al., 2001). However, Krafft et al. (2017) found that when low-income families have access to subsidy, they select higher-quality FCC. Therefore, FCC providers who participate in the childcare subsidy program may play an important role in helping low-income families access high-quality childcare.
QRIS
In the USA, QRIS have become the primary way through which states operationalize the quality of ECE programs. Almost all states have a QRIS or are piloting one (QRIS Compendium, n.d.), and FCC providers are eligible to participate in many existing QRIS. Increasing FCC participation in QRIS has become a topic for national discussion and research. Hallam et al. (2017) asked FCC providers why they chose to participate or not participate in a statewide QRIS. They found that providers primarily joined because of the financial incentives or because they wanted to increase their professionalism, but perceived that unreasonable and overwhelming requirements were a barrier to participation. Learning more about FCC providers’ perspectives on quality and QRIS can make an important contribution to QRIS efforts (Tonyan et al., 2017). QRIS often offer a range of supports that have the potential to help FCC providers improve quality, such as coaching or technical assistance and access to workshops.
Often QRIS standards for FCC providers are adapted from the standards for center-based programs, and therefore they may not adequately account for the unique aspects of FCC. Additionally, the most widely used quality measures in QRIS were designed for center-based programs and modified to apply to FCC. Therefore, these measures may not capture the aspects of quality that are unique to FCC, such as location in a home environment and the enrollment of multi-age children.
Little research has considered the perspectives of FCC providers about quality in the USA or internationally. Additionally, there are few previous studies that focus specifically on those providers who care for low-income children or on high-quality providers. Gaining a better understanding of how FCC providers themselves conceptualize quality may help ECE systems—including not only QRIS but also other quality improvement supports available to the ECE workforce—to tailor their supports and regulations to better address the needs and strengths of this segment of the workforce. By specifically focusing on providers who serve low-income children and families and who have opted to participate in a voluntary QRIS, this study provides insight into a population that may be of particular interest to researchers and policymakers.
The purpose of this study is to examine the perspectives of an under-represented population of US FCC providers, and explore how they conceptualize quality and quality improvement. This study seeks to answer the following question: How do FCC providers who serve low-income children and participate in a QRIS define quality?
Methods
Participants
The participants in this study were FCC providers who were participating in a voluntary statewide QRIS in one mid-Atlantic state in the USA. The QRIS has five levels, and an observational assessment of quality is required to reach Star Level 3 and higher using the FCCERS–R. The FCC providers could select to participate in professional development and technical assistance related to the FCCERS–R, but this was not required. All of the QRIS participants had access to ongoing technical assistance. Additionally, they received financial incentives when they achieved higher star levels. These were tied to their level and the number of children receiving childcare subsidy who they served.
The participants were all rated at a Star Level 3 or higher, or were in the process of verifying at a Star Level 3 or higher within the QRIS. All of the participants had completed an FCCERS–R assessment and earned at least the necessary threshold score of 3.0 required to reach a Star Level 3. The sample was further restricted to those providers with at least 40% of their enrollment receiving childcare subsidy. All English-speaking providers in the state who met these criteria for inclusion were invited to participate. Because of these sampling characteristics, the participants were not representative of the larger population of FCC providers in the state, even among those participating in the QRIS; the participants were more likely to be rated at a high star level and to serve a high proportion of children on subsidy. Of the 65 eligible providers, 28 attended three focus groups. The demographic information about the participants and their childcare programs is displayed in Table 1.
Demographic data for the participants.
