
Abstract
Objectives
Despite the rise in the common rheumatological and musculoskeletal disorders (RMDs) in Africa, rheumatology remains an under recognized field with limited training and exposure of medical students. We assessed the knowledge of undergraduate medical students in Uganda on RMDs occurring in our settings.
Methods
A descriptive cross-sectional study was conducted among clinical year medical students at 9 universities in Uganda offering undergraduate medical degrees in March and April 2022. A self-administered, semistructured questionnaire was used to collect data on sociodemographic characteristics and basic knowledge on RMDs online using KoboToolbox. Sufficient knowledge was defined as a score of ≥50% (pass mark for undergraduate students in Uganda). Multivariable logistic regression was performed using STATA 16 to determine factors associated with knowledge acquisition on RMDs.
Results
We enrolled 359 medical students from 9 medical training institutes across Uganda. Overall, 126 (35.1%) participants had sufficient knowledge and the overall mean score for all participants was 41.2%. Factors independently associated with sufficient knowledge were: being in fourth (adjusted odds ratio [aOR]: 2.6, 95% confidence interval [CI]: 1.49-4.64, P < .001) and fifth year (aOR: 2.2, 95% CI: 1.18-4.18, P = .013) compared to third year of study, awareness of the speciality of rheumatology (aOR: 4.0, 95% CI: 1.96-8.06, P < .001), formal classes on rheumatology (aOR: 2.0, 95% CI: 1.15-3.35, P = .012), prior bedside teaching on RMDs (aOR: 2.3, 95% CI: 1.49-3.69, P < .001), awareness of common RMDs (aOR: 3.2, 95% CI: 1.67-6.04, P < .001), and having seen a patient with an RMD (aOR: 1.8, 95% CI: 1.14-2.77, P < .01).
Conclusion
There was a significant knowledge gap among undergraduate medical students nationwide on rheumatology. There is an urgent need to increase exposure to RMDs for undergraduate medical students to address the rising burden of RMDs in Uganda.
Introduction
Rheumatological and musculoskeletal disorders (RMDs) are the second leading cause of disability in the world with the fourth highest impact on disability-adjusted life years. 1 RMDs pose a significant limitation of participation in several activities by the patients that is further coupled with reduced quality of life of the affected individuals.2,3 RMDs such as rheumatoid arthritis, systemic lupus erythematosus (SLE), Sjogren's syndrome, etc are chronic, autoimmune, and inflammatory disorders that affects multiple organ systems, particularly joints, skin, and muscles.4,5
RMDs are one of the most common causes of morbidity and yet rheumatology—the study of RMDs, is still not given the appropriate attention in the undergraduate curriculum. 6 Having realized that undergraduate medical education in rheumatology was inadequate early in the 21st century, robust efforts have since been employed to improve education to this effect. Early exposure of medical students to rheumatology not only increases their awareness of the RMDs but also raises the chances of the students choosing this field of study.7,8 However, whereas the specialty of rheumatology in Africa is still growing, it is worth noting that it has made more progress. 4 RMDs such as SLE and rheumatoid arthritis are increasingly recognized in African countries, including in Uganda. 4
Rheumatology is under-recognized in the undergraduate curricula of many medical schools. In medical schools in Uganda, the topics on RMDs are taught in a single 2 to 3h lecture or tutorial in fifth year of undergraduate medical training under internal medicine under the guidance of a rheumatologist. Thereafter, the students are expected to attain additional knowledge on RMDs from bedside teachings upon encountering a patient with one of the RMDs. However, patients with RMDs are often admitted due to opportunistic infections, which make the points of discussion, rather than the RMDs. In addition, there are fewer chances of topics on RMDs appearing in the final internal medicine exams for undergraduate medical students than the other topics such as infectious diseases. This has led to insufficient awareness and exposure of medical students on RMDs. This has been attributed to the limited number of rheumatologists and other health professionals trained as educators to contribute to the students’ expertise in rheumatology. 8 Recent publication from India showed that only 11% of medical students scored more than 50% in all domains of rheumatology. 9 Therefore, there is an existing gap in knowledge on rheumatology among undergraduate students which has continuously affected primary care of patients with RMDs.
Medical students eventually become the primary care providers who ought to have basic knowledge on RMDs. Knowledge on RMDs among medical students in Africa has not been widely reported, with only a few studies conducted highlighting the inadequate knowledge among medical students in Africa.10,11 We sought to assess the awareness of rheumatology and knowledge on common RMDs and their treatment among undergraduate clinical year medical students in Uganda.
