
Abstract
OBJECTIVES
Previous studies have found that the inclusion of medical humanities in medical education was associated with improvements in learner reflectivity and empathy. There is less data, however, on the impact of medical humanities on perceived patient care and mediators of learner outcomes. Our study aimed to determine the impact of medical humanities on perceived learner well-being and patient care, and the mediators of these outcomes in medical undergraduates undergoing psychiatric training.
METHODS
This cross-sectional study was conducted from August 2021 to December 2022 within undergraduate medical students undergoing psychiatry rotations and who attended sessions entitled “Humanities in Psychiatry.” Both quantitative and qualitative data were obtained through anonymized online feedback forms. Path analysis was performed to examine the relationship between learners’ perception of the medical humanities writing activity and its potential to improve their well-being, patient care, as well as mediators of these outcomes.
RESULTS
Overall, 97 medical undergraduates (response rate 67.4%) participated in the study and more than four-fifths reported improvements in listening, reflection, empathy, personal well-being, and perceived patient care. Males showed more interest in additional medical humanities sessions (mean rank 57.9 vs 42.5, P = .005) and greater improvements in personal well-being (mean rank 55.1 vs 44.5, P = .044). Path analysis showed that reflective capacity of learners mediated the relationship between reflective writing and perceived improvements in learner well-being (β = 0.596, 95% CI = 0.409-0.737) and patient care (β = 0.557, 95% CI = 0.379-0.702).
CONCLUSIONS
Our study found that the majority of learners responded positively to the medical humanities sessions, which suggests that its use could be beneficial in fostering empathy, reflection, learner well-being, and improved patient care. Using the PRISM model, we present practical implications for educators to consider when using medical humanities in relation to psychiatry training.
Introduction
Medical humanities is defined broadly as “an interdisciplinary field concerned with understanding the human condition of health and illness to create knowledgeable and sensitive health care providers, patients, and family caregivers.” 1 Of note, while recent reviews have observed the increased introduction of medical humanities (use of literary arts being most common) into the curriculum of health professions education including medical undergraduate education, there are reported gaps in the literature including data on learner assessment and outcome.2–4 Although there are associations between the incorporation of medical humanities and better reflectivity and empathy among the learners, 5 the impact on other learner outcomes including perceived benefit on patient care as well as mediators of the inter-relationships between medical humanities and learner outcomes are less examined.3,4
Earlier studies have highlighted the place of medical humanities in the inclusion of aspects of human experience which can facilitate the learner's reflection and awareness during learning. 6 The promotion of reflective practice had been conducted through expressive writing, 7 poetry, 8 use of comics and photo essay assignment9,10 related to topics in healthcare ranging from social determinants of health 10 to care for individuals with dementia. 8 We previously described the use of stories in the form of narratives within the teaching of topics, including psychotic disorders among medical undergraduates and research ethics within postgraduate learners, and found that medical humanities could enhance engagement, improve appreciation of the content and address underlying motivational factors behind learning and understanding.11,12 Empathy, the ability to understand a patient's personal experience without having to directly bond with them, constitutes an important facet of a clinician's ability to communicate effectively with patients. 13 In a sense, medical humanities shift the focus away from the scientific paradigms of understanding illness, which transcend the individual in an attempt to clarify universal truths, back to the individual human experience of illness, thus allowing the clinician to share in the experience of the patient's illness in a meaningful way.14,15 A recent quasi-experimental study of medical interns, in which those who participated in medical humanities sessions were compared to those who did not, found that empathy scores increased significantly in the former group, both post-test and in comparison with the latter group. 16 In another recent study by Liao and Wang, a group of students from a variety of backgrounds in healthcare underwent a medical humanities program, where they were allowed to discuss and reflect on ethical/moral dilemmas seen in stories, novels, dramas, or films. 17 This group was then compared to a control group who did not undergo such an intervention and the former group had higher post-test scores in “behavioral” and “affective” empathy. Huang et al, in their qualitative study, also found empathy to be a prominent theme in the reflections of medical undergraduates within a medical humanities program. 18
However, there is less literature on the perceived impact of medical humanities programs on patient care, as reported by learners or other observers. Although the use of medical humanities has also been associated with better learner well-being,19,20 the mediators of this relationship have not been sufficiently explored. Thus, our study aimed to study the learner feedback on the incorporation of medical humanities teaching within medical undergraduate students undergoing their clinical psychiatry rotations, specifically pertaining to promotion of reflection, empathy, perceived effect on learner well-being, patient care as well as the mediators of these learner outcomes.
