
Abstract
Background
The importance of integrating humanities into medical education has been recognized. However, the medical humanities curriculum is usually lacking during standardized training for residents in China. This study aims to determine the feasibility and effectiveness of pilot-specific courses in medical humanities in standardized residency training.
Methods
We designed specific courses in medical humanities, composed of 3 courses: Identifying and Managing Common Psychological Disorders of Patients, Patient-Clinician Communication, and Medical Dispute Cases Analysis and Resolution. The courses were scheduled monthly throughout the one semester, and a total of 118 residents participated in the curriculum. Participants completed the evaluation containing ethic-legal knowledge and humanistic competencies related to course content before and after the curriculum.
Results
Most participant residents had a bachelor's degree (85.6%) and were in the first year of standardized residency training (61.0%). Their disciplinary backgrounds are diverse, encompassing 18 different clinical medical specialties. The residents’ average scores of postcourse self-assessments keep a steady increase in humanistic competencies compared with precourse average scores. All postcourse self-assessments showed significant improvement compared to precourse (P < .05), particularly in influential communication skills and diagnostic associations of processing ability.
Conclusion
The specific courses in medical humanities are feasible and effective in teaching residents in China. The pre-post course evaluation indicates that this humanities-based curriculum significantly improved residents’ ethic-legal knowledge and humanistic competencies during standardized residency training.
Introduction
In recent years, medical schools and universities have embraced the humanities in medical education, employing various models of humanities-based curricula at the undergraduate and graduate medical education levels. 1 The importance of integrating humanities into medical education has been recognized for a long time, which is significantly correlated with positive personal qualities, including empathy, self-efficacy, and spatial skills. 2 Programs such as those for medical students at Mayo Clinic Institution 3 and neurology residents at the University of Virginia School of Medicine 4 are 2 recent examples of medical humanities curricula introduced.
Physicians undoubtedly need skills, knowledge, and technical competence, yet other personal qualities undeniably constitute “a well-rounded doctor.” 5 This concept has prompted a search for a more comprehensive way to train physicians by improving the content and teaching of medical humanities in medical education. As stated by Shapiro p.192, the aim is to help students of the health professions “better understand and critically reflect on their professions to become more self-aware and humane practitioners.” 6
A study reviewed learning outcomes of humanities curricula for medical students and found that the most widely described medical humanities were philosophy, ethics, anthropology, and arts in several forms. 7 In China, instruction in and research on medical humanities has increased at many medical colleges since the 1980s, later than in the United States or Europe. 8 Given the current tensions in the doctor-patient relationship and the mindset that “medical technology comes first” in China, experts argue that the most efficient way is to emphasize medical humanities and reshape medical curricula setting. 9 Over the past few years, more medical humanities curricula have been launched, such as an online course entitled Introduction to Medical Humanities, which was created at Fudan University in 2015 and has attracted considerable attention from around the country. 10 Medical humanities education is typically conducted in colleges but is usually lacking during standardized training for residents in China. In December 2013, guidance on establishing a standardized residency training system was published by the National Health Commission of China. According to the guidance, all medical clinicians with a bachelor's degree and above should receive standardized training for residents, and all provinces should comprehensively launch standardized training for residents by 2015. 11 However, there are few reports of medical humanities programs in standardized training for residents.
In China, the frequency of medical disputes was high, as were the levels of perceived tensions with patients. Close to half of the clinicians had experienced at least 1 dispute with a patient over the past 12 months in a survey. 12 High-quality communication will always rest at the heart of medicine, serving the patients’ needs for both information and empathy and alleviating the tense clinician-patient relationship. 13 Individual clinician communication skills do not improve reliably with time or experiences, and clinicians actually need to overlearn communication skills to be able to use them under stress. 14 Medical humanities education is typically conducted by theoretical courses in colleges, but residents in their early careers generally lack experience in avoiding and handling medical disputes.
The support of relevant courses tried to establish, from the beginning to enhance medical humanities quality at the residency training phase. To determine the feasibility and effectiveness of humanities-based courses for residents, we set up small-group specific courses that incorporate multidisciplinary medical humanities enriched with simulated patient interactions. These courses aim to enhance communication skills, foster positive personal qualities, and ultimately train a well-rounded doctor.
