
Abstract
Background
With a growing population of older people in all Western countries, interprofessional education (IPE) can help to prepare students for the complex care for these patients. Which aspects of this complex care could benefit from IPE? In this study we evaluated the differences in content of health care plans made by students who participated in IPE.
Methods
Undergraduate nursing and medical students were included and attended four sessions in which they wrote a health care plan for a paper-based geriatric patient case. Approximately half of the students were included in the IPE-group. To evaluate the content of interprofessional collaboration between the students, the other half of the students were included in a ‘uniprofessional education’ (UPE) group. UPE-students made the health care plan alone. In the IPE-group a medical and a nursing students compiled the health care plan together. All health care plans were assessed by comparing them with a validated health care plan. We zoomed into the differences in the content of the health care plans, and calculated a score ratio, proportion of correct items.
Results
The health care plans made by IPE-students had an average score ratio of 0.31. The health care plans made by UPE-students had an average score ratio of 0.22. Most differences were found in the subcategories medication, nursing actions and aftercare. Specific items within these categories were more frequently thought of in the IPE-group than in the UPE-group, for example delirium interventions and consultation with a transfer nurse.
Conclusion
This study gives insights into which health care actions are more often considered by interprofessional couples in IPE than by students in UPE. Awareness of these items in clinical practice could make a difference in the care for older patients.
Keywords
Background
In all Western countries the population is aging. The number of people over 65 years old will be doubled in 2050 and the proportion of people over 80 years old will increase.1–4 Most patients over 65 years old, that are admitted in hospitals, have complex health care issues and multimorbidity.5–7 Governments are struggling with the costs and the shortage of health care professionals that accompany this increase in health care complexity and consumption. Collaboration between different disciplines can improve healthcare processes and outcomes for geriatric syndromes.8,9 The World Health Organization suggests that interprofessional education (IPE) and collaborative practice is one of the most promising solutions to the worldwide shortage of 4.3 million healthcare workers. 10 Besides, IPE could prepare students to care for older adults with complex needs.9,11 IPE is defined as “when two or more professions learn about, from and with each other to enable effective collaboration and improve health outcomes”. 10
In the last decades there has been a growing interest in IPE and it's evaluation. 12 The effects of IPE interventions can be classified according to the modified Kirkpatrick levels for learner outcomes, defined by Barr et al: (1) Reaction; (2a) Modification of attitudes/perceptions; (2b) Acquisition of knowledge/skills; (3) Behavioural change; (4a) Change in organisational practice; (4b) Benefits to patients.13,14 Most IPE studies focus on the first 3 levels, for example feelings towards IPE or readiness for IPE, or collaborations-skills. 12 Effects on patient care (level 4b) are of course the most desirable effects of an IPE initiative, but those effects are also the most difficult to measure. Additionally, it could be useful to investigate which aspects of patient care improve due to IPE interactions. Comprehension about this could shape the content of education, interprofessional as well as ‘uniprofessional’: Do students in IPE think of different topics while considering the care for older patients, than students in a uniprofessional setting? More attention to specific topics may decrease the risk of complications or high costs.
Thus, our research question was:
What are the differences in the content of the health care plans for older patients of nursing and medical students in uniprofessional versus interprofessional education, especially in the subcategories: diagnostics, medication, consulting different specialists, nursing actions and aftercare?
Materials and methods
Research design
Between March 2018 and February 2020 we conducted a comparative mixed method study. In this study we used written health care plans in classroom education to reflect ‘patient care’ in clinical practice, level 4b of the modified Kirkpatrick levels. The content of health care plans for older patients, written by the students who participate in IPE, was compared with health care plans written by students in uniprofessional education (UPE) (Figure 1). Although we realize that comparing students together with students alone can create a bias, we chose the UPE group because uniprofessional education is still the standard in most curricula. Besides, a professional working in clinical practice is often working solo. We emphasize we looked at the differences in content of the health care plans – not if one is better than the other.

Research design.