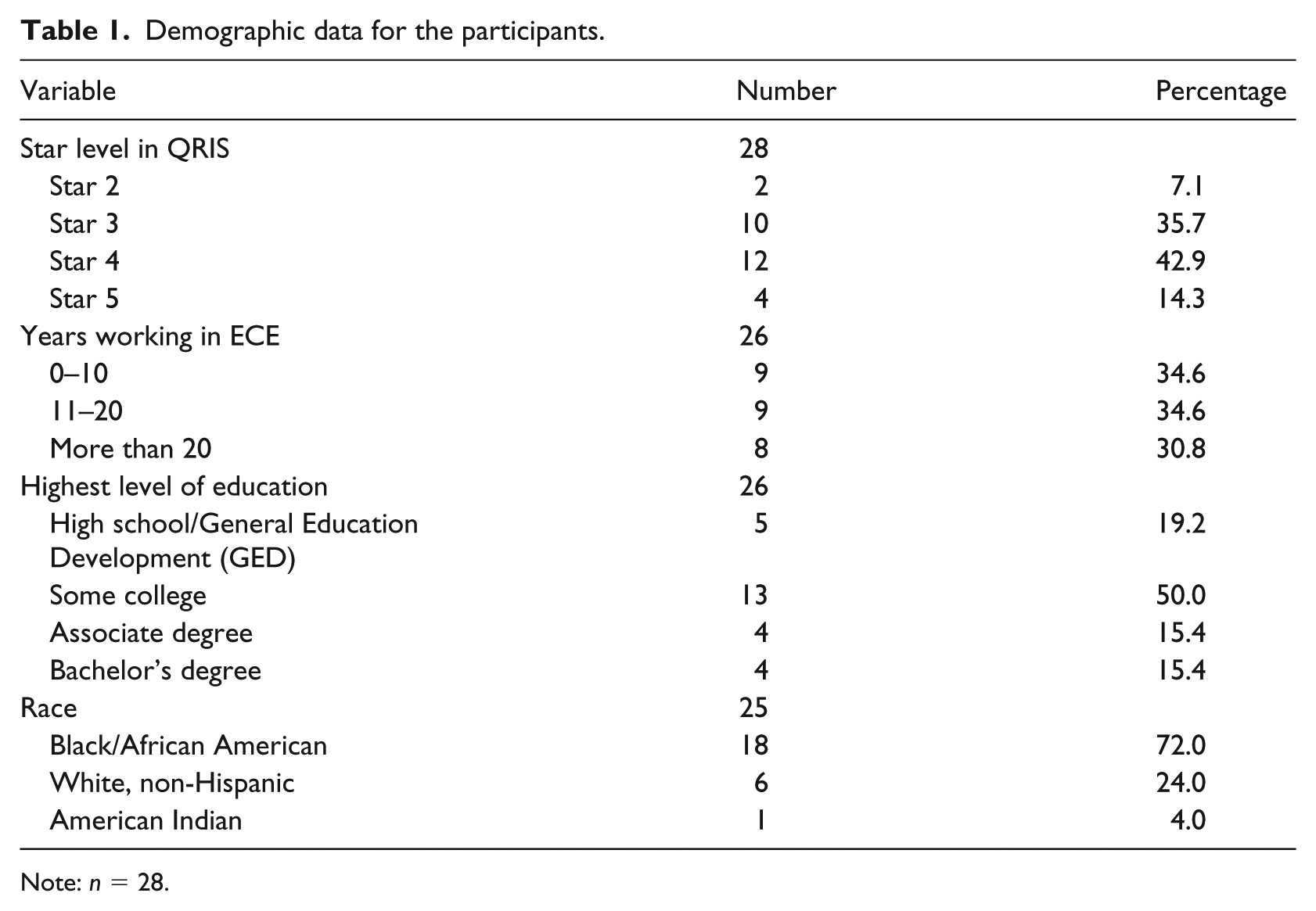
Note: n = 28.
Procedures
Three focus groups were held across the state. Focus group methodology was selected because it allows researchers to gain insight into complex issues and participants to discuss beliefs without feeling targeted (Keim et al., 1999). The structure and moderation followed the guidelines of Krueger and Casey (2015). The focus groups were facilitated by faculty and graduate students with expertise in ECE and experience working with FCC providers. The groups lasted an average of 57 minutes. At the start of the focus group sessions, the providers completed a demographic form and signed a consent form. The participants received a gift card as an incentive for participating.
Measures
Focus group protocol
A semi-structured focus group protocol was developed with eight questions and accompanying prompts designed to capture the providers’ understanding of quality. The providers were asked to define quality; describe what high-quality and low-quality FCC programs look and sound like; and describe the typical daily experiences of a child attending a high-quality FCC program. They were also asked what supports have helped them provide high-quality care in their program.
