
Abstract
Background
Engaging students in curriculum development provides valuable insights and promotes alignment with their learning needs. Premedical curricula often overemphasize basic sciences, highlighting the need to incorporate social sciences and earlier patient exposure. This study involved students as key stakeholders in redesigning and evaluating the curriculum's clinical relevance.
Methods
A two-phase mixed-methods study was conducted, guided by the context, input, process, product (CIPP) evaluation model. Phase one (context and input) utilized a 5-point Likert-scale questionnaire to assess perceptions of 380 students on premedical learning and its relevance to the preclinical curriculum, alongside open-ended suggestions. Student group activities identified key curriculum issues, informing revisions made in collaboration with the curriculum committee and student representatives, aligned with national medical competency standards. In phase two (process and product), 90 third-year students evaluated the revised curriculum using the same questionnaire with student representatives leading the process. Statistical analyses (Cramér's V, Chi-square, and t-tests) and content analysis were employed.
Results
In the previous curriculum, only 38.48% of students agreed/strongly agreed that premedical subjects aligned with preclinical learning, citing limited clinical relevance and disconnected content (n = 21). A student-led review, in collaboration with the curriculum committee, reduced pure science subjects and integrated them into more clinically relevant content, including early patient exposure in community settings, while maintaining alignment with national medical competency standards. The revised subjects were well received by students. Following these changes, 64.45% of students agreed/strongly agreed that it aligned with preclinical learning, and overall perception scores significantly increased from 18.03 ± 0.16 to 19.08 ± 0.35 (t = 2.819, p = .003).
Conclusion
A student-driven approach, supported by the CIPP model, helped redesign the premedical curriculum. It integrated relevant basic sciences with early community and clinical exposure to enhance alignment, engagement, and preparedness for clinical training.
Keywords
Introduction
Student engagement is essential for developing effective and responsive educational programs, 1 as it fosters a sense of belonging and empowers learners to critically reflect and reframe their perspectives, aligning with established theories such as Mezirow's transformative learning theory.2,3 In medical education, involving students as co-creators alongside a diverse group of stakeholders—including academic staff, Information Technology personnel, curriculum committees, administrative officers, quality assurance teams, and student support services—ensures that curriculum development is collaborative and inclusive 4 This participatory approach, consistent with Arnstein's principles of engagement and Harden's perspectives on modern medical education, 5 enables curricula to remain relevant and adaptable to student needs across disciplines, including premedical subjects that may initially challenge learners.6,7 Consequently, research across multiple fields continues to emphasize the importance of student involvement in curriculum design and evaluation. 8
Modern medical education increasingly emphasizes not only biomedical knowledge but also competencies in Health Systems Science (HSS), Social sciences, and the Medical humanities—critical components for fostering professionalism, cultural humility, and community-responsive care9-11 As the “third pillar” of medical education, HSS encompasses healthcare delivery, population health, and social determinants of health, 9 promoting a more rounded approach to patient care. Early integration of public health and community-based learning nurtures systems thinking and ethical awareness, helping to develop compassionate, well-rounded physicians.10,12
In Thailand, where the medical curriculum follows a six-year direct-entry model that reflects unique cultural and societal needs,13,14 broader goals such as student-centered learning and systems-based education are also gaining momentum. 14 The curriculum consists of premedical, preclinical, and clinical phases. Although recent reforms have emphasized student engagement and clinical competence, revisions typically occur only once every 6–7 years and are driven by key stakeholders—often resulting in outdated content. Additionally, premedical subjects may be perceived by students as burdensome, 7 while community exposure is frequently delayed until the clinical years, limiting early understanding of healthcare systems. These challenges highlight the need for each medical school to implement strategies for early curriculum evaluation and timely adaptation, tailored to its own institutional culture and context.
While previous studies have incorporated student engagement to gain valuable insights,15,16 students have rarely taken a leading role in shaping program development—particularly in the premedical curriculum. Traditionally, their involvement has been limited to providing feedback through structured evaluations, with minimal opportunity to influence or initiate reform. In contrast, this study adopts a student-driven approach, positioning students as the primary stakeholders responsible for initiating the project, leading data collection, conducting evaluations, and participating in final decision-making. By placing students at the center of the entire process, this approach fosters a stronger sense of ownership, deeper engagement, and the potential for more meaningful and contextually relevant curriculum insights. 6
To address student expectations and improve integration across academic years, Phramongkutklao College of Medicine (PCM) in Bangkok, Thailand, revised its traditional premedical science courses to align more closely with clinical education through vertical integration. Guided by the context, input, process, product (CIPP) model and student feedback, the new curriculum emphasizes clinically relevant basic sciences to better support preclinical learning. This study evaluates gaps in the previous curriculum and examines students’ perceptions of curriculum alignment before and after the reform, highlighting how student engagement can guide effective curriculum redesign.