Setting and participants
This study is conducted at the Northwest Academy: the educational institute of the Northwest Clinics in Alkmaar, the Netherlands. Undergraduate medical and nursing students without prior interprofessional training experience were included. The nursing students were in their third year of a four-year educational program in which classroom education alternates with participation in clinical practice. All groups in that stage of their education program at our facility between March 2018 and March 2019 were included in the study, which meant three groups of nursing students. Assignment to the IPE- or UPE-group took place at the first session. The nursing students were individually randomly (alphabetically) assigned to the IPE- or UPE-group.
The medical students were starting their master's program, after finishing a 3-year bachelor's program. The master's program consists of different clerkships. Every six weeks a group of maximum 9 students started their clerkships at the Northwest Academy. All students of all groups that started between March 2018 and March 2019 were asked if they would like to participate in the study. Assignment to the IPE- or UPE-group took place at the first session. Before assigning them to one of the two groups, their schedule was evaluated for a match with the nursing students’ program at all sessions. If there were sessions, for example during holiday breaks of the nursing education program during which the medical students could not collaborate with nursing students, the whole group of medical students was assigned to the UPE-group.
Between the research sessions, the students attended their scheduled internships at different hospitals.
Assignment
All students attended four sessions IPE or UPE over the period of one year. During each session the students wrote a health care plan for a paper-based geriatric patient case. Four cases were constructed with the involvement of different experts (eg, clinical specialists, nurses, general practitioners), to ensure that perspectives from the different care-givers were well-represented. 15 The four patient cases had an increasing level of difficulty to match students’ progression in their studies. A patient case included information about the patient's background, medication, description of the current health problem, social and functional status and some results from a physical examination.
Students were asked to draw up a health care plan ‘like they would in clinical practice’. They were allowed the use of books or guidelines, but were not allowed to discuss with others (except their assigned partner if they were in the IPE-group). In the instructions the students were suggested to think of diagnostics, medication, consultation of different specialists, nursing interventions and ‘to-do’ tasks before discharge. The first patient case is visible in the Supplementary Files, as an example (Supplementary file 1 – Case one). All students, nursing and medical, had had practice and teaching about how to write a care plan in their regular educational program, before entering the study.
In the UPE group, students wrote their health care plans on their own. In the IPE group, the health care plans were written by randomly paired medical and nursing students. In each session different pairs were assembled to create diversity among the collaboration partners and their input.
The IPE group was placed in a different (class)room, separate from the UPE group. A researcher or research assistant supervised the students for identifying (non-)collaboration and was available to answer procedural questions.
To ensure confidentiality, all treatment plans were filled out with research identification numbers. Students worked out their treatment plans in a word-document which was sent by the researcher, so that the their identity was secured in the file properties.
To minimize students’ effort, all sessions of all different groups were scheduled in the regular time of the students’ educational program. Other educational obligations such as upcoming examinations were taken into account while planning the sessions. The scheduled time for the assignment was 45 min. To thank the students for their effort, cookies were offered to all students during each session.
Assessment of the health care plans
All health care plans drawn up by the students were first coded by a research assistant to blind the researchers towards the UPE and IPE group status.
Subsequently the plans were assessed by comparing them with validated health care plans formulated by the same experts that were also involved in the case construction. 15 For the four cases, experts agreed upon a list of actions that would be appropriate to carry out for such a patient. Each validated plan consisted of 20 (case 1, least complicated) to 30 items (case 4, most complicated). The items were scored as either present (1) or not present (0) in a student's health care plan.
All plans were assessed by the same person (author 1). Uncertainties in the identification of present or absent items were discussed with educational and clinical specialists after assessing the first 10 plans of each case. Subsequently the first 10 plans were reassessed by author 1 in consideration with the input of the educational and clinical specialists. After consistency was found in the assessment (intra-rater reliability of 1.00), all other plans were assessed. During the assessment of the health care plans it was sometimes necessary to fine-tune the boundaries to consider an item correct (1 point) or incorrect (0 points). If boundaries were adjusted, all care plans were reassessed for that specific item.