Demographic form
The participants completed a demographic form with information about themselves, including their age, years of experience, and level of education, and their program characteristics, including QRIS rating, enrollment, and location.
Analysis
The focus groups were audio-recorded and transcribed verbatim. The three authors read all of the transcripts and hand-coded the transcripts independently to gain familiarity with the content and begin identifying and organizing key ideas (Creswell, 2013). They then met to discuss and compare the themes. The preliminary conclusions were presented at a national conference, and the authors spoke one-on-one with others who research and support FCC providers to gather their feedback on the initial interpretations.
Following this initial analysis, the transcripts were imported into NVivo 11 software, and a second round of coding was completed by the first author and a graduate student. The data analysis was guided by principles from grounded theory (Glaser and Strauss, 1967). The coders first independently examined the transcripts using an inductive method of open coding (Strauss and Corbin, 1990), specifically focusing on the data related to how the participants defined quality. The three procedural steps outlined by Gibbs (2007) were followed to ensure that the data was coded reliably. These include double-checking all coded transcripts in order to identify any mistakes in codes; frequently comparing coded data with the original definitions for codes to avoid drift; and cross-checking coding to ensure agreement. The coders followed an iterative process of identifying the initial codes separately, discussing and defining those codes together, revising the codes, and recoding the transcripts (Glaser and Strauss, 1967). They met to discuss any differences in coding and reached a consensus (Creswell, 2013). As new codes and themes were identified, they were applied to all of the transcripts (Corbin and Strauss, 2015).
In order to ensure the validity of the qualitative analysis, including the credibility and trustworthiness of the findings (Lincoln and Guba, 1985), rich thick descriptions and peer debriefing were used. In order to reduce bias from the researcher and aid transferability, direct quotes from the participants were used in the analysis (Creswell, 2013).
Results
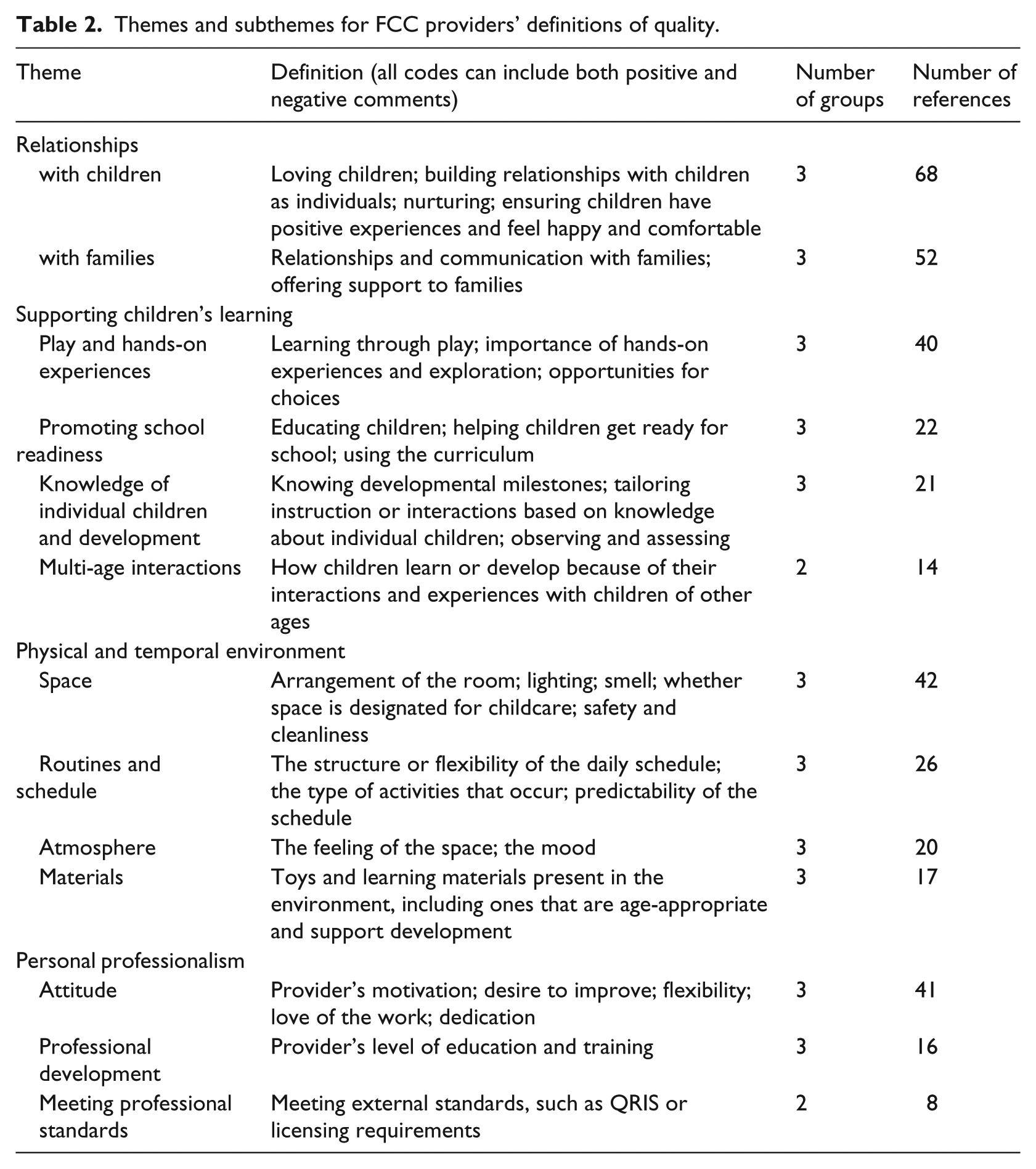
From the analysis of the focus group transcripts, several themes arose that answer the research question. The participants were readily able to define quality and describe a high-quality and low-quality FCC program. Based on their comments, the following overarching themes were identified: (1) relationships; (2) supporting children’s learning; (3) the physical and temporal environment; and (4) personal professionalism. Each theme was divided into subthemes, which are described below. Additionally, Table 2 includes definitions of each subtheme and frequency counts showing how often each subtheme was discussed.
