
Abstract
OBJECTIVES
The SARS-CoV-2 pandemic is a destabilizing experience for medical students and resident doctors and troubles their training in the hospital setting. This narrative review aims to identify the effect of health crises on the academic and personal lives of medical trainees and to develop solutions to support them.
METHODS
EducationSource, MedLine and PsychInfo were consulted on June 30th and December 16th, 2020 to identify the articles explaining the effect of SARS-CoV-1 (2002), A/H1N1 (2009) or SARS-CoV-2 (ongoing) on medical learners. Exclusion criteria included policy papers, letters to the editor or articles detailing the impact on undergraduate medical curricula, on nonmedical trainees, on the residency application process, or the physical impact of the disease. The quality of the selected papers was appraised using CASP for qualitative studies and NHLBI-NIH for cross-sectional studies.
RESULTS
Ninety-four manuscripts were initially generated and 229, secondarily, of which respectively 14 and 16 were included in the final analysis according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and reviewed qualitatively. It was found that the learners consider their education compromised by exam delays, the suspension of academic activities, and elective surgeries. Anxiety associated with this academic disruption developed. Burnout is exacerbated by the heightened workload. The main difference between the two searches was the long-term effect of COVID-19, including the opportunity for didactic innovation, the worry regarding professional identity formation and the development of mental health issues. The proposed solutions varied from continuous access to mental health resources to the follow-up of learners’ well-being.
CONCLUSION
It would be interesting to assess the impact of medical trainees’ specialty and country’s development on their experience with COVID-19.
Introduction
The unfolding COVID-19 pandemic has sewn fear worldwide and obliged the reconsideration of essentiality. While it overengorges hospitals, the limited and occasionally shortaged medical material has complicated healthcare workers’ workload and potentially heightened the disease's mortality rate. 1 It has thus acutely impacted healthcare workers and trainees by the way they deliver their care, but also by threatening their academic development and mental health. Particularly, medical trainees, such as medical students and residents, have seen their training in the hospital setting perturbed. 2
Medical students are seeking opportunities for clinical exposure to select a specialty to pursue and become reliable resident doctors while residents themselves are looking to acquire the competencies necessary to become adept clinicians. The destabilization endowed by the current pandemic imposes changes to the normal progression of their training. This inevitably alters their academic trajectory, which in turn impacts their personal life, including their mental health. This carries weight because it raises the questions of medical education curricula, delivery reformation and trainee well-being amidst a health crisis.
Although the literature on the impact of COVID-19 on medical trainees is expanding, there is no study, to our knowledge, concentrating on the data detailing both the academic and personal repercussions of COVID-19 and previous similar health crises. In this narrative review, we aimed to describe the effect of SARS-CoV-1, A/H1N1, and SARS-CoV-2 on the academic and personal lives of medical students and residents. Both populations were included because the academic changes induced and the personal effects compelled by such health crises may be similar in both groups.3,4 Our secondary objective was to gather solutions from the literature to better support them.
Methods
A narrative literature review was conducted to qualitatively determine the academic and personal impact of COVID-19 and similar past health crises on medical students and residents. Although this is not a systematic review or a meta-analysis, the search was performed in adherence with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (Figures 1 and 2) for organizational purposes of the articles generated. 5 Our research is exempt from the Research Ethics Board Review.

PRISMA diagram of literature search and exclusion criteria from first search on June 30th, 2020. Of notes, articles were excluded by a human, without the use of automation tools. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.

PRISMA diagram of literature search and exclusion criteria from the first search on December 16th, 2020. Of notes, articles were excluded by a human, without the use of automation tools.
Eligibility criteria
The target populations were medical students and doctors in training at the residency level. Language restrictions were set to include English and French articles. Articles detailing the effect of the 2002 SARS-CoV-1 outbreak, the A/H1N1 pandemic and the ongoing SARS-CoV-2 pandemic were included. Articles were included if they addressed the academic or personal impact of a specific crisis on residents and/or medical students. Articles were excluded if they were inaccessible, policy papers, letters to the editor or detailed the impact on undergraduate medical curricula, on the residency application process, on nonhealthcare workers or students or discussed the physical impact of the disease.
Information sources
The search study was elaborated with the help and expertise of a Health Sciences librarian at the Library of the Faculty of Medicine of the University of Ottawa. An automated search on the databases EducationSource, MedLine, and PsychInfo was conducted to identify the articles explaining the effect of SARS-CoV-1, A/H1N1 or SARS-CoV-2 on medical students and residents. The search was performed twice, once on June 30th, 2020 during the first wave of COVID-19 and once more on December 16th, 2020 during the second wave, to assess the evolution of the data as COVID-19 unfolded in its early phases. Articles reviewed were published until these respective dates. All references were managed by Mendeley Reference Manager v1.19.8. Duplicate articles were removed automatically with a revision from one reviewer (M.C.).
Search strategy
The search strategy was built on the PICO principle (population, intervention, comparison, outcome). 6 The population was medical students and/or residents. Interventions were SARS-CoV-1, SARS-CoV-2, or H1N1. Comparison was not required. The outcome was an impact on academic and personal life. There were no restrictions on study design. The final input is described in Table 1.
Search algorithm.

