
Abstract
OBJECTIVE
This literature review aims to explore research and conceptual pieces on the state of ophthalmology education and suggest potential ways to address current challenges.
METHODS
A search was conducted in PubMed, ERIC, Web of Science, and Google Scholar with combinations of the following search terms: “ophthalmology education,” “undergraduate medical education,” “medical student,” “United States,” and “Canada.” Eliminating irrelevant articles yielded 47 articles. Three were excluded because of region and focus, leaving 44. After examining the citations, we generated an additional 22 texts for review, totaling 66 articles.
RESULTS
Four primary themes were identified: (1) challenges to ophthalmological education in the U.S. and Canada, (2) potential remedies for optimizing ophthalmology curriculum, (3) technology in ophthalmology education, and (4) innovative ophthalmology teaching approaches. Major challenges included the lack of a standardized curriculum and inadequate clinical exposure and skills training. A number of remedies were proposed, such as standardizing curriculum and furthering faculty involvement, utilizing technology as time-effective learning aids, and employing innovative teaching approaches such as service learning.
CONCLUSION
In light of challenges in ophthalmology education, curriculum designers should consider Cognitive Load Theory (CLT) to assist students to remember meaningful exposures to ophthalmology knowledge and techniques. Based on CLT, we suggest two potential approaches to incorporating ophthalmology curriculum. The first is to embrace interdisciplinary collaborations and place ophthalmology knowledge in varied contexts to facilitate schema construction. The second is to incorporate ophthalmology diagnostics requirements into OSCEs and utilize simulation models for students to gradually increase the fidelity of tasks and devote cognitive resources fully to learning.
Keywords
Introduction
As the U.S. and Canadian population ages, demand for visual care will significantly rise in the next few decades.1,2 Consequently, it has become increasingly imperative that primary care physicians possess the basic skills to distinguish emergent eye findings from those that are chronic or benign. Major eye diseases that contribute to low vision and blindness such as cataract, glaucoma, and age-related macular degeneration increase in frequency with age. 3 This is especially crucial for generalists who practice away from large academic centers in underserved communities with limited resources and inadequate access to readily available ophthalmology consultation. Nevertheless, there has been a continuous decline in ophthalmology education in medical school curriculum in the U.S. and Canada. 4 Due to the rapid expansion of scientific information, Medical schools have increasingly focused on the core areas of medical education, rather than smaller specialties like ophthalmology. 5 Furthermore, because the Liaison Committee on Medical Education does not specifically require ophthalmological training, the number of ophthalmology rotations and courses continued to dwindle in medical institutions across U.S. and Canada. 5
Research shows that lack of a standard ophthalmology curriculum and clinical rotations has resulted in a negative impact on the basic ophthalmological skills of medical students and graduates. It was found that 70% of medical school graduates could not use an ophthalmoscope correctly, and most primary care residents in their study did not meet the ophthalmological skill standards set by the Association of University Professors of Ophthalmology (AUPO). 5 Without basic ophthalmology evaluation skills, primary care physicians are unable to effectively discern chronic stable eye diseases from those that require immediate attention, possibly resulting in permanent damage and blindness that could otherwise be avoided while patients wait for specialist care. Potential remedies of ophthalmology curriculum should be explored to address these issues and improve ophthalmology education for medical trainees.
This scoping review explores the major research and conceptual pieces on the state of ophthalmology education in the U.S. and Canada to investigate potential ways to address current challenges in existing ophthalmology curriculum and better prioritize ophthalmology curriculum time in medical school curricula. Ophthalmology education encompasses a wide range of topics that are strongly applicable to other parts of medical education, including practical skills training, acquisition of scientific knowledge, clinical reasoning, decision making, as well as cultivation of empathy and interpersonal skills. Insights gained through this study will not only contribute to ophthalmology education but could also be extended to improve curriculum development in other areas of medical, health, and nursing education. Furthermore, this study provides a framework for curriculum development in areas beyond medicine to address gaps that require flexible solutions with a tight timeframe.
This study will begin with an overview of the methodology used. The next section will provide a discussion of the overarching themes found, followed by a comprehensive critique of current research. We frame our discussion of the literature through the lens of cognitive load theory (CLT), taking into account students’ cognitive architecture when devising recommendations for integrating ophthalmological learning tasks and activities into an already dense general curriculum. 4 Finally, the conclusion will provide a summary of the main themes identified and recommendations for practice.