Themes and subthemes for FCC providers’ definitions of quality.
Relationships
The most frequently discussed aspect of quality that the providers described was relationships. Through their comments, they described the importance of positive relationships with both children and families.
Relationships with children
In each focus group, the participants defined relationships with children as the central tenet of quality. The providers indicated that children are happy and feel comfortable and nurtured because of a positive relationship with the provider in high-quality programs. The primary way that the providers described building this relationship was through one-on-one interactions. The providers frequently mentioned the importance of spending individual time with each child.
When a participant discussed multiple components of quality, they often emphasized relationships as the most essential component. For example, one provider said: “I think it’s important to have the love and the understanding for the child and build the relationship, because you can have all the proper toys and everything, but if they don’t feel loved, then it’s nothing.” The participants discussed making children feel special, respecting them, speaking to them at eye level, and greeting them on arrival. One provider talked about how this aspect of quality is not always related to provider characteristics like education. Describing a provider with a degree, she said: “Yeah. I know someone with a degree. However, their interaction with the children leaves a lot to be desired. And so, okay, you’re educated. You have this degree. But your personal skills are not personable to the child.” Another provider summed up the importance that FCC providers place on positive interactions and relationships with children by saying: “Just think of each child: if this was their only day that they had, how would you make a difference?”
Relationships with families
The providers talked about how they act as an extension of the child’s family or as another member of the family, even when they were not related to any of the children in their care. For example, a participant said: “I look at myself as the extension of their families. So, I’m another component of their actual family.” They talked about how their relationships with families are often different from those of center-based providers: You’re getting to really work with that family in a deeper connection I feel than when you’re in a center. It’s definitely different. They’re also seeing you. You’re there when they are dropping off and when they’re picking up, and you’re spending years as well.