Methods
Study design
A descriptive analytic cross-sectional study was conducted, and data collected quantitatively between March 19 and April 23, 2022.
Study setting
The study was conducted in 9 universities in Uganda offering undergraduate medical degrees, that is, Makerere University Kampala (Mak), Mbarara University of Science and Technology (MUST), Gulu University (GU), Kampala International University (KIU), Kabale University (KU), Busitema University (BU), Islamic University in Uganda (IUIU), King Caesar International University (KCU), and Uganda Christian University (UCU). Mak, GU, MUST, BU, and KU are public universities, and the remaining universities are private. The combined population size of all these medical schools is about 6000 to 7000 students. The undergraduate medical curriculum in Uganda involves undertaking biomedical sciences in the first 2 years and clinical work in the last 3 years of medical school, where learning is facilitated through lectures, tutorials, clinical rotations on wards and in clinics and community placements.
Study population
The study involved undergraduate clinical year medical students-years 3, 4, and 5, pursuing Bachelor of Medicine and Bachelor of Surgery (MBChB); an undergraduate degree program in the abovementioned universities.
Selection criteria
Undergraduate medical students pursuing MBChB at the abovementioned universities; aged 18 years and above were enrolled and participated in the study. A random sampling technique was used. Only those who consented to participate were included. Those without access to internet were excluded.
Sample size
The sample size was calculated using the modified Kish and Leslie formula, with an estimated knowledge of 50% and a population size of 540, and type 1 error of 5%



Data collection
Quantitative data was collected using a self-administered, semistructured questionnaire that had both open and closed ended questions, and a consent form appended to it for the participants to provide informed consent. Questionnaires were used to collect the data; with the KoboToolbox link circulated using students’ WhatsApp platforms by their respective class leaders. The questions were developed based on rheumatology textbooks, pre-existing publications and expertise of physicians experienced in the management of RMDs.6,9,11–13 The questionnaire consisted of 2 parts: sociodemographic characteristics, knowledge on common RMDs, clinical features, and their management. The questions covered the common rheumatological diseases which were considered as part of the basic awareness in the field of rheumatology.
Study variables
We assessed knowledge on common RMDs. Additional data collected included, social demographics; age, university, year of study, prior training, rheumatology clinical exposures, and formal classes/bedside teaching on RMDs.
Operational definition
Sufficient knowledge was defined as a score of ≥50% on a set of 41 questions which were carefully evaluated by 2 physicians with experience in rheumatology (MK and FB). A score of 50% is the standard pass mark for all subjects taught as undergraduates in Uganda.
Statistical analysis
The data was analyzed using Microsoft Excel 2016 and the STATA version 16.0 software. Numerical data was summarized as mean and standard deviation for normally distributed or median and interquartile range for non-normally distributed data. Categorical data was presented as proportions and frequencies. Chi-square and Fischer's exact tests were used to compare categorical variables and t-tests or Mann-Whitney U for numerical data. Multivariable logistic regression analysis was used to determine predictors of knowledge on common rheumatological diseases. Statistical significance was set a P < .05.
Ethics approval
Ethical approval was sought from Mulago Hospital Research and Ethics Committee (approval number: MHREC 2162). All participants provided informed consent by signing a consent form appended to the questionnaire. The study was conducted in observance of the Declaration of Helsinki.
Public and patient involvement
There was no public or patient involvement in the design, conducting, reporting, or dissemination plans of our research.