Methods
Study Design and Participants
This study leveraged student engagement to identify curriculum gaps and assess perceptions following a curriculum redesign. A two-phase serial mixed-methods design was used, based on PCM's annual course evaluations. Student representatives—year leaders (typically six per class) and academic club members—were invited annually to assist with planning and data collection.
The sample size calculation indicated a minimum requirement of 80 participants per academic year, based on a total population of 100, with a desired power of 80% and a 5% margin of error. 17 The current study employed census sampling to ensure comprehensive representation of the entire population. The inclusion criteria were all students at PCM who had completed the third-year medical curriculum, while the exclusion criteria were students who declined to participate in the study.
Phase one analyzed evaluations from 396 students who had completed their third year under the previous curriculum between 2018 and 2021. Surveys and group discussions were used to identify and prioritize areas for improvement. Participants in Phase two were PCM students who completed the new third-year curriculum, also selected using census sampling, involving 95 third-year students. Figure 1 summarizes the study steps, participants, findings, decisions, and key contributors in each phase.
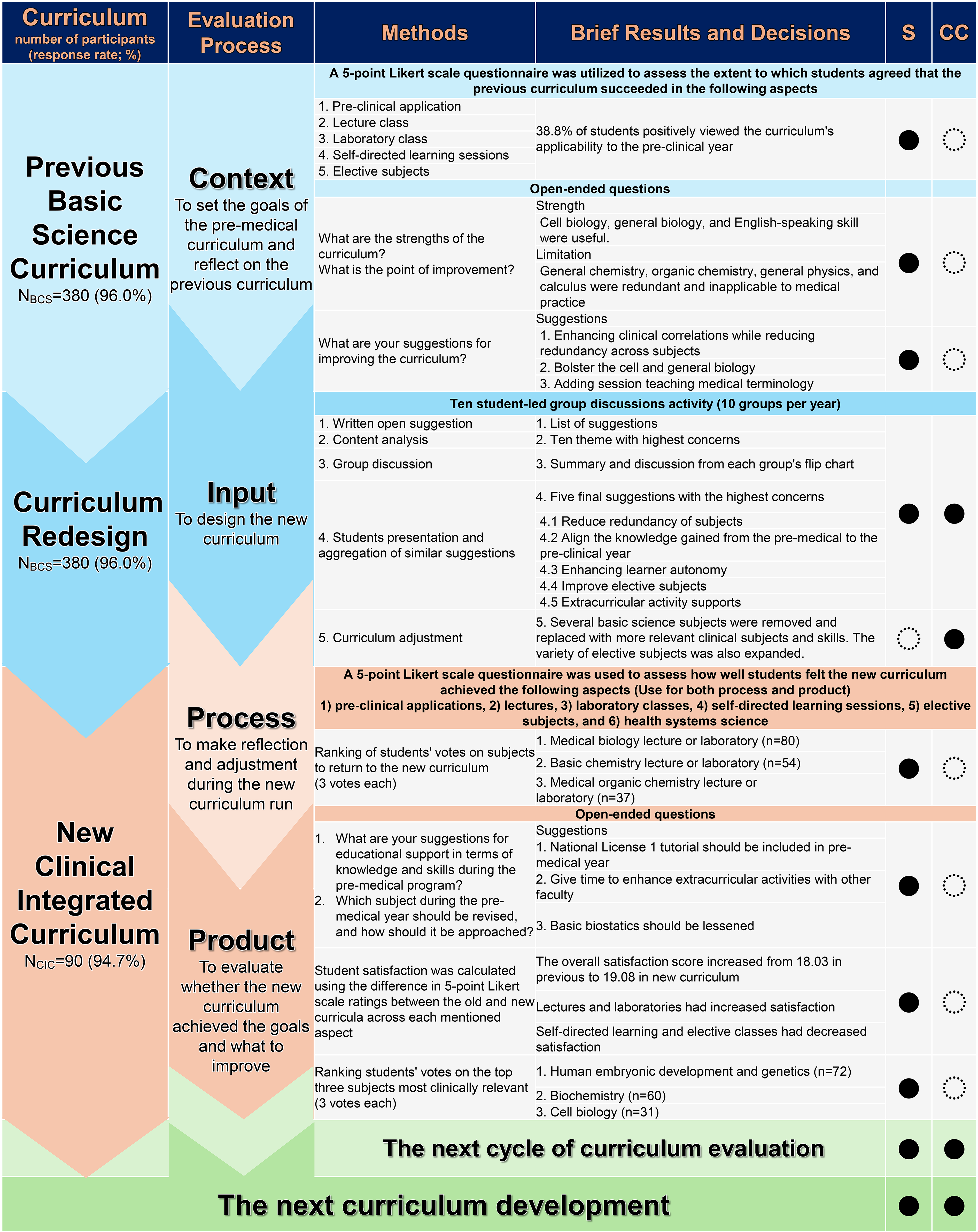
The Flow of the Study, its Brief Results, and the Decision. S, Student; CC, Curriculum Committee; BCS, Basic Science Curriculum; CIC, Clinical Integrated Curriculum. ●, Principal Contributor; ◌, Co-contributor.