Ratios and scores
To make the total number of identified items between groups and cases comparable, ratios were calculated. Each care plan had a different total number of items: case 1 = 20 items, case 2 = 24 items, case 3 = 29 items and case 4 = 30 items. Score ratios were the proportion of actions identified, and were calculated by dividing how many items a student was able to identify, by the total number of items of that case. For example, if a student identified 8 items for case 1 (case 1 has 20 items), then the score ratio is 8/20 = 0.4.
The maximum number of items within each category (as a total of case 1 to 4) were also unequal: Additional research = 31, Medication = 10, Consultations = 11, Nursing actions = 46, To-do before discharge = 5. To compare the proportions between categories, we also calculated score ratios: score ratio = number of identified items/total number of items in that category.
Figure 2 depicts the procedure of assessment of the health care plans.

Health care plan assessment.
Statistical analysis
SPSS version 28.0.0.0 was used to process and analyse the results. The mean score ratios of the IPE and UPE group were compared. In case of normally distributed score ratios, independent samples T-test was used. In case of non-normally distributed score ratios, Mann-Whitney-U test was used. The score ratios of each category (diagnostics, medication, consultation of different specialists, nursing interventions and to-do before discharge) as a total of case 1 to 4 were also computed. Chi-square analysis was used to compare the scores of the UPE- and IPE-group for each single item in all of the four cases.
Results
Participants
A total of 135 students were included in this study. Six students dropped out because they quit their education or were not present during the sessions. Table 1 depicts the characteristics of the UPE and IPE groups. The groups did not differ in age or gender prior to the research.
Student characteristics.

Not every student was present in all of the four sessions, and sometimes, because of an incomplete IPE-couple, a student from the UPE-group joined the IPE-group or vice versa. Three students switched for one session to the UPE group and four students switched for one session to the IPE group. Table 1 depicts the group to which students were assigned and in which they participated for most of the sessions.
Because not every student was present during all four sessions, the number of finished health care plans varied between 56 and 71 in the UPE-group. In the IPE-group the number of health care plans varied between 29 and 30. In the supplementary files, there is an overview of all included students in each group and all drop-outs (Supplementary file 2 – Overview of students’ numbers).
Sessions
On an average students completed the assignment between 10 to 30 min. During supervision it was clear that all couples were collaborating during their assignment. All students in the UPE group were quietly working alone on their assignment.
One session couldn’t be scheduled in regular time. That was the only session in this study for which we asked students to come to school.
Mean score ratios of the health care plans
Table 2 depicts the mean score ratios in each group (UPE or IPE) of each care plan.
Mean score ratios for each plan.

Mean score ratios per category
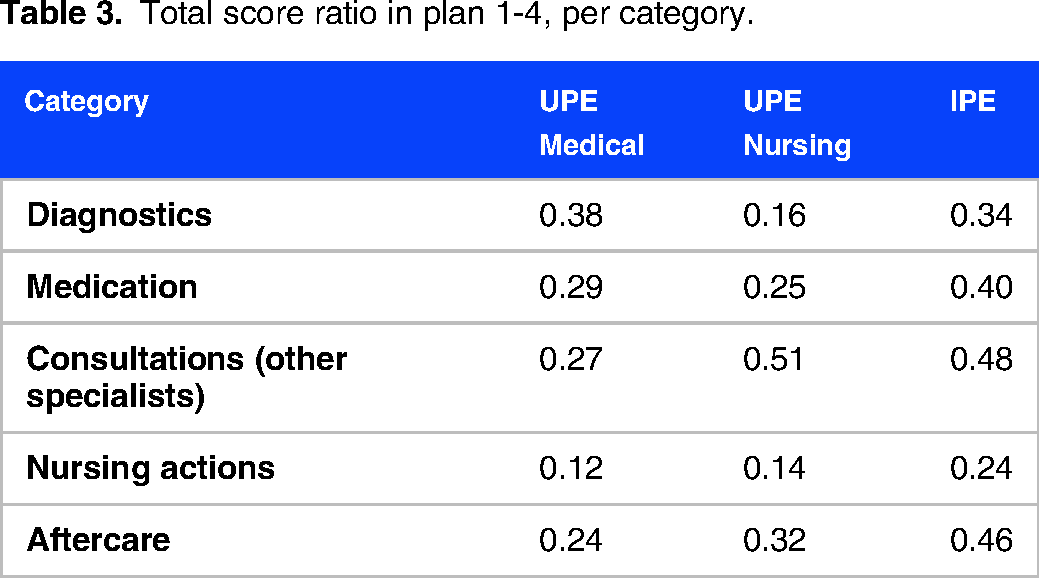
Table 3 depicts the score ratios of the different categories in the health care plans 1 to 4. In the UPE-group we expected different scores between the medical students and nursing students in different categories, because of different expertise, so both groups are shown separately.