Some of the providers described how they seek to educate parents: “It’s my job to give the parents that education, you know, help them … that’s a sign of the quality of care that we’re giving.” Another provider shared: There’s a lot of parents in my program that’s single parents, and they might work two jobs or they might got four kids, and they don’t read to the children. So, it’s our job to read a book. Reading means so much—like, I visited a house last night. The parent is just going through something. We be there for the parents. I mean, I just go extra for my parents.
This provider went on to describe a parent who had to work late and was going through a personal struggle. When the parent was late picking the children up, the provider fed the children dinner and drove them home to support the parent. There were similar stories shared in all three focus groups. The providers talked about giving families resources and supplies like clothing, and doing activities with children that parents may be too busy to do.
It was notable that the providers spoke positively about families, even when families struggled to provide for their children physically and emotionally, and they seemed to believe that each family wanted what was best for their child. One provider summed this up: Most parents are looking for someone who is going to be them. Even good, bad, indifferent parents. At the end of the day, they really are looking for a substitution of themselves, or someone better than what they could be, because of whatever.
They talked about how high-quality FCC providers partner with families: “Some don’t have the education and this and that, but we’re not stepping on their toes. We’re just joining together with them to make it better for the children.”
Supporting children’s learning
The providers described how high-quality FCC programs support learning through interactions among multi-age children, providers’ knowledge of individual children and child development, play and hands-on experiences, and promoting school readiness. The providers talked about the learning experiences they provided that were hands-on and incorporated play and creative expression.
Play and hands-on experiences
The most frequently mentioned way in which the providers discussed supporting learning was through providing opportunities for play and hands-on experiences. In high-quality programs, children have ample time for free play, opportunities to make choices, and engaging and hands-on activities. They contrasted this with a low-quality program, where children would have few or no choices, or may be “just stuck in our living rooms in front of a TV or things like that, thinking that [providers are] going to meet their needs through different educational programs on TV.”
Some of the participants shared that learning through play was not always something in which they believed. For example, one provider shared: I had to learn that myself: you set it up where they can just have a choice, their free choice in what they want to do. They learn a lot better. And then you have those teachable moments that come in; even though you may have a curriculum or a plan, sometimes it’s that teachable moment right then that means the world.
Promoting school readiness
The participants agreed that a high-quality FCC program prepares children for kindergarten, both academically and socially: “When they do go to school, they understand how to be in a structured environment and how to interact and what to do, when to do it, how to do it. I think that’s important.” One way the providers promote school readiness is through having a curriculum. One participant shared how at first they resisted the QRIS standard about utilizing a curriculum: I was really butting the system on this curriculum, but that wound up being the best thing for the children. Because I just thought, you know, “Okay, everybody says I have this great imagination, and I’ve been using it for years, so I don’t need a curriculum.” But the curriculum kind of put the icing on the cake.
Several of the participants described feeling like they had provided a high-quality experience when they received positive feedback about how a child with whom they had worked was doing well in school: My two kindergarteners, they had to go take their test … They both passed, and they were so happy when they passed. They came up and gave me a kiss and thanked me. And that was an “a-ha” moment for me too, because I’m always telling them, “Those teachers are going to be so happy to get you girls. Y’all already know it.” So anyway, that was a very [good moment] for them and me.
Knowledge of individual children and child development
In high-quality programs, providers are aware of child development and individualize their instruction. One provider described quality as follows: “I would say the developmental milestones, knowing them. Then that way you can pinpoint to make sure they’re developing right.” The providers described observing and assessing children as an important aspect of quality: Observations and assessments allow you to know what areas of the child’s development you and the parent together need to work on. If you don’t observe, you don’t know where they are or what will benefit and what will not benefit … You know, to add to that, early detection. A lot of times when you find out that there is a concern, then you can make that referral prior to that child attending kindergarten. So that’s a big role for us, is preparing them for that next step in life.
One provider described identifying a hearing concern in a child who was newly enrolled through consistent observation. They were able to inform the parent, which led to the child receiving surgery to improve their hearing.