Methods
We limit our study to the U.S. and Canada, where undergraduate medical education is completed after achieving a bachelor's degree and following a similar curriculum. The literature search was conducted on PubMed, ERIC, Web of Science, and Google Scholar, with various combinations of the following search terms: “ophthalmology education,” “undergraduate medical education,” “medical student,” “United States,” and “Canada,” including all articles from 2005 to 2021. The most recent search date was July 9, 2022. Two hundred and ten articles were generated from the search and screened for relevance to undergraduate ophthalmology education. Forty-seven articles passed the screening and were further reviewed; 3 of which are excluded because of region and focus, leaving 44 remaining articles. To cover articles not labeled by search terms, we have also examined citations of the above articles, which generated 22 extra texts, totaling 66 articles. See Figure 1 for the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram and Table 1 for literature details.
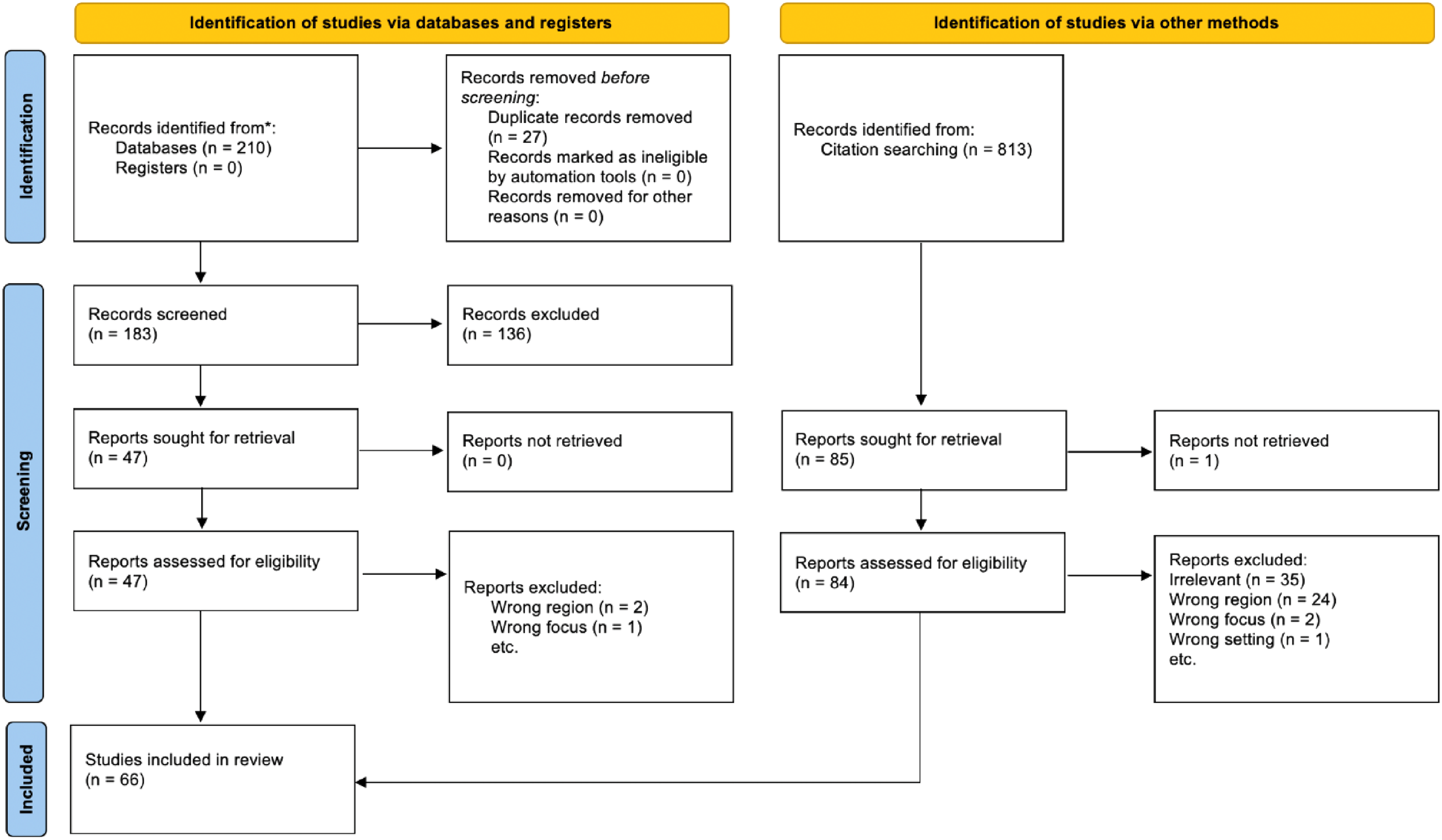
Prisma diagram.
