
Abstract
Background
The traditional medical school curriculum has offered few opportunities to enhance and support interest in primary care (PC), particularly for medical students who have completed their core clinical clerkships. The Primary Care Senior Seminar (PCSS) is a 4-week course at the Keck School of Medicine for post-clerkship medical students consisting of clinical and didactic experiences, leadership training, skills-based workshops, and exploration of community-based health resources. The PCSS curriculum teaches critical PC concepts and skills to further motivate and solidify student interest in PC careers. This study examines the impact of the PCSS on medical students' knowledge and confidence in foundational PC skills and their future residency plans.
Methods
Thirty-six medical students enrolled in the PCSS completed a pre- and post-survey. Quantitative analysis was conducted in Qualtrics and Excel with significance at P < 0.05.
Results
Students participating in the PCSS gained significant knowledge and skills in foundational PC areas including patient communication, healthcare systems, preventive medicine, chronic illness management, in-office procedures, quality improvement (QI), and leadership. Additionally, participation in the PCSS appeared to support and motivate students to pursue PC careers. At the end of the course, students who entered feeling confident they would pursue a PC career remained confident in their decision, and many students who were initially undecided became more committed to PC.
Conclusions
The PCSS can serve as a replicable model for implementing a PC curriculum that will help medical schools train more highly skilled PC doctors and motivate undecided student to pursue PC careers.
Introduction
With a significant shortage of United States primary care (PC) physicians, 1 there have been multiple efforts to increase PC undergraduate and graduate medical education training programs. 2 Medical schools have developed strategies to attract and retain students entering PC, including longitudinal pathway programs, PC clerkship experiences, and rural training programs3,4; however, there is limited data about efforts during the post-clerkship period to increase PC match rates and PC skill-building.
Traditional medical school curriculums allow only a few months after students' third-year clinical clerkships to complete required sub-internships or electives and apply to residency. With an emphasis on allowing medical students more autonomy to individualize their training, more medical schools are changing their curriculums to an 18 month pre-clerkship, 12 month clerkship, and 18 month post-clerkship model. 5 Additional time during the post-clerkship period allows more opportunity for students to explore their desired specialty through sub-internships and electives, most of which are purely clinical and specialty-specific. There is minimal research in the literature on post-clerkship electives blending clinical experiences and didactics and focused broadly on PC—most existing research focuses on clinical electives in rural settings and/or within a particular specialty such as Family Medicine. 4
The Keck School of Medicine (KSOM) of University of Southern California (USC) adopted an 18-month post-clerkship model beginning in 2021 with the class of 2025. 6 With the first student cohort now reaching their post-clerkship period, the Primary Care Initiative 7 developed a new PC-focused elective, the Primary Care Senior Seminar (PCSS). The PCSS provides an opportunity for advanced PC training for post-clerkship medical students who have demonstrated PC interest since their matriculation as well as those who developed an interest in PC during medical school. The PCSS curriculum is unique in that it blends clinical experience and formal skills-based didactics and is designed for students planning to pursue PC but who may not know what, specifically, they want to do within PC in terms of specialty and/or scope of practice. Additionally, the PCSS takes place in an urban setting with emphasis on caring for urban underserved populations. This study builds on the existing literature of PC post-clerkship electives by discussing the impact of this elective on general PC skills acquired and specialty decision making among students.
This study describes the attributes of the PCSS curriculum and the outcomes of the first PCSS cohort of KSOM students. It offers a model for other schools developing an advanced PC curriculum and uniquely contributes to the literature by reporting on how such a curriculum can potentially influence students' planned specialty choice and scope of practice. With a national deficit of PC-bound medical students, curricular models that enhance PC skills, encourage PC career trajectories, offer PC advocacy and leadership training, and describe PC opportunities, are essential to continue to attract and retain future PC physicians.
