
Abstract
Purpose
A dermatoscope, a hand-held magnifying polarized illuminating device, is a powerful tool in the clinician's tool kit for skin cancer examination (SCE), allowing for better screening and diagnostic accuracy. Yet, few physicians are trained to leverage its potential. This scoping review explores current approaches to dermoscopy education among undergraduate medical trainees. A systematic scoping review was conducted by searching 5 databases: Medline, Embase + Classic, Scopus, Web of Science, and Education Resources Information Center.
Major Findings
A total of 12 primary articles met the inclusion criteria published between 2012 and 2024 with a total of 1286 participating medical students, most of whom were clerks (nstudies = 6, 50.0%, nparticipants = 498/1286 = 38.7%). Most studies were pre- and posttest control trials (nS = 5, 41.7%, nP = 980/1286 = 76.2%) assessing SCE performance after dermoscopy teaching. Short-term retention and performance were evaluated in 9 studies (nS = 9, 75.0%, nP = 884/1286, 68.7%), in which 5 studies reported immediate statistically significant improvement in posttest scores following their respective educational intervention (P < .05) (nS = 5, 41.7%, nP = 323/1286 = 25.1%). Long-term retention was assessed in 3 studies with heterogenous findings (nS = 3, 25.0%, nP = 432/1286 = 33.6%). Many studies lack explicit reference to a structured framework for teaching dermoscopy (nS = 7, 58.3%, nP = 849/1286 = 66.0%).
Conclusions
The literature has shown successful curricular implementation and effectiveness of dermoscopy teaching at this level. Future research may focus on strategies for curricular integration, long-term retention, and connections to later stages of training and patient care.
Introduction
Dermatology education for medical students is disproportionately limited compared to the prevalence of skin conditions encountered in real practice. 1 In Canada, undergraduate medical education (UGME) dedicates an average of 25.6 h to dermatology across all 4 years of medical school, with 75% of the teaching delivered in the early preclinical years. 1 Similar limitations are reported in the United Kingdom, United States, Australia, and Spain. 2 Yet, skin conditions account for up to 25% of general practice consultations.3,4 Among these, skin cancer is a significant concern, with melanoma incidence rising rapidly, emphasizing the need for screening and early diagnosis to reduce morbidity and mortality.5,6 Dermoscopy uses polarized light for detailed skin examination and offers greater sensitivity and specificity than macroscopic skin inspection.7,8 Despite its potential to improve early skin cancer detection and recommendations for its integration into general practice,7,8 dermoscopy use remains limited due to insufficient training. 9 Surveys reveal gaps in education: 28% of graduating U.S. medical students had never observed skin cancer examination (SCE) being performed, and 26.7% lacked formal training.10,11 The extent of dermoscopy education in UGME is unknown. Additionally, less than 40% of U.S. primary care residents felt adequately prepared to diagnose skin conditions, 12 and only 35% of dermatology residents received dedicated dermoscopy training, according to a survey of over 118 U.S. dermatology program directors. 13 Expanding dermoscopy use may require upstream integration at the UGME level, yet little is known about current educational approaches for medical students.
This scoping review explores empirical studies on dermoscopy education for undergraduate medical trainees, helping map current educational interventions and providing a foundation for future curriculum planning to complement broader dermatology education. Early introduction and exposure to dermoscopy in UGME may serve as a foundation for awareness and future skill development.
Methods
This scoping review was conducted using the Joanna Briggs Institute methodology and guided by the PRISMA scoping review checklist (Supplemental Material 1, Table 1).14–16
Information sources and search strategy
A comprehensive search was conducted across Medline (OVID), Embase + Classic (OVID), Scopus, Web of Science (all indexes), and Education Resources Information Center via ProQuest. Specific search terms addressed two primary concepts: UGME and dermoscopy (Supplemental Material 2, Tables 1-6). The UGME concept encompassed terms related to medical schools and medical students, while the dermoscopy concept included relevant synonyms such as “dermatoscopy” and “epiluminescence microscopy.” Database-specific subject headings (eg, MeSH in Medline, Emtree in Embase) and exploded commands were employed where applicable to optimize the search.
