
Abstract
INTRODUCTION
Human trafficking is a widespread public health problem across the United States. In recognition of the incredible need among victims and survivors of human trafficking for longitudinal, trauma-informed care, the Medical Safe Haven (MSH) was developed in 2016 through the Dignity Health Family Medicine Residency Program in Sacramento, California, and subsequently expanded to 2 other Dignity Health residency program sites. The MSH program included 3 sessions of trafficking-specific curriculum for resident physicians to prepare them to provide care for MSH patients. The current study aimed to evaluate resident physician learner confidence after participating in the MSH curriculum along with perceptions of the MSH program as a whole upon their graduation.
METHODS
The study was a retrospective, preassessment/postassessment design. Resident physicians completed surveys that assessed learner confidence after each of the 3 training sessions, utilizing Likert scale items. Third-year resident physicians also completed a survey that included scaled and open-ended questions. Paired t-tests were used to evaluate the data in addition to content analysis for the open-ended questions.
RESULTS
There were significant increases in learner confidence after the training sessions on all items measured, including identifying and caring for victims and survivors of trafficking. Third-year residents responded that the MSH program helped them to more effectively communicate and care for victims and survivors and many planned to take the trauma-informed care model to their future practices.
CONCLUSION
While generalizability of the study was limited due to the retrospective design, the MSH program was found to have a meaningful impact on the resident physicians who participated in the training.
Introduction
Human trafficking is a widespread public health problem defined by the U.S. Department of Justice as a crime that involves compelling or coercing a person to provide labor or services, or to engage in commercial sex acts. 1 Data from the U.S. National Human Trafficking Hotline showed that since 2007, there were 82 301 situations and 164 839 victims of trafficking identified. 2 Trafficking is a widespread phenomenon, with worldwide estimates of the number of trafficked persons varying widely. The International Labour Organization estimates that there were 49.6 million people living in modern slavery in 2021, including 27.6 million people in forced labor. 3
Many victims, >50% in a survey conducted by the Coalition to Abolish Slavery and Trafficking, encountered a healthcare provider at least once while they were being exploited. 4 Chisolm-Straker et al 5 found that 68% of 163 identified victims of human trafficking had seen a healthcare provider while being trafficked, with the largest proportion having seen providers in emergency and urgent care settings, followed by primary care, dentistry, and obstetrics and gynecology. The majority did not disclose their trafficking status secondary to barriers such as fear, shame, limited time with healthcare providers, and language. 4 They often went unrecognized as victims of trafficking and never received resources to help them leave their situations.
The trauma-informed care (TIC) model has expanded tremendously in numerous health settings as the impact of trauma on health outcomes across various medical conditions is becoming better understood. A TIC model for primary care includes 5 components, including screening and recognition of trauma, understanding the health effects of trauma, patient-centered communication and care, emphasis on emotional safety and avoiding triggers, and knowledge of helpful treatment. 6
In the United States, California had the largest percentage of substantive signals, including phone calls, emails, and text messages, to the National Human Trafficking Hotline. 2 In 2014, Dignity Health initiated the Human Trafficking Response Program to develop protocols to identify and care for victims and survivors of trafficking in healthcare settings. 7 As part of this initiative, providers and staff were educated on human trafficking and TIC. In addition, resources and partnerships within the community were expanded to support this patient population. Mercy Family Health Center, a family medicine residency training center affiliated with Dignity Health's Methodist Hospital, developed the Medical Safe Haven (MSH) in order to provide comprehensive TIC in addition to longitudinal health services.
The goal of the MSH was to create a “medical home” where these patients felt safe and trusted their providers. Residency training programs were identified as particularly well suited for the MSH model. 8 Resident physicians would not only learn to identify and provide care for victims and survivors of human trafficking, but they would also take those skills to their future practices upon graduation, thus broadening access to care for this vulnerable patient population through a ripple effect. In 2019, 3 years into the MSH program's inception, Mercy Family Health Center provided over 500 clinical visits for victims and survivors of trafficking annually, averaging over 25 visits per resident physician per year. 7 Given the success of the Sacramento primary care site, the MSH model was expanded to 2 additional Dignity Health family medicine residency training programs in California: Northridge and Redding.
In establishing the MSH, resident physicians participated in a training curriculum focused on human trafficking and TIC. There were 3 training sessions that comprised the MSH curriculum: human trafficking MSH (HTMSH) training, TIC training, and patient–physician encounter (PPE) training. Each session was typically 2 h in length. Topics discussed included an introduction to human trafficking, with an emphasis on prevalence in the residents’ own community, common signs that a patient may be a victim or survivor of trafficking, and role play on how to conduct intake visits. During some sessions, survivors and representatives from community organizations spoke with the resident physicians about their experiences and what they felt medical providers should know. Resident physicians typically completed at least 1 training session prior to working with patients in the MSH clinic. The other training sessions were held throughout the year during didactic lectures.
