
Abstract
There are multiple complexities within the practice of medicine wherein the vantage of the medical community might be limited or in direct conflict with the vantage of a patient population. Reproductive justice (RJ) is a framework developed from the vantage of Black women's health activists to identify and address inequitable reproductive health outcomes, consider the intersection of reproductive rights and social justice, and center the experiences of historically marginalized communities. Using the contemporary example of the federal Medicaid Sterilization Form, we highlight how the pedagogy of classroom debate can teach medical students to engage thoughtfully with the complex intersection between community population perspectives and the medical profession's advocacy for standardized provision of health services. Debate has long-standing use in education and can build core medical student communication and professionalism competencies while facilitating active learning around complex medical care topics. However, it can have limited efficacy without careful attention to the development of a psychologically safe learning environment and the inclusion of nuanced and diverse perspectives. Herein, we share our debate curriculum and demonstrate how this approach aligns with the community-developed RJ framework that recognizes systems outside medicine that contribute to reproductive outcomes. Our method encourages students to critically evaluate existing literature for authorship, representation, and community participation—a crucial practice for all students to understand the importance of equity in medical research development and healthcare.
Keywords
Introduction
All medical learners will care for patients deeply affected by inequitable—disparate and unjust—health opportunities and outcomes. This is particularly true when rotating within reproductive health. Maternity care deserts, highly variable state regulations and restrictions, and structural racism all contribute to Black U.S. women suffering from three times greater risk of death in childbirth than White women at all levels of income and education. 1 More than half of these deaths are preventable. 1 Black women also have higher rates of severe maternal morbidity and cervical cancer and lower rates of sexually transmitted infection detection and treatment and human papillomavirus vaccination.2–5
These disparities in U.S. reproductive health outcomes, despite long-standing recognition, are worsening.6–8 Likely, we have been unable to make headway in these disparate health outcomes in part because of the narrow view through which the medical profession views the problem. Medical research, clinical policies, and educational curricula are largely developed by medical and scientific professionals who carry power, privilege, and positionality that limit the vantage through which they investigate, understand, and teach healthcare disparities. Apart from the small discipline of community-based participatory research (CBPR), members of involved populations are rarely included in helping medical professionals understand contributors to health disparities. Modern medical education largely relies on the scientific literature developed for and by medical and scientific professionals. Therefore, the perspectives and understanding of affected community members rarely make their way to learners unless we deliberately seek out these community voices when developing curricula. 9
Reproductive justice (RJ) is a framework developed by Black women's health activists in 1994 to identify and address inequitable reproductive health outcomes by considering the intersection of reproductive health, reproductive rights, and social justice. Critically, RJ relies on centering the experiences of people with marginalized identities. 10 “Nothing about us, without us” is a key tenet of RJ, indicating programmatic development requires inclusion of community members of the population of interest. 9 Furthermore it draws on influences outside the medical system—such as laws, policies, education, economic opportunities, safety, housing, and food security—that affect reproductive health access and outcomes. Within the United States, these influences vary along identity axes of race, gender, sexual orientation, and disability. Therefore, RJ serves as an excellent example framework for medical learners. It allows them to contextualize marginalized perspectives and examine how health disparities and structural racism shape medical practice and clinical outcomes.
Given the differing, and sometimes conflicting, perspectives between medical professionals and community members, we believe debate provides a unique opportunity to highlight this interaction in the medical classroom. A well-developed debate curriculum can effectively elevate patient community voices in student learning. In this report, we describe a novel application of classroom debate as an educational method to ground a contemporary RJ example, engage students in complex critical thinking, and accentuate the value of the voices of an affected community.