Results
Baseline characteristics
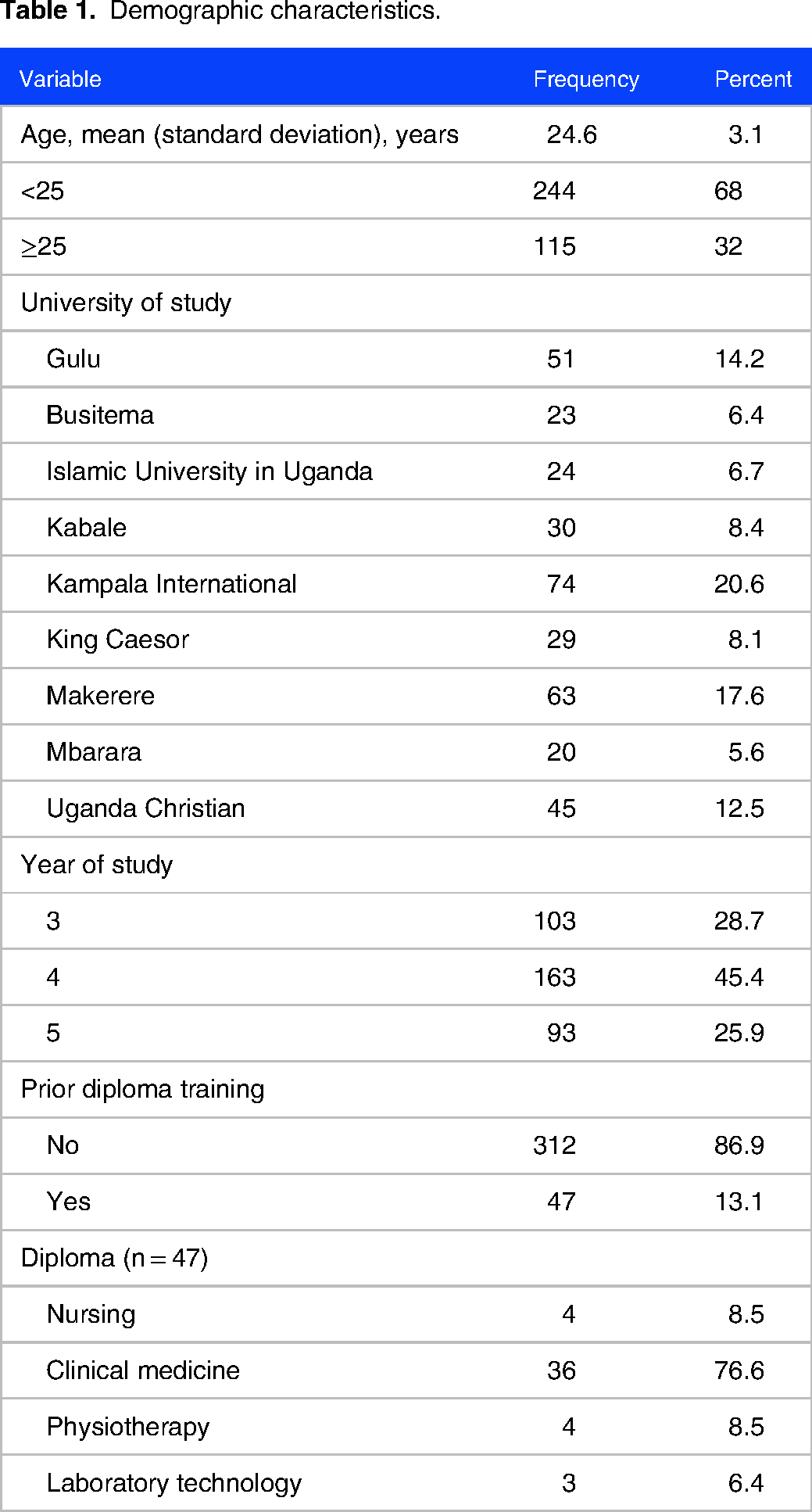
Overall, 700 clinical year medical students (an average of 78 students per medical school) were asked to participate in the study and had the questionnaire sent to them. Of the anticipated 384 responses, 359 (response rate 359 of 700) were returned. Most participants were from KIU (n = 74, 20.6%) and MUK (n = 63, 17.6%). The mean age of all participants was 24.6 (SD: 3.1) years. Most (45.4%, n = 163) participants were in their fourth year of study. Forty-seven (13.1%) participants had a prior diploma training, mostly (76.6%, n = 36) in clinical medicine, Table 1.
Demographic characteristics.
Rheumatology teaching and clinical exposure
Majority of the student had ever heard about (83.8%, n = 301), and had formal classes (73.5%, n = 264) on RMDs/rheumatology. However, only 126 (35.1%) participants had ever had a bedside teaching on RMDs and majority of these were on rheumatoid arthritis (63.5%, n = 90). A total of 247 (68.8%) participants reported seeing patients with RMDs during their clinical rotations and only 150 (41.8%) had heard about disease modifying antirheumatic drugs, Table 2.
Rheumatology teaching and clinical exposure.

Interestingly, 54 (15.0%) participants thought rheumatology was the study of rheumatic fever and/or rheumatic heart disease, Table 3.
Knowledge on diagnosis and management of common rheumatic diseases.

Knowledge on rheumatology
Overall, 126 (35.1%) participants had sufficient knowledge on rheumatology. The overall mean score was 41.2 (SD: 17.8) %. Only 4 (1.1%) scored above 80%. The mean score significantly increased from third through fifth year of study (P < .001), Figure 1. There was a statistically significant variation in marks scored across the various medical schools with participants from BU (49.2%), MUST (47.7%), and KIU (47%) scoring the highest marks and GU (31.9%), IUIU (39.9%), and MUK (37.4%) scoring lower marks (P < .001), Figure 2.