With the integration of new clinic models and training curricula, it was important to assess the effectiveness of such implementations on resident physician competencies. The current study sought to evaluate learner confidence after participating in human trafficking and TIC curricula across 3 training locations. In addition, the purpose was to evaluate third-year resident physicians’ learner confidence and experience upon graduation from the MSH program. The current study was conducted in order to improve upon resident physician education within the MSH clinic model, along with gathering data to support the expansion of the MSH clinic model to more residency training sites across the United States.
Methods
Funding
In 2018, Dignity Health received funding from the Department of Justice, Office for Victims of Crime to expand mental health services for patients of the MSH clinic in Sacramento and to expand the MSH model to 2 additional Dignity Health residency training sites in California: Northridge and Redding. This funding also supported a formal evaluation of the MSH program, which was contracted to LPC Consulting Associates, Inc., who helped design and conduct an overall program evaluation. 8 The grant period was over the 3-year period from October 2018 through October 2021. Institutional Review Board approval was obtained through Dignity Health, ID #CANV DHIRB-2019-487, with an approval date of January 13, 2020, and a closure date of September 26, 2022.
Study Design
LPC Consulting met with the directors of the MSH program at the Sacramento location to develop a program evaluation utilizing the logic model, a graphic representation of a program's resources, activities, outcomes, and impacts. 9 The current study focused on the resident education component of the program evaluation. The design of the evaluation and data collection was conducted in conjunction with LPC Consulting. The authors independently reviewed the raw data and performed their own analyses and conclusions. The nature of the current study was a retrospective, prequantitative/postquantitative, and qualitative assessment utilizing survey methodology.
Resident Physician MSH Training Survey
The MSH model was integrated and assessed at 3 Dignity Health family medicine residency programs in California: Sacramento, Northridge, and Redding. 7 Sacramento began training resident physicians with the MSH curriculum in 2016, with data collection starting with the graduating class of 2018. Northridge began training resident physicians in September 2020, and Redding began in March 2021.
Inclusion criteria included any resident physician from the Sacramento, Northridge, or Redding Dignity Health family medicine residency programs who attended 1 of the MSH training sessions. On the survey, participants were asked to identify as a resident physician or “other,” which included medical students and staff. Participants who marked “other” or left this question blank were excluded from the study. Residents were not compensated for their participation.
At the completion of each training session (HTMSH, TIC, and PPE), resident physicians completed anonymous curriculum-specific surveys assessing learner confidence with the material. These surveys were either completed on paper for in-person sessions or online for Zoom sessions necessitated by the COVID-19 pandemic. A document was provided with the survey indicating the purpose and voluntary nature of the study, including the clause: “Being in this study is optional, and completing the survey will be considered consent.” Respondents could opt out at any time including not answering questions after starting the survey. This method of consent was approved by the Dignity Health Institution Review Board.
The surveys included a retrospective component, asking residents to respond as if they were completing the questions prior to attending the training session. The posttraining questions asked participants to select a response after attending the training. The “before” and “after” questions were incorporated into the same survey completed at the end of the training session. While not an ideal methodology, the current study was limited to providing the survey only after the training given multiple factors such as the training sessions being held during didactic sessions with unspecified attendance from resident physicians in addition to guest lecturers traveling long distances to facilitate the training sessions, particularly with the Northridge and Redding sites. The retrospective presurvey was implemented for ease of administration and to allow for a larger number of residents to participate in order to better evaluate the program. A recent study by Thomas et al 11 evaluating traditional versus retrospective preassessment/postassessment suggested that retrospective methodology can improve response-shift bias and can be a useful and cost-effective technique for training evaluations.
The survey questions were unique to each training session (ie, HTMSH, TIC, and PPE) and were analyzed separately. The HTMSH and TIC surveys included 11 Likert scale items that assessed learner confidence in addition to 3 Likert scale items that assessed training satisfaction and 1 free response question. The PPE survey was similar but only included 10 Likert scale questions assessing learner confidence; the other questions were the same as those included in the other surveys. The questions were developed in conjunction with LPC Consulting and were derived from the logic model. Validated scales were not used.
All of the aforementioned survey questions incorporated a 5-point Likert scale, with the definition of the scale varying per section of the survey (ie, 1 = not at all aware to 5 = extremely aware, 1 = strongly disagree to 5 = strongly agree). The before and after responses were evaluated using paired t-tests and 1 unpaired t-test performed through GraphPad Prism Software 2023. 12 Results from the training satisfaction questions were not evaluated or discussed in the current study.
The surveys also included 1 open-ended question that provided the option for narrative feedback (ie, What additional information do you need to help you as a physician working with human trafficked victims/survivors?).
MSH Third-Year Resident Survey
Graduating third-year residents across all 3 training sites in California were given the opportunity to complete an MSH Third-Year Resident Survey. Data collection was initiated in April 2020. Sacramento residents from the classes of 2018 and 2019 were invited to participate via a survey link that was emailed to them. The residents from the classes of 2020 and 2021 across all 3 sites completed the survey either on paper or online.
