
Abstract
Background:
Clinicians are key drivers for improving health care quality and safety. However, some may lack experience in quality improvement and patient safety (QI/PS) methodologies, including root cause analysis (RCA).
Objective:
The Department of Veterans Affairs (VA) sought to develop a simulation approach to teach clinicians from the VA’s Chief Resident in Quality and Safety program about RCA. We report the use of experiential learning to teach RCA, and clinicians’ preparedness to conduct and teach RCA post-training. We provide curriculum details and materials to be adapted for widespread use.
Methods:
The course was designed to meet the learning objectives through simulation. We developed course materials, including presentations, a role-playing case, and an elaborate RCA case. Learning objectives included (1) basic structure of RCA, (2) process flow diagramming, (3) collecting information for RCA, (4) cause and effect diagramming, and (5) identifying actions and outcomes. We administered a voluntary, web-based survey in November 2016 to participants (N = 114) post-training to assess their competency with RCA.
Results:
A total of 93 individuals completed the survey of the 114 invited to participate, culminating an 82% response rate. Nearly all respondents (99%, N = 92) reported feeling at least moderately to extremely prepared to conduct and teach RCA post-training. Most respondents reported feeling very to extremely prepared to conduct and teach RCA (77%, N = 72).
Conclusions:
Experiential learning involving simulations may be effective to improve clinicians’ competency in QI/PS practices, including RCA. Further research is warranted to understand how the training affects clinicians’ capacity to participate in real RCA teams post-training, as well as applicability to other disciplines and interdisciplinary teams.
Introduction
The Institute of Medicine maintains that patient safety and unintentional patient harm is an urgent public health issue. 1 Patient harm is often a consequence of medical errors, which can involve system-based mistakes, including missed or delayed diagnoses, miscommunication between care teams, and misadministration of medication.2-5 The resulting impact on the patient ranges from no harm to death.2-5 While current initiatives and collaborative practices strive to make patient care safer, adverse events still occur. In the United States, medical errors have emerged as the third leading cause of death, accounting for more than 250 000 deaths each year. 6 This further emphasizes the need to improve patient safety. Common efforts include standardization of care processes, or recognizing and improving specific aspects of care.2-5 Moreover, hospitals dedicated to patient safety may use a more foundational approach, such as establishing and promoting a patient safety culture.7,8 This may result in system-wide changes that improve a broader range of care aspects. One framework for this approach is high-reliability organizations (HROs), which are often used in industries such as commercial aviation.7,8
High-reliability organizations adhere to 5 core principles: (1) sensitivity to operations and how they affect the organization; (2) reluctance to accept simple explanations and striving to identify the root source of problems; (3) preoccupation with failure including anticipating and correcting potential problems before they occur; (4) deference to individuals with expertise of the particular task at hand, regardless of hierarchy; and (5) commitment to resilience, and adaptive when developing new solutions to unexpected problems.7,8 As a result, major harm events in HROs are rare.7,8 When applied to the health care system, a culture of safety means identifying systematic causes contributing to patient harm, encouraging error reporting and removing individual blame, and promoting multi-level collaboration to develop solutions that may prevent similar errors from happening again.7,8 There are existing tools intended to support this process, such as root cause analysis (RCA).9,10 Clinicians in particular are key drivers for improving health care, but some may lack experience or knowledge in the use of such systems-based practices or quality improvement and patient safety (QI/PS) methodologies, including how to conduct an RCA.11-13
Although RCA has been promoted as both tangible evidence of high reliability and an important tool for improving patient safety, literature suggests that execution of RCA within the health care system is often suboptimal.13,14 One leading cause of this is a lack of knowledge and skill of personnel carrying out the RCA.15,16 There is substantial literature outlining the ideal RCA process; however, little information is available regarding a formal curriculum for RCA in the published literature.15,16 Kung et al 17 developed and implemented a case-based teaching method involving a 1-hour presentation on RCA for radiology residents. In addition, Lambton and Mahlmeister 18 paired a simulation activity with RCA training for nursing students. While these 2 studies put forward the concept of a simulation-based method to teach RCA, both describe a more superficial overview of the RCA process rather than a structured curriculum.
This work is unique in that we report on our development and execution of an interactive, simulation-based method to teach RCA in a short session. The purpose of this report is to share the curriculum and results of using RCA simulations for training, and clinicians’ preparedness to conduct and teach RCA after the training. Furthermore, this study provides educational materials and details on the curriculum to teach RCA using a low-technology simulation method.