The initial literature search was conducted in August 2024 and updated in October 2024 to capture recent publications. A reference sampling approach was used by manually screening the reference lists of all included full-text articles to identify additional relevant studies. The search strategy was collaboratively designed by the authors and an expert librarian from McGill University.
Eligibility criteria
Inclusion criteria comprised all primary literature on empirical studies that addressed the teaching of dermoscopy in UGME (Supplemental Material 2, Table 1). Eligible studies were published in English or French, with no date restrictions. Studies were excluded if they were: review articles or other nonprimary literature; focused on macroscopic skin assessments rather than dermoscopy; unrelated to medical school training.
Data charting and data items
Two independent reviewers (SM and ASA) assessed each study against the eligibility criteria using Covidence Software (SaaS Enterprises, US). The initial screening process focused on titles and abstracts, followed by a full-text review. Disagreements were resolved through one-on-one meetings and consensual discussions. For eligible articles, data extraction was performed by one reviewer (SM) and verified by a second reviewer (ASA). Data collected included the study title, publication year, geographical location, study design and purpose, dermatology subfield, sample size and description, dermoscopy-specific training length and frameworks, pedagogical methodologies, reported outcomes and implications for practice.
Statistical analysis
This scoping review did not include a metaanalysis due to the heterogeneity of study designs, interventions, and outcome measures across the included studies. The data was analyzed descriptively using Excel (Microsoft, US) with the Analysis ToolPak. Frequencies and proportions were calculated for categorical variables (eg, study design, country, level of training), and descriptive statistics (mean, median, standard deviation, and range) were calculated for continuous variables where appropriate (eg, training duration). The extracted data was then synthesized narratively in the results.
Results
Characteristics of studies