Methods
We implemented small-group, multidisciplinary, specific courses for residents in 2024. Early in the curriculum design, we conducted an online anonymous survey, which showed an inclination to attend medical humanities-based curricula with the help of the “Questionnaire Star” platform (Figure 1). Given their interest, the 3 specific humanities-based courses were involved for standardized training residents, which included Identifying and Managing Common Psychological Disorders of Patients, Patient-Clinician Communication, and Medical Dispute Cases Analysis and Resolution. The specific courses used the case-based learning (CBL) method, covering various clinical scenarios a resident may encounter, designed to identify psychological disorders, foster empathy, and enhance communication skills and capacity for handling medical disputes in order to improve the doctor-patient relationship.

Residents’ inclination to attend medical humanities-based curriculum.
Three courses in the series were scheduled monthly throughout the one semester, with 4 hours per course. A maximum of 40 residents are allowed to elect the curriculum, ensuring sufficient interaction between teachers and students. The course “Identifying and Managing Common Psychological Disorders of Patients” uses case-based learning, narrative learning, and simulated patients, which help residents identify psychological disorders, understand patients’ experiences, and foster empathy. The course “Patient-Clinician Communication” uses case-based learning, scenarios role-play, and real patient interactions, which help residents master communication skills. The course “Medical Dispute Cases Analysis and Resolution” uses case-based learning and lectures by multidisciplinary experts, which help residents earn the capacity for handling medical disputes (Figure 2).

Curriculum design consisting of 3 monthly courses, including identifying and managing common psychological disorders of patients, patient-clinician communication, and medical dispute cases analysis and resolution.
At the beginning and end of the courses, residents were required to complete the evaluation, and the evaluation contained ethic-legal knowledge and humanistic competencies related to course content. The evaluation of ethic-legal knowledge and humanistic competencies is based on the humanistic ability evaluation system of the China National Medical Practitioner Examination. The ethics-legal knowledge evaluation covered a range of foundational principles in medical ethics and health law, and it was evaluated through single-choice and multiple-choice questions. The humanistic competencies were evaluated using a 10-point Likert scale. Humanistic competencies are defined by the interdisciplinary humanities approach to developing appropriate analytical attitudes, ethical and professional behavior, effective communication, respect for diversity, and empathy. 15 Each item of the scale was explained in detail. For example, the ability to build trust was explained as encompassing respect, warmth, sincerity, and active listening. The Cronbach's Alpha of humanistic competencies is 0.982, and the Bartlett's Test of Sphericity is 0.939.