The literature.

QN = quant; QL = qual; Mixed = mixed methods.
Statistical analysis
Data from most articles were collected from surveys, but some also included program information from institutional websites, test scores, and patient data. Use of data was varied based on the type of research. For quantitative studies and the quantitative part of mixed method studies, authors primarily used statistical analyses such as paired t-test and ANOVA. The qualitative data of mixed method studies consisted of collected written feedback from participating students, faculties, and focus group discussion records.
Results
We identified four primary themes: (1) Challenges to ophthalmological education around the world, (2) Standardizing curriculum with more faculty involvement in medical school administration, (3) Utilizing technology in ophthalmology education, and (4) Innovative ophthalmology teaching approaches. The first theme outlined challenges and issues with current educational practices and the last three focused on proposed remedies to those challenges.
Challenges to ophthalmology education
Many studies evaluated the state of ophthalmological education and raised challenges with regard to the lack of standardization in ophthalmology curriculum. Shah et al 4 pointed out that the Liaison Committee on Medical Education, the organization responsible for creating guidelines for curriculum and accrediting medical schools, has no guidelines with respect to ophthalmology education. While the International Council of Ophthalmology (ICO) has recommended ophthalmology guidelines, they are not mandatory and thus not typically followed by medical schools. It was found that only 20% of Canadian medical schools have core curricula that follow the ICO guideline. 15
The lack of a standardized core curriculum may have caused current ophthalmology curricula content and length to vary across institutions, since ophthalmology curriculum is left entirely to the institutions without mandatory guidelines. Moxon et al 17 surveyed U.S. and Canadian institutions and found that while 94.7% of medical institutions include some form of ophthalmology exposure, the content varies institution by institution, with 78.9% requiring preclinical coursework only, 13.7% requiring both preclinical and clinical coursework, and 7.4% offered clinical exposure only. Chan et al 13 also investigated the adequacy of medical school ophthalmology teaching and stated that there was a wide variation between ophthalmology instruction time in different institutions in Canada. Ophthalmology curricula seem to remain inconsistent across the U.S. and Canada, which poses a significant challenge to ophthalmology education.
Furthermore, ophthalmological clinical exposure and skills training has been reported to be inadequate in multiple studies.4,6,10,15–17 Shah et al 4 surveyed U.S. and Canadian medical institutions in 2012–2013 and found that only 18% of institutions had required clinical exposure to ophthalmology, a drastic decline from 68% of institutions in 2000. In 2018, the percentage of U.S. and Canadian schools requiring an ophthalmology clinical rotation has further declined to 16%. In addition, 20% of medical schools do not require any exposure to ophthalmology skills training unless sought by individual students. As a result, 70% of medical school graduates do not know how to use an ophthalmoscope properly, and primary care residency program directors reported that most of their residents do not meet AUPO standards. 17 In addition, Esparaz et al 10 discovered that students not only had a substantial gap in ophthalmology clinical knowledge, but they also performed particularly inadequately on managing ocular conditions compared to diagnosing. The lack of management skills and ability to recognize when to perform a referral to an ophthalmologist significantly impacts the quality of care delivered to primary care patients. Overall, these studies reveal a pervasive lack of clinical rotations and skills training dedicated to ophthalmology, contributing to the lack of practical ophthalmology skills for primary care residents.
Remedies to challenges
While all these articles recognized the problem of a lack of ophthalmological training during medical school, most focused on possible remedies. These studies fell into three camps: standardization of curriculum and more faculty involvement, utilization of technology, and innovative teaching methods.