A total of 611 articles were identified across five databases and reference sampling (Figure 1).17,18 Following duplicate removal and screening, the majority of records were excluded on the basis of study design (nonprimary literature), focus (not specific to dermoscopy), or population (not involving undergraduate medical trainees). Ultimately, 12 studies published between 2012 and 2024 were included in this review.17–28 Collectively, these studies encompassed 1286 medical students (Supplemental Material 3, Table 1).17–28 Five studies were pre- and posttest control trials (nS = 5, 41.7%, nP = 980/1286 = 76.2%),19,21,23–25 and 5 studies were pre- and posttest cohort studies (nS = 5, 41.7%, nP = 214/1286 = 16.6%).17,20,22,26,28 Two cohort studies (nS = 2, 16.7%) had only posttest evaluations (nP = 92/1286 = 7.2%).18,27 Five studies were conducted in Europe (nS = 5, 41.7%, nP = 450/1286 = 35.0%),21,23,26–28 and 4 studies were conducted in North America, which had the largest number of participants (nS = 4, 33.3%, nP = 652/1286 = 50.7%).19,20,22,24 Two studies (nS = 2, 16.7%) were conducted in Asia (nP = 119/1286 = 9.3%),17,25 and one study was conducted in South America (nS = 1, 8.3%, nP = 65/1286 = 5.1%). 18 Eleven studies were carried out in high-income countries (nS = 11, 91.7%, nP = 1281/1286 = 99.6%),18–28 and one study was conducted in an upper-middle income country (nS = 1, 8.3%, nP = 5/1286 = 0.4%).17,29 Half of studies reported on clinical medical students (clerks) (nS = 6, 50.0%, nP = 498/1286 = 38.7%),17,18,21,25,27,28 and a quarter of studies reported on preclinical students (nS = 3, 25.0%, nP =364/1286 = 28.3%).20,22,24 One study (nS = 1, 8.3%) included both clinical and preclinical students (nP = 288/1286 = 22.4%), 19 and 2 studies (nS = 2, 16.7%) did not report the training levels of the medical students (nP = 136/1286 = 10.6%).23,26
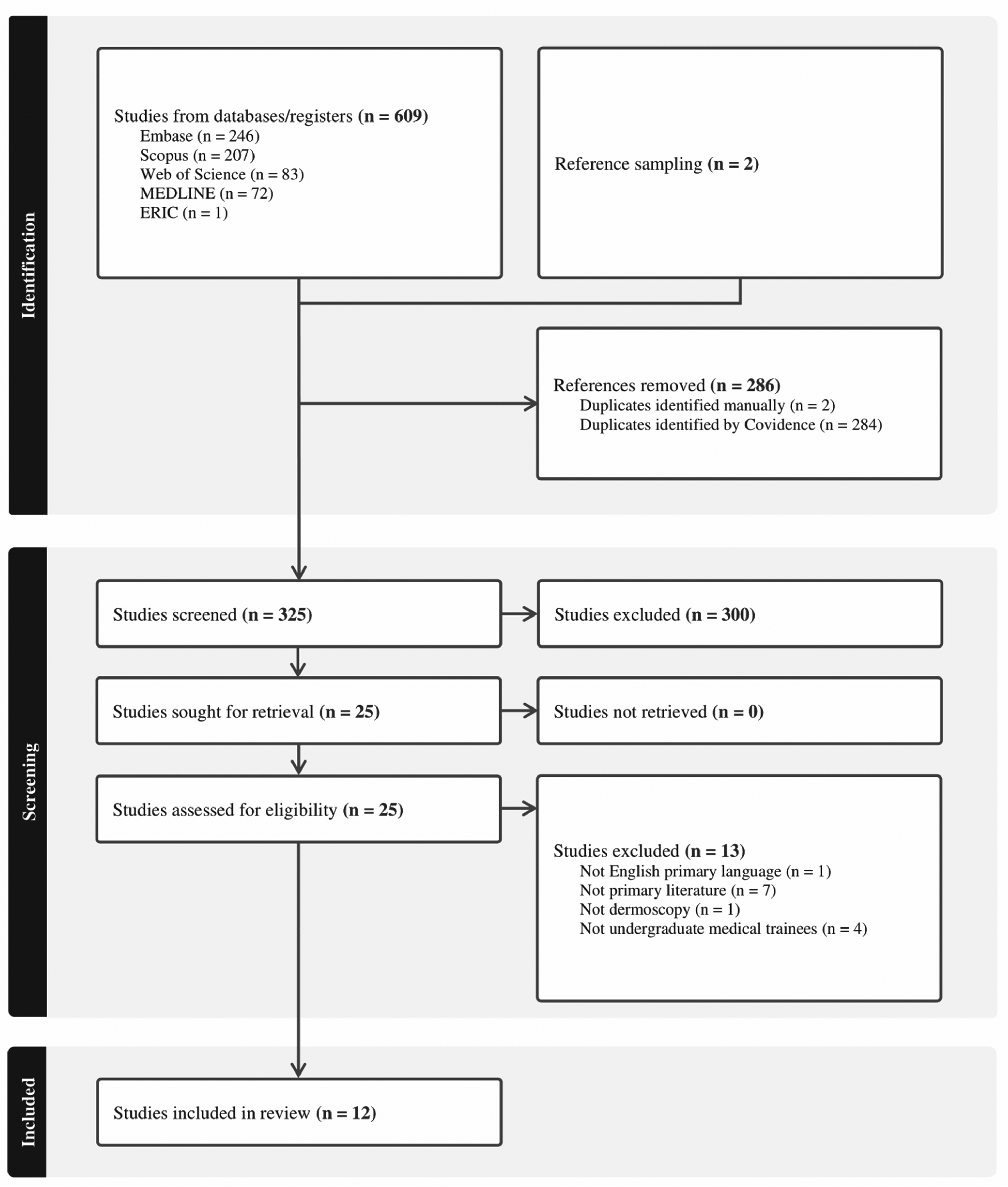
PRISMA flow diagram. 16
All 12 studies measured the diagnostic performance of medical students as evaluated on an image-based questionnaire differentiating benign versus malignant or pathologic findings (Table 1, Supplemental Material 4, Table 1).17–28 Two focused on the sensitivity and specificity of dermoscopic diagnoses postulated by medical students in pigmented lesions (nS = 2, 16.7%, nP = 92/1286 = 7.2%) (Supplemental Material 4, Table 1).18,27 Three studies provided long-term follow-up for retention metrics as it pertains to overall skin cancer detection (nS = 3, 25.0%, nP = 432/1286 = 33.6%).19,23,28 Four studies also assessed the beliefs and attitudes of medical students as they pertain to dermoscopy (nS = 4, 33.3%, nP = 833/1286 = 64.8%).19–21,24
Dermoscopy Educational Interventions Descriptors (n = 12).