Methods
Students
All KSOM students are allowed to choose a senior seminar elective halfway through their clerkship year. Senior seminar elective options were PC, Medical Education, Business of Medicine, Quality and Safety, Global Health, Digital Medicine, Narrative Medicine, Biomedical Research, and Social Medicine and Advocacy.
Thirty-seven out of 186 third-year KSOM medical students (20%) elected to participate in the 4-week PCSS. Students in the longitudinal KSOM PC pathway, the Primary Care Program (PCP), 8 were given enrollment priority. 27 PCP students enrolled in the PCSS (out of 32 PCP students) and 10 non-PCP students enrolled.
Primary Care Senior Seminar Curriculum
Content Overview
PCSS curriculum supplemented and enhanced the regular medical school curriculum for students interested in pursuing PC careers. The course took place February 26-March 22, 2024 after students' clerkship year. The 4-week course had 40 h/week of curriculum (Supplementary File 1), with six key components:
Clinical experience, Didactics/small group discussions, Skills workshops, Leadership training, Quality Improvement (QI), and Community exploration.
Clinical Experience
Students spent 2 days/week (8 days total) working with PC preceptors (Family Medicine, Internal Medicine [IM], Pediatrics [Peds], and Med-Peds) in community clinics. Each student was assigned to a different clinic/preceptor based on their interests within PC (ie, a student interested in working with pediatric patients was placed with a pediatrician or a FM physician seeing a high volume of pediatric patients). Most students were placed in community clinics working with underserved patient populations, and many were able to enhance their skills providing care in a language other than English.
Didactics/Small Group Discussions
The remaining 3 days/week were split among didactics, workshops, leadership training, QI, and community exploration. In accordance with adult learning theory, the PCSS emphasized active, experience-based learning.
9
Didactic sessions were interactive and often centered around small group discussions or projects. Each week emphasized different themes:
Week 1: Communication Week 2: Health systems Week 3: Advocacy Week 4: Care across the lifespan and vulnerable populations
Some didactic sessions involved “field trips” relevant to the subject material (ie, the substance use disorder [SUD] lecture was given at a residential SUD treatment facility and included a facility tour). Lectures and workshops were led by PC KSOM faculty and guest speakers including physicians, pharmacists, social workers, dieticians, community leaders, and patients.
Workshops
Workshops focused on teaching practical, hands-on skills, including Point of Care Ultrasound, and office-based procedures. Students practiced procedures in gynecology, dermatology, and sports medicine with learning aids (ie, papayas were used to simulate a uterus for the endometrial biopsy workshop). All workshops were preceded by an overview of the indications and methods for a given procedure, as well as reviewing the process of obtaining informed consent.
Leadership Training
Leadership and community exploration were integrated into multiple aspects of the curriculum. Prior to the PCSS, students completed a CliftonStrengths leadership assessment, 10 to characterize their personal leadership style. Students attended weekly leadership lectures where guest speakers representing different stages and styles of leadership spoke about their leadership paths, and students completed team-based exercises. Students wrote and submitted a leadership journal reflecting on their own leadership journey.
QI Project
During the PCSS, students were tasked with initiating a QI project in their community clinic. Students were introduced to the principles and purpose of QI during their first day of the elective. They worked with their community clinic preceptor to identify a QI topic relevant to their clinic. Students then initiated a needs assessment to characterize the current state of their target measure and performed a literature review. They worked with clinic providers to set a goal for improvement and to design an intervention. Given the short time frame, implementation was not required, though some students did implement their intervention. Students completed QI progress reports each week and completed a final write up and presentation. Some students used this opportunity to complete a KSOM requirement for research, taking additional research elective time to further their QI projects and develop posters, abstracts, and peer reviewed publishable manuscripts.
Community Resource Exploration
Students were given flexible time to explore a community organization of interest (ie, Alcoholics Anonymous, food bank) for at least 2-4 h and learn about the populations they serve and the resources they provide. PCSS staff assembled and shared a full list of these community resources for students to utilize in their future careers. Students had the opportunity to explore the value and importance of community resources and future referral sources for patient support, a PC foundational skill.