Debate as a Pedagogical Method in Medical Education
Debate is a well-established pedagogical method used for centuries in education. It has ancient origins, dating back to Ancient Greece where Protagoras of Abdera, often called the “father of debate,” first introduced the concept in an educational setting.11–13 It has been employed in medical education in recent decades to help learners engage with complex and controversial clinical scenarios and ethical dilemmas.12,14 Classroom debate is a form of experiential learning where students, through critical analysis and selection of evidence, provide support for an assigned “side” of an issue. 11 Classically, these “sides” are designated as “for” or “against” a particular viewpoint or assertion. However, there can be flexibility in the format used for debate. Debates can involve three or more “sides,” role-play, think-pair-share, and group problem-solving formats, among others. 13
Critics of debate cite concerns about an excessive workload in preparation for debate, a potential for biasing learners toward a black-and-white dualistic mindset, a reinforcement of students’ existing beliefs instead of challenging them to consider nuanced viewpoints, and the development of a confrontational classroom environment that may affect psychological safety.12,13 However, with careful consideration of the preparation time, the classroom culture that is cultivated, and the engagement of the medical learner, debate can be incredibly effective and formative for trainees,15,16 with a resulting resurgence of this pedagogy noted in contemporary undergraduate medical education. 14
When crafted and facilitated well by faculty, classroom debate is a highly effective learning modality that promotes evidence-based investigation, content reinforcement, team communication, public speaking, active listening, critical thinking, learner self-evaluation, as well as affective engagement with the debated topic.12,14,16–18 Debate offers an opportunity to explore a complex topic without resorting to oversimplification or generalization. It has been shown to support adult learning by making students responsible for their learning through active engagement in a problem-centered, experiential approach. 14 These outcomes have also been consistently expressed and appreciated in studies of student perceptions. Students tend to view classroom debate positively and appreciate the development of teamwork skills, confidence, respect for other viewpoints, and a deeper understanding of the debated topic.14,18,19
Overall, classroom debate has significant potential to enrich the learning experience of medical students when designed with careful attention to student workload, nuanced viewpoints, and the laying of respectful classroom ground rules. Moreover, we have found this pedagogical approach can be used to highlight and eliminate gaps in traditional medical education where marginalized patient community voices are missing. Our proposed methodology for a RJ-centered classroom debate aims to build from existing advantages of the debate approach while deliberately creating space for medical trainees to learn, understand, and advocate for the historically marginalized voices previously absent from the medical curriculum.
Our Model for a Reproductive Justice Debate
The conflict
We developed a debate surrounding the Federal Medicaid Title XIX Sterilization Consent Form (MSF). The MSF was developed and mandated by Congress in 1976 in response to widespread coercive and involuntary sterilization practices throughout the United States. With few exceptions, the MSF must be signed by publicly insured patients with their doctors 30 days before any female or male sterilization procedure. 20 On one hand, the MSF works as intended: to insert delay and increase the interactions with the healthcare system needed to ensure a sterilization procedure is being undertaken voluntarily and without coercion. Any person on publicly funded insurance has this requirement, affecting hundreds of thousands of economically disenfranchised people each year. 21 Because of this extra layering of protection for patients that hold a great deal of medical skepticism, the RJ community often advocates for the importance and continued use of the MSF protection against the risk of contemporary involuntary sterilizations. 20
On the other hand, the perspective of those from within the medical community is that the MSF creates barriers to timely sterilization and differences in care by insurance status; a patient with private insurance can receive permanent sterilization when desired without delay. In a recent cohort study using the nationally representative 2013 to 2015 National Survey for Family Growth, people with Medicaid were 56% less likely to complete sterilization than those with private insurance. 21 The medical scientific literature, developed almost exclusively by healthcare professionals, has demonstrated concerns regarding the MSF's contribution to high rates of unfilled sterilization requests, lack of improved consent due to poor MSF readability, and limited sterilization access for immigrants and patients under age 21. 20 These two perspectives generate a tension involving long-standing medical mistrust, medical paternalism, and good medical intentions to eliminate healthcare disparities and honor patient autonomy.
The learners
Advanced undergraduate medical students enrolled in a four-week selective course dedicated to sex- and gender-informed medicine, were assigned a position to argue. To avoid the two-sided, black-and-white perspective argued by critics of debate, we organized students into three groups. Group A argued for repeal of the MSF and waiting period, Group B argued against repeal, and Group C recommended a policy replacement that considers protections for vulnerable communities while minimizing over-regulation and disparities in access and health care delivery. Groups, with about 8 students, were provided with position statements and relevant literature to support their position as a starting point for further research (Supplement). Students were asked to note the literature's authorship and the identities of the primary voices supporting their position. To date, we have run this activity with four class cohorts of up to 25 students each.
The intervention
Students were alerted to the debate requirements, the guiding materials (Supplement), and the random group assignments on the first day of the course in a course orientation, giving them close to four weeks to prepare. Student groups met individually over the month to brainstorm their approach, read the relevant literature, and plan their presentations. On the day of the debate, faculty provided an introduction, and each group had 10 minutes to present their argument, with 5 minutes of questions from students in other groups or faculty. Group C heard arguments from both sides and often incorporated new supporting content into their previously developed consensus-building solutions. At the time of the presentation, an entire group stood before the class and worked collaboratively, with each student leading one portion of their group's position. Students had flexibility in presentation style; most used visual aids, case stories of affected individuals, and literature, both scientific and community-developed, to help argue their position. The class discussion concluded with a large group debrief on the positions as a whole, highlighting challenges students encountered researching and arguing their positions, the author voices of the literature they relied on, and questions generated by the debate. The faculty asked questions to the individual groups, and the class as a whole, to help highlight the limitations in the students’ stance in the argument in a supportive and encouraging way.