Methods
Nature of the study
This was a cross-sectional study conducted with a mixed methods research model, collecting both quantitative and qualitative data for analysis. Specific aspects of our methodology are highlighted below. We used the STROBE cross-sectional checklist when writing our report. 21
Participants and training session
This cross-sectional study was conducted from August 2021 to December 2022. Batches of 4th-year undergraduate medical students (total course duration being 5 years) from the Yong Loo Lin School of Medicine at the National University of Singapore undergo a psychiatry rotation lasting 6 weeks that comprises generally of 3 weeks of academic teaching at the University, and 3 weeks of clinical attachment at a tertiary psychiatric hospital and/or department of psychological medicine at a general hospital setting. Since August 2021, those undergraduate medical students who completed a psychiatry rotation at the Institute of Mental Health would also be scheduled to attend a 90-min teaching session entitled “Humanities in Psychiatry” in their last week of clinical attachment.
The sessions were conducted via teleconferencing medium during Covid-19 pandemic and then converted to onsite format when the pandemic improved. Each session was facilitated by a senior psychiatrist following a format comprising of sharing of a narrative, close reading and reflective writing.22,23 First, each session commenced with an introduction of a short prose by the facilitator, with students invited to take turns to read the narrative piece aloud in the session. Narrative pieces were curated based on their content involving human experience of psychological conflict or distress and with relevance to learning and caring in medicine. Sources of such prose included the reflection sections of major medical journals such as Piece of My Mind in Journal of American Medical Association (JAMA), Art of Medicine in Lancet, Perspective in JAMA Internal Medicine, and From the Heart in JAMA Cardiology. Second, the learners participated in a close reading drill to hone their sensitivity to the stories read. The close reading drill included consideration of 5 important aspects of any prose, such as the frame (who wrote this, where, when, and why was it written), form (such as visible structure, metaphor, allusion etc), timeline, plot (storyline, main events), and desire (such as sources of motivation that enable or obstruct the reader from engaging) of the prose. Time was then allowed for participants to reflect upon the piece, with the facilitator then inviting them to share their reflections about the prose and how it related to their experience of learning about psychiatry and caring of patients during the clinical attachment. Third, the participants were encouraged to write a short reflection on the session which they were welcomed to share before the facilitator brought the session to a close. This reflective writing exercise was unstructured, though participants were encouraged to share how they felt not only about the session, but about what specifically resonated with them, and what they felt was meaningful to their learning and patient care in psychiatry. Participants were encouraged to actually engage in the act of writing after spending some time in reflection. The above steps in the session are highlighted in Table 1.
Steps in HIP session.

Data collection
At the end of the session, participants were invited to provide anonymized feedback on the session. This was done via an online form which was administered by an administrative staff from the Education Office who was not involved in the evaluation of the learners. The items on the feedback form comprised of several questions about the session (such as whether the session helps the learner to listen better to the story of narrator, reflect better on patient care, enhance empathy, whether writing during the session was cathartic, whether the session can improve personal well-being and patient care) which were rated on a 5-point Likert scale (from strongly disagree to strongly agree). In addition, qualitative feedback on the session was also obtained. The responses of all participants who responded to the survey were included, and there was no exclusion criteria. The study was approved as an exempt study by the Institutional Review Board of the National Healthcare Group, Singapore (NHG DSRB Ref: 2014/00422).