Quantitative items included questions that assessed the number of years working in the MSH and how many trafficked patients they treated. The survey assessed residents’ confidence related to working with trafficked patients. The assessment included a retrospective component, asking residents to think back to when they first started working in the MSH clinic to answer the before questions. Then residents were asked to rate their confidence after working in the MSH clinic. Both before and after questions were completed in the same survey, utilizing a 4-point scale (ie, 1 = no confidence to 4 = confident). There were 4 items, evaluated with paired t-tests performed through GraphPad Prism Software 2023. 12
A qualitative component included the following 3 open-ended questions: did your experience at the MSH clinic prepare you to care for the medical needs of trafficked victims and survivors using a victim-centered approach? What additional training/experiences would have helped you when working with trafficking victims/survivors? Take a moment to think about your future as a physician. How do you plan to take your experiences with the MSH clinic with you/how do you envision using these experiences? A content analysis of responses identified major themes utilizing the consolidated criteria for reporting qualitative research model. 13 The responses were coded to identify how many individuals reported on each theme.
Results
Resident Physician MSH Training Survey
Over the 3-year study period, a total of 81 residents across the 3 sites participated in 1 or more MSH training sessions. This included 31 residents from Sacramento, 32 residents from Northridge, and 18 residents from Redding. The results were broken down into curriculum-specific evaluations.
HTMSH Training
In total, 39 resident physicians completed the survey after attending the HTMSH training. Learner confidence scores significantly increased on all items evaluated (see Figures 1 and 2). Participants’ awareness of the industries where labor and sex trafficking most often occur increased from before (M = 2.49, SD = 0.79) to after training (M = 4.31, SD = 0.69), t(38) = 10.59, p < .001. Participants’ awareness of the physical indicators of a trafficked victim/survivor increased from before (M = 2.56, SD = 0.94) to after training (M = 4.26, SD = 0.59), t(38) = 11.83, p < .001. Similarly, awareness of the indicators that may signify trafficking increased from before (M = 2.77, SD = 0.90) to after training (M = 4.36, SD = 0.54), t(38) = 10.0, p < .001. Awareness that human trafficking takes place in my own country increased from before (M = 2.92, SD = 1.09) to after training (M = 4.59, SD = 0.59), t(38) = 9.19, p < .001. Awareness of the scope of human trafficking in the USA and worldwide changed from before (M = 3.13, SD = 0.80) to after training (M = 4.46, SD = 0.55), t(38) = 11.29, p < .001. Awareness of the impact of chronic trauma on the brain and symptomatology increased from before (M = 3.15, SD = 1.11) to after training (M = 4.41, SD = 0.82), t(38) = 7.51, p < .001. Awareness that commercial sexual activity is considered human trafficking, whether forced or voluntary, if the individual is <18 years of age increased from before (M = 3.31, SD = 1.15) to after training (M = 4.59, SD = 0.55), t(38) = 7.62, p < .001.

HTMSH survey learner confidence scores. Utilizing a 5-point Likert scale (1 = not at all aware to 5 = extremely aware), participants reported their awareness of the items before and after they completed the training curriculum. (*) signifies p value <.001.

HTMSH survey learner confidence score, part II. Utilizing a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), participants reported their confidence in the items before and after they completed the training curriculum. (*) signifies p value <.001.
Posttraining, participants’ confidence in where to find resources for a human trafficking victim (M = 2.56, SD = 0.91) was higher than before training (M = 4.00, SD = 0.86), t(35) = 10.72, p < .001. Confidence in recognizing common indicators, signs, and symptoms of abuse, neglect or violence, and human trafficking increased from before (M = 2.94, SD = 0.83) to after training (M = 4.11, SD = 0.62), t(35) = 11.49, p < .001. Participants indicated that human trafficking education is an important component of resident physician training, with an after-training score (M = 4.81, SD = 0.40) that was higher than the before-training score (M = 4.42, SD = 0.73), t(35) = 4.24, p < .001. Participants indicated that it is essential to empower adult human trafficking victims to make their own choices regarding their trafficking situations, with an after-training score (M = 4.81, SD = 0.40) that was higher than the before-training score (M = 4.39 SD = 0.73), t(35) = 4.51, p < .001.
TIC Training
In total, 45 resident physicians completed the TIC training survey. Posttraining, learner confidence significantly increased on all items (see Figures 3 and 4). Awareness of the importance of putting victims’/survivors’ wishes, safety, and well-being as a priority increased from before (M = 4.27, SD = 0.86) to after training (M = 4.80, SD = 0.50), t(44) = 5.71, p < .001. Awareness of the scope and impact of trauma, including adverse childhood experiences increased from before (M = 3.73, SD = 0.93) to after training (M = 4.48, SD = 0.70), t(43) = 6.62, p < .001. Awareness of the impact of chronic trauma on the brain and symptomatology increased from before (M = 3.52, SD = 1.06) to after training (M = 4.30, SD = 0.82), t(43) = 7.56, p < .001. Awareness of the long-term impacts of trauma bonding on victims/survivors increased from before (M = 3.52, SD = 1.07) to after training (M = 4.45, SD = 0.63), t(43) = 6.68, p < .001. Awareness of the potential physical indicators of a trafficked victim/survivor increased from before (M = 3.2, SD = 0.87) to after training (M = 4.38, SD = 0.58), t(44) = 9.48, p < .001. Awareness that victims/survivors can be triggered and/or retraumatized during routine healthcare visits increased from before (M = 3.47, SD = 1.08) to after training (M = 4.60, SD = 0.58), t(44) = 8.75, p < .001.