Total score ratio in plan 1-4, per category.
Differences in specific items
Table 4 depicts the frequency of all items of cases 1 to 4 which had a significantly different frequency between the UPE- and IPE-group. The percentages depict the proportions of health care plans which contained that specific item.
The frequency of the items in health care plans 1 to 4 which had a significantly different frequency between the UPE- and IPE-group.

*P < .05, P < .001**.
A Supplementary File with all items of the health care plans is provided (Supplementary file 3 – Results of all items in each case).
The four plans contained a total of 103 items. Four items were not written down by any of the students. Within the other 99 items, there is a spread of 1% to 100% of the students that identified a specific item.
Twenty items were significantly more often identified by the IPE-group than by the UPE-group. There were no items more often identified by the UPE-group than the IPE-group.
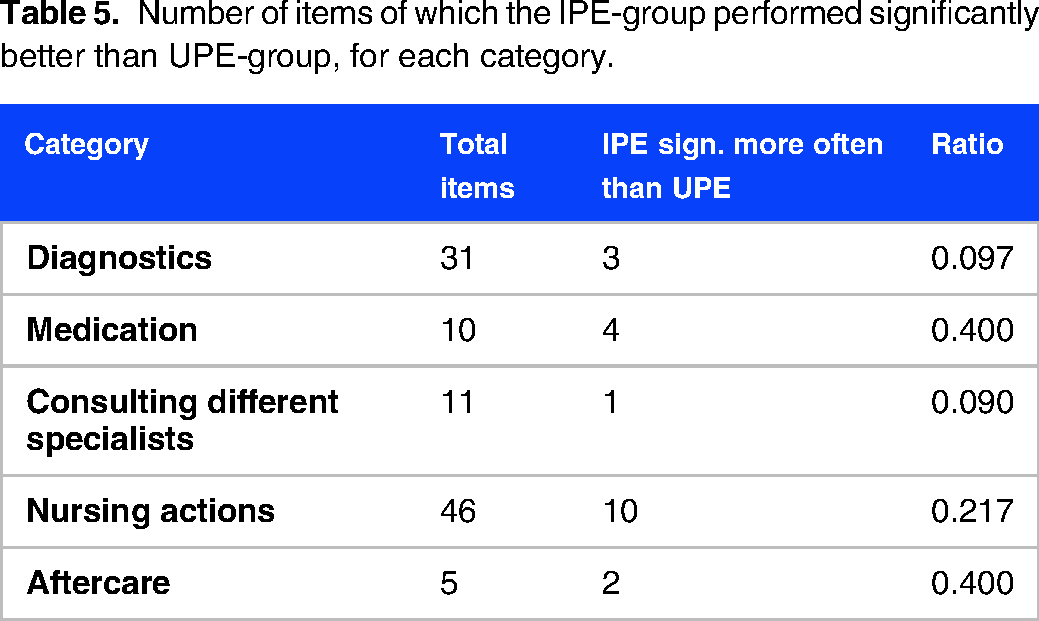
The 20 items, that the IPE-group identified significantly more often than the UPE-group, are spread over the five different categories unequally. Table 5 shows to which category the items belong. To see which category has the largest proportion of items on which IPE-plans score higher than UPE-plans, ratios were calculated, which are depicted in the last column in Table 5.
Number of items of which the IPE-group performed significantly better than UPE-group, for each category.