Data analyses
We used SPSS Version 22 for statistical analyses. We examined the distribution of responses for all questions among the learners, as well as the correlation between these items. We also explored the difference in responses between genders, if any, using a Mann–Whitney U test. We used SmartPLS v.3.3.5 for path analysis. 24 We examined the relationship between learners’ perception of the writing activity and its potential to improve their well-being, patient care, as well as mediators of these outcomes. The items related to the session's ability to enhance empathy, and to encourage reflection about patient care were entered as mediators in the partial least squares structural equation (PLS-SEM) model. We used bootstrapping with subsamples to determine the significance of indirect paths in the model. For qualitative data, themes were identified by the authors by analyzing the responses to the open-ended questions in the survey by the participants, based on similarities in word usage and phrasing as well as content expressed. The themes identified individually by each author were discussed by the co-authors as a group, before deciding on the final 3 top themes.
Results
Overall, a total of 97 out of 144 (response rate 67.4%) undergraduate medical students in their 4th year of training participated in the study. More than four-fifths of the respondents agreed/strongly agreed that the session was helpful for their learning in various ways, for example, listening better to narrator (84.5%, n = 82), reflecting better on patient care (89.6%, n = 87), enhancing empathy (83.5%, n = 81), improving personal well-being (82.5%, n = 80), improving patient care (87.7%, n = 85). Separately, 71.2% (n = 69) of the participants expressed that the cathartic experience of the writing activity was helpful.
Of note, there was a significant difference between the genders on 2 items of the questionnaire. Male learners indicated significantly more interest in having more medical humanities sessions (P < .01), and had more positive perception of the session's potential to improve their personal well-being compared to female learners (P < .05) (Table 2).
Comparison between genders (Mann–Whitney U test).

*P < .05.
In terms of path analysis, the indicator loadings for the latent variable (learners’ reflective capacity) formed by their perception of session's ability to encourage reflection on patient care and enhance empathy were 0.954 and 0.951, respectively. The specific indirect path from writing as a cathartic activity to its potential to improve learner well-being through enhancing the learners’ reflective capacity was significant (β = 0.596, 95% CI = 0.409-0.737). The specific indirect path from writing as a cathartic activity to its potential to improve patient care through encouraging reflection was also significant (β = 0.557, 95% CI = 0.379-0.702) (Figure 1).
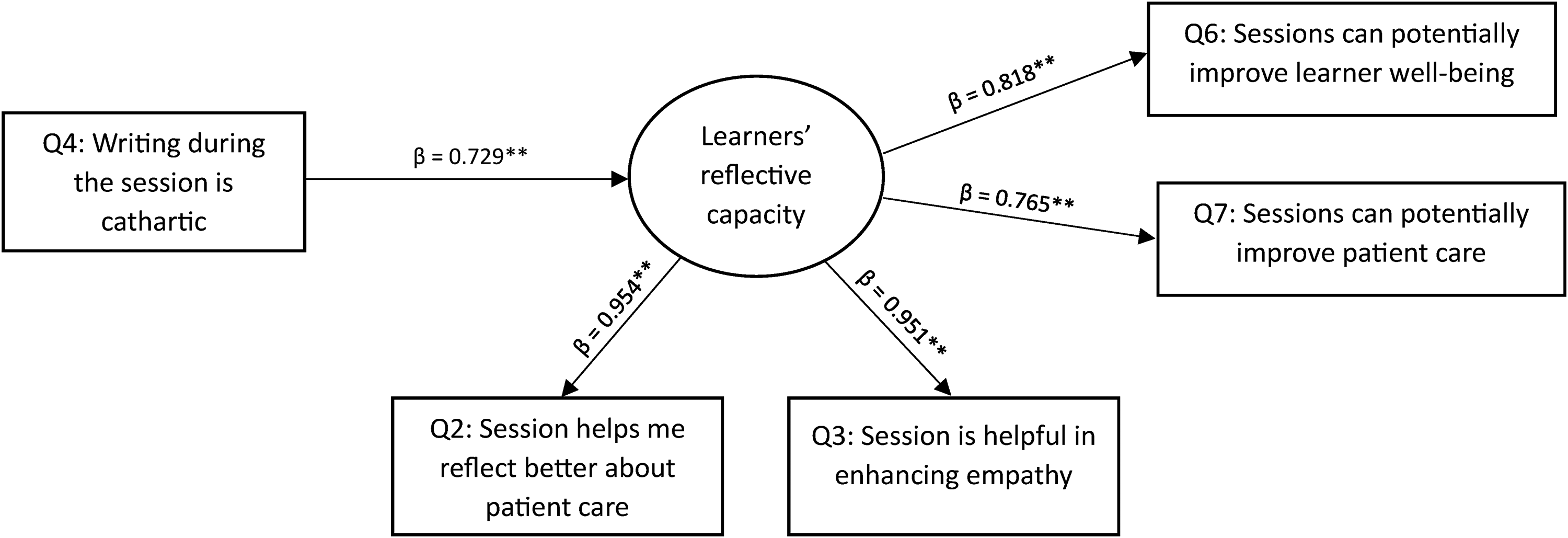
Path analysis.