Grading
PCSS grading strongly emphasized participation and professionalism. To receive credit, students were required to:
Attend all didactic sessions, workshops, and leadership lectures and complete associated assignments, Attend all clinic sessions and meet KSOM clinic performance and professionalism standards, Initiate, write up, and present a clinic-centered QI project, and Volunteer or shadow at a designated community organization.
All sessions were held in person. Absences could be requested and excused on an individual basis according to KSOM policies, and students completed make-up assignments determined by the course directors for any sessions missed.
Survey Instrument
All PCSS students were eligible to complete the survey. A Qualtrics survey link was shared with students on their first day (pre-survey) and last day (post-survey) (Supplementary File 2). Students were given class time to complete the survey. The survey was optional. Survey questions were divided into 10 categories. Eight categories correspond to explicit course content taught during the PCSS, including: (1) communication, (2) health systems, (3) office-based procedures, (4) healthcare maintenance and cancer screening guidelines, (5) chronic disease management, (6) vulnerable populations, (7) QI, and (8) leadership. Category 9 questions explored students' professional development skills in areas like leadership, advocacy, and teaching, and their intent to incorporate these into their future career. Category 10 questions asked about intended career path and specialty choice. Within each category, students rated their responses on a 5-point Likert scale (strongly disagree to strongly agree). All answers were self-reported.
Data Analysis
Likert scale responses were quantified so that a comparison of means pre- and post-PCSS could be conducted for statistical significance determined at P < 0.05. The numeric values assigned to each question were 1—strongly disagree; 2—disagree; 3—neither agree nor disagree; 4—agree; 5—strongly agree. Analysis was conducted through Qualtrics and Excel. The study was deemed exempt by USC's IRB (UP-20-01459). The reporting of this study conforms to the DoCTRINE Guidelines (Supplementary File 3). 11
Results