Note. ABCDE, asymmetry, border, color, diameter, evolution; BCC, basal cell carcinoma; MCQ, multiple choice questions; MM, malignant melanoma; MN, melanocytic nevus; NFC, nail fold capillaroscopy; NN, neural network; NVC, nail fold capillaroscopy; SCE, skin cancer examination; SK: seborrheic keratosis; TSBE, total body skin exam.
Dermoscopy pedagogical approaches
Dermoscopy approaches focused mainly on skin cancer detection (nS = 11, 91.7%, nP = 1237/1286 = 96.2%),17–25,27,28 and only one study focused on nail fold dermoscopy (nS = 1, 8.3%, nP = 49/1286 = 3.8%) (Table 1). 26 Only 4 studies reported participants having access to hands-on dermatoscopes during the teaching interventions (nS = 4, 33.4%, nP = 652/1286 = 50.7%).19,20,22,24 All-type dermoscopy-specific training length varied from 7 min to 10 days (median: 60 min, mode: 15 min, SD: 4322 min),17–20,22–28 with one study with nonreported focused training time (nS = 1, 8.3%) (Table 1). 21
Half of the studies focused on tutorial-based teaching sessions (nS = 6, 50.0%, nP = 736/1286 = 57.2%),19,20,22,24,27,28 with a mean tutorial time of 41.2 min (SD: 33.6, Mode 15 min) (nS = 6, 50.0%, nP = 736/1286 = 57.2%).19,20,22,24,27,28 Of those, all demonstrated statistical significance (P < .05) posteducational intervention, except one which did not achieve statistical significance and one where pre- and poststatistical comparisons were not performed, respectively.24,27
A quarter of the studies investigated asynchronous, self-directed e-learning modules (nS = 3, 25.0%, nP = 206/1286 = 16.0%).17,23,25 Asynchronous, self-directed e-learning had vastly ranging modalities from MCQ-based mobile applications to slide-show-based annotated images to cellphone wallpapers (nS = 3, 25.0%, nP = 206/1286 = 16.0%),17,23,25 and did not appear to have a trend regarding statistical improvement likely due to the group and reporting heterogeneity. 17
Three studies were based on didactic lectures (nS = 3, 25.0%, nP = 206/1286 = 16.0%),18,21,26 where 2 studies report positive improvements post seminars,21,26 and one does not provide pretest comparison. 18
Dermoscopy frameworks
Seven studies did not report a specific framework for dermoscopy teaching (nS = 7, 58.3%, nP = 849/1286 = 66.0%).19–21,23,25–27 Only 5 studies reported on using dermoscopy frameworks (nS = 5, 41.2%, nP = 437/1286, 34.0%),17,18,22,24,27 namely:
Triage Amalgamated Dermoscopic Algorithm (TADA) by Rogers et al (2017) (nS = 1, 8.3%, nP = 49/1286 = 3.8%)22,30; Three-point Checklist by Soyer et al (2004) (nS = 2, 16.7%, nP = 326/1286 = 25.3%)18,24,31; Chaos and Clues framework by Kitter et al (2007) (nS = 1, 8.3%, nP = 57/1286 = 4.4%)28,32; Menzies Dermoscopic Method by Menzies et al (1995) (nS = 1, 8.3%, nP = 5/1221 = 0.4%).17,33–35
The “TADA Framework” and “Chaos and Clues” frameworks showed statistically significant improvement posttest (P < .05) (nS = 2, 16.7%, nP = 106/1221, 8.2%),22,28 while the “Three Point Checklist” did not (nS = 1, 8.3%, nP = 261/1286 = 20.3%). 24 The second study using the “Three Point Checklist” only reported posttest descriptive data. 18 Interestingly, the “Chaos and Clues” method was compared with the heuristic method (ie, simple pattern recognition), and there were no statistical differences between groups. 28 The study using the “Menzies Dermoscopic Method” did not report comparative statistics for the medical student subgroup (nS = 1, 8.3%, nP = 5/1286 = 0.4%). 17
Learning retention
The diagnostic performance, as assessed on image-based questionnaires, of medical students using dermoscopy for differentiating benign findings versus malignant or pathologic findings was analyzed with short-term posttest comparisons in nine studies (nS = 9, 75.0%, nP = 884/1286 = 68.7%) (Supplemental Material 4, Table 1).17,18,20–22,24–26,28 Of the latter, 5 studies reported immediate statistically significant improvement in posttest scores following their respective educational intervention (P < .05) (nS = 5, 41.7%, nP = 323/1286 = 25.1%).20,22,25,26,28 Of which, 2 studies focused on preclerks (nS = 2, 16.7%, nP = 103/1286 = 8.0%),20,22 and 2 focused on clerks (nS = 2, 16.7%, nP = 171/1286 = 13.3%).25,28 Three of the studies showing statistically significant improvement in posttest scores were of tutorial-based interventions (nS = 3, 25.0%, nP = 160/1286 = 12.4%).20,22,28 Two did not demonstrate statistical significance (P ≥ .05) (nS = 2, 16.7%, nP = 491/1286 = 38.2%),21,24 and two did not report statistical significance for the medical student group.17,18