Mean knowledge score of participants stratified by year of study. There was a statistically significant trend toward better knowledge with higher level of education.

Mean knowledge score of participants stratified by university of study. Abbreviations: BU, Busitema University; GU, Gulu University; IUIU, Islamic University in Uganda; KCU, King Ceasor University; KIU, Kampala International University; KU, Kabale University; Mak, Makerere University, Kampala; MUST, Mbarara University of Science and Technology; UCU,Uganda Christian University.
Factors associated with sufficient knowledge on rheumatology
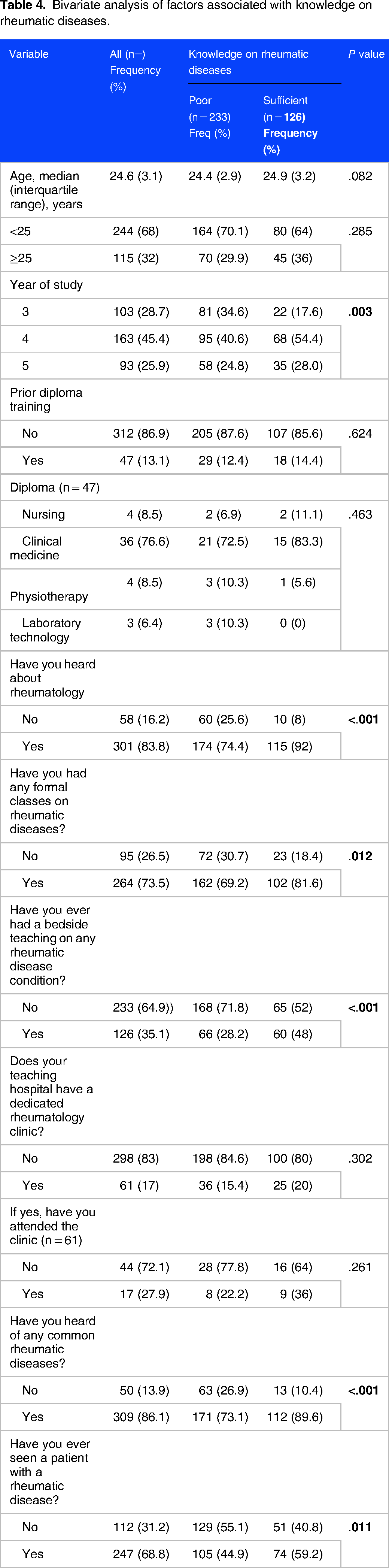
At bivariate analysis, factors significantly associated with sufficient knowledge on rheumatic diseases were year of study (P = .003), awareness about rheumatology (P < .001), having had formal classes on rheumatology (P = .012), prior bedside teaching on RMDs (P < .001), awareness of common rheumatic diseases (P < .001) and having seen a patient with a rheumatic disease (P = .011), Table 4.
Bivariate analysis of factors associated with knowledge on rheumatic diseases.
At multivariable logistic regression see Table 5. Factors independently associated with sufficient knowledge on rheumatology were: being in fourth (adjusted odds ratio [aOR]: 2.6, 95% CI: 1.49-4.64, P < .001) and fifth year (aOR: 2.2, 95% CI: 1.18-4.18, P = .013) compared to third year of study, awareness of the speciality of rheumatology (aOR: 4.0, 95% CI: 1.96-8.06, P < .001), formal classes on rheumatology (aOR: 2.0, 95% CI: 1.15-3.35, P = .012), prior bedside teaching on RMDs (aOR: 2.3, 95% CI: 1.49-3.69, P < .001), awareness of common RMDs (aOR: 3.2, 95% CI: 1.67-6.04, P < .001) and having seen a patient with an RMD (aOR: 1.8, 95% CI: 1.14-2.77, P < .01).
A multivariable logistic regression analysis of factors associated with knowledge on rheumatic diseases.

Discussion
In this study, we assessed the knowledge of undergraduate medical students in Uganda about rheumatology and RMDs, we found that about 84% of clinical year medical students had ever heard about rheumatology as a specialty. However, only about one-third of medical students had sufficient knowledge on the common RMDs. Moreover, the overall mean score was below average (41.2%) even though majority of the medical students had formal classes on rheumatology. Some of the factors that were positively associated with knowledge on rheumatology include being in fourth or fifth year, having had formal classes, bedside teachings as well as having seen a patient with a rheumatological condition. Rheumatology needs to be integrated into undergraduate curriculum to enhance awareness on the epidemiology, diagnosis, and treatment of the common RMDs in Uganda and similar settings across Africa where rheumatology practices are poorly established.