Multi-age interactions
When the participants discussed working with multi-age children, they focused on the benefits rather than the challenges. They described how younger children learn from the older children—“I think it’s great cause the little ones learn, I think, faster”—and how older children benefit as well: The older ones learn from the little ones as well. Because they learn how to be leaders. They learn how to have patience. They learn that they have to help the little ones. So, you know, it goes back and forth.
They described learning that resulted from multi-age interactions related to self-help skills like toilet training and eating at a table. They also described how younger children learn literacy through observing and participating in activities with older children.
Physical and temporal environment
When describing the environment, the providers talked about the materials present, the childcare space, the daily schedule and routines, and the atmosphere.
Materials
The providers discussed having materials that were age-appropriate and supported development across multiple domains, whether these were store-bought or home-made. As one provider described: “It’s more than having the toys … but having the right tools to provide the quality: the puzzles, the tables, the shelves.” They also talked about the importance of making these materials available to children throughout the day, rather than keeping them put away or making them teacher-controlled. The providers also discussed the importance of offering a range of materials, such as providing more than one type of block and changing the theme represented in dramatic play materials.
Space
When describing the space, the providers discussed the lighting, smell, cleanliness, safety, and room arrangement. Some of the providers described the importance of having a designated space in their home for childcare, although not all thought that this was necessary for quality. They did agree on the importance of spaces for different types of activities and displaying children’s artwork. One provider said: “During free play, that all children have the centers and things like that. That’s what [the QRIS] helps you hone in on.” Other providers agreed that they had made changes to their space through participating in the QRIS that they believed improved their quality.
In two of the three focus groups, the participants specifically discussed their initial reluctance to hang children’s artwork and display posters and photographs for the children, especially when they did not have designated space for childcare. When someone from the QRIS initially suggested that they add a child-friendly display, one provider recalled saying: “Wait a minute. Pictures on my walls? You got to be kidding me … they are my walls. My family is coming this weekend—how am I going to take them down?” However, they shared how much the children enjoyed the display and the learning they observed that resulted from seeing pictures of children from different cultures.
Routines and daily schedule
The participants discussed the importance of establishing routines and teaching those to the children. These routines seemed to help them as the only adult present. One provider said: A routine [is important] as well. Because if you get a parent to come in and the children are already engaged in whatever it is that they’re doing, they’re doing it. And you’re able to speak to the parent without them being all over the place.
They also emphasized how their routines are beneficial to children who may experience inconsistency in their home lives. The providers talked about the consistency that is possible in FCC programs, which can be different from centers: Sometimes within center programs, there’s high turnover and things like that, so you don’t know how long your child’s going to be with that particular teacher. So, in home childcare, we thrive on being the consistent provider of that child throughout many years of their lives, opposed to [centers, where] you have the infant room, toddler room, three-year-old room, and things like that.
The providers agreed that it was important to have flexibility and plenty of time for free play in the schedule, but that there should also be some structure. Many of the providers talked about how allowing child choice was a shift from their previous practice: I had to learn that myself, and you set it up where they can just have a choice, their free choice in what they want to do. They learn a lot better and then you have those teachable moments that come in.
Atmosphere
A less tangible aspect of the environment that was frequently discussed was the atmosphere. The providers talked about being able to tell the quality of an FCC space by the atmosphere when someone enters the space. The providers described a high-quality atmosphere as happy, comfortable, busy, and inclusive. They contrasted this to the atmosphere in a low-quality program: I’m going to just say atmosphere and like the mood when you walk in the room. You may not necessarily see anything out of the norm, but it’s just, you know how you can walk into a situation and know it’s just tension or stressed? You walk into the daycare room and you can always tell when the kids are bored or they’re sitting off by themselves and they really don’t want to be there.
Personal professionalism
The participants specifically discussed how, in FCC, the quality of the provider is synonymous with the quality of the program. They described three aspects of an FCC provider that lead to a high-quality program: the provider’s attitude, professional development, and adherence to professional standards.