Three studies assessed long-term retention via follow-up image-based posttests (nS = 3, 25.0%, nP = 432/1286 = 33.6%).19,23,28 Of these, one study focusing on preclinical medical students found retention of dermoscopy skill in differentiating benign from malignant lesions was either maintained or improved 12 months later (P < .05) (nS = 1, 8.3%, nP = 288/1286 = 22.4%). 19 Another study on medical students in their clerkship years found that the diagnostic accuracy in distinguishing benign from malignant pigmented lesions had decreased significantly 6 months later (nS = 1, 8.3%, nP = 57/1286 = 4.4%). 28 In a third study, long-term retention of dermatoscopic skills for skin cancer detection was compared based on prior histopathology-focused dermoscopy teaching and did not show a significant long-term difference (nS = 1, 8.3%, nP = 87/1286 = 6.8%). 23 In addition, one study compared dermoscopy and videodermoscopy teaching methods. It found no difference between groups in identifying dermoscopic features of benign and malignant skin lesions in posttests (nS = 1, 8.2%, nP = 54/1221 = 4.2%) 20 ; however, both groups improved their skills from baseline (P < .05). 20
Diagnostic accuracy of learners
One study assessed via an image-based questionnaire the sensitivity and specificity of medical students trained in dermoscopy of pigmented skin lesions compared to an artificial intelligence (AI) neural network (trained with the same content of basal cell carcinomas, dermatofibromas, melanomas, melanocytic naevi, seborrheic keratoses and vascular lesions) and found comparable diagnostic accuracy in identifying malignant lesions (sensitivity 86% vs 90% respectively, specificity 79% vs 71% respectively) (nS = 1, 8.3%, nP = 27/1286 = 2.1%). 27 One study noted a sensitivity and specificity for differentiating malignant lesions at 89.7% and 61.99%, respectively, (nS = 1, 8.3%, nP = 65/1286 = 5.1%) with moderate interrater agreement (κ = 0.50; CI [0.47-0.54]). 18 In one study, students performed as well as trained primary care physicians in identifying malignant skin lesions after the workshop (P = .11) (nS = 1, 8.3%, nP = 49/1286 = 3.8%). 22
Beliefs and attitudes of learners
Four studies also assessed the beliefs and attitudes of medical students as they pertain to dermoscopy (nS = 4, 33.3%, nP = 833/1286 = 64.4%).19–21,24 One study found that students’ confidence in distinguishing benign growths from skin cancer diminished over 1 year due to a lack of practice in clinical settings. 19 However, during routine physical exams, the cohort that received the dermoscopy tutorial was reported to have routinely inspected skin more than the cohort that did not (P < .05). 19 Another study found that self-confidence in identifying benign and malignant lesions increased in both groups of dermoscopy and videodermoscopy for all lesion types (except warts, melanocytic nevi, and melanoma). One study reported that students who received dermoscopy teaching had an increased perceived importance of routine skin examinations (mean scores 4.38 to 4.57, P = .03) and considered buying a dermatoscope in their future clinical practice (61%, P = .037). 21 One study did not report statistically significant differences between cohorts concerning attitudes toward the value of learning total skin examinations. 24
Thematic analysis of author recommendations and implications for practice
Key themes across studies include the recommendations for early integration of dermoscopy in UGME, the importance of accessible tools and mentorship, the value of short and scalable interventions (including e-learning), and the role of structured frameworks (Table 2).