Discussion
This study explored the differences in content of health care plans of students in interprofessional education versus those of students in an uniprofessional setting. The IPE health care plans had significantly higher score ratios than the UPE health care plans, which means that the IPE health care plans consisted of more correct items than the UPE health care plans. In our earlier research, we were unable to validate the assessment of the standard health care plan because of a lack of agreement between experts. 15 For this reason we advise caution in concluding that the plans of the IPE group were better than the plans of the UPE group. Variation in assessment of different experts is a well-known issue. 16 Nevertheless we can conclude that IPE couples were able to write down more correct items than UPE students. This could possibly lead to more correct actions for a real patient in clinical practice.
In this study twenty out of a total of 103 items were significantly identified more in one group than in the other. All twenty items were in favor of the IPE group. These items were found in all of the five subcategories: diagnostics, medication, consulting different specialists, nursing actions and aftercare. The categories medication, nursing actions and aftercare had the highest ratio of significantly different items.
When zooming into each category, some remarkable differences were found. First, some standard nursing actions like EWS, NRS and SNAQ are more often identified in an IPE plan than in an UPE plan. Medical students in the UPE-group might not have knowledge of these items. Nursing students should be aware of these standard actions, since they perform them every day. However, when writing down the assignment alone, they seemed to forget to make it explicit, while with the IPE couples, these actions were discussed with students that weren’t familiar with them (medical students) and are therefore made explicit. This exchange of discipline specific knowledge is reported in the literature as one of the main outcomes of IPE.17–19 Second, delirium interventions and DOS-scores were also significantly more often mentioned in an IPE plan than in an UPE plan. This is an important finding for the prevention and early recognition of delirium, which is major problem in hospitalized older patients. 20 The DOS is a delirium screening tool which is validated for hospitalized older adults. 21 Education around delirium and screening has already been shown to improve knowledge and correct evaluation of delirium. 22 This study shows how interprofessional collaboration can also improve the awareness around delirium screening.
The proportion of items that were significantly more often identified in IPE plans than in UPE plans is also high in the ‘medication’ category: in 4 out of 10 items the IPE group identified the item significantly more often than the UPE group. Apparently when medical students and nursing students discuss a case together, they think about medication more often, or they more often write down the right medication actions. This is consistent with the literature about how IPE programs can improve medication knowledge in health professionals and reduce medication errors in hospitalized patients.23–25 This is an important finding since polypharmacy is major topic in elderly patients. 26
The last category which showed the highest ratio of significantly different items was the ‘aftercare’ category. Although this category contained very few items (5 in total of the four care plans), IPE couples seem to think more often about arrangements and the care which is necessary to discharge a patient from the hospital than UPE students. When these arrangements and care are adequately tackled, it can have a direct influence on improving patient wellbeing and reducing health care costs. 27 IPE or better interprofessional collaboration in clinical practice may have, for that reason, a positive influence on reducing health care expenses.
The score ratios in the ‘consultations’ category were not better in the IPE group than in the UPE group. This is in contrast to earlier research by Sanders et al, 28 where students reported better knowledge about referring to other disciplines after IPE.
Overall, all students scored relatively low ratios on all four cases, between 0.20 and 0.34. This could be due to different reasons. First, the health care plan which was used to compare the students’ plans with, should not be seen as “an answer key to a test”, where one expects the best students to score near 90% or 100%. The validated health care plan was a compilation of plans of different specialists and should be interpreted as a list of things you could do ‘right for this patient’. Students wrote down some of these items, and were ‘rewarded’ for each right item, but students at this stage may not be capable of having oversight for all items. Therefore, we did not expect students to get a total ratio of 1. To better interpret the level of students’ knowledge and skills compared to the standard health care plan, 13 residents were asked to write health care plans for case 4. Their mean ratio was 0.27, while the UPE group scored 0.22 and the IPE group scored 0.30. Therefore we conclude that the low ratios were not due to our sample, but mainly due to the ‘procedure’: the high standard and the way of assessing. This leads to the second possible reason: the assessment of the care plans may have been too strict. For example, when students had written down ‘delirium interventions’, without examples or specifications, there were no points given. In educational settings teachers try to train students to be more specific and explain what they mean, to ensure that they have an understanding of what they write down. In clinical practice there would probably be questions asked about a vague formulation and the item would be specified and executed. If assessed more leniently, the scores would have been higher. This did not matter while comparing the scores as all plans were assessed in the same way and in a blinded manner. Third, students commented that they would have appreciated receiving feedback after each assignment. Because the sessions about case 1 were spread over a one-year period, and all treatment plans of 1 case were assessed at the same time when all sessions were completed to ensure consistency in the assessment, it was not possible to give feedback to each student individually between each assignment. If feedback had been provided, the scores may have been higher.