Among the 37 PCSS students, 36 students completed both the pre- and post-survey (97%). 100% of respondents were satisfied or very satisfied with their PCSS experience. Additionally, 100% agreed or strongly agreed that they were exposed to multiple PC role models. Results are presented below in the 10 survey categories (Table 1).
Senior Seminar Pre- and Post-Survey Results.
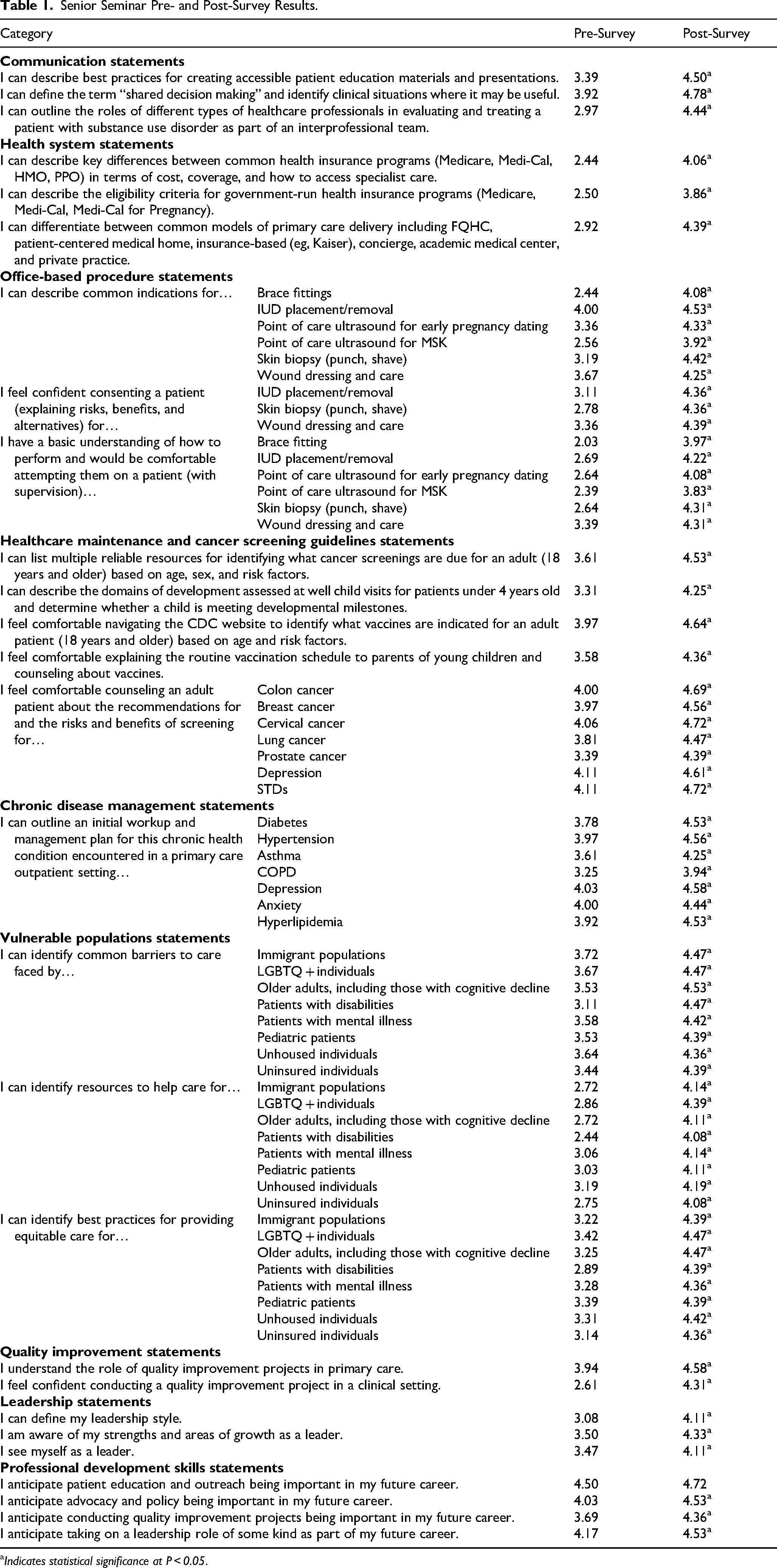
Indicates statistical significance at P < 0.05.
Communication
The average increase on the 5-point Likert scale for the 3 communication questions was 1.15 (3.425 pre; 4.573 post) and increases for each question were statistically significant. Questions focused on knowledge/comfort surrounding creating accessible patient education materials/presentations, understanding and implementing “shared decision making”, and identifying the roles of interprofessional healthcare professionals to treat patients with substance use disorders.
Healthcare Systems
The average increase on the 5-point Likert scale for the 3 health care system questions was 1.48 (2.62 pre; 4.10 post) and increases for each question were statistically significant. Questions focused on describing the differences between and eligibility criteria for various health insurance programs and models of PC delivery.
Office-based Procedures
The average increase on the 5-point Likert scale for the 15 office-based procedure questions was 1.27 (2.95 pre; 4.22 post) and increases for each question were statistically significant. Questions focused on recognizing indications for procedures, consenting a patient, displaying a basic understanding of how to perform and being comfortable attempting a variety of procedures including brace fitting, skin biopsy, IUD placement, and wound care.
Healthcare Maintenance and Cancer Screening Guidelines
The average increase on the 5-point Likert scale for the 11 healthcare maintenance and cancer screening guideline questions was 0.73 (3.81 pre; 4.54 post) and increases for each question were statistically significant. Questions focused on identifying reliable resources for cancer screening guidelines, describing domains of development and determining developmental milestones, identifying indicated vaccines, explaining routine vaccination schedules to parents, and counseling patients about screening recommendations/risks/benefits for a variety of cancers, depression, and STDs.