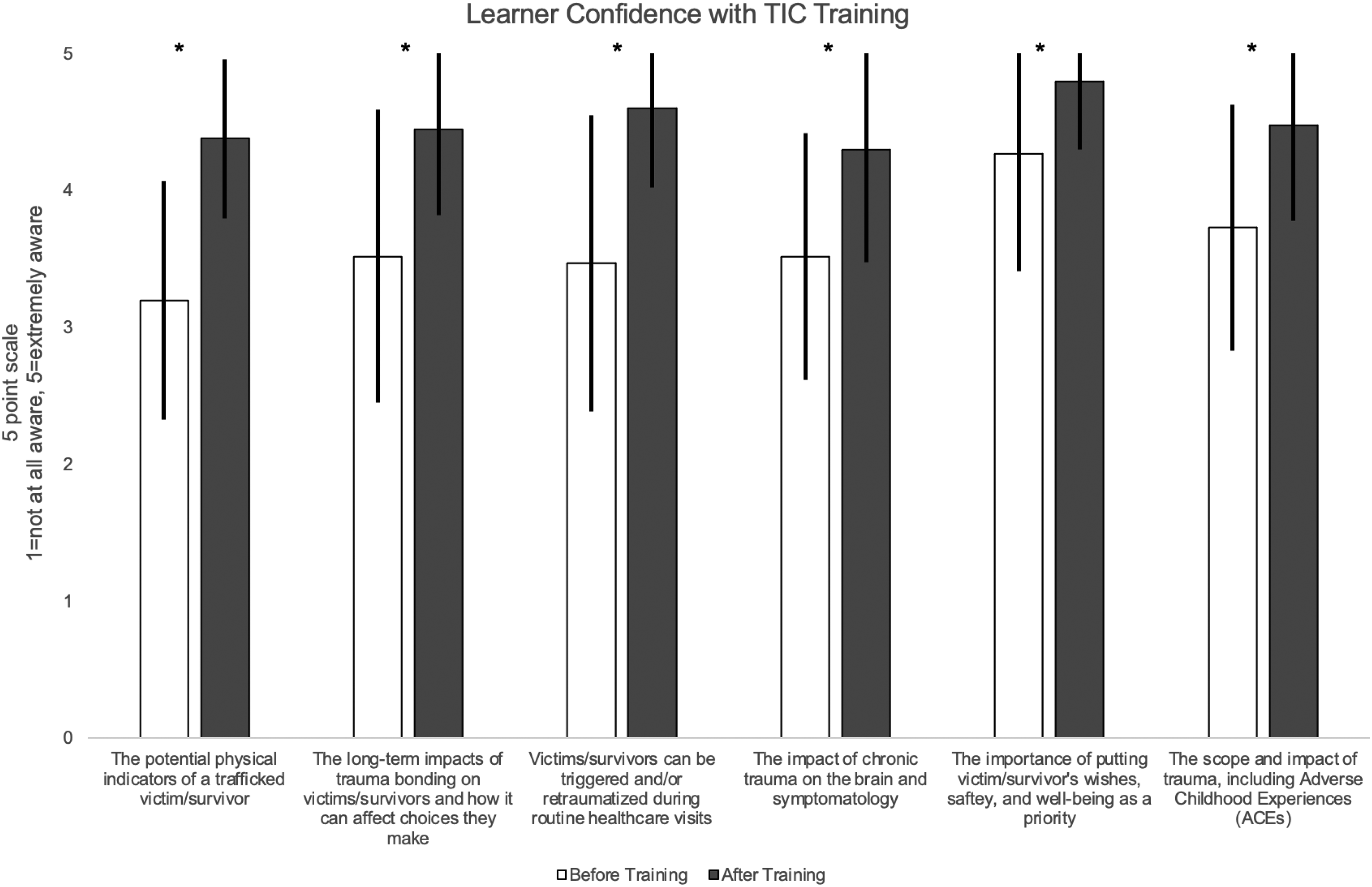
Trauma-informed care (TIC) survey learner confidence scores. Utilizing a 5-point Likert scale (1 = not at all aware to 5 = extremely aware), participants reported their awareness of the items before and after they completed the training curriculum. (*) signifies p value <.001.