Professors from the hospital and university carried out the course design and implementation. The criteria for experts qualified in teaching these 3 courses: (1) Clinicians with over 15 years of experience in both clinical and teaching in university hospitals; or (2) professors with over 5 years of experience in handling medical disputes and major in ethics, health law, or psychology. In particular, the Medical Dispute Cases Analysis and Resolution course was conducted with 3 professors: a medical ethics professor, a health law professor, and a clinician from the Department of Emergency.
The reporting of this study conforms to the DoCTRINE Guidelines and the EQUATOR Network guidelines. 16 Categorical variables were analyzed as frequencies (percentages), and group differences were compared using the chi-square test. Continuous variables presented as T-test compared mean ± standard deviation. Analyses were performed using SPSS for Windows version 23.0. Outcomes were considered statistically significant when P < .05.
Results
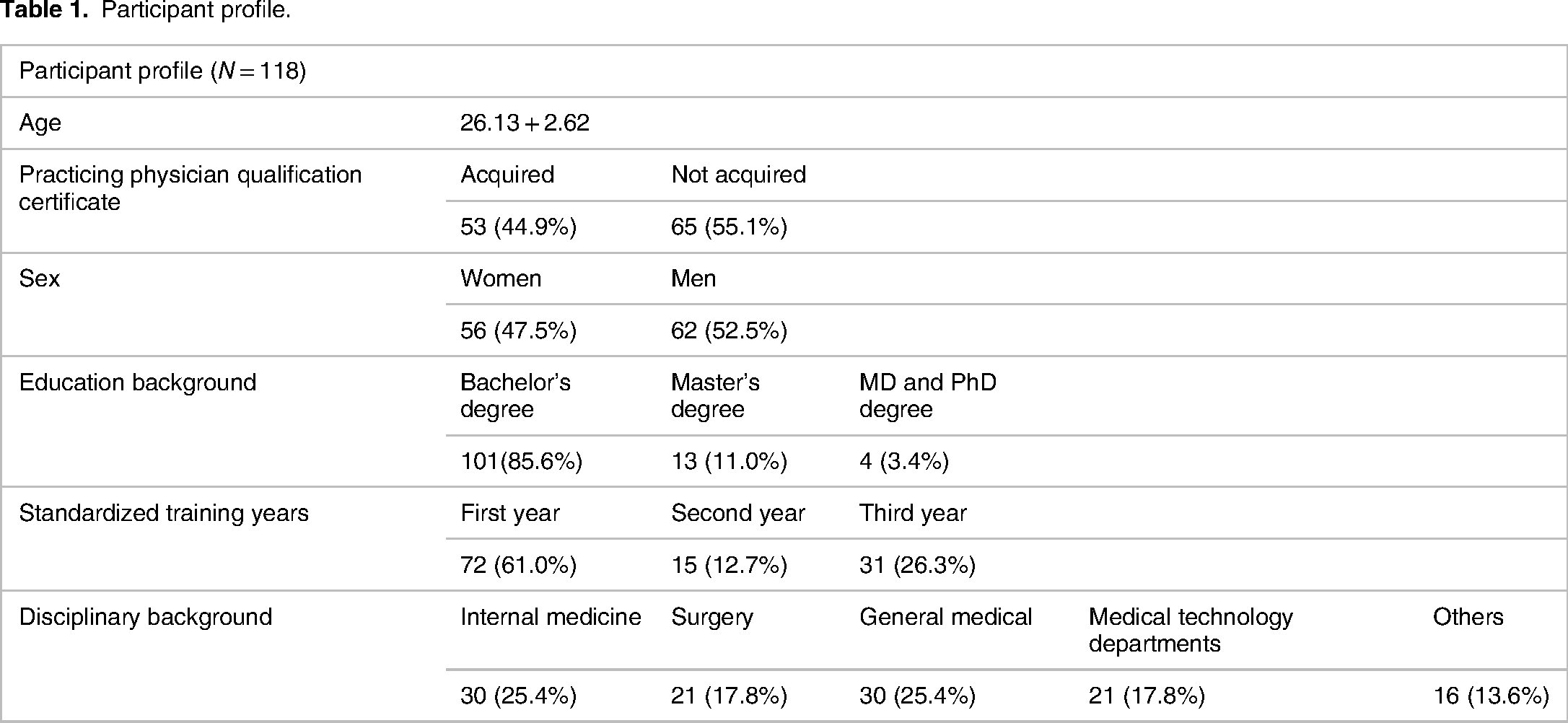
The 118 residents from different disciplinary backgrounds attended the curriculum, with 38–40 residents participating per course. All participants (100%) completed the curriculum evaluation precourse and postcourse. The courses generated lively discussions, and the residents particularly enjoyed the Medical Dispute Cases Analysis and Resolution. Most participants had a bachelor's degree (85.6%) and were in the first year of standardized residency training (61.0%). Their disciplinary backgrounds are diverse, encompassing 18 different clinical medical specialties, including internal medicine, surgery, general medical, obstetrics/gynecology, pediatrics, ophthalmology, dermatology, oncology, anesthesiology, radiology, pathology, and emergency medicine (Table 1).
Participant profile.
Precourse and postcourse evaluations were distributed to participating residents to evaluate the effectiveness of these specific courses in medical humanities. The accuracy of postcourse answers on ethic-legal knowledge was significantly higher than precourse (Table 2). Residents lack basic concepts of ethic-legal knowledge before the curriculum, as indicated by precourse error rates of 80.5%, 97.5%, and 87.3% for questions 1–3. However, our study shows that postcourse error rates significantly decreased after the curriculum for questions 1–3 (Q1:
Comparison of residents’ ethic-legal knowledge precourse and postcourse.

As shown in Figure 3, the residents’ average scores of postcourse self-assessments keep a steady increase in humanistic competencies compared with precourse average scores. All postcourse self-assessment items showed significant improvement compared to precourse (P < .05), particularly in the items of influential communication skills and diagnostic associations of processing ability (7.75 ± 1.66 vs 8.75 ± 1.19, P < .000. 7.55 ± 1.73 vs 8.72 ± 1.21, P < .000) (Table 3). The results indicated that the specific courses in medical humanities effectively helped residents improve humanistic competencies.

The trend of residents’ humanistic competencies average scores precourse and postcourse.
Comparison of residents’ self-assessments in humanistic competencies precourse and postcourse.