Chronic Disease Management
The average increase on the 5-point Likert scale for the 7 chronic disease management questions was 0.61 (3.79 pre; 4.40 post) and increases for each question were statistically significant. Questions assessed comfort in counseling an adult about the recommendations/risks/benefits of treatments for chronic conditions including asthma, depression, and diabetes.
Vulnerable Populations
The average increase on the 5-point Likert scale for the 24 vulnerable population questions was 1.13 (3.20 pre; 4.33 post) and increases for each question were statistically significant. Questions focused on identifying common barriers to care and providing equitable care for vulnerable populations including unhoused, uninsured, and LGBTQ individuals.
Quality Improvement
The average increase on the 5-point Likert scale for the 2 QI questions was 1.17 (3.278 pre; 4.444 post) and increases for both questions were statistically significant. Questions assessed understanding of the role of QI projects in PC and confidence in conducting a QI project.
Leadership
The average increase on the 5-point Likert scale for the 3 leadership questions was 0.83 (3.352 pre; 4.185 post) and increases for each question were statistically significant. Questions assessed respondents' ability to define their own leadership style, strengths, areas of growth, and ability to see themselves as leaders.
Professional Development Skills
The average increase on the 5-point Likert scale for the 4 professional development questions was 0.44 (4.097 pre; 4.535 post). Students reported a statistically significant increase in anticipating that the following will be important in their future career: advocacy and policy (P = 0.008), conducting QI projects (P = 0.001), and taking on leadership roles (P = 0.03). Students did anticipate incorporating education and outreach into their future careers (4.50 pre, 4.72 post), but the difference between pre and post was not statistically significant.
Future PC Career
Students were asked about their intent to pursue a PC career and the specialty they planned to pursue pre- and post-PCSS. The average increase on the 5-point Likert scale for the 2 questions was 0.22 (3.64 pre; 3.86 post). There was not a statistically significant aggregate difference; However, we further analyzed results by comparing individual respondents' answers pre- and post-PCSS. For this section, “agree” encompasses strongly agree and agree responses, and “disagree” encompasses strongly disagree and disagree responses.
Students indicated their agreement with the statement, “I am certain (90% or more) that I will pursue a career in PC.” We compared each individual's response pre- and post-PCSS. The most common response patterns were 44.5% (n = 16) agreed pre- and post-PCSS; 19.5% (n = 7) neither agreed nor disagreed pre-PCSS and then agreed post-PCSS; and 17% (n = 6) neither agreed nor disagreed pre- and post-PCSS (Table 2, Figure 1).

Certainty of Pursuing a Career in Primary Care.
Career Survey Questions Categorizing Pre- and Post-Survey Patterns.

Students also indicated their agreement with the statement, “I am certain (90% or more) of the specialty I will pursue” pre- and post-PCSS. The most common response patterns were 53% (n = 19) agreed pre- and post-PCSS, 14% (n = 5) neither agreed nor disagreed pre-PCSS and then agreed post-PCSS; 14% (n = 5) neither agreed nor disagreed pre- and post-PCSS (Table 2, Figure 2). Among students who indicated they were certain of their specialty post-PCSS (n = 25), 15 said they planned to apply in FM, 4 said IM, 1 said Peds, 1 said OB/GYN, 1 said Psychiatry, 1 said Emergency Medicine, 1 said General Surgery, and 1 said IM or Peds (Table 3).

Certainty of Specialty Pursuit.
Specialty Choice Among Students Pre- and Post-Senior Seminar.

Discussion
The PCSS was successful in achieving its two overarching goals: First, to provide students interested in PC with practical knowledge and skills to prepare them to be successful PC residents, physicians, and effective leaders. Second, to expose students undecided about their specialty to PC core values, mentors, and practice models to motivate and educate them about the benefits/opportunities of a future PC career. This study builds on existing literature by evaluating a broadly PC-focused post-clerkship, combined clinical and didactic elective in an urban setting, and by reporting on its effects on students' planned scope of practice and specialty within PC.