Dermoscopy Education Intervention Recommendations and Implications for Practice (n = 12).
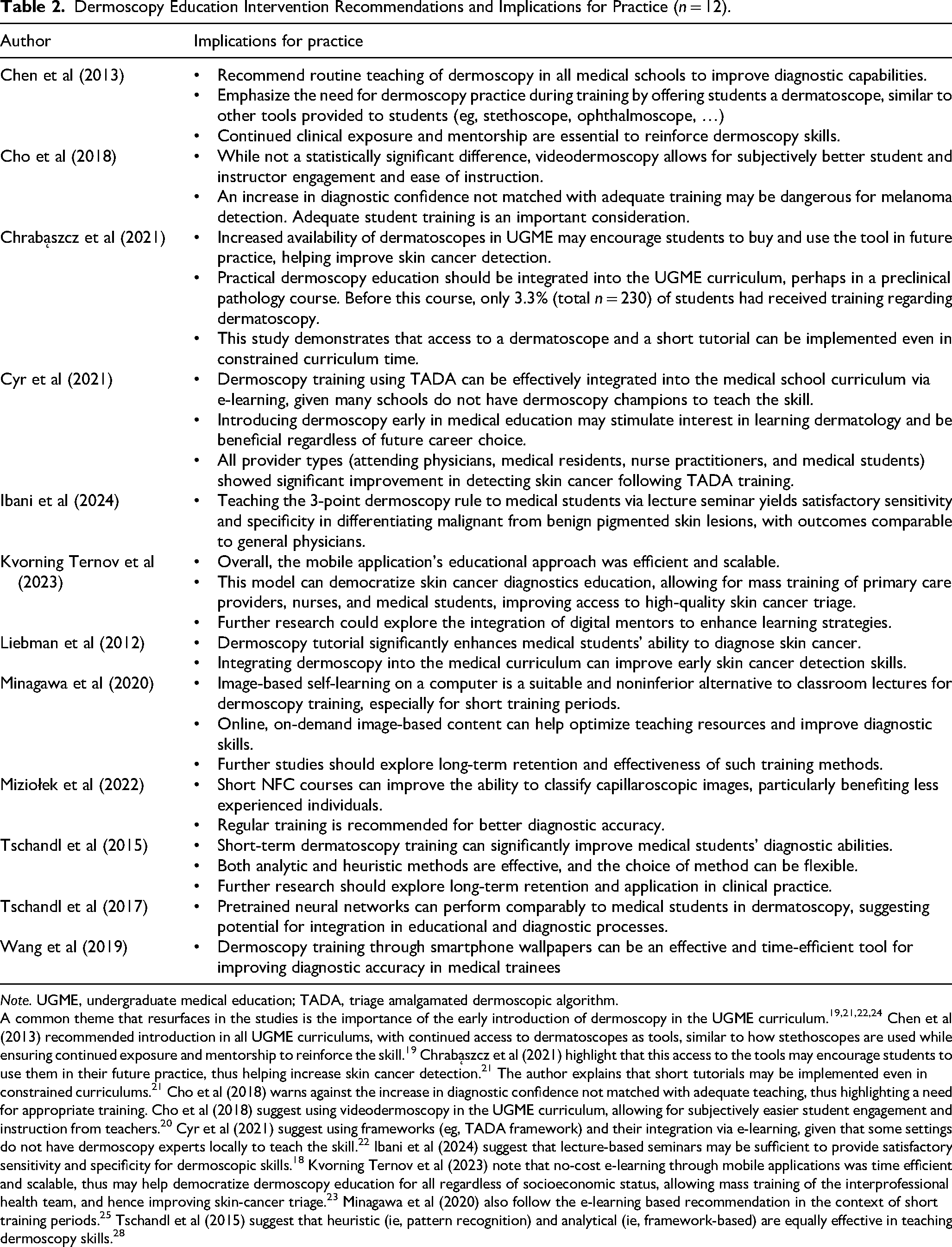
Note. UGME, undergraduate medical education; TADA, triage amalgamated dermoscopic algorithm.