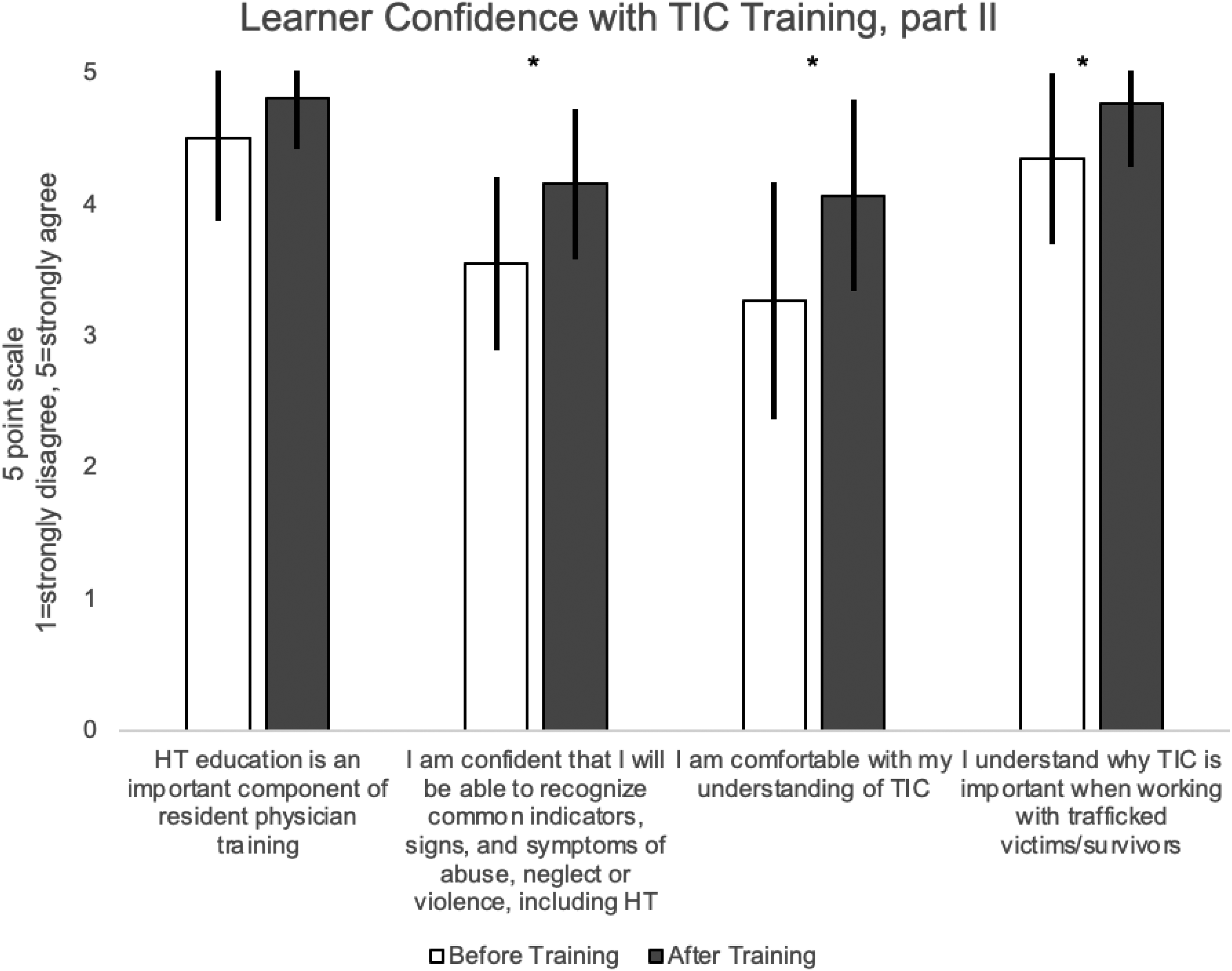
Trauma-informed care (TIC) survey learner confidence scores, part II. Utilizing a 5-point Likert scale (1 = no confidence to 5 = confident), participants reported their confidence in the items before and after they completed the training curriculum. (*) signifies p value <.001.
Posttraining, participants’ confidence on all items increased as well, including residents’ understanding of TIC, from before (M = 3.27, SD = 0.90) to after training (M = 4.07, SD = 0.73), t(43) = 5.835, p < .001. Confidence increased in recognizing common indicators, signs, and symptoms of abuse, neglect, or violence, including human trafficking, from before (M = 3.55, SD = 0.66) to after training (M = 4.16, SD = 0.57), t(43) = 6.58, p < .001. Participants indicated that human trafficking education is an important component of resident physician training, with an after-training score (M = 4.81, SD = 0.39) that was higher than the before-training score (M = 4.51, SD = 0.63), t(42) = 3.55, p = .001. In addition, residents indicated that [they] understand why TIC is important when working with trafficked victims/survivors, with an after-training score (M = 4.77, SD = 0.48) that was higher than the before-training score (M = 4.35, SD = 0.65), t(42) = 5.50, p < .001.