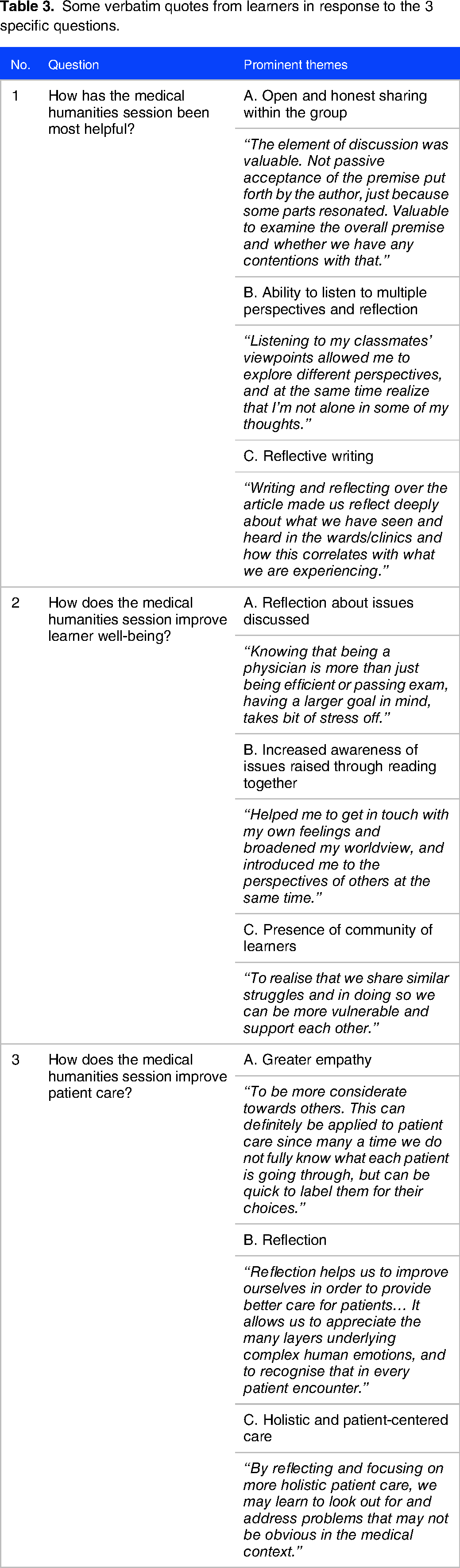
In addition, the qualitative comments to 3 specific questions revealed relevant themes (Table 3). For the question regarding how the medical humanities session had been most helpful, the 3 top themes were open and honest sharing within the group, ability to listen to multiple perspectives and reflection on thoughts shared, as well as reflective writing. This challenged learners to be open to different viewpoints, and to relate their learning to clinical practice. For the question related to how the medical humanities session can improve learner well-being, the 3 top themes related to reflection about issues discussed, increased awareness of issues raised through reading together, and presence of a community of learners. Learners reported better emotional awareness, and helped them to realize that they were not alone in the struggles they faced. It also allowed them to take a step back and evaluate their reason for pursuing medicine. For the question regarding how the medical humanities session can improve patient care, the 3 top themes pertained to greater empathy, reflection, and need for holistic and patient-centered care. Learners reflected a deeper understanding of the unspoken difficulties that patients may be going through, and demonstrated better awareness of a patient's psychosocial needs that may often be neglected in the medical context.