Discussion
Medical humanities are commonly associated with “soft” skills relevant to clinical practice; humanities-engaged clinical education helps build social and relational skills, compassion, self-reflection, interpersonal skills, critical reflection, etc. 17 This pilot study developed specific courses in medical humanities for standardized training residents in China. Residents’ sustained and active participation supports the feasibility of using humanities-based strategies in a residency curriculum. The pre-post course evaluation indicates that these specific courses in medical humanities significantly improved residents’ ethic-legal knowledge and humanistic competencies. The results demonstrated that our courses are feasible and effective in teaching residents in China.
Since 2016, the number of medical disputes in China has increased by almost 100,000 cases annually. 18 Moreover, China is the only country in which the prevalence of workplace violence by month has been studied, and the rate of death (12.8%), severe injury (6%), and hospitalization (24.2%) have resulted from serious workplace violence. 19 To prevent medical disputes in such circumstances, it is crucial to identify the causes of medical disputes. Medical disputes typically involve doctors, hospitals, patients, and their families. 20 Multiple causes, such as patients misunderstanding medical behavior and complex medical procedures, contribute to medical disputes. However, the truth is that over 80% of medical disputes are related to doctors, and insufficient communication is the most prominent factor. 21 The present study was to help residents identify psychological disorders, foster empathy, and enhance communication skills and capacity for handling medical disputes. Earning this capacity of doctors during standardized residency training is significant in improving the doctor-patient relationship.
Effectively developing professionalism requires a programmatic view of how medical humanities should be incorporated into an educational continuum that begins in medical school and stretches across residency and throughout one's practice. 22 But medical educators have consistently prioritized medical schools incorporating medical humanities. A few programs integrate medical humanities curricula in residency: a review showed that an art-based medical humanities curricula conducted in surgical residency, 23 and a program had been implemented in Medical Humanities & Arts to medical students and residents at the University of California. 24 As mentioned in the previous part, China is gradually improving as a society that has embraced standardized training of residents for only a decade. 11 A Chinese survey showed that most residents were positive toward the communication skills training curriculum and would value further humanities-based curriculum. 25 We implemented pilot-specific courses in medical humanities after considering residents’ workloads and interest, it contained 3 courses covering the disciplines of medical ethics, health law, and medical psychology. This effectively developing curriculum may contribute to the training of a professional and well-rounded doctor.
There are a few limitations. Similar to most previous studies, our results are limited by small numbers and lack a control group. Our study encountered traditional potential bias in pre-post self-assessment designs when the learner's understanding of the measured construct changes as a result of the intervention. Another limitation of this study is the inability to conduct longitudinal comparisons due to the fact that it is only the first semester of the academic year. Longitudinal comparisons are important to draw robust conclusions about the long-term effects of medical humanities-based curricula for residents in China.
The specific courses in medical humanities are feasible and effective for residents in China. The curriculum we have described is now in its 2 semesters, and the course content has added new clinical cases and humanities-based topics in the 3-year residency cycle. The major goal of medical education in humanities is to promote humanistic skills and professional conduct in a well-rounded doctor. Patient-centered skills enable learners to become medical professionals, whereas a comprehensive humanities curriculum assists learners to appraise the concept and implementation of medical professionalism critically. 26
Conclusions
The specific courses in medical humanities are feasible and effective in teaching residents in China. The pre-post course evaluation indicates that this humanities-based curriculum significantly improved residents’ ethic-legal knowledge and humanistic competencies during standardized residency training.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241307444 - Supplemental material for Medical Humanities in Resident Training: A Pilot Study of Specific Courses in a Large Comprehensive Hospital in China
Supplemental material, sj-docx-1-mde-10.1177_23821205241307444 for Medical Humanities in Resident Training: A Pilot Study of Specific Courses in a Large Comprehensive Hospital in China by Xiaoyun Yang, Lifang Guo, Xiaoxiong Chen, Ju Zhang and Qiang Xiang in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The professors from the Department of Emergency of the First Affiliated Hospital and Army Medical University supported this work. They were instrumental in helping collect clinical cases, teaching, and formulating course content.
Author Contribution
QX contributed to the study's conceptualization, methodology, supervision, and project administration. XXY contributed to study investigation, data analysis, writing—original draft and review & editing, and funding acquisition. LFG contributed to the study investigation and data analysis. XXC contributed to study validation, data curation, and writing—review & editing. JZ contributed to the formulation of course content and course teaching.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due to the hospital's management requirements. Still, they are available from the corresponding author on reasonable request.
Ethical Approval
Not applicable.
Funding
This study was supported by grants from the Research Project on Medical Education and Teaching Reform at the Institutional Level After Graduation of Army Medical University (Number:2023bjg101).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.