Students often resort to a position of compromise to resolve the weaknesses of their assigned position's arguments. By assigning a separate group, students in Groups A and B were required to think about the strengths of their position's arguments independently. Group C provided a logical conclusion to the debate by identifying areas of compromise, unification, and improvement surrounding sterilization regulation. They addressed the complexity and nuance of the MSF issue as a whole, considering the feasibility of an improved policy that would protect vulnerable patients while also not setting their healthcare apart as different from those with private insurance.
RJ Debate Aligns with Key Medical Student Learning Objectives
In a curriculum development study, a panel of varied RJ experts determined through the Delphi method that a RJ-specific medical curriculum should address 11 domains: (a) historical injustices, (b) RJ definitions, (c) oppression, power and bias training, (d) contemporary law and policy, (e) healthcare access, disparities, and structural competency, (f) cultural safety, (g) LGBTQI health, (h) reproductive health, (i) patient care, (j) approaches to reproductive healthcare, and (k) advocacy training. 9 The alignment of RJ learning domains relevant to the debate, with the Accreditation Council for Graduate Medical Education (ACGME) core educational competencies for medical students is shown in Table 1. 9
Alignment of debate-relevant reproductive justice learning domains and ACGME core competencies and reproductive justice debate (adapted from Loder et al 2019). 9
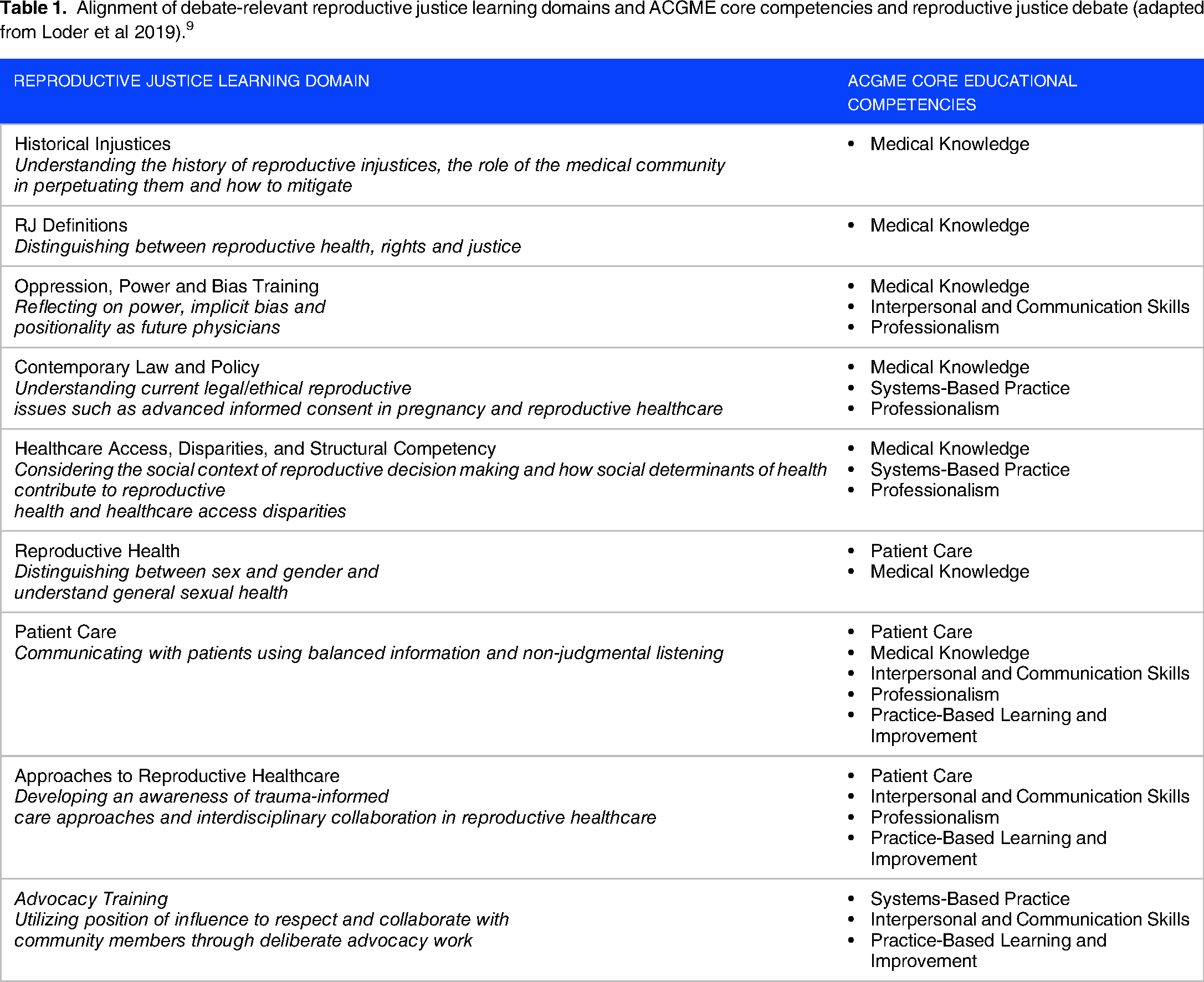
Our debate format aligns closely with these RJ curriculum learning objectives. 9 In the context of the MSF, students were able to consider historical injustices to patients of color and debate the merits of a contemporary policy. In preparation for the debate, they learned how the MSF affects access to safe sterilization and can create disparities in reproductive health outcomes along axes of identity. Through the process of debate itself, they learned how to present evidence supporting their viewpoint and amplify the perspectives of the communities they represented—a crucial skill for advocacy work.
The debate format itself allows students to practice skills likely transferable to the ACGME core competencies of interpersonal and communication skills, professionalism, systems-based practice, and practice-based learning and improvement. 9 We anticipate students can also use these skills to critically evaluate other health disparities that require a dualistic lens from both the medical community and the patient population perspective.
Conclusion
Today, within the United States, the practice of medicine is impacted by geographic, political, and regulatory contexts. While reproductive health provision and education serve as important examples, especially after the fall of Roe v. Wade, the debate approach could apply to other complex and disparity-driven topics in medicine, including religious exemptions, medical ethics, and the use of artificial intelligence in healthcare.