Some verbatim quotes from learners in response to the 3 specific questions.
In terms of negative responses, Table 4 highlights some of the negative responses to the medical humanities program in the survey. Regarding qualitative feedback, only one of the participants reflected that the HIP session was “not helpful” in terms of the specific questions asked (as seen in Table 3).
Negative responses to humanities in psychiatry (HIP).

Discussion
There are several findings in this study. First, the majority (more than 80%) of medical undergraduates responded positively regarding the session on “Humanities in Psychiatry” for their personal growth (better empathy, reflection), learner well-being and clinical care (perceived better patient care) during training. While there were some negative responses, these were a small minority, ranging between 3% and 13% of respondents for the individual questions. Second, we found that the reflective capacity of the learner mediated the relationship between the writing activity at the end of the session and perceived improvements in learner well-being and patient care. The above findings were supported by the prominent themes from the qualitative comments. Third, male learners had more positive perception of the session's potential to improve their own well-being and indicated greater interest in having more sessions.
The findings of our study add to the growing evidence supporting the use of medical humanities in fostering empathy and reflective practice in medical undergraduate training. An earlier study of the determinants of empathy among medical undergraduates found that time spent in medical humanities among other activities was correlated with higher empathy scores. 25 Apart from previous reviews,2,3 recent studies have found objective improvements in empathy scores with the use of medical humanities in medical training.26,27 One of the concerns regarding clinical practice is the phenomenon of “ethical erosion,” in which clinicians experience a decline in empathy as they begin their careers. 28 Given the benefit of medical humanities in fostering empathy, there is a greater role for its place within medical training, in order to combat this phenomenon. Charon suggested that the use of medical humanities fosters empathy in readers through the practice of reflection 14 and this can occur in the context of listening to multiple perspectives, sharing, and expressive writing within the community of learners as seen within the qualitative comments.
In our study, participants also indicated improved personal wellbeing after going through the medical humanities session. This finding corroborated previous evidence that narrative medicine programs can help to improve wellbeing in medical training.5,19 A recent study of third-year medical students in Florida found that even a brief narrative medicine session (in this case a small-group sharing session and written assignment) enabled these students to identify strategies to improve their own wellbeing. 29 In addition, the path analysis showed that reflective capacity mediated the relationship between writing and learner well-being. A systematic review by Chen et al in 2014 found that the act of reflective writing was associated with significant improvements in empathy and reflectivity. 30 In this regard, the reflective writing allowed participants to get in touch with their own emotions, and the ensuing catharsis could account for the perceived improvement in well-being.31,32 Concurrently, the improved empathy and reflectivity arising from the session is not just experienced internally but interpersonally among the community of learners (as seen in the qualitative themes) which can contribute towards improved learner wellbeing.
We also found that reflective capacity mediated the relationship between reflective writing and perceived better patient care. While there is evidence supporting the role of medical humanities in fostering empathy10,17,18 and the association between empathy and improved patient care,33–35 there is less research into whether the use of medical humanities directly impacts patient care, though some theories as to how this might be achieved have been proposed. Building on the work of Charon, 14 Lapite proposed that by fostering empathy for patients, medical humanities help to improve the clinician–patient relationship. 36 Rosti suggests that medical humanities not only improves communication of clinicians with their patients, but can also help clinicians to supplement objective assessments with the subjective experiences of patients (such as experience of loss, pain, disappointment, different emotions), which can facilitate better treatment. 37 This is particularly important in the field of psychiatry where objective assessments are often inadequate in fully capturing the internal experiences and difficulties of the individual. It is conceivable that the specific act of expressive writing allows participants to reflect about their own personal experiences and emotional responses vis-a-vis the content and context of the narrative, which then allows for contextualization to patient care in their training. 7
In our study we found that male learners had better perceived improvement in their well-being and indicated greater interest in having more sessions. This was in contrast with study by Chen et al. 30 which reported that female learners experienced a greater initial improvement in empathy scores after undergoing a medical humanities program, although the empathy scores of male learners eventually caught up over time. 26 Chen and colleagues suggested that initially, male learners may take a longer time to digest the emotional experiences within the medical humanities session but subsequently improved in their capacity to empathize. 26 Conducting the medical humanities session via a teleconferencing platform may lessen concerns and discomfort of open and vulnerable sharing in a bigger group, promote empathy and reflection via reflective writing activities, with better learner wellbeing and desirability for more sessions as a result. It is also possible that the male participants found medical humanities to be more novel than the female participants, which could account for more positive responses to the program. The role of gender, as well as other socio-cultural factors, in the perception of medical humanities certainly warrants further investigation.