Standardization of curriculum and involvement of faculty administrators
One remedy suggested by multiple sources4,10,15,18 is to standardize the ophthalmology curriculum by adhering to existing guidelines and establishing a baseline for curriculum duration and clinical components. Shah et al 4 emphasizes further standardization of ophthalmology curriculum in medical school by integrating previous attempts like the AUPO standardization of core competencies, 14 and the ICO guidelines for required training. 67 Gostimir et al 15 also recommended greater adherence to the ICO guidelines. They pointed out that the ICO strongly recommends using teaching methods including didactic lectures with clinical demonstration, and that clinical exposures and operating room experiences should be mandatory. Having conducted a longitudinal study of student acquisition and retention of ophthalmic knowledge, Lippa et al 68 discovered that current skills training in the second year is not sufficient for students to retain and apply ophthalmic examination skills unless it is supplemented with the ophthalmology clerkship. They also suggested that medical schools should incorporate more ophthalmology skills training throughout the four-year curricula to ensure competency for graduates. While Moxon et al 69 did not directly advise an increase in curriculum time, they also questioned whether the current number of ophthalmology hours and clinical exposure in medical school are sufficient to produce core competencies.
In addition to standardizing requirements to include all core competencies, some research suggests that ophthalmology faculty should be encouraged to become more involved in administration and to establish ties between the ophthalmology department and other departments as well as general medical education. Shah et al 4 pointed out that ophthalmology departments tend to disengage themselves from medical student education and suggested increasing ophthalmology faculty participation in administrative roles may result in increased influence and awareness of the importance of ophthalmology training. Moxon et al 17 suggested appointing a dedicated Director of Medical Student Education (DMSE) position for ophthalmology departments. They argued that institutions with a DMSE offer more clinical coursework (11.9 h vs 10.8 h) and have higher rates of faculty engagement. Gostimir et al 15 recommended more evidence-based teaching that pairs ophthalmology education with other related fields. They suggested that a closer connection with medical school administration and educational practice will increase the influence of ophthalmology and likely lead to increased attention and curriculum time.
Utilizing technology in ophthalmology education
Multimedia technologies can be leveraged to improve students’ knowledge acquisition and self-regulated learning experiences in ophthalmology. Allen et al 30 made use of cognitive load theory to develop a virtual interactive three-dimensional eye model, aiming to reduce cognitive load for learners and improve their learning of ocular anatomy. Steedman et al 31 designed and evaluated multimedia tools in the form of presentations consisting of audio, video, text, and visual images. The authors noted that students assigned to multimedia tools received higher scores on questionnaires and spent 72% less time reviewing the educational content compared to those reading a textbook excerpt of the same content. Furthermore, prerecorded mini-lectures have become a new trend and a part of student-centered educational approaches. Research has shown that this method of dividing information into “bite-sized” materials is beneficial for students. 70 Multiple studies utilized short, prerecorded videos in their ophthalmology teaching approaches and received higher student satisfaction, sense of involvement, and preference over traditional lecture format of teaching.55,63
The development of multimedia gave rise to virtual ophthalmology courses, which became even more essential and widespread during the COVID-19 pandemic. Lee et al surveyed all Directors of Medical Student Educations (DMSEs) of AUPO and found that while 44% of the institutions had no online component in their courses prior to the COVID-19 pandemic, the majority (78.3%) of the institutions have increased their online components in response to the pandemic. 8 Previous in-person clinical courses are successfully transitioned into virtual courses, and extracurricular activities into online formats, allowing students increased flexibility and easier access to materials. 8 Studies have found that virtual courses effectively enhanced student knowledge and interest in ophthalmology.37,38 In particular, Abou-Hanna et al 37 compared the performance of medical students enrolled only in an online course with those enrolled in the same online course and an additional clinical component. They found that the online group scored only slightly inferior in the ophthalmology knowledge test compared to the combined online and clinical group, and suggested that online courses may provide a sufficient knowledge base and exposure to those not intending to specialize in ophthalmology. In addition, He et al found that virtual learning can mitigate inequality in medical education and promote inclusion. 39 Even after the lift of the COVID-19 onsite restrictions, the online courses and resources developed will continue to transform medical education and provide increased accessibility and value to medical students.