Provider’s attitude
The importance of a positive attitude and commitment to the field and to improving practice were the most frequently discussed aspects of provider professionalism. One provider described this by saying: It ultimately starts with us, like our want to be able to do this. I think that is our want, our drive. Because it’s different; we’re just not getting up in the morning and going to punch a clock. Our quality is a little bit different because we have to want to get up and go down the steps and start the breakfast or the snack and unlock the front door and our happy face is on.
They talked about characteristics like preparedness and having a positive attitude and growth mindset. In a high-quality program, providers set aside their personal problems and their personal errands while caring for children, and have a passion for their work: You have to enjoy what you’re doing. You have to love children to begin with. Let’s start there and have a love for what you’re doing, that you want to do it and not as something as a means to an income. It has to be a love you have to want to do it. And so there are people who have that degree and fall into that line and say, “This is what I can do. This is what I been doing for years, and so this is what I’m going to continue to do.” But they just don’t have that heart for it, so that in itself will have that low quality even though they have all the credentials to qualify.
The desire to grow was highlighted as an especially important provider characteristic: No matter what level you come in and start at, to have that desire to say, “I want to do more, I want to give more, I want to be able to offer more. How do I do that? Show me how to do that. If I’m not doing it right, tell me what I’m not doing right so that I can do better.”
One way that the providers discussed showing this desire was through seeking out additional learning opportunities, including joining the QRIS.
Professional development
The providers discussed the importance of their own learning and education, specifically through participating in ongoing professional development: “A provider who is trained and continues to stay up on the latest information—to me, that’s going to provide them with what they need, as long as you stay current.” They agreed that the level of education alone was not enough to ensure that a provider was of high quality. One provider said: “Education doesn’t stop after your degree in high school or college … anything that you’re doing to continually educate yourself to the newest and best ways to care for children within this field.”
Meeting Professional Standards
Some participants described how they viewed meeting professional standards, specifically licensing regulations and QRIS standards, as a definition of quality. When asked how they would determine whether a program was high-quality, they mentioned seeing whether the program was in good standing with child care licensing. They talked about whether the program was in the QRIS and at what level as they way to determine if the program was high quality. The providers also talked about how the QRIS could be a tool to improve quality.
Discussion
This study builds on the existing research base about quality in ECE by considering the perspective of a population of interest—FCC providers who serve low-income children and are engaged in a voluntary QRIS in the USA. FCC is an important sector of ECE that is often overlooked. Gaining a better understanding of FCC providers’ perspectives of quality, especially those who actively participate in quality improvement supports and who serve at-risk children and families, has the potential to help researchers and policymakers design quality improvement initiatives that will better meet their needs and that they will view as relevant in the USA and internationally. The four themes found here align closely with those identified in previous literature, including the importance of close relationships with children and families, the caregiving environment, enriching learning opportunities, and the continued learning of the provider (Ceglowski, 2004; Doherty, 2015).
The participants in this study described a deep connection with the families of the children enrolled. They expressed a desire to support families facing challenges and to build on families’ strengths. Their comments suggest that having strong relationships with families is an important aspect of quality in FCC. Although QRIS standards may include a section about family engagement, in general, this is not widely measured in the measures and standards currently used in QRIS, including the FCCERS–R observational tool. Including measures like the recently developed Family Provider/Teacher Relationship Quality measures (Kim et al., 2014) has the potential for ensuring this aspect of quality that is important to FCC providers.
It is notable that when these FCC providers described quality, they emphasized relationships and children’s happiness and holistic well-being more often than academic school-readiness skills. Although the importance of relationships and provider–child interactions is acknowledged in larger quality research and in the implementation of systems like QRIS—for instance, through the use of the Classroom Assessment Scoring System tool—the overall narrative tends to focus on academic outcomes, which the providers in this study identified as just one component that made up the larger construct of quality.
The providers naturally described how quality in FCC includes different components than quality in center-based settings, even though they were not asked to contrast the two settings. Specifically, they talked about how the personal characteristics and quality of the FCC provider are synonymous with the quality of the FCC program, which they identified as something that makes quality in FCC different from quality in center-based care. This aligns with the findings from Doherty et al. (2006) about the importance of provider characteristics, including intentionality and use of support services, to FCC program quality.