Comparing student self-report responses pre- and post-PCSS, students gained a statistically significant increase in knowledge of or confidence in each of the studied content areas: communication, health systems, office-based procedures, healthcare maintenance, chronic disease management, vulnerable populations, QI, and leadership. This suggests the PCSS was successful in transmitting desired advanced PC knowledge and skills to students. The course directors targeted these content areas because they believe them to be foundational in PC practice and/or under-represented in the general medical school curriculum.
The results also suggest that PCSS participation influenced students' views of their professional development, particularly the non-clinical elements of their future practice. After participating in the PCSS, students were statistically more likely to report that their future career would involve advocacy and policy, QI, and taking on a leadership role compared to pre-PCSS. Students also reported a higher likelihood of incorporating teaching into their career post-PCSS, though this difference was not statistically significant, perhaps because so many students anticipated teaching being a part of their career pre-PCSS, leaving little room for increase. By highlighting the variety of ways that PC can be practiced and the many roles that PC physicians can adopt, the PCSS may have broadened students' view of what activities PC entails to include more advocacy, scholarly pursuits, and leadership.
Perhaps most impactfully, the PCSS data show that this type of curriculum can influence students' intent to pursue a PC career. The inclusion of data on students' intended career trajectories in this study is unique to other studies published on PC electives during the post-clerkship. Data show that 44% of students started the course with a strong intent to pursue PC and retained this interest, suggesting the course supported their existing PC commitment. The next largest category (19%) was the undecided students who started the course not yet sure they would pursue PC (Likert scale 3) and ended with a stronger commitment to PC (Likert scale 4 or 5). PCSS may help undecided students solidify their PC commitment through education and focused PC exposure. There was still a sizable proportion (17%), however, who began the course uncertain of their intent to pursue PC and remained uncertain (Likert scale 3), and a small percentage of students who indicated lower interest in PC pre- and post-PCSS. There were no students, however, who started the course ambivalent (Likert scale 3) and were dissuaded from PC by the end (Likert scale 1 or 2).
When students were asked about specialty choice, results showed a similar pattern. A majority of students were confident about their chosen specialty pre-PCSS and remained confident post-PCSS (53%). The next largest categories of students were those who were somewhat unsure of their intended specialty pre-PCSS (Likert scale 3) and either became surer (14%) or remained unsure (14%) post-PCSS. Again, these data suggest that the PCSS helped at least some students who were unsure about their specialty choice make a decision. Overall, among students who listed their intended specialty post-PCSS (n = 25), the largest category was FM (15 students), followed by IM (4), with fewer students (1 each) in Pediatrics, OB/GYN, Psychiatry, Med-Peds, Emergency Medicine, and General Surgery. Among students who were confident about their intended specialty, there were no students who changed their intended specialty from pre- to post-PCSS.
Challenges and Lessons Learned
The first iteration of the PCSS was overall successful, as evidenced by student survey responses demonstrating increased knowledge, improved career discernment, and high course satisfaction. However, the PCSS team also faced some challenges. Planning and implementing the PCSS required a great deal of time from two Family Medicine faculty and two support staff over the course of at least 6 months. In addition to the typical tasks of creating a syllabus, new lecture/workshop content, course assignments, and grading criteria, PCSS tasks that required the most time and/or advance planning included:
Identifying and scheduling guest speakers (approximately 57 total), who volunteered their time and often had to block their clinic or other responsibilities months in advance Identifying and coordinating community clinic preceptors (approximately 60 total), whose schedules were not always consistent from week to week, necessitating some students working with more than one preceptor Onboarding medical students to their assigned clinic, which had to happen at least one month in advance, in most cases Securing and training standardized patients Obtaining necessary supplies (models, medical equipment, etc) for workshops
An additional challenge was making decisions about what content to include in didactic sessions given the limited time and the broad scope of PC. Because of the amount of content course directors felt should be included, didactic days were long (often about 7-8 h of content 3 days per week), and though there was an emphasis on active discussion and workshops rather than lectures, some students commented in their feedback for the course that they felt tired and less engaged by the end of the day or end of the week. This feedback will be incorporated into future iterations of the PCSS.