Methods
This project was reviewed and approved by the Research and Development Committee, White River Junction, VA Medical Center. Participants were US-based clinicians from various medical specialties in the Department of Veterans Affairs (VA) Chief Resident in Quality and Safety (CRQS) training program. The CRQS program was developed for residents to gain experience teaching QI/PS concepts and leading related projects.19,20
Conceptual model
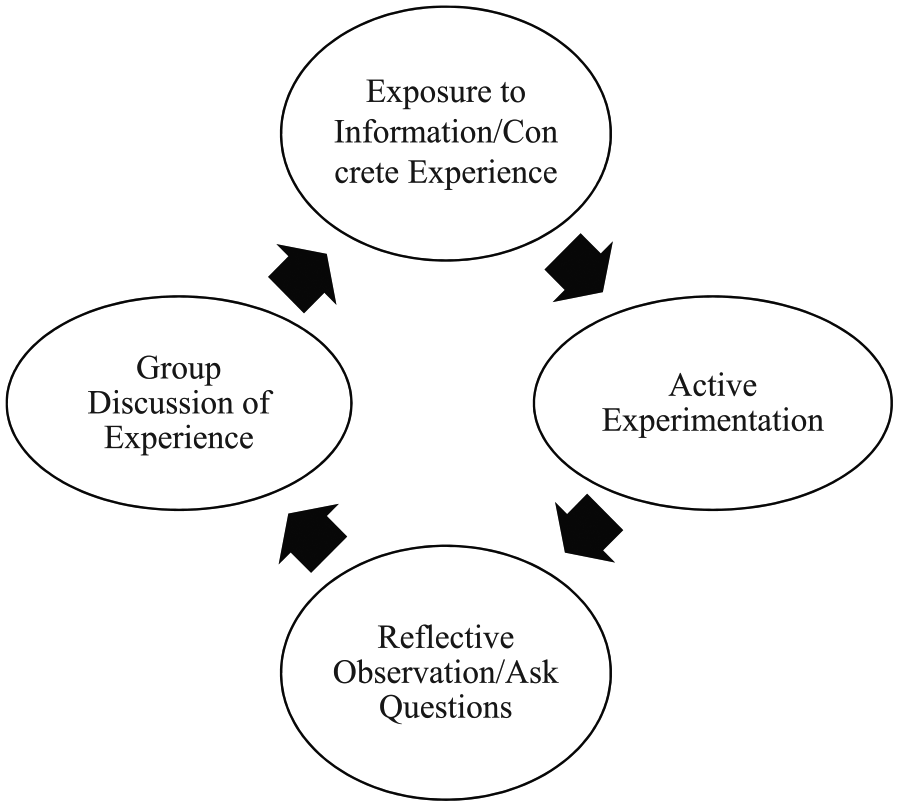
The overall course design was informed by adult learning theory (Figure 1). This conceptual model is based on the work of Kolb et al, which suggests that learning is best accomplished through concrete experience, followed by reflection and discussion. Participants are exposed to new information or have a concrete experience, actively practice what was learned with example cases, reflect on the experience and ask questions, and internalize or learn the abstract concepts through group discussion.21,22
Learning objectives
The course learning objectives were developed through consensus discussion among patient safety experts. These objectives were based on the course’s goal to develop clinicians’ ability to actively engage in patient safety activities such as RCA. The learning objectives included (1) basic structure of an RCA (eg, main components and how it is done), (2) how to do an initial understanding and final event flow diagram, (3) how to collect information for RCA (eg, interviews), (4) how to do cause and effect diagramming to obtain actionable items (eg, fishbone diagram), and (5) how to develop actions and outcomes. We developed course materials, including presentations, a role-playing case, and an elaborate RCA case. Presented information may be found in Table 1, and case summaries may be found in Table 2. The full version of these materials is available online and may be modified to meet user needs.