A common theme that resurfaces in the studies is the importance of the early introduction of dermoscopy in the UGME curriculum.19,21,22,24 Chen et al (2013) recommended introduction in all UGME curriculums, with continued access to dermatoscopes as tools, similar to how stethoscopes are used while ensuring continued exposure and mentorship to reinforce the skill. 19 Chrabąszcz et al (2021) highlight that this access to the tools may encourage students to use them in their future practice, thus helping increase skin cancer detection. 21 The author explains that short tutorials may be implemented even in constrained curriculums. 21 Cho et al (2018) warns against the increase in diagnostic confidence not matched with adequate teaching, thus highlighting a need for appropriate training. Cho et al (2018) suggest using videodermoscopy in the UGME curriculum, allowing for subjectively easier student engagement and instruction from teachers. 20 Cyr et al (2021) suggest using frameworks (eg, TADA framework) and their integration via e-learning, given that some settings do not have dermoscopy experts locally to teach the skill. 22 Ibani et al (2024) suggest that lecture-based seminars may be sufficient to provide satisfactory sensitivity and specificity for dermoscopic skills. 18 Kvorning Ternov et al (2023) note that no-cost e-learning through mobile applications was time efficient and scalable, thus may help democratize dermoscopy education for all regardless of socioeconomic status, allowing mass training of the interprofessional health team, and hence improving skin-cancer triage. 23 Minagawa et al (2020) also follow the e-learning based recommendation in the context of short training periods. 25 Tschandl et al (2015) suggest that heuristic (ie, pattern recognition) and analytical (ie, framework-based) are equally effective in teaching dermoscopy skills. 28
Discussion
This scoping review explored dermoscopy education in UGME to guide curriculum planning and future research. The findings demonstrate that basic dermoscopy instruction can be effectively integrated into UGME, equipping students with early exposure and introductory skills in SCE.
Twelve studies involving 1286 medical students across diverse geographic locations demonstrated consistent improvements in diagnostic performance following educational interventions. Most used pre- and posttest designs, demonstrating improved diagnostic performance posttraining in all but 2 studies (P ≥ .05).21,24 Tutorial-based approaches were the most common (nS = 6, 50.0%) and effective, often requiring less than an hour.19,20,22,24,27,28 Lecture-based learning, although less popular (nS = 3, 25.0%),18,21,26 showed statistical significance in diagnostic accuracy improvements.21,26 Self-directed e-learning (nS = 3, 25.0%), though convenient and scalable, showed mixed results, likely due to heterogeneity in content and delivery.17,23,25 Long-term retention of dermoscopy skills varied, with some studies reporting sustained or improved performance up to a year postintervention, while others noted significant declines.19,23,28 This variability highlights the need for follow-up strategies to reinforce learning over time.
The International Skin Imaging Collaborative (ISC) suggest innovating from the regular container model educational theory for dermoscopy teaching (ie, didactic lectures).36,37 ISC recommends using whole-task learning approaches (ie, series of clinical scenarios based on real-life cases), delivering instructions in short segments (microlearning to alleviate cognitive load), using perceptual learning (ie, a library of training cases with feedback on performance) or adaptive learning methods (ie, algorithm retired specific learning goals based on mastery).36,37 In this study, didactic lectures were the least used methodology,18,21,26 and instead, half of the teaching sessions were tutorial-based, with a mean tutorial time of 41.2 min.19,20,22,24,27,28 Asynchronous e-learning, particularly mobile apps with annotated images, has emerged as a scalable and accessible option, though its effectiveness depends on content quality and learner engagement, as demonstrated in this review.17,23,25 Kvorning Ternov et al (2023) showcased a mobile application based on perceptual learning theory with hundreds of annotated dermoscopy images in which the learning curve decelerated at approximately 100 learning cases for both pigmented and nonpigmented lesions. 23 Wang et al (2019) used microlearning theory by having annotated dermoscopy smartphone wallpapers which change every minute for 10 days. 17 The ISC recommendations may be applied in various formats; however, e-learning may be more accommodating for educators and students.