Settings
Thailand's Doctor of Medicine (M.D.) program is a direct-entry track from high school, following a standardized national curriculum. Most students come from a science-focused background with strong foundations in Biology, Chemistry, Physics, and Calculus. Admission is through the Thai University Central Admission System (TCAS), a national exam ensuring consistent baseline knowledge among entrants.
At PCM, the program begins with a premedical year focused on basic sciences, followed by two preclinical years linking human body systems with clinical concepts. Clinical exposure intensifies in years four and five, while the sixth year involves full-time externship rotations.
The premedical year is divided into two terms, totaling 20–22 credits per term. The previous curriculum emphasized traditional science subjects (eg, General Chemistry, Physics, Calculus), with 86.3% of credits delivered via lectures. In contrast, the revised curriculum incorporates clinically integrated content (eg, Embryology, Genetics, Biochemistry) and digital skills training, while retaining some original subjects.
Data Collection and Curriculum Evaluation
The curriculum committee developed a questionnaire for the annual evaluation of the premedical and preclinical programs, incorporating components identified from previous course evaluation issues. The questionnaire covers all subjects, learning objectives, and domains, and aligns with the AMEE assessment framework (Supplemental Figure 1). 18 It was designed to collect information on program design, implementation, and outcomes, aiming to monitor and enhance program quality and effectiveness in accordance with the program evaluation definition. 19
The questionnaire development and validation process included the following steps:
Questionnaire development: This involved a literature review of the AMEE framework
18
and item generation, structured into three parts—demographic information, premedical program evaluation, and open-ended questions related to individual subjects. Content validity: Five senior course coordinators assessed the content validity using the item-objective congruence (IOC) method. All items achieved an IOC index of 0.60 or higher, exceeding the acceptable threshold of 0.50.
The student representatives were tasked with distributing the questionnaire and briefing participants about its aims, which focused on facilitating curriculum improvements by integrating students’ perceptions.
CIPP Framework
Program evaluation frameworks include systematic, naturalistic, decision-oriented, and value-oriented approaches. 20 The widely used CIPP model, introduced by Stufflebeam in 1971, fits within systematic and decision-oriented categories.20,21 Rather than focusing solely on outcomes, the CIPP model supports holistic, continuous program improvement and informed decision-making. Its four interrelated components offer structured guidance, especially for inexperienced developers like students. This study used the CIPP model to integrate quantitative and qualitative data, capturing curriculum changes from students’ perspectives. Phase one identified gaps in the previous curriculum (context, input), and phase two evaluated the redesigned curriculum (process, product).
Phase One
Context Evaluation
The context study evaluated the previous premedical course regarding the subjects provided in the curriculum and whether it aligned well with the complexity of clinical correlation.
The general characteristics included gender, age, overall grade point average (GPAX), and type of scholarship. Student satisfaction was assessed using five items rated on a 5-point Likert scale 22 to evaluate the quantitative outcomes of the previous premedical curriculum. The questions covered key components of the program: Applicability of premedical knowledge to the preclinical years, appropriateness of lecture and laboratory sessions, effectiveness of self-directed learning (SDL), and the suitability of elective subjects. Next, an open-ended question followed the questionnaire to evaluate the advantages and disadvantages of applying premedical knowledge to the required and elective subjects in the preclinical year (Supplemental Figure 1).
Input Evaluation
A student-driven approach was employed to design the new curriculum through a structured five-step process (Supplemental Figure 2). Initially, each student individually documented suggestions and concerns regarding the previous curriculum. Student leaders—including heads of academic clubs, class presidents, and volunteers—were then briefed on the goals of the redesign and performed a content analysis to identify recurring themes. These student leaders were trained by a senior faculty committee using a structured, preapproved discussion protocol to ensure consistency and clarity prior to facilitating peer discussions. Several practice rounds were conducted to assess their readiness, as evaluated by the committee.
Small group discussions were conducted after the students completed their third year, with each group consisting of 8–12 participants drawn from approximately 100 students per academic year. Each group summarized the key discussion points on flipcharts. Representatives from the groups presented their findings to the curriculum committee, teachers, and other student groups, after which overlapping suggestions were aggregated.
The five most frequently mentioned and highly prioritized themes were selected. The curriculum committee used these recommendations to revise subject content and reallocate credits, as shown in Supplemental Table 1. These new topics were aligned with, and in some cases served as simplified introductions to, preclinical subjects. They were designed to meet the Medical Competency Assessment Criteria for National Licensing, while remaining within the scope of available resources and the foundational knowledge expected of first-year medical students. 23
Phase Two
Process Evaluation
The process study assessed the implementation of the new premedical program during its execution, providing formative information to guide subsequent revisions of the process.
Students were asked to vote on subjects from the previous basic science curriculum, “Which subjects should be added to the new curriculum?”. Furthermore, a 5-point Likert scale 22 was employed, like that used in the previous curriculum. The preferences for subjects to be returned to the new clinical integrated curriculum were analyzed by ranking students’ votes.