RCA presentation content and take-home message for each learning objective. 23
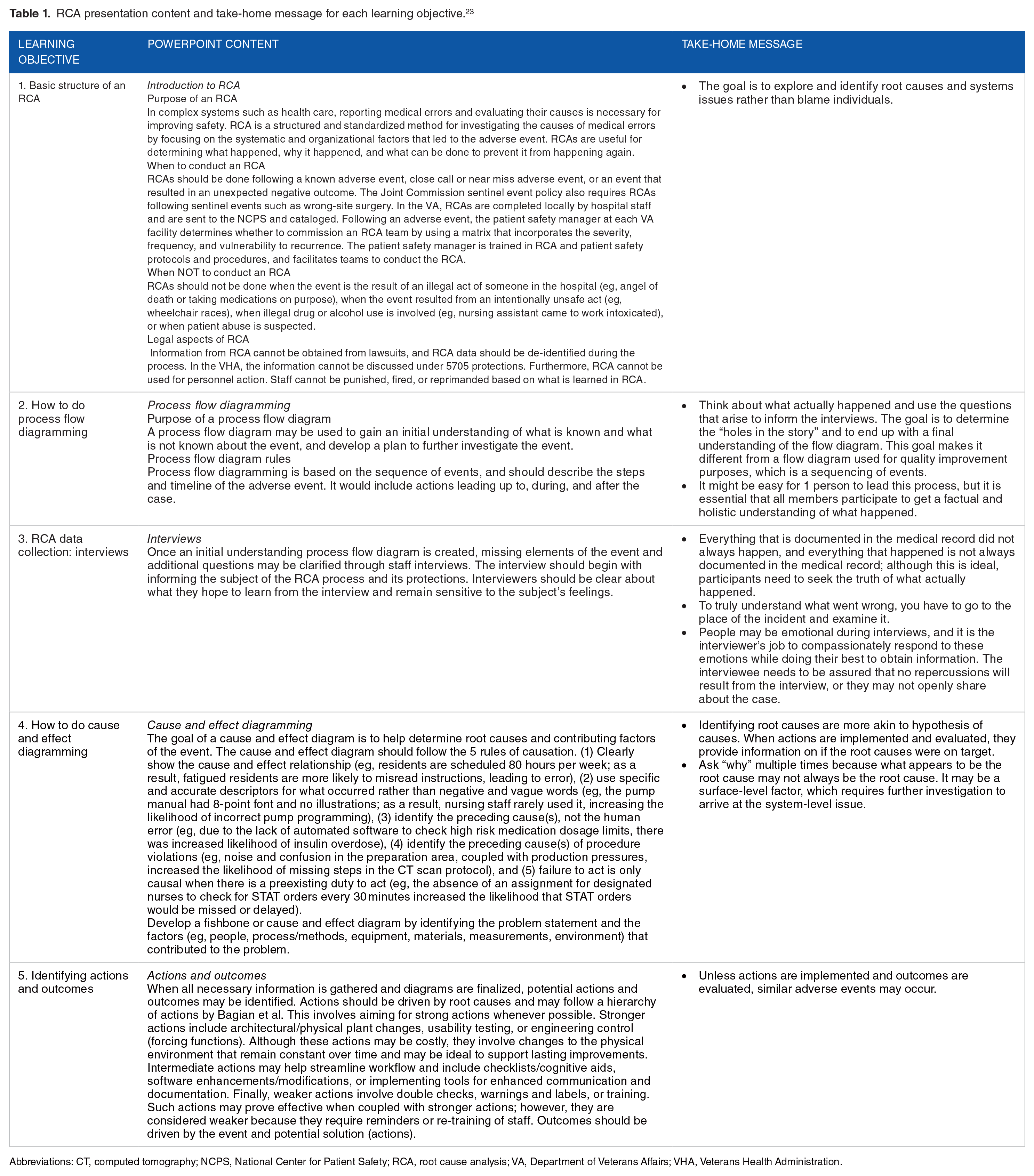
Abbreviations: CT, computed tomography; NCPS, National Center for Patient Safety; RCA, root cause analysis; VA, Department of Veterans Affairs; VHA, Veterans Health Administration.
Case summaries.

Abbreviations: ACL, anterior cruciate ligament; ER, emergency room; RCA, root cause analysis.
Course structure: 3 parts
The course is taught in a workshop format. It involves brief lectures, followed by exercises and discussions facilitated by faculty. Most exercises are done in small groups of 3 to 5 learners.
Part 1 (approximately 45 minutes)
The course begins with a presentation (10 minutes) introducing RCA concepts and how to construct a process flow diagram. Please see Supplemental Appendix A for the full presentation. Participants read and act out the role-play case (5 minutes; Supplemental Appendix B). They practice constructing an initial understanding process flow diagram with the given information, and are encouraged to reflect on the process (eg, what was the purpose, what was easy and/or hard) and ask questions of the course instructors (20 minutes). This exercise is followed by group discussion of RCA structure and process flow diagramming, and participants are instructed to make a list of questions about the case that they still want to know to complete the final process diagram (10 minutes).