The insights generated by this study can help to shape future case-based IPE to enhance the quality of students’ health care plans. Directly before a session a teacher can provide information on how to formulate health care plans, and also make the different perspectives of nursing and medical students more explicit. Afterwards the health care plans should be assessed within a short period and students should receive feedback before writing the next health care plan. Differences between writing it on your own or with someone from a different profession can also be discussed with students, to make the different perspectives more comprehensible and make students appreciate the other one's view. These would be our recommendations to set up case-based IPE in order to enhance the quality of health care plans.
Study limitations
This study is subject to limitations. First the couples worked on the health care plan together, while in the uniprofessional group the students worked on the assignment alone. As mentioned in the methods section, we chose this solo assignment in the uniprofessional group, because it best reflects standard education (being mostly uniprofessional) and standard clinical practice. Another methodological option could have been to pair up two students of the same profession to work on the health care plan. This collaboration between two students of the same profession was not investigated, and seemed less relevant, since professionals more often work on health care plans alone. They might discuss their plans during hand-offs and Multidisciplinary Team Meetings, but we believe the dynamics in these discussions are different from the dynamics we investigated. Although theoretically two students may come up with more points than an individual student, our study focused on the actual differences between the plans and not only on the quantitative scores. Uniprofessional collaboration may have also improved the plans, but since there is no knowledge transfer in uniprofessional setting, it is questionable if UPE-couples would identify the same items as IPE-couples in this study. Within the UPE- and IPE-groups, 7 students could have benefitted from some knowledge transfer, because they switched between the two groups for a single session. The three students that worked on a health care plan alone for one session might have learned something from previous IPE-sessions. The four students that joined the IPE group for once, might have learned something from that session and transferred that to the next UPE-session(s) four months later. Nevertheless, we don’t think this lead to bias in our results, because it is a small number of students, it was only one session, and each patient case was different.
Second, when interprofessional couples were collaborating about the treatment plans, overhearing conversations of other couples was not ruled out. To minimize this effect, couples were placed away from others as much as possible, also using workplaces outside of the classroom and at the library. The researcher and research assistants that supervised the sessions facilitated other workplaces and enough space between couples.
Third, this study was conducted in a classroom setting, so we don’t know if the same results could be attained with real patients in clinical practice.
Last, we did not perform a power analysis prior to this study. With no existing literature on the content of students’ health care plans to base our power analysis on, we deemed a power analysis uninformative.