PPE Training
In total, 41 resident physicians completed the PPE training survey. Posttraining, participants’ confidence in all items significantly increased (see Figures 5 and 6). Awareness that victims/survivors can be triggered and/or retraumatized during routine healthcare visits increased from before (M = 3.90, SD = 0.84) to after training (M = 4.58, SD = 0.55), t(39) = 6.15, p < .001. Residents’ understanding of the patient advocate in the MSH increased from before (M = 3.15, SD = 1.22) to after training (M = 4.34, SD = 0.66), t(40) = 7.42, p < .001. Awareness of the long-term impacts of trauma bonding on victims/survivors and how it affects choices they make increased from before (M = 3.40, SD = 0.82) to after training (M = 4.45, SD = 0.55), t(39) = 6.92, p < .001. Residents had increased awareness of mandated reporting requirements/responsibility for an identified trafficking victim who is under 18 years old compared to a victim 18 or older, from before (M = 3.54, SD = 1.10) to after training (M = 4.24, SD = 0.70), t(40) = 5.37, p < .001. Awareness increased of the impact of chronic trauma on the brain and symptomatology, from before (M = 3.58, SD = 1.10) to after training (M = 4.37, SD = 0.73), t(40) = 5.91, p < .001, in addition to the physical indicators of a trafficked victim/survivor, from before (M = 3.35, SD = 1.03) to after training (M = 4.08, SD = 0.66), t(40) = 6.10, p < .001.

Patient–physician encounter (PPE) survey learner confidence scores. Utilizing a 5-point Likert scale (1 = not at all aware to 5 = extremely aware), participants reported their awareness of the items before and after they completed the training curriculum. (*) signifies p value <.001.

Patient–physician encounter (PPE) survey learner confidence scores. Utilizing a 5-point Likert scale (1 = no confidence to 5 = confident), participants reported their confidence in the items before and after they completed the training curriculum. (*) signifies p value <.001.
Participants felt more confident raising questions about human trafficking with victims/survivors from before (M = 3.05, SD = 0.92) to after training (M = 4.26, SD = 0.59), t(38) = 8.15, p < .001. Residents also felt more comfortable with (their) understanding of human trafficking victims, both labor and sex after training (M = 4.10, SD = 0.63) compared to before (M = 3.25, SD = 1.03), t(39) = 6.45, p < .001. Residents responded that it is essential to empower adult human trafficking survivors to make their own healthcare choices and support their wishes, safety, and concerns, with an after-training score (M = 4.80, SD = 0.41) that was higher than the before-training score (M = 4.45, SD = 0.71), t(39) = 3.81, p < .001. Residents also indicated that they understand the importance and reasons for the “crucial points” to patient visits, with an after-training score (M = 4.15, SD = 0.83) that was higher than the before-training score (M = 3.38, SD = 0.93), t(39)=, p < .001.
Additional Information Requested
Lastly, each training survey concluded by asking if there was any additional information needed to help resident physicians work with human trafficked victims/survivors. A content analysis of the responses identified 3 main themes that were carried through among all 3 surveys: resources, experience, and additional training.
Participants requested information on resources, such as easily accessible resource sheets or lists of established trauma-informed providers. Some requested information on legal resources available to the MSH and other safety net programs (ie, food stamps, and housing) to help victims out of their exploitative situations. Another suggested resource was a list of questions to help facilitate conversations with trafficked patients to encourage them to talk about their experiences.
Many resident physicians stated they needed more experience with trafficked patients, as well as experience with the MSH tools and processes. Suggestions included using role-playing and case examples during training sessions and having senior resident physicians speak about common challenges they faced in the MSH clinic. Some resident physicians requested more training to learn to identify signs of trafficking in patients, such as local branding tattoos.
MSH Third-Year Resident Survey
Thirty third-year resident physicians from all 3 family medicine training sites participated in the survey with the following breakdown: 7 from Northridge, 6 from Redding, and 17 from Sacramento. Ninety percent of residents who participated in the survey were from the classes of 2020 and 2021.
Learner confidence significantly increased on all items (see Figure 7). Residents’ confidence in identifying trafficked victims/survivors increased from before (M = 1.87, SD = 0.68) to after involvement in the MSH program (M = 3.30, SD = 0.79), t(29) = 9.61, p < .001. Confidence increased when working with victims/survivors from before (M = 1.90, SD = 0.80) to after involvement (M = 3.33, SD = 0.88), t(29) = 8.08, p < .001. Confidence increased in addressing the issues of victims/survivors from before (M = 1.83, SD = 0.79) to after involvement (M = 3.23, SD = 0.86), t(29) = 7.92, p < .001. Confidence also increased in providing TIC from before (M = 1.87, SD = 0.86) to after involvement (M = 3.33, SD = 0.96), t(29) = 8.25, p < .001.

Third-year resident physician survey confidence scores. Utilizing a 4-point Likert scale (ie, 1 = no confidence to 4 = confident), participants reported their confidence in the items. (*) signifies p value <.001.
An unpaired t-test showed that there was no significant difference between confidence when working with victims/survivors between residents who had spent 3 years with the MSH program (M = 3.75, SD = 0.45) and residents who had spent 2 years or less with the MSH program (M = 3.28, SD = 0.83), t(28) = 1.80, p = .08.
A content analysis was performed on 21 residents’ feedback in the open-ended questions. For the first question addressing how the MSH experience prepared residents to work with trafficked victims and survivors, 7 residents reported that they learned how to communicate more effectively with this patient population. Other themes included learning how to identify victims and survivors (mentioned 5 times), having a clinic structure including the increased time that allowed for trust (mentioned 3 times), and training sessions that were beneficial (mentioned twice).