Part 2 (approximately 45 minutes)
Part 2 of the course is parallel to Part 1. Several additional components of RCA are described that largely focus on the investigative aspects of RCA, including how to conduct interviews and perform site visits. Cause and effect diagrams as well as construction of actions and outcomes are also described. Participants use their unanswered questions from Part 1 to structure their interviews, and practice interviewing simulated providers. They use the information obtained from the interviews to complete their cause and effect diagram, and identify actions and outcomes (35 minutes). They are encouraged to reflect on the process (eg, did they have enough information to determine causality, did they go backward enough in the causal cascade, what was easy and/or hard about the process), as well as ask questions of the course instructors. This exercise is followed by group discussion (10 minutes). If pressed for time, faculty could proceed directly to the more elaborate RCA case to practice skills instead of conducting mock interviews on the role-play case. Please see Supplemental Appendix C for a sample agenda.
Part 3 (approximately 2 hours)
After the initial exposure and experience, participants practice again with a more complex RCA case. Participants apply the learned skills from Parts 1 and 2 to entirely new information, and they gain experience conducting an RCA from start to finish. They are first given a simulated medical record (Supplemental Appendix D) that includes an adverse event, and learners construct an initial flow diagram of the event (Supplemental Appendix E). Please see Supplemental Appendix F for the RCA medical unit diagram. Based on this initial understanding of the case, learner groups develop a list of people from the case that they would want to interview and draft a list of questions for each interview. The instructors coach the learner RCA teams on how to conduct interviews during RCA. Participants then conduct interviews with faculty who play the roles of the various staff involved in the case. The role-play simulation is directed by an interview guide for each simulated role (Supplemental Appendix G). These guides inform the individuals simulating the roles about what information they know, and how they should behave during the interview. After completing the interviews, each group completes a final understanding process map (Supplemental Appendix H), constructs a cause and effect diagram (Supplemental Appendix I), and identifies actions and outcomes. This section of the course lasts for approximately 1 hour 45 minutes.
Debriefing (15 minutes)
The course ends with a 15-minute debriefing exercise. Learners have an opportunity to discuss any lingering unclear points. The focus of the debriefing is a discussion of planned involvement with future RCAs at their institution.
Course evaluation
External evaluators administered a voluntary, non-incentivized, web-based survey to participants following RCA training in November 2016 (N = 114) using Qualtrics (Provo, UT, USA). The goal of this survey was to evaluate participants’ preparedness to conduct RCA and teach the key principles of RCA. The question types were Likert-type scale (1 = not at all, 5 = extremely), and we calculated the frequency as a basic descriptive statistics.
Results
Participants
A total of 93 individuals completed the survey of the 114 invited to participate, culminating an 82% response rate.
Preparedness to conduct and teach RCA
Nearly all respondents (99%, N = 92) reported feeling at least moderately to extremely prepared to conduct and teach RCA following training (Figure 2). The majority of respondents reported feeling very to extremely prepared to conduct and teach RCA (77%, N = 72).
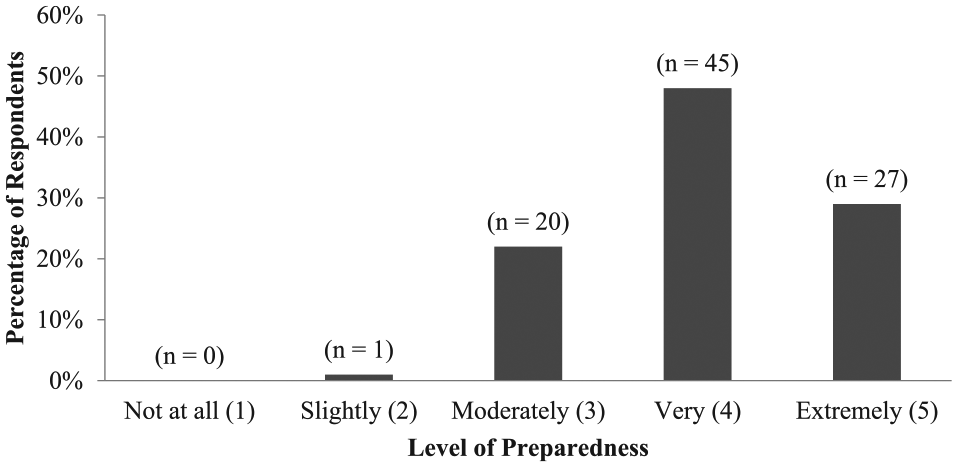
Reported preparedness to conduct and teach root cause analysis among 93 alumni of the Chief Resident in Quality and Safety program. Chief Resident in Quality and Safety alumni are US-based clinicians from various medical specialties. The data presented are Likert-type scale (1 = not at all, 5 = extremely) and were collected through a voluntary, non-incentivized, web-based survey administered in November 2016.