Next, open-ended questions were posed to gather insights into educational support. Students were asked questions such as, “What are your suggestions for educational support in terms of knowledge and skills during the pre-medical program?” and “Which subject during the pre-medical year should be revised, and how should it be approached?”
Product Evaluation
The outcomes of the new curriculum were evaluated using the same questionnaire previously employed in the context evaluation of the former curriculum. Differences in student satisfaction between the previous and new curricula were analyzed using independent t-test, Mann-Whitney U, and Cramer's V. Next, open-ended questions were collected “What are your suggestions for the pre-medical curriculum?” Students were also asked, “Which three subjects are most closely correlated with the subsequent clinical years of the study program?”.
Role of Curriculum Committee in Each Step of Evaluation
The curriculum committee, comprising school directors, department heads, and coordinators, invited student representatives to participate voluntarily in the evaluation process. Students were guided through the CIPP model to ensure understanding and were empowered to lead the evaluation independently. Figure 1 outlines the key contributors at each stage. The role of the committee can be summarized as follows:
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement, which provides guidelines for ensuring transparency and completeness in observational research. The completed STROBE checklist has been included as a
Ethics Approval and Consent to Participate
The study was approved by the Medical Department Ethics Review Committee for Research in Human Subjects, Institutional Review Board, RTA (approval no. M039 h/66_Xmp), in accordance with the international guidelines, including the Declaration of Helsinki, the Belmont Report, CIOMS Guidelines, and the International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use–Good Clinical Practice (ICH-GCP). Written informed consent was obtained from all participants, or their legally authorized representatives in applicable cases (eg, minors or individuals unable to provide consent), following the COPE guidelines.
Statistical Analysis
Quantitative Analysis
All quantitative analyses were performed using StataCorp, 2021, Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC. All statistical tests were two-sided, and a p-value less than .05 was considered statistically significant. The categorical data were expressed as frequency and percentages. Continuous variables were presented as either means and standard deviations (SDs) or medians and interquartile ranges (IQRs) as appropriate. Comparisons between perceptions on previous and new curriculum were conducted using the independent t-test, Mann–Whitney U test, or Cramér's V, as appropriate. The internal consistency reliability of the questionnaire was assessed using Cronbach's alpha, and construct validity was evaluated through exploratory factor analysis (EFA).
Qualitative Analysis
Content analysis was employed to examine students’ suggestions and perceptions as expressed in open-ended questions. This process was divided into five stages: Familiarization with the data, condensing, coding, categorizing, and thematizing. 25 All authors and student representatives participate in this iterative process each year, convening to finalize the codes and themes. The number of student answers that fell into the themes was counted and presented. The final findings are presented as codes, subthemes, themes, and quotations within the framework of the CIPP model.
Results
Characteristics of Participants
A serial survey of 470 students’ perspectives was conducted. Phase one gathered the views of 380 students from the 2015 to 2018 premedical basic science program. The response rate for phase one was 96.0%. The total number of students enrolled from 2015 to 2018 was 98, 101, 86, and 95, respectively, with response rates of 100.0%, 97.1%, 88.7%, and 97.9%. Phase two collected 90 students’ views about the new premedical curriculum (Response rate 94.7%) (Figure 1).
Phase One of the Premedical Curriculum Evaluation
Context
The premedical curriculum at PCM was evaluated annually from 2015 to 2018. The questionnaire had acceptable internal consistency reliability (Cronbach's alpha = 0.77). EFA supported its unidimensionality (eigenvalue ratio = 2.65:0.78; KMO = 0.79; Bartlett's test p < .001), with factor loadings ranging from 0.63 to 0.81 (Figure 2).

Exploratory Factor Analysis of the Questionnaire on Perceptions of Curriculum Activities.