Ophthalmoscopy training is another area in which diverse forms of technology are often leveraged to improve student learning. Ocular fundus imaging technology has been promising in improving medical students’ visualization of the ocular fundus and providing a method for instructors to objectively evaluate ophthalmoscopy training. Kelly et al 41 conducted a study in which medical students learned to examine the ocular fundus through direct ophthalmoscopy and fundus photographs. They discovered that students preferred fundus photographs and were also significantly more accurate in identifying fundus features through photographs than ophthalmoscope. One year after the previous study, students still performed better using fundus photographs compared to direct ophthalmoscopy. 40 Furthermore, in scenarios in which ophthalmoscopy is required, instructors usually have difficulty determining how accurate a student visualizes the fundus. Afshar et al 33 suggested that fundus photos provide an objective way to assess a student's ability with ophthalmoscopy. They recruited volunteer patients, took photographs of their optic nerve in one eye, and then had medical students examine each patient with ophthalmoscope and match the respective volunteer with their optic nerve photo. Evidence such as the improvement of students in identifying the correct photo through training and the superior performance of ophthalmology residents and fellows supports the validity of the method. 33 As such, fundus imaging techniques have provided new insights into the visualization of ocular fundus and ophthalmoscopy evaluation, and can be further leveraged through software applications to improve learning. 36
Other tools such as smartphone ophthalmoscopy and ophthalmoscopy simulators also benefit ophthalmoscopy skill acquisition. Recently, many smartphone ophthalmoscopes have been developed, which capture ocular fundus images using a smartphone camera and an adaptor. 29 Kim et al 29 discovered that students were able to visualize the optic nerve better with the smartphone ophthalmoscope compared to the direct ophthalmoscope, and students also reported a more positive experience and higher confidence using the smartphone ophthalmoscope. They suggested that smartphone ophthalmoscopy can be a supplement or an alternative to current ophthalmoscopy teaching. Many studies have also utilized the Eyesi virtual reality simulator to assist student learning.25,26,28 A study by Tso et al discovered that students are generally more comfortable and confident in performing direct ophthalmoscopy on a patient following an Eyesi simulator session compared to traditional teaching session. 28 In addition, the Eyesi simulator is also found to be able to accurately evaluate and differentiate skill levels in ophthalmoscopy. 71 Integrating these technologies into direct ophthalmoscopy learning will provide valuable tools for student skill acquisition and evaluation.
Innovative ophthalmology teaching
Approaches to innovative ophthalmology teaching include new methods such as the flipped classroom, service learning, and art observation. The flipped classroom is a learner-centered educational paradigm that promotes active learning at the learner's own pace. 72 Instead of giving lectures in class and having students complete assignments after class, the flipped classroom technique ask students to study prerecorded lecture videos or other materials ahead of time, and then enter the classroom for discussions, small group exercises, and projects, thus flipping the classroom. 72 Upon comparing the traditional classroom experience with the flipped classroom experience, Diel et al 55 discovered that students found the flipped classroom teaching session more valuable, experienced increased interactions with faculty, and sensed a higher level of inclusion as a part of the team. It was also noted that most students enjoyed the flipped classroom experience more than traditional lectures and expressed interest in continuing to receive instructions in this approach. 63 In some cases, the learner also spent less time in the flipped classroom lectures compared to the traditional classroom approach, while the knowledge assessment performance remains comparable to traditional lectures. 63 In the future, the flipped classroom can be further leveraged to promote more active engagement and higher student satisfaction in ophthalmology learning.
Service learning is a rapidly growing area that not only allows students to practice clinical skills, but also cultivates emotional competency through exposure to diverse patient populations and encouragement of systems thinking, as well as providing much-needed service for the underserved. In 2018, there are 23 student-run health clinics offering ophthalmology service over the United States, with each one providing 5.15 h per month of services on average. 60 Many studies investigated demographics of the patient population and efficacy of the service clinic model on skills acquisition.1,44,51 MacLean and Hindman 1 conducted research on the University of Rochester Well Eye Care service project and found that patients served by participating students came from diverse backgrounds, including undocumented immigrants and individuals exempted from filing federal tax returns due to low income. Another example is a study by Williams et al 51 who studied a service program at the Guerrilla Eye Service at the University of Pittsburgh. They noted that students provided referrals to a university clinic for patients with advanced disease so that they can receive free longitudinal care there. Similarly, Byrd et al 44 developed a community vision project that recruited second year medical students from the University of New Mexico to serve in the mobile clinic in Albuquerque and rural areas of the state of New Mexico. After a month, the students’ knowledge was compared with that of peers and internal medicine residents. They found that participants’ median knowledge assessment scores were 48% higher than their classmates and 37% higher than those of internal medicine residents, suggesting that service learning is an efficient model for incorporating ophthalmic training in medical curriculum.