Practical implications
Using the PRISM 38 model for considering the functions of medical humanities in the context of medical undergraduate training in psychiatry together with our study findings, there are several practical implications. This model provides pedagogical flexibility in considering 4 functions of medical humanities in health professions education which are elaborated below. The PRISM model considers 4 main functions of the arts and humanities: as expertise (used for mastering skills), as dialogue (used for perspective taking, and relational goals), as transformation (used for personal insight and growth), and as expression (used for activism). 38 Here, we focus on the soft skill learning domain of compassion in psychiatry training as an example. First, in the area of mastering of skills, educators need to carefully curate materials used during such medical humanities sessions to focus on the learner's journey and compassionate patient care. We can broaden the content (covering medical contexts within and outside psychiatry) and genre (prose, novella, poetry, even other mediums such as visual arts) covered to expand the scope and horizons of discussion about the importance of compassion in psychiatry. Second, in the area of perspective taking, educators can use medical humanities to encourage understanding of alternative viewpoints via listening, reflection, reflective writing, and sharing with other learners. This was evident in the prominent theme of reflection being mentioned in the qualitative comments as a key internal activity and element in fostering better perceived patient care. Third, in the area of personal insight, medical humanities can be adopted to encourage reflection about compassion towards others and self. This in turn underscores the importance of self-care and learner well-being in training. Fourth, in the area of social advocacy, educators can use medical humanities to engender critical reflection about the place of the person in an ever-evolving healthcare system including psychiatric care. This can prompt consideration of issues such as person-centered care, holistic care, and reasons behind observed disparities in clinical care.
Limitations
There were several limitations in this study. First, the sample size was relatively small and power calculation was not performed. Second, it is possible that, as the medical humanities sessions were recently added to the curriculum, it is something different and a break from traditional didactics within medical undergraduate school teaching. Hence, the medical humanities session could have been perceived in a positive light by some of the participants more for its novelty, rather than its inherent value in fostering listening, reflection, and empathy. Third, we did not include previously pilot tested or validated rating scales and the employment of such formal scales to measure outcomes such as empathy could be used to supplement the learner feedback obtained from our study. Fourth, the cross-sectional nature of the study, and the implementation of a single medical humanities session, rather than multiple sessions, preclude conclusions about whether perceived improved empathy, reflection, learner wellbeing and patient care would be sustained over time. Fifth, we did not include a control group. Sixth, the prose used in the sessions was mainly of western origin, and we did not explore the impact of our participants’ individual cultural backgrounds and perspectives on their experience of the prose and the session. This could have had an impact on their survey responses. Finally, our results reflect subjective improvements as experienced by the participants, and future studies can look into further translation into observed patient outcomes.
Conclusions
Our study highlighted the value of medical humanities in fostering reflectivity, empathy, and perceived improvements in learner wellbeing and patient care within medical undergraduates in psychiatry training. Future sessions and studies may want look into the use of medical humanities in addressing specific issues within psychiatry training using different pedagogical lenses which relate to various functions of medical humanities, and evaluate longer term outcomes within learners and their practice in patient care.
Footnotes
Acknowledgments
The authors would like to thank all the participants for taking part in this study. They also like to acknowledge the staff of our Education Office for administering the surveys to the participants and collating the responses.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent statement
The study was approved as an exempt study by the Institutional Review Board of the National Healthcare Group, Singapore (NHG DSRB Ref: 2014/00422). The requirement of informed consent was waived.