For other schools seeking to implement a similar curriculum, the course directors wish to emphasize the importance of:
An administrative team and dedicated time for planning and implementation Contacting speakers and preceptors well in advance and confirming availability regularly Support from the medical school and/or a PC grant to finance workshop supplies and standardized patients Delivering the course ideally in February-April of the students' third year (post-clerkship) to maximize opportunity for career exploration prior to applying for residency
Limitations
One of the study limitations in determining the effect of the course on specialty choice is that students were only asked to specify their intended specialty if they were 90% or more sure. In the future, all students will be asked to provide a ranked list of their specialty choices pre- and post-PCSS. It may also be helpful in the future to ask students qualitatively about how their experiences in the PCSS affected their view of their future career. Another limitation is that all survey items relied on self-report. For content questions, students were not objectively assessed on these measures. Additionally, students reported their intended career path post-PCSS, but this cohort of students had not yet begun the residency application cycle, and those who apply in IM and Peds may still elect to specialize after residency training. Finally, we did not ask survey respondents to identify whether they were part of the PCP or not, which might have impacted their experience in the PCSS, and future surveys will address. Future studies should survey course participants during and after residency to better assess what type of medicine students ultimately practice and also include a larger sample size.
Conclusion
The study results examining the first cohort of PCSS participants show that students gained significant knowledge and skills through their participation in the course in areas foundational to the practice of PC, including communication, preventive medicine, chronic illness management, in-office procedures, QI, and leadership. Students who planned to pursue a career in PC pre-PCSS remained committed to PC post-PCSS, and many students who were undecided pre-PCSS expressed stronger interest in PC careers post-PCSS. Other medical schools seeking to enhance their post-clerkship PC training and encourage students to apply to PC residencies may consider using the PCSS curriculum as a template to design a similar course at their institution.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251335995 - Supplemental material for Primary Care Senior Seminar: An Advanced Skills, Leadership, and Career Training Model
Supplemental material, sj-docx-1-mde-10.1177_23821205251335995 for Primary Care Senior Seminar: An Advanced Skills, Leadership, and Career Training Model by Isabel Edge, Ilana Simon Greenberg and Jo Marie Reilly in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251335995 - Supplemental material for Primary Care Senior Seminar: An Advanced Skills, Leadership, and Career Training Model
Supplemental material, sj-docx-2-mde-10.1177_23821205251335995 for Primary Care Senior Seminar: An Advanced Skills, Leadership, and Career Training Model by Isabel Edge, Ilana Simon Greenberg and Jo Marie Reilly in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205251335995 - Supplemental material for Primary Care Senior Seminar: An Advanced Skills, Leadership, and Career Training Model
Supplemental material, sj-docx-3-mde-10.1177_23821205251335995 for Primary Care Senior Seminar: An Advanced Skills, Leadership, and Career Training Model by Isabel Edge, Ilana Simon Greenberg and Jo Marie Reilly in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
We would like to acknowledge Dr Matthew Sayre (KSOM FM chief resident at time of PCSS) who helped develop and deliver curriculum. We would also like to acknowledge Bryan Ayala-Rivera who assisted with coordinating and administering the PCSS. Finally, we'd like to acknowledge the preceptors and instructors who taught our students throughout the PCSS.
Ethical Considerations
The study was deemed exempt by USC's IRB (UP-20-01459).
Consent to Participate
Participants were provided with a study information sheet that described the purpose of the study and that participation was voluntary prior to completing the study. Per the USC IRB, because this was considered an exempt study, no written or verbal consent was required aside from including the information sheet prior to the start of the survey.
Author's Contributions
Isabel Edge and Jo Marie Reilly developed the Primary Care Senior Seminar course. Survey instrument was developed by all authors. Data analysis was conducted by Ilana Simon Greenberg. All authors contributed to the writing and editing of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.