One resident stated [The MSH] gave me a framework to think about [victims’] encounters with medical professionals (especially from the perspective of a chronically traumatized patient). [It] allowed me to loosen the structure for the interview, understanding that there was no way to get the patient to tell me a straight story and that trying to do so wasn't helpful for either of us. [It] gave me permission to not always get all the data if it came at the expense of making a patient feel like they weren't in control of the encounter and if they didn't feel safe because of it.
Another resident responded, Our initial training improves our ability to identify victims and safe ways to approach provision of resources and care to these patients in a non-threatening, patient-centered way. The structure of our clinic allows for us to get these patients folded in for MSH intake appointments if we identify them. Most often, they come to our clinic through community resource partners… Scheduled visits with these patients are primarily structured to enable the patient to do the talking and the provider to do the listening and because intakes are given an entire hour, patients are usually able to start opening up about their experiences. This is key to building trust. Constant contact within our outpatient clinic with our MSH patients from the time of their intake onwards regardless of their medical needs is key to continuing trust-building and key to normalizing medical visits for these patients who formerly feared medical attention due to its connotation with punitive measures.
One resident stated, I am more comfortable with initiating conversations and questions about trafficking and I am familiar with the different community resources available to help these victims. It has made the most impact on my medical career. I think all residents should undergo this training and learn to care for these patients.
Another responded, “I have learned how to best approach sensitive issues and make people feel more comfortable sharing. I have learned to accept whatever the person is sharing in a nonjudgmental way.”
Additionally, one resident reported, [It] taught me how to ask questions and also to make the victim/survivor feel more confident in their provider and building trust (physician–patient trust relationship). [It] also taught me a lot more about trauma-informed care, and what other nonverbal concerning clues to look for during clinic encounters.
Regarding training sessions, 1 resident stated, “The lectures were very comprehensive and not isolated events. The team came back on several other occasions to go into more depth with real-life cases. It really opened my mind.”
When the residents were asked what additional training/experiences would have helped in order to work with trafficking victims/survivors, 5 residents stated they did not need additional training. Seven residents stated they needed more experience with patients. Other residents had the following responses: “working at gender health clinic with trans patients (many of whom are or were engaged in survival sex work). Listening to lectures provided by community leaders and organizers such as those who work at Weave [community organization],” “working with the District Attorney's office to have some insight into the legal issues these patients deal with,” and “continue yearly training sessions as refreshers.”
When residents were asked how they would use this training in the future, 6 specifically mentioned incorporating the “TIC” model into their future practice. Eight mentioned it would help them “identify” or “recognize” victims. Four mentioned they would “initiate” training for other providers they worked with.
One resident stated, Trauma informed care is now a regular part of my practice, regardless of whether I'm working with trafficking victims/survivors or not. I pay attention to non-verbal communication more critically and inquire about those kinds of things on a regular basis to figure out if it is just an odd behavior or more of a red flag. If I'm ever in a practice setting where trauma informed care is not practiced, I'd advocate for training for all staff (not just physicians).
Another responded, These experiences have been instrumental in developing my approach to patient care. I plan to start a medical safe haven in my future practice and to teach the other physicians to care for these patients there. I discussed this with them prior to joining [their practice].
Another said, “I plan to be more vigilant and screen patients as necessary when I am concerned about them being victims. I would like to provide a safe environment for them to obtain the care that they need and deserve.”
One stated, I hope to replicate the Dignity Health approach/model to identifying and treating victims at my future hospitals. I have started to use trauma informed care in many of my encounters, even those that are not directly related to human trafficking victims.
Discussion
From a learner perspective, the MSH program is comprised of trafficking-related training in addition to resident physicians caring for victims and survivors of trafficking throughout the course of their residency training. The MSH program evaluation assessed learner confidence after participating in each of the 3 MSH training. For all items assessed, there was a significant increase in learner confidence after resident physicians completed the training compared to confidence with the material prior to the training. Items of note included increased confidence in recognizing physical indicators of a victim of trafficking, where to find resources for a trafficking victim, and the impact of trauma on the brain and symptomology. Before and after training, residents indicated that human trafficking is an important component of resident physician training.
Graduating third-year resident physicians were also assessed upon completion of their participation in the MSH program. Learner confidence significantly increased after participation in the MSH program on all items assessed, including confidence in providing TIC, identifying trafficked victims/survivors, addressing the issues of victims/survivors, and working with victims/survivors. A content analysis of the open-ended questions revealed that many planned to continue using the TIC model for patients who have experienced trafficking in addition to their other patients. Residents felt that the clinic structure allowed for trust to be built between provider and patient, specifically having extra time with these patients and ready access to community resources through a patient advocate. Furthermore, some hoped to initiate an MSH program at their new place of employment, or at least continue a TIC model. Some residents stated they were positively impacted by the MSH program and recommended this type of training to other resident physicians.
There was no significant difference in confidence when working with victims/survivors between residents who had completed 3 years with the MSH program compared to residents who had completed 2 years or less. This analysis was limited by sample size, and in the future, it would be beneficial to assess whether there is a correlation between residents’ confidence and the number of patients seen in the MSH clinic.