The heuristic method, called the “blink” approach, is learning dermoscopy using pattern recognition until one develops a “déjà-vu” effect. 38 In contrast, the analytical method, called pattern analysis, relies on a set of features to reach a diagnostic conclusion. 38 Although both methods are widely accepted, the analytical method has been preferred in instances of little clinical experience.38–40 Over a third of the studies based their educational intervention on previously studied dermoscopy frameworks.17,18,22,24,27 The “TADA Framework” and “Chaos and Clues” frameworks showed statistically significant improvement posttest in medical students,22,28 while the “Three Point Checklist” did not. 24 This analytical approach may be easier for educators to implement when there is a paucity of dermoscopy experts available to teach a large body of learners. Importantly, these interventions should be understood as providing early exposure and familiarity rather than producing independent dermoscopy practitioners. Structured frameworks may serve as beginner-appropriate tools that can be revisited during residency or continuing education for mastery.
Contrary to concerns that dermoscopy is too advanced for UGME, after short training sessions, medical students achieved diagnostic performance comparable to that of trained physicians or AI systems.18,22,31,41 Dermoscopy education complements the growing integration of AI in dermatology by providing a critical safeguard against diagnostic errors and biases. While cost and time constraints are common barriers, this review highlights that effective teaching can occur in short tutorials without hands-on access to dermatoscopes.19,20,22,24,27,28 These results should be interpreted as evidence of feasibility and value for early exposure, rather than suggesting that UGME training alone can achieve full competency.
Studies also assessed the beliefs and attitudes of medical students as they pertain to dermoscopy.19–21,24 Dermoscopy training positively influenced students’ confidence, reported routine skin examination practices, and interest in using dermoscopy in their future careers.19–21,24 Some studies reported diminished confidence without continued practice.19–21,24 This highlights the importance of integrating dermoscopy into clinical settings to reinforce skills and sustain motivation. While Liebman et al (2012) did not report statistically significant differences between cohorts concerning attitudes toward the value of learning skin examination, 24 educators should harness this increased interest and motivation when available to push learners in their proximal zone of development.
This review has several limitations. The small number of studies (n = 12), predominantly from high-income settings, limits generalizability to low-resource environments. Methodological heterogeneity and inconsistent reporting precluded subgroup analyses, and no gray literature search was conducted. Furthermore, only articles written in English or French were included, which may have excluded relevant studies published in other languages. Future research should prioritize longitudinal studies to assess retention, explore cost-effective asynchronous learning tools, and evaluate dermoscopy education in low-resource contexts. Collaborative efforts could help create standardized, scalable training modules that address diverse institutional needs.
Conclusion
In conclusion, the literature has shown successful yet heterogeneous curricular implementation and level-appropriate effectiveness of dermoscopy teaching in UGME. While these interventions cannot substitute for advanced training, they provide early exposure that may help strengthen students’ foundational skills in SCE and pique learner's future interest in continuing medical education in the domain. Future directions should investigate strategies for longitudinal retention, cost-effective delivery, and how early exposure might be integrated into later stages of medical training and direct patient care.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251385824 - Supplemental material for Dermoscopy Education in Undergraduate Medical Education: Scoping Review of Pedagogical Approaches and Gaps
Supplemental material, sj-docx-1-mde-10.1177_23821205251385824 for Dermoscopy Education in Undergraduate Medical Education: Scoping Review of Pedagogical Approaches and Gaps by Sarah Moussa, Ammar Saed Aldien, Sarah A.E. Aboushawareb, Renata Sava, Elena Netchiporouk and Tamara Carver in Journal of Medical Education and Curricular Development
Footnotes
Abbreviations
Acknowledgments
Many thanks to research librarian Andrea Quaiattini from the faculty of medicine of McGill University for their guidance in the research protocol.
Ethical Considerations
Ethics approval is not applicable.
Contributions
The research protocol was established by SM, ASA, SA, and TC, with clinical guidance from RS and EN for their expertise in dermoscopy. SM led the acquisition and analysis of the data, with ASA as the second reviewer. SM, ASA and TC interpreted the data. SM drafted the manuscript, and ASA, SA, and TC revised it critically for important intellectual content. RS and EN contributed to the discussion with his expertise in ophthalmology. All authors reviewed the reviewers’ comments and provided important intellectual content based on their clinical expertise. All authors read and approved the final version to be published. All authors agree to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
This published article and its supplementary information files include all data generated or analyzed during this study.
Supplemental Material
Supplemental material for this paper is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.