Emphasizing the importance of observation in ophthalmology examinations, Gurwin et al 45 conducted a randomized control study of art observation training on improving medical student ophthalmology skills. They randomized 36 students into 1:1 art training and control groups. Students in the training group received instructions from professional art educators during six 1.5 h art observation sessions over a three month period. All students completed pre- and post-testing in which they described a work of art, retinal pathology images, and photos of eye diseases. They found that observational skills measured by descriptive training significantly increased in the training group compared to the control group and suggested art observation may improve clinical observational abilities. Such innovative projects allow medical students to develop observational skills beneficial to ophthalmology skills acquisition while exposing them to educative experiences not usually offered in traditional settings.
Discussion
This review highlighted the lack of ophthalmology exposure and curriculum standardization in medical school and analyzed promising efforts in improving ophthalmology education. In this age of rapidly expanding knowledge and increasingly crowded medical curricula, medical students are often overburdened with information. Given the limited amount of time of medical school and continuous advances in medicine, it is difficult to incorporate every field comprehensively in the medical curriculum. Future incorporations of ophthalmology instruction and practice should base instructional strategies upon the learner's cognitive capacity, and thus consider the integration of cognitive learning theory into curriculum design.
The cognitive learning theory (CLT) is a theory aimed to develop instructional design strategies based on human cognitive architecture. 69 CLT assumes that the human cognitive system has a limited working memory and unlimited long-term memory composed of cognitive schemas. According to Cramer et al, 73 “intrinsic cognitive load describes the inherent complexity of the information being taught, whereas extraneous cognitive load describes excessive instructional convolution, which distracts from the learning goals.” The ideal is reached with germane cognitive load. Germane load refers to the ideal amount of instruction and task complexity for promoting learning. As learners mindfully combine simple ideas into complex schemas in long-term memory, they develop expertise. CLT holds that the human cognitive system has a limited working memory that can only hold 5–9 elements and actively process 2–4 elements simultaneously. 69 However, medical students often encounter complicated learning situations involving multiple elements of complex information and are often overloaded on information and unable to process that information into long-term memory. 74 Consideration for the realities of cognitive load placed on learners when designing ways to add ophthalmology training to expansive medical education content could be accomplished by using approaches such as the competency-based curriculum 39 and scaffolding instruction. 73
Out of all the articles on curriculum, only Allen et al 30 and Steedman et al 31 utilized principles of cognitive load theory for curriculum design. Allen et al 30 implemented a 3D eye model and interactive learning modules, designed to use both the learner's auditory and visual channels through visual modeling and voice narration to reduce cognitive overload. Secondly, they removed extraneous details from materials and information within the modules was divided into small chunks to limit the burden placed on working memory. Thirdly, students can hover their mouse over the anatomical subcomponents in the software and see visible labels, utilizing the special contiguity effect by keeping labels close to visual representations of these components. Finally, they incorporated a personal and welcoming narrative voice, intending to create a “personalization effect” that has been shown to improve learning. Steedman et al 31 designed a multi-media learning tool (MMLT) for teaching ophthalmological contents and evaluating its effectiveness. They have developed the MMLT format based on CLT studies that found students retain more information when topics are presented in multiple channels. Both articles utilized tenets of CLT to better optimize the working memory of medical students when learning about ophthalmology.
Based on what we learned through this review and careful considerations of CLT, we suggest two potential remedies to incorporate ophthalmology time-efficiently into the medical school curriculum. The first is to embrace interdisciplinary collaboration between ophthalmology and other specialties such as neurology, dermatology, and ENT. By holding classes together with these specialties on overlapping topics and skillsets, repetition can be avoided and instruction time saved without compromising content. Furthermore, collaborating with other disciplines allows students to put ophthalmology skills in varied medical settings and assists the formation of schemas in long-term memory. Instead of memorizing ophthalmological concepts separately, students can learn about how an eye disease manifests in the context of other specialties, thus constructing their understanding of ophthalmological concepts under the larger framework of medical education.