Participant feedback
We report a few antidotes from participants but did not receive enough open-ended responses to conduct any analyses.
“The content was very useful and practical, and designed to engage learners at all levels.” “I enjoyed the interactive nature of the class, there was never an opportunity to check out. I felt each session was very hands-on, which helped me to remember major concepts and implement the concepts we were being taught. I also thought that the manner in which the information was presented gave me ideas for ways I could teach the residents at my program.” “The hands-on, practical approach to the session in which we utilized real-world examples was useful and effective.” “Some of the material was a little basic, and we could have benefited from more in-depth knowledge and discussion of the topic.”
Discussion
To achieve the goal of safer health care aligned with high-reliability principles, heath care workers must gain an understanding of event investigation tools such as RCA. It is highly desirable to have personnel specifically trained to participate in RCA teams, and we provide an easy to implement, low-technology, simulation-based RCA curriculum to aid in this process. We tested our curriculum on clinicians of the national CRQS program and evaluated their perceived sense of competency with RCA following training. Overall, physician attendees reported better confidence in their ability to conduct and teach RCA with the training they received. The novelty of this work is that it provides the materials to simulate an RCA in a relatively brief time period (4-5 hours). Studies have demonstrated that to maximize learning, participants need to experience, reflect, and engage in active experimentation to make abstract concepts meaningful.12,21,24-27 Participants appeared to enjoy this hands-on, interactive, and practical aspect of the course. However, we suggest modifying the difficultly of the course content depending on participants’ experience with the topics to ensure they remain engaged. At the start of the course, we suggest asking participants whether they have participated in an RCA team or whether they have been asked to teach about RCA.
We acknowledge several limitations to this study. Our evaluation strategy was not mature, and we ideally would need to evaluate participants’ performance on a real RCA team following training to obtain a better performance assessment. We are unable to make any definitive conclusions on their knowledge gained because we did not have an RCA testing scenario, and we did not assess for a baseline knowledge score before participating in the course. Furthermore, clinicians’ experience with QI/PS, including RCA, may have differed prior to course involvement. This study may also be subject to sampling bias, because our participants are residents that took 1-year off to participate in the CRQS program, and were eager to learn QI/PS methodology and tools. Therefore, it is unclear how this method would work on mid-career providers or medical students, where QI/PS is not typically a core aspect of their training.
Experiential learning is not a new teaching modality, and this advanced training is commonly used for various educational purposes, including graduate medical education, clerkships, and residency.12,19,24,25,27-31 However, we believe that application of these methods including the use of simulation to teach about content specifically related to quality and patient safety is novel. Students and clinicians master what they learn in the classroom by practicing with patient actors and real-life cases. Furthermore, this method is not specific to only clinicians and may be applied to any discipline or interdisciplinary team. Watts et al 26 report that experiential learning worked well when used for industrial engineers and related industries. Increasing emphasis has been placed on educating clinicians regarding ways to deliver safer, higher quality care, and some graduate medical programs are incorporating QI/PS into their curriculum.12,24,25,29,31
The Accreditation Council for Graduate Medical Education (ACGME) developed the Clinical Learning Environment Review (CLER) program to provide guidance for an optimal clinical learning environment.11,32 The goal of CLER is to promote experiential learning and enhance clinicians’ competency in QI/PS practices.11,32 Clinical Learning Environment Review focuses on the idea that QI/PS work should be similar to clinical care training, where the expectation is that clinicians should be directly involved in the work to gain proficiency with such skills.11,32 As health care systems move toward meeting the goals of CLER, they should try to provide both basic and advanced education on tools for QI/PS, including RCA.11,32,33 We provide an example of how this may be achieved. In addition, Boussat et al 33 developed a simple model for standardized RCA reporting that presents causes and corrective actions, and may be used during time-constraining circumstances. Overall, clinicians reported enjoying the course, and our hope is that it will enhance their capacity to meaningfully participate in RCA teams by the end of the training.