Only 38.78% of students agreed the curriculum supported preclinical learning. Five key concerns emerged from 131 open-ended responses:
Input
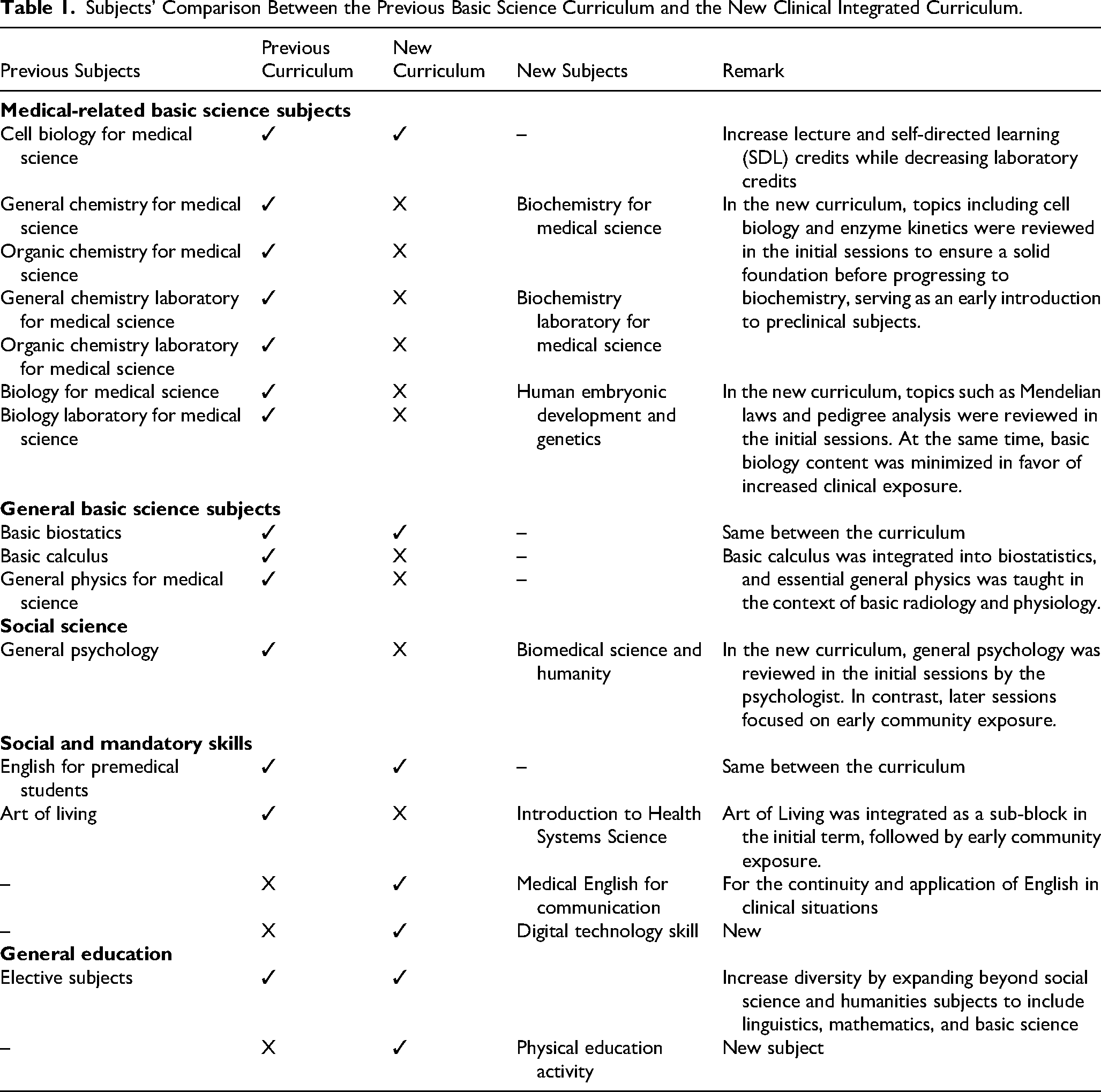
The new PCM premedical curriculum was developed in response to prior student feedback. Sixteen themes of concern were identified over four years (Supplemental Table 2), with 11 addressed through ongoing revisions. These led to five key recommendations: reduce redundancy, link to preclinical content, promote learner autonomy, improve electives, and support extracurriculars. As a result, the revised curriculum added Biochemistry, Biomedical Science, Embryology, and Genetics, while reducing or integrating less relevant subjects such as Calculus, Physics, and Chemistry—for example, essential Calculus concepts were retained through Biostatistics. To align with HSS principles and strengthen clinical relevance, early community exposure was introduced, helping students understand healthcare delivery and patient care in real-world settings. Elective offerings were also expanded to support diverse interests and interdisciplinary learning. Subject and credit comparisons appear in Table 1.
Subjects’ Comparison Between the Previous Basic Science Curriculum and the New Clinical Integrated Curriculum.
Phase Two of the Premedical Curriculum Evaluation
Process
Supplemental Figure 3 presents student votes on subjects to reinstate during curriculum implementation. Of 194 votes, few supported calculus (n = 2, 1.0%), logic (n = 5, 2.6%), or physics (n = 8, 4.1%), suggesting the revised curriculum met most students’ needs. Notably, 23 students (25.6%) did not vote.
Open-ended responses in Phase two (n = 42) highlighted three themes:
NL1 Preparation from Year 1 (n = 10): Students recommended early preparation since premedical topics appeared in the third-year NL1 exam. One noted, “Each subject should be correlated with NL1 preparation,” while another added, “There should be an NL examination tutorial since 1st medical year.” Limited Time for Review (n = 6): Tight Year 2–3 schedules hindered NL1 revision. A student said, “With the packed schedule in the 2nd and 3rd years, we simply don’t have enough time to review and understand all the basic science topics for the exam.” More Time for Extracurriculars (n = 2): Students wanted flexibility for cross-faculty activities, as one stated, “We need more time for extracurricular activities with students from other faculties.”