The mean score across all the medical schools in Uganda was below 50%. This indicates a significant knowledge gap regarding the speciality of rheumatology and RMDs among medical students in their clinical years in Uganda. Our finding is consistent with a study conducted in India by Thomas and colleagues, which showed that about 4 in 5 of medical students had insufficient knowledge on rheumatology and RMDs. 9 In the same study, rheumatoid arthritis was the most known RMD to medical students. This finding is similar to that in our study where majority (about 63.5%) had a formal teaching about rheumatoid arthritis. Rheumatoid arthritis is the most common autoimmune RMD in Uganda and, patients have higher chances of being admitted during the flares.3,14 This therefore offers an opportunity for the students to interface with patients with rheumatoid arthritis, however, this may not be the case for other rheumatological disease conditions. There are limited studies across Africa and the world at large on rheumatology which is an area for future studies to guide training of primary care physicians given the increasing burden of RMDs globally.
Rheumatology is an emerging speciality in many countries. There are few rheumatologists and rheumatology clinics across Uganda. In fact, there are <5 physicians specialized in care of patients with RMDs. Therefore, clinical exposure and bedside teaching for students is much more limited compared to other disease conditions such as infectious diseases which are highly endemic in Uganda. 15 This could explain why about one-quarter of the participants attributed rheumatology as a study of rheumatic heart disease/fever. Rheumatic heart disease is the most commonly acquired heart disease in Uganda due to postinfectious sequel of Streptococcus pyogenes pharyngitis or skin disease.16,17 Our findings suggest that RMDs are still under-recognised in the undergraduate curricula of medical schools and has resulted into a significant knowledge gap among medical students necessitating significant intervention to improve healthcare provided to patients with RMDs.
Only 1 university, Mak, has a dedicated rheumatology clinic in its teaching hospital (Mulago National Specialised Referral and Teaching Hospital). Consequently, our findings show that over 80% of the participants did not have access to a dedicated rheumatology clinic in their teaching hospital of which, only a few (27.9%) of those had ever attended the clinic. This significantly contributes to the existing knowledge gap. Having formal classes or bedside teachings has been shown to provide basic knowledge to medical students on the topic in question. Therefore, having more formal classes, tutorials, and bedside teachings on rheumatology as part of the core undergraduate curriculum in addition to a dedicated rheumatology clinic accessible to each medical school will significantly improve overall knowledge on RMDs and essentially, patient care. 9
Our study has some limitations. The questionnaire we used was not standardized, however, it was based on rheumatology textbooks, pre-existing publications, and expertise of physicians experienced in the management of RMDs in Uganda. Future standardization of the questionnaire is recommended to advance development of locally appropriate rheumatology course contents for undergraduate medical students. Secondly, much as our sample size was powered to answer the prespecified research objectives, it was small to adequately reflect the awareness and knowledge of the entire body of medical students in Uganda. However, this is the first study to report on knowledge on RMDs among undergraduate students in Uganda. The self-administered nature of the questionnaire could have enabled participants to lookup answers to the questions. This study's strengths included the multicentre nature of the study that included several medical schools in Uganda as well as including medical students from more than just one clinical year.
Conclusions
In summary, we found a significant gap in knowledge on rheumatology and RMDs among medical students in Uganda. Our findings highlight the need for interventions to increase contact time between students and rheumatologists as well as patients living with RMDs to improve their knowledge in that regard.
Footnotes
Acknowledgments
The authors acknowledge the contribution of the following team of individuals in the data collection process. The team is as follows: Mujuzi Patricia Nalugemwa; Uganda Christian University, Achieng Leticia Obbo; King Caesar University, Atim Immaculate Kaducu; Kabale University, Nsubuga Yakobo; Gulu University, Wandera Uthman; Islamic University in Uganda, Kyozira Patricia; Mbarara University, and Sanyu Chelsea Edwards; Busitema University.
Contributorship statement
All authors contributed significantly to the conceptualization, data collection, analysis, interpretation, and manuscript writing. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Fogarty International Center of the National Institutes of Health. Department of State's Office of the U.S. Global AIDS Coordinator and Health Diplomacy (S/GAC), and President's Emergency Plan for AIDS Relief (PEPFAR) under Award Number 1R25TW011213.