The debate format allowed flexibility for sharing clinical cases and discussion reaching a depth appropriate to the students’ experience level. When presented with a contentious topic, students may favor one dominant perspective—either because it is the current practice, supported by field experts, or aligns with the ideological viewpoints of their mentors, course directors, and learning environment. This can lead to anchoring and bias in students’ understanding that would go unchecked without a teaching format encouraging them to interrogate multiple viewpoints.
We encourage medical educators to utilize debate in curriculum planning, especially for nuanced, complex medical care delivery. It will be important to incorporate space for student reflection on the experience of arguing positions they may disagree with and the impact of their varied lived experiences, both of which are important for the professional growth and learning process, especially in values-based medical decision making. We recognize that productive debate only occurs when students feel psychologically safe and adequately prepared to discuss these often emotionally valenced topics. Future application of debate strategies must be coupled with establishing classroom norms to foster these safe spaces, as well as formal impact evaluation of student learning.
Medical students frequently engage with scholarly literature as part of their learning and are rarely provided with or seek out community-based writing outside of the peer-reviewed literature. The practice of examining the authorship and viewpoints represented in this research and writing applies to every domain of their training and will help students both recognize and advocate for the communities whose voices are historically silent.
Glossary
Supplemental Material
sj-docx-1-mde-10.1177_23821205251329720 - Supplemental material for Classroom Debate as a Pedagogical Method to Explore the Relationship Between the Medical System and Patient Community Members
Supplemental material, sj-docx-1-mde-10.1177_23821205251329720 for Classroom Debate as a Pedagogical Method to Explore the Relationship Between the Medical System and Patient Community Members by Naeema Hopkins-Kotb, Elizabeth Janiak, Alex S. Keuroghlian and Deborah Bartz in Journal of Medical Education and Curricular Development
Footnotes
Author Contributions
EJ and DB developed the original debate. DB and AK facilitated the debate as course instructors. NHK and DB wrote the initial manuscript and subsequent revisions. AK and EJ reviewed and edited the manuscript.
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Alex S. Keuroghlian reports royalties as editor of a McGraw Hill textbook on transgender and gender-diverse health care and editor of an American Psychiatric Association textbook on gender-affirming psychiatric care.
Ethical Considerations
This article does not contain any studies with human or animal participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.