Product
Table 2. Compares the students’ satisfaction between the previous and new curricula. The overall perception score increased from 18.03 ± 0.16 in the previous curriculum to 19.08 ± 0.35 in the new curriculum (t(465) = 2.819, p = .003, Cohen's d = 3.18) (Figure 3). The median (IQR) score for knowledge application of premedical to preclinical years improved from 3 (3-4) to 4 (3-4) (U(1) = 4.798, p < .001). The median (IQR) satisfaction with the lectures and laboratory subjects also increased significantly. Moreover, 38 students (42.2%) agreed or strongly agreed that early community exposure was appropriate in the new curriculum, with a median (IQR) score of 3 (3-4).
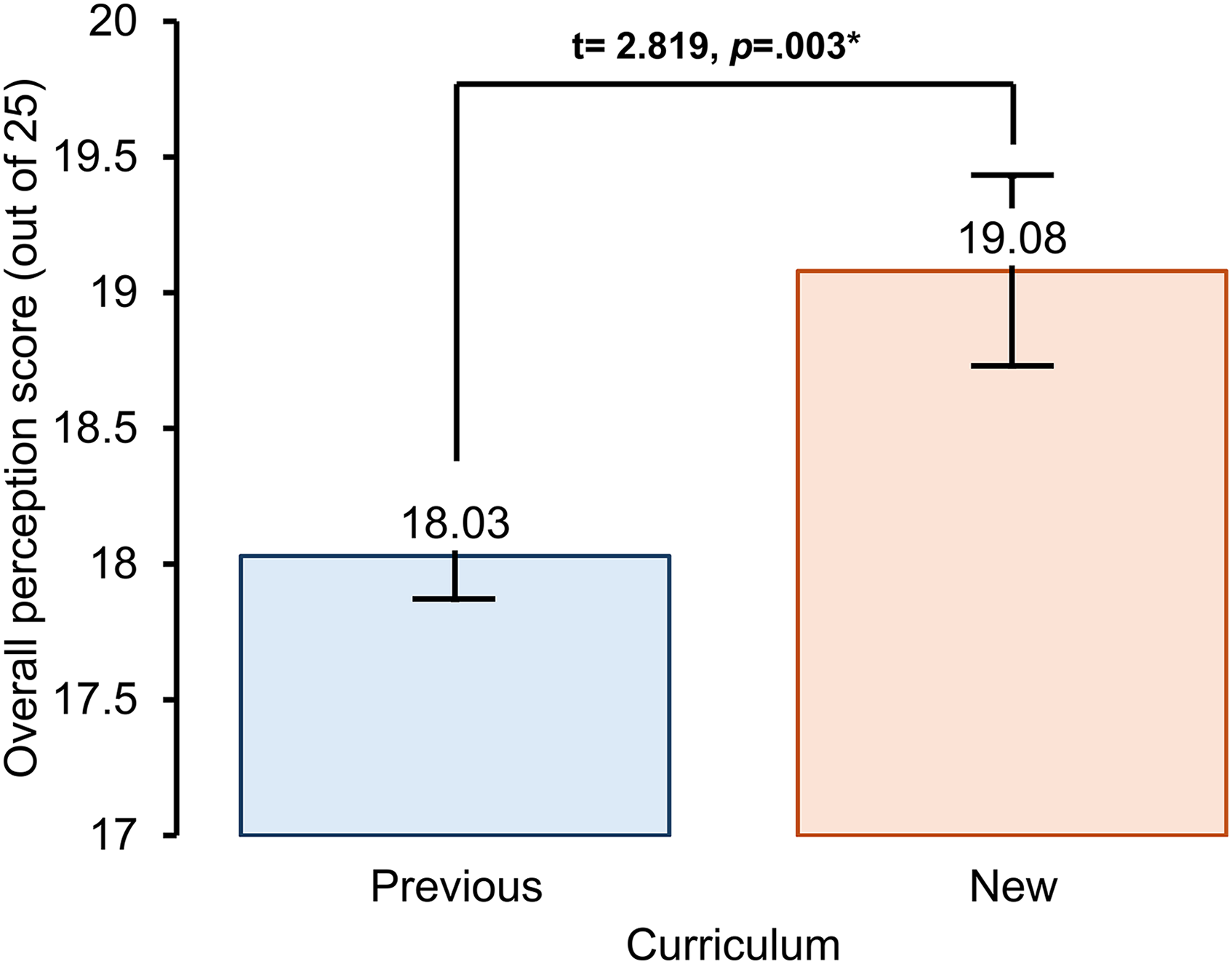
Overall Students' Perception Comparing Previous and New Curriculum, *Indicate Significant Difference of p-Value.
Comparison of Students' Perception Between the Previous and New Curriculum (N = 470).

SD, standard deviation; IQR, interquartile range. aindependent t-test. bMann-Whitney U test. cCramer's V.