Conclusion
This study highlights the differences in content of health care plans for older patients between students in interprofessional and uniprofessional setting. In some topics students lack knowledge and capability. Additional attention to these topics in education could make a difference for patients in clinical practice, but future research about that topic is necessary. For educational practice, we can conclude that working together with another profession can help students to make his/her own actions more explicit. It helps them to formulate more complete health care plans. This could facilitate learning about diagnostics, medication, treatment and care options for patients.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241283304 - Supplemental material for The Differences in Content of Health Care Plans of Medical and Nursing Students in Interprofessional and Uniprofessional Education
Supplemental material, sj-docx-1-mde-10.1177_23821205241283304 for The Differences in Content of Health Care Plans of Medical and Nursing Students in Interprofessional and Uniprofessional Education by Carolyn Teuwen, Hanke Scheffer, Suheda Sekmen-Algin, Rashmi A. Kusurkar, Hermien Schreurs, Hester Daelmans and Saskia Peerdeman in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241283304 - Supplemental material for The Differences in Content of Health Care Plans of Medical and Nursing Students in Interprofessional and Uniprofessional Education
Supplemental material, sj-docx-2-mde-10.1177_23821205241283304 for The Differences in Content of Health Care Plans of Medical and Nursing Students in Interprofessional and Uniprofessional Education by Carolyn Teuwen, Hanke Scheffer, Suheda Sekmen-Algin, Rashmi A. Kusurkar, Hermien Schreurs, Hester Daelmans and Saskia Peerdeman in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205241283304 - Supplemental material for The Differences in Content of Health Care Plans of Medical and Nursing Students in Interprofessional and Uniprofessional Education
Supplemental material, sj-docx-3-mde-10.1177_23821205241283304 for The Differences in Content of Health Care Plans of Medical and Nursing Students in Interprofessional and Uniprofessional Education by Carolyn Teuwen, Hanke Scheffer, Suheda Sekmen-Algin, Rashmi A. Kusurkar, Hermien Schreurs, Hester Daelmans and Saskia Peerdeman in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205241283304 - Supplemental material for The Differences in Content of Health Care Plans of Medical and Nursing Students in Interprofessional and Uniprofessional Education
Supplemental material, sj-docx-4-mde-10.1177_23821205241283304 for The Differences in Content of Health Care Plans of Medical and Nursing Students in Interprofessional and Uniprofessional Education by Carolyn Teuwen, Hanke Scheffer, Suheda Sekmen-Algin, Rashmi A. Kusurkar, Hermien Schreurs, Hester Daelmans and Saskia Peerdeman in Journal of Medical Education and Curricular Development
Supplemental Material
sj-doc-5-mde-10.1177_23821205241283304 - Supplemental material for The Differences in Content of Health Care Plans of Medical and Nursing Students in Interprofessional and Uniprofessional Education
Supplemental material, sj-doc-5-mde-10.1177_23821205241283304 for The Differences in Content of Health Care Plans of Medical and Nursing Students in Interprofessional and Uniprofessional Education by Carolyn Teuwen, Hanke Scheffer, Suheda Sekmen-Algin, Rashmi A. Kusurkar, Hermien Schreurs, Hester Daelmans and Saskia Peerdeman in Journal of Medical Education and Curricular Development
Footnotes
List of abbreviations
Acknowledgements
We would like to thank all of the students involved for the time and effort they invested in our assignments.
Authors’ contributions – CRediT statements
Author 1: Conceptualization, Methodology, Formal analysis, Investigation, Resources, Writing – original draft, Project administration. Author 2: Conceptualization, Methodology, Formal analysis, Investigation, Resources, Project administration. Author 3: Conceptualization, Methodology, Formal analysis, Investigation, Resources, Project administration. Author 4: Conceptualization, Methodology, Writing – review & editing, Supervision. Author 5: Conceptualization, Methodology, Writing – review & editing, Supervision. Author 6: Conceptualization, Methodology, Writing – review & editing, Supervision. Author 7: Conceptualization, Methodology, Writing – review & editing, Supervision. All authors state that all questions about accuracy and integrity are appropriately resolved and give their final approval of the version to be published.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The study was submitted to the local scientific board of Northwest Clinics, the Netherlands, which considers all study proposals within the institution. Since the study does not fall within the scope of the Dutch Medical Research Involving Human Subjects Act (section 1.b WMO, 26th February 1998), the local scientific board of Northwest Clinics approved the study and waived the need for approval by an Ethics Committee/Institutional Review Board. All participants received an information letter informing them about the goals and planning of the research, the anonymity of the assignments and that (non-)participation would not have any influence on their education. Participation was voluntary. Written informed consent was obtained from all participants. All methods were performed according to the relevant guidelines and regulations.
Availability of data and materials
The privacy officers of Amsterdam UMC advised to not share the data due to ethical considerations: we didn’t asked students their permission at the start of the study, and we are not able to do it retroactively. We anonymized the file, but because it is a small sample size, and we included two different groups of students (medical and nursing), students (or others) might be able to identify themselves. No intermediary data can be de-identified without compromising anonymity.
Consent for publication
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.