A second approach is to incorporate ophthalmology diagnostics requirements into objective structured clinical examinations (OSCEs). While most students know the relation between certain conditions and systemic illnesses, physical diagnostics skills competencies are rarely enforced. Utilizing a formal simulation machine or simple creative simulation models such as those proposed by Kylstra and Diaz 75 in OSCE allows students to demonstrate ophthalmological skills and visualize conditions. In the context of CLT, learning tasks should start from a low-fidelity (decreased element interaction) environment and gradually increase to a high-fidelity environment. 76 By having students start from reading textual explanations, moving on to simulation, and finally to conducting diagnostics on real patients, the fidelity of the tasks is gradually increased and intrinsic load is reduced, freeing up resources to be solely devoted to learning. Gaming technology can also be leveraged to create simulation applications for medical students and assist their visualization, while allowing a limited degree of autonomy in exploring ophthalmological conditions. Utilizing teaching tools such as simulation software and gaming technology, combined with mandatory hands-on examinations on real patients can help students to retain knowledge and improve learning.
With the ever-increasing amount of information medical students are required to consume, CLT should always be a consideration when designing or updating medical school curricula. Careful curriculum design incorporating CLT, combined with learning technologies and innovative teaching approaches such as service-learning, will enable students to learn, process, and remember meaningful exposures to ophthalmological information and techniques. In the future, it will be increasingly important to strive for germane load in curriculum design and continue to seek creative ways of teaching that enable future physicians to achieve their ophthalmology competencies.
While this scoping review explored a variety of research in diverse topics, there are some inherent limitations in the types of articles available and survey questions used in these studies, leading to challenges in accurately assessing the quality of current ophthalmology education and devising effective strategies.
Firstly, almost all of the studies examined are quantitative except for some mixed-method studies, which also tended to focus on the quantitative aspects. While they provide important information about ophthalmology education through Likert-scaled surveys and data analysis on test scores, qualitative studies about ophthalmology curriculum and extracurricular activities are needed to provide insight about the students’ and educators’ points of view. A lot of questions about the transition from content-based to competency-based curriculum remain unanswered, such as whether students feel that the competency-based curriculum prepared them better for residency, or whether they encountered any major setbacks with the curriculum. Educators’ experiences and what they consider to be important would also be helpful for future educators as the competency-based curriculum continues to expand. Service-based learning is another topic area with great potential for qualitative research. It would be interesting to explore what students felt they learned from service-learning projects in order to understand their experience from a holistic perspective. While the focus on quantitative studies is understandable since ophthalmology is a relatively technical specialty, qualitative aspects of ophthalmology education should also be addressed for students and educators to have enhanced experiences in the future.
In addition, most of the surveys cited consisted of close-ended questions such as Likert scaled or yes/no questions, which can lead to different interpretations of the questions from what the researchers originally intended and do not allow participants to clarify their answers. A combination of close-ended and open-ended questions would provide more insight on the thought process of the person answering the survey.
Conclusion
This review highlighted the inadequacies of ophthalmology education in the medical school curricula, including the lack of standardization of ophthalmology curriculum and insufficient clinical exposure and skills training. It also reviewed promising efforts to improve undergraduate ophthalmology education, such as standardizing curriculum and encouraging faculty involvement, utilizing technology to improve student learning, and employing innovative teaching techniques. Based on the tenets of Cognitive Load Theory, we have suggested two additional approaches to improve ophthalmic learning, including interdisciplinary collaboration with related specialties to reduce instruction time, and incorporating ophthalmological diagnostics requirements into clinical examinations and utilizing simulation technology to practice for these exams. We hope that the integration of CLT in curriculum design can inspire innovative teaching approaches and further improve physician capabilities in ophthalmology.
Footnotes
Acknowledgment
All authors have no conflict of interest with regard to this review.
Authors’ Contribution
JL conceived design of project, conducted research, and wrote manuscript. RRW conceived design and wrote manuscript. RRW and GKV revised manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.