Further analysis of student feedback on the new subjects in the curriculum revealed that students are generally satisfied with the integration of Embryology and Biochemistry into the premedical curriculum. “Embryology is suitably integrated into the pre-clinical year curriculum.” Some respondents say that “it is crucial to allocate more time to study Human Embryology” (n = 27 responses). Moreover, they found it enhanced the accessibility and benefits of preclinical studies (n = 24 responses). A student mentioned, “It is also easy to apply Biochemistry studied in the pre-medical year to the pre-clinical subjects.”
Discussion
This study enrolled 470 students and effectively demonstrated student engagement in the curriculum redesign using the CIPP model as a guiding framework. It also demonstrated the evaluation cycle, from identifying the background and areas for improvement to assessing the outcomes of the premedical curriculum. The findings suggest that the new clinical integrated curriculum offered enhanced clinical correlation, while reducing redundancy of subjects, as elements of students’ perceptions of the previous curriculum were extracted and implemented. Additionally, the study revealed students’ perceptions of the premedical curriculum, which could serve as a guide for several medical schools with similar curriculum contexts.
Similar to the present study, medical curriculum reform faces several challenges, including limited curricular time, increased teaching demands, and the influence of national licensing requirements. 7 Although efforts to reduce redundancy in basic science content are well-intentioned, they have often led to a diminished emphasis on biomedical sciences.26,27 Therefore, while integrating new topics, it is essential to preserve core scientific content and ensure alignment with the Medical Competency Assessment Criteria.
Previous studies have highlighted additional pressures from the integration of HSS, which competes for faculty time and curricular space. 27 Educators must respond to modern students’ learning preferences while upholding academic rigor and preparing them for clinical uncertainty. 5 To address these challenges, some institutions have reinstated subject-based courses, such as pathology, to preserve foundational knowledge. 26 Therefore, coordinated, nonmodular integration of core and emerging topics may thus offer a more sustainable approach without compromising the integrity of medical science education.
The CIPP model, a well-established and systematic framework,20,21 supports student involvement in each phase. While previous uses were resource-intensive,17,28 this study demonstrated that streamlined, student-led evaluation is feasible and meaningful even in resource-limited settings. However, the time and cognitive load required for students to participate in such evaluation should not be underestimated. Nevertheless, the strong student adherence in this study likely stemmed from a participatory design that fostered autonomy, competence, and belonging, consistent with self-determination theory.29,30 Importantly, incorporating student feedback helped bridge gaps in the student–instructor relationship 6 and promoted inclusivity, even when the framework was initially unfamiliar. This is particularly important in diverse student groups, where such considerations should be prioritized.6,8
Context Evaluation
A validated questionnaire, combining both structured and open-ended questions, demonstrates internal consistency and construct validity through testing, thereby enhancing the evaluation's robustness and ensuring the questionnaire accurately measures the intended constructs. The context evaluation captured comprehensive student concerns, highlighting needs for nontechnical skills like Medical English and digital literacy, 31 skills increasingly vital in the artificial intelligence era. 32 Therefore, the importance of nontechnical skills, which may be underemphasized in many medical schools, should be considered more. 33
Input Evaluation
A five-step student-driven approach was implemented to generate key recommendations for the curriculum committee in redesigning the curriculum. This method facilitates thorough program evaluation and prioritization of concerns. The systematic approach enhances student engagement, promotes collaborative decision-making, fosters leadership and critical thinking, and ensures transparency. These attributes are essential for student engagement and inclusivity,6,8 thereby supporting sustainable evaluation cycles.
Process Evaluation
The process evaluation assessed whether curricular adjustments aligned with students’ expectations and academic needs. Students favored replacing basic science subjects with applied medical sciences to reduce cognitive burden. Interactive methods, such as team-based learning, helped contextualize knowledge within clinical applications. 34
Product Evaluation
The new curriculum was rated more favorably by students, reflecting improved alignment and perceived relevance. However, challenges remain, particularly concerning inadequate SDL. These concerns are particularly relevant as new subjects are integrated, raising questions about time allocation and potential learning inefficiencies. 35 Curriculum overload and limited independent study time continue to pose barriers to meaningful engagement. For first-year students who are still developing clinical reasoning, additional support and appropriately allocated SDL time are essential. As this is the first postimplementation evaluation, ongoing refinement and longitudinal assessment will be critical to ensure lasting improvements. 36
Key Information from the Premedical Curriculum Redesign
Preparation for the NL1 examination was a primary concern for medical students. Research indicates that serial evaluations during preclinical years help predict NL1 performance, with intense study habits being key to success. 37 In response, an NL1 preparation course may be considered, as suggested by students. However, debate persists over whether the exam accurately assesses medical competency. Given their short-term memorization, some students view foundational sciences as irrelevant to clinical practice. This may lead to an underappreciation of basic sciences in clinical settings. 38 Moreover, an excessive focus on NL1 tutorials may place undue emphasis on cognitive domains, potentially neglecting other essential areas, such as affective and psychomotor domains.