Conclusions
Clinicians are leaders in patient safety and integral to the success of health care improvement initiatives. However, to meaningfully participate in such practices, they need to be trained in QI/PS methodologies and tools, including RCA. We report success with RCA simulations and experiential learning to improve their competency in QI/PS practices. Further research is needed to understand how the training affects clinicians’ capacity to participate in actual RCA teams following training, as well as applicability to other disciplines and interdisciplinary teams.
Supplemental Material
AppendixA_RCA_Powerpoint_xyz27040aa30c22c – Supplemental material for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes
Supplemental material, AppendixA_RCA_Powerpoint_xyz27040aa30c22c for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes by Maya Aboumrad, Julia Neily and Bradley V Watts in Journal of Medical Education and Curricular Development
Supplemental Material
AppendixB_DocUDrama_Sticky_Eyeball_xyz27040c674734e – Supplemental material for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes
Supplemental material, AppendixB_DocUDrama_Sticky_Eyeball_xyz27040c674734e for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes by Maya Aboumrad, Julia Neily and Bradley V Watts in Journal of Medical Education and Curricular Development
Supplemental Material
AppendixC_RCA_Session_SampleAgenda_xyz27040c148b9c5 – Supplemental material for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes
Supplemental material, AppendixC_RCA_Session_SampleAgenda_xyz27040c148b9c5 for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes by Maya Aboumrad, Julia Neily and Bradley V Watts in Journal of Medical Education and Curricular Development
Supplemental Material
AppendixD_RCA_Case_Medical_Chart_xyz27040b5af615f – Supplemental material for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes
Supplemental material, AppendixD_RCA_Case_Medical_Chart_xyz27040b5af615f for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes by Maya Aboumrad, Julia Neily and Bradley V Watts in Journal of Medical Education and Curricular Development
Supplemental Material
AppendixF_RCA_Medical_Unit_Diagram__xyz270402ac53212 – Supplemental material for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes
Supplemental material, AppendixF_RCA_Medical_Unit_Diagram__xyz270402ac53212 for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes by Maya Aboumrad, Julia Neily and Bradley V Watts in Journal of Medical Education and Curricular Development
Supplemental Material
AppendixG_RCA_Simulated_Interview_Key_xyz27040d8527b6c – Supplemental material for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes
Supplemental material, AppendixG_RCA_Simulated_Interview_Key_xyz27040d8527b6c for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes by Maya Aboumrad, Julia Neily and Bradley V Watts in Journal of Medical Education and Curricular Development
Supplemental Material
AppendixH_Final_Flow_Diagram_xyz27040b1edcd2d – Supplemental material for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes
Supplemental material, AppendixH_Final_Flow_Diagram_xyz27040b1edcd2d for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes by Maya Aboumrad, Julia Neily and Bradley V Watts in Journal of Medical Education and Curricular Development
Supplemental Material
AppendixI_Cause_and_Effect_Diagram_Answer_Key_xyz270409a808698 – Supplemental material for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes
Supplemental material, AppendixI_Cause_and_Effect_Diagram_Answer_Key_xyz270409a808698 for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes by Maya Aboumrad, Julia Neily and Bradley V Watts in Journal of Medical Education and Curricular Development
Supplemental Material
Appendix_E_Initial_Flow_Diagram_xyz27040ca1139cf – Supplemental material for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes
Supplemental material, Appendix_E_Initial_Flow_Diagram_xyz27040ca1139cf for Teaching Root Cause Analysis Using Simulation: Curriculum and Outcomes by Maya Aboumrad, Julia Neily and Bradley V Watts in Journal of Medical Education and Curricular Development
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is the result of work supported with resources and the use of facilities at the Department of Veterans Affairs National Center for Patient Safety at the Veterans Affairs Medical Centers, White River Junction, Vermont. The views expressed in this article do not necessarily represent the views of the Department of Veterans Affairs or of the US Government. This work was supported by the Department of Veterans Affairs, and as a government product, we do not hold the copyright.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Each author was involved in the conceptual design or acquisition of data, data analysis or presentation of results and drafting, revision, or final review of the manuscript.
Presentation/Publication
This paper has not been previously presented or published in any format.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.