It is clear that these participants valued their own continued professional growth and saw themselves and their knowledge and dispositions as a component of their overall program quality. Doherty (2015) found that providers specifically identified addressing the challenges that are inherent to FCC as an important component of their quality, which is similar to what was found here. Therefore, systems seeking to support FCC quality should provide a range of quality improvement initiatives that are relevant and accessible to FCC providers, many of whom work alone (Tonyan et al., 2017). The attitude of the FCC provider or classroom teacher is not typically included in definitions and measures of early childhood quality, and may be an important aspect of quality to incorporate into quality measures and quality improvement initiatives, especially in FCC settings.
There is some evidence that participating in the QRIS may have altered the FCC providers’ perceptions of quality. The providers brought up practices that they did not realize were important before participating in the QRIS, such as having learning centers and time for free play. This highlights the importance of ensuring that the way quality is measured in QRIS is capturing best practices, because some providers will alter their practices and even their beliefs based on what is promoted through the QRIS. It is encouraging to see how providers’ practices and beliefs are malleable, but it raises questions about the appropriateness of the quality measures currently used in QRIS. For example, it is worth considering whether organizing an FCC space into learning centers is necessarily a best practice for all FCC settings. Additionally, this raises the question of how providers’ understandings of quality are shaped by a QRIS and other dominant narratives about quality which tend to be center-centric.
Limitations
Because this study utilized a small sample of FCC providers in one US state and represents a specific subset of FCC providers—those serving low-income children and actively participating in a voluntary QRIS—it is not generalizable to the larger population of FCC providers nationwide or internationally. The participants represent higher QRIS levels and serve more children on subsidy than the larger population of FCC participants in the state who participate in the QRIS. Additionally, the sample is predominantly African American—more so than the larger population of FCC providers in the state and nationwide. There is little research about how providers’ race and ethnicity may influence their beliefs about quality, but it is possible that this may influence the findings here as well. This sample has distinctly different characteristics than in previous research about FCC quality, which is important to consider when interpreting the findings.
While Table 2 identifies the number of references for each code and the number of groups which discussed the codes, individual participants were not labeled in the transcripts, and therefore it is not known how many participants discussed each code. Although we refer to the participants as high quality, this is based solely on their ratings within the QRIS. The data for this study comes from a small sample—three focus groups with 28 total participants. However, this represents an important population that has rarely been the focus of previous research. The focus group data comes from one point in time, once the participants were highly rated in the QRIS, so it is unclear how QRIS participation may have influenced the providers’ opinions about quality. Collecting data at multiple time points would allow a more nuanced understanding of how FCC providers define quality before entering a QRIS and how definitions may change through QRIS participation and access to QRIS supports.
Implications for research, policy, and practice
These results provide several possible directions for future research and practice. More research is needed to understand FCC providers outside of this one state QRIS. Further study could explore how representative these quality definitions are to providers at other quality levels, in other states, and serving different demographics of children and families. Examining perspectives of quality over time could help determine to what extent FCC providers’ views of quality are related to their choice to participate in QRIS and whether being in a QRIS shapes how they view quality. Future work could use a similar approach to understand quality definitions among center-based administrators and teachers, as well as to learn how similar or different they are to FCC providers.
It may be beneficial to examine current measures as well as standards of quality to see to what degree they capture the aspects of quality that are relevant to FCC providers. The findings indicate that there are aspects of quality that are salient in the daily lives of FCC providers which are not currently being measured in most QRIS or, if they are measured, are only a small component of the overall quality rating. Finding ways to include these aspects may help increase FCC providers’ participation in QRIS, because they will view the QRIS as more relevant to their work. Additionally, increasing the emphasis on relationships with children and families, as well as the FCC provider’s own professional growth, may lead to an operationalization of quality that is more aligned with providers’ views.
This study reveals that high-quality FCC providers serving low-income children and families have a multifaceted view of quality and see their nurturing relationships with children as an essential component of their quality. Learning more about FCC providers and how they construct their definitions of quality is an important step in understanding this population and better supporting them through systems like QRIS that can assist them in providing high-quality experiences for children and families.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.