When removing subjects such as Calculus, Physics, and Chemistry and revising the Basic Biology Curriculum to incorporate Human Embryonic Development and Genetics, it is crucial to ensure that the newly introduced subjects align with the standards set by the Medical Competency for National Licensure. 23 Additionally, these subjects should be designed to be accessible without requiring advanced prerequisite coursework. Moreover, although the admission system ensures a fundamental level of knowledge among students, some variability in their high school backgrounds may lead to gaps in foundational knowledge. To address this, SDL resources, such as e-learning modules covering essential fundamental concepts, should be provided before the advanced lessons. For instance, before studying cell biology, students could be given introductory resources on biological molecules, cellular structures, and fundamental life processes to ensure a more uniform understanding.
Strengths and Limitations
To the best of our knowledge, this is the first study to apply the CIPP model through a student-led framework in premedical education. The approach centers students as key stakeholders, reinforcing their sense of belonging, autonomy, and competence. It also enhances communication between students and educators, promoting a more collaborative academic culture and laying the groundwork for future co-creation. 6
However, several limitations must be acknowledged. The cross-sectional nature of this evaluation restricts insight into long-term outcomes. Future research should assess academic performance, licensing exam results, and clinical readiness to gauge the lasting effects of curricular changes. Additionally, as this study was conducted at a single institution, generalizability may be limited. The success of student-led evaluation also depends on the commitment and representativeness of student participants. Early planning, mentorship, and voluntary engagement are therefore essential. Furthermore, as qualitative data were collected continuously over multiple years, specific interventions were implemented annually to address students’ concerns. Given the evolving nature of these concerns, with new issues and themes potentially emerging each year, achieving data saturation may have been a challenging task. Nevertheless, the main concerns of the students were focused and tackled each year. Lastly, the study focused primarily on student perspectives, along with input from curriculum committee members who do not hold additional administrative roles. Perspectives from other key personnel, such as Academic Affairs staff and Information Technology staff, were not included. Future evaluations should incorporate input from faculty and a broader range of stakeholders to build a more comprehensive understanding. Despite these limitations, the study demonstrates that structured, student-led evaluation using the CIPP model is both feasible and impactful, offering a replicable model for curriculum development in other settings.
Conclusion
This study demonstrates the value of student engagement in curriculum redesign, using the CIPP model as a structured yet accessible framework. The model supported a comprehensive evaluation process, from identifying student expectations to informing decisions and assessing curricular changes. Integrating students as key stakeholders ensured their perspectives were prioritized, fostering intrinsic motivation and active participation. Importantly, the findings offer practical insights for premedical curriculum reform. Students emphasized the need for stronger clinical integration within basic sciences and recommended removing less relevant content. These modifications improved curricular alignment with core medical concepts and enhanced student satisfaction and engagement.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251374898 - Supplemental material for Student Engagement in Program Evaluation: Redesigning the Premedical Curriculum Through Instructor–Learner Co-Creation
Supplemental material, sj-docx-1-mde-10.1177_23821205251374898 for Student Engagement in Program Evaluation: Redesigning the Premedical Curriculum Through Instructor–Learner Co-Creation by Panrawee Sertsuwankul, Sethapong Lertsakulbunlue, Mathirut Mungthin and Anupong Kantiwong in Journal of Medical Education and Curricular Development
Supplemental Material
sj-doc-2-mde-10.1177_23821205251374898 - Supplemental material for Student Engagement in Program Evaluation: Redesigning the Premedical Curriculum Through Instructor–Learner Co-Creation
Supplemental material, sj-doc-2-mde-10.1177_23821205251374898 for Student Engagement in Program Evaluation: Redesigning the Premedical Curriculum Through Instructor–Learner Co-Creation by Panrawee Sertsuwankul, Sethapong Lertsakulbunlue, Mathirut Mungthin and Anupong Kantiwong in Journal of Medical Education and Curricular Development
Footnotes
Abbreviations
Acknowledgments
The authors sincerely appreciate the Phramongkutklao College of Medicine and its esteemed academic leaders, whose active support was vital for completing this work. Their names are too numerous to mention individually, but their involvement was instrumental in making this project possible. We also utilized ChatGPT-4.0 to assist with grammar editing of the manuscript; however, the authors remain fully responsible for the accuracy and integrity of the content.
Abbreviations
Ethical Approval
This study was approved by the Medical Department Ethics Review Committee for Research in Human Subjects, Institutional Review Board, Royal Thai Army (RTA) (Approval no. M039 h/66_Xmp), in accordance with international ethical standards including the Declaration of Helsinki, the Belmont Report, CIOMS Guidelines, and ICH-GCP.
Informed Consent
Written informed consent was obtained from all participants, or their legally authorized representatives in applicable cases (eg, minors or individuals unable to provide consent), following the COPE guidelines.
Authors’ Contributions
The concept for the study was developed by SL, PS, MM, and AK. SL, PS, MM, and AK collected the data, SL and PS analyzed the data, and SL, PS, and AK wrote the first draft. All authors contributed to and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the author on reasonable request. (contact xxx via xxx).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.