Residents noted that extra time with patients was important for their ability to build trust with this patient population. The clinic structure and resources of a residency clinic enabled intake visits to have an allotted 1.5 h for MSH patients. This time allowed for the patient to meet with the Patient Advocate at the beginning and end of the visit if needed in addition to allowing for the resident physician to build rapport with the patient and to precept with the attending physician. In a nonresidency clinic, the intake visits likely would not require that amount of time, given the lack of need for precepting. In addition, clinic support staff could meet with the patient while the attending physician is scheduled with other patients, to make the program feasible in a nonresidency clinic model.
Overall, resident physicians felt that the curriculum and hands-on experience helped them feel more confident in caring for this vulnerable population and to continue this care in the future. From the resident perspective, important aspects of the curriculum included teaching residents how to ask trauma-informed questions, build trust, help patients feel comfortable, and approach the patients nonjudgmentally.
Future research should target the perceptions and health outcomes of victims and survivors of human trafficking who receive care in an MSH. It would also be beneficial to assess the effects on emergency department utilization among victims and survivors of trafficking and the general community impact of the MSH.
Limitations
There were several limitations to the current study. For the training surveys and third-year resident surveys, the presurvey questions were retrospective, asking participants to answer as if they were responding before completing the training, though they had already participated in the training. The study also relied upon residents who chose to participate in the study. This methodology can contribute to recall and selection bias. The study design would have been strengthened if the presurvey was completed prior to the educational intervention, to evaluate whether learner confidence increased with less inherent bias. A presurvey was not administered due to time and resource requirements necessitated by this methodology.

Another limitation was that only learner confidence was evaluated in the current study, and a true knowledge, skills, and abilities assessment would have required a preintervention and postintervention skills assessment to be objectively evaluated. Further, the questions assessing learner confidence were not developed from a validated scale and rather were developed in conjunction with the LPC Consulting firm utilizing the logic model for program evaluation. The methodology would have been strengthened if validated scales were used. In addition, there was a small response rate for the third-year resident survey, and a sample size/power analysis was not performed. Given these limitations, the generalizability of the current study is limited.
Conclusion
Participating in the MSH program likely benefited the Dignity Health resident physicians meaningfully in the course of their early careers. The current study showed that learner confidence increased after the training sessions and participation in the program as a whole. The MSH was incorporated into residency clinics in order to have a ripple effect of increasing providers who are trained to care for this vulnerable patient population. The results of this study may be suggestive of just that, with multiple graduating third-year residents reporting that they will not only continue using the trauma-informed care model in their future practices, but they will also work to initiate and replicate this training with their future colleagues. It is the authors’ hope that the MSH model will be incorporated into other residency clinics to expand the resources available to victims and survivors of trafficking.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231184013 - Supplemental material for Resident Physician Education in the Human Trafficking Medical Safe Haven
Supplemental material, sj-docx-1-mde-10.1177_23821205231184013 for Resident Physician Education in the Human Trafficking Medical Safe Haven by Kiersten Kelly, Matthew Gibson and Ronald Chambers in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205231184013 - Supplemental material for Resident Physician Education in the Human Trafficking Medical Safe Haven
Supplemental material, sj-docx-2-mde-10.1177_23821205231184013 for Resident Physician Education in the Human Trafficking Medical Safe Haven by Kiersten Kelly, Matthew Gibson and Ronald Chambers in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205231184013 - Supplemental material for Resident Physician Education in the Human Trafficking Medical Safe Haven
Supplemental material, sj-docx-3-mde-10.1177_23821205231184013 for Resident Physician Education in the Human Trafficking Medical Safe Haven by Kiersten Kelly, Matthew Gibson and Ronald Chambers in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205231184013 - Supplemental material for Resident Physician Education in the Human Trafficking Medical Safe Haven
Supplemental material, sj-docx-4-mde-10.1177_23821205231184013 for Resident Physician Education in the Human Trafficking Medical Safe Haven by Kiersten Kelly, Matthew Gibson and Ronald Chambers in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-5-mde-10.1177_23821205231184013 - Supplemental material for Resident Physician Education in the Human Trafficking Medical Safe Haven
Supplemental material, sj-docx-5-mde-10.1177_23821205231184013 for Resident Physician Education in the Human Trafficking Medical Safe Haven by Kiersten Kelly, Matthew Gibson and Ronald Chambers in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
Thank you to the directors and coordinators of the MSH, including Jennifer Cox, Sarah Chaffin, MD, Nancy Nguyen, DO, Duane Bland, MD, Pamela Davis, MD, Christine Woroniecki, MA, and Colleen Warnesky, PsyD. Thank you to Tracey Weld, MS, from LPC Consultants for contributing to the evaluation of the MSH model. Thank you to all of the resident and attending physicians who care for victims and survivors of human trafficking.
Author contributions
Study conception and design: MB & RC; data collection: MG & RC; analysis and interpretation of results: KK & RC; draft manuscript preparation: KK. All authors reviewed the results and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grant funding was obtained through the Department of Justice, Office for Victims of Crime (DOJ OVC) to the Dignity Health Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.