Selection process
All imported references were first screened by their title and abstract by a sole reviewer (M.C.). Those meeting inclusion criteria were preserved. Inclusion criteria were further applied to the preserved articles, which were secondarily assessed in their entirety by the same reviewer. Those failing to meet the criteria are listed in Tables 1 and 2 of the Supplemental data with the exclusion criteria they fulfill. All articles retained from then were reviewed and validated with the field expert (M.P.). The entirety of this process was organized with and on Google Spreadsheets. The references of these articles were assessed in the same manner to find pertinent references that may not have been generated in the database searches.
Data presentation of articles included from both searches.

Legend: USA = United States of America; UK = United Kingdom.
Data collection process
Upon analysis of the articles included in qualitative synthesis, data was organized on a spreadsheet to include the following variables from each article: year of publication, journal, country, type of study, health crises discussed, target group investigated, sample size, main objective, article summary, limitations, academic impact, personal impact, and proposed solutions. This process was undertaken by the first author (M.C.) and reviewed and validated with the field experts (M.P. and L.P.).
Risk of bias inherent in each study
Articles meeting inclusion criteria were reviewed by a sole reviewer (M.P.). The data collected from them was reviewed by and validated by field experts (M.P. and L.P.). Only the articles that were cross-sectional studies, systematic reviews or qualitative studies were evaluated for risk of bias. These were evaluated by a sole reviewer (M.C.). These were assessed according to NHLBI-NIH Quality Assessment Tool for Cross-Sectional Studies, 7 NHLBI-NIH Quality Assessment Tool for Systematic Reviews, 7 CASP Quality Assessment Tool for Qualitative Studies. 8 The quality of the selected papers was appraised using the following tools.
Synthesis of results
A qualitative description of results for academic impact, personal impact and proposed solution was summarized.
Results
Study selection
A total of 94 articles were identified during the first search. Ninety were screened, of which 45 were ultimately assessed for eligibility. Reasons for exclusion are listed in Figure 1. Fourteen articles were included for qualitative synthesis. Two out of the 14 articles pertained to the SARS-CoV-1 epidemic while the remaining 12 discussed the SARS-CoV-2 pandemic. None pertained to A/H1N1. Two hundred and twenty-nine articles were identified in the second search. One hundred forty-four were screened, of which 65 were assessed for eligibility. Reasons for exclusion are listed in Figure 2. Sixteen articles were included for qualitative synthesis. These all pertained to the current SARS-CoV-2 pandemic.
Study characteristics
In the first search, 221 medical learners were surveyed in the context of SARS-CoV-1 within the specified timeframe. At least 9848 learners were questioned in the context of SARS-CoV-2. The exact number of participants cannot be valued precisely as some articles did not specify this information or were not designed to do so (ie commentaries, systematic reviews). In the second search, at least 3614 medical learners were queried. Table 2 detail the target group, sample size, main goal, and issues addressed yielding from the first and second search, respectively. Table 3 details the results of individual studies.
Results of individual studies.

Risk of relative and cross-study bias
Of the 17 cross-sectional studies included, three have a low risk of bias.17,21,33 One has a high risk of bias because the participation rate of eligible persons was not at least 50%, there was no sample size justification, power description, or variance and effect estimate, the exposure of interest was not measured prior to the outcome being measured, the timeframe was not sufficient to reasonably expect to see an association between exposure and outcome, the exposure was not assessed more than once over time and there were no confounding key variables measured and adjusted statistically for their impact on the relationship between the exposure and outcome. 25 The remainder have an intermediate risk of bias.4,9,11–13,15,23,24,27,29,30,34,35 Table 4 shows a summary of the analysis of these 17 studies.
Bias assessment of cross-sectional studies.

Criteria: I. Was the research question or objective in this paper clearly stated? II. Was the study population clearly specified and defined? III. Was the participation rate of eligible persons at least 50%? IV. Were all the subjects selected or recruited from the same or similar populations (including the same time period)? Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants? V. Was a sample size justification, power description, or variance and effect estimates provided? VI. For the analyses in this paper, were the exposure(s) of interest measured prior to the outcome(s) being measured? VII. Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed? VIII. For exposures that can vary in amount or level, did the study examine different levels of the exposure as related to the outcome (eg, categories of exposure, or exposure measured as a continuous variable)? IX. Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? X. Was the exposure(s) assessed more than once over time? XI. Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? XII. Were the outcome assessors blinded to the exposure status of participants? XIII. Was loss to follow-up after baseline 20% or less? XIV. Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)? Global risk of bias: if more YES than NO, then low risk; if more NO than YES, then high risk, if equal YES and NO, then intermediate.
Of the two systematic reviews included in this study, one has a low risk of bias 2 while the other, an intermediate risk of bias. 18 Table 5 shows a summary of the analysis of these two studies.
Bias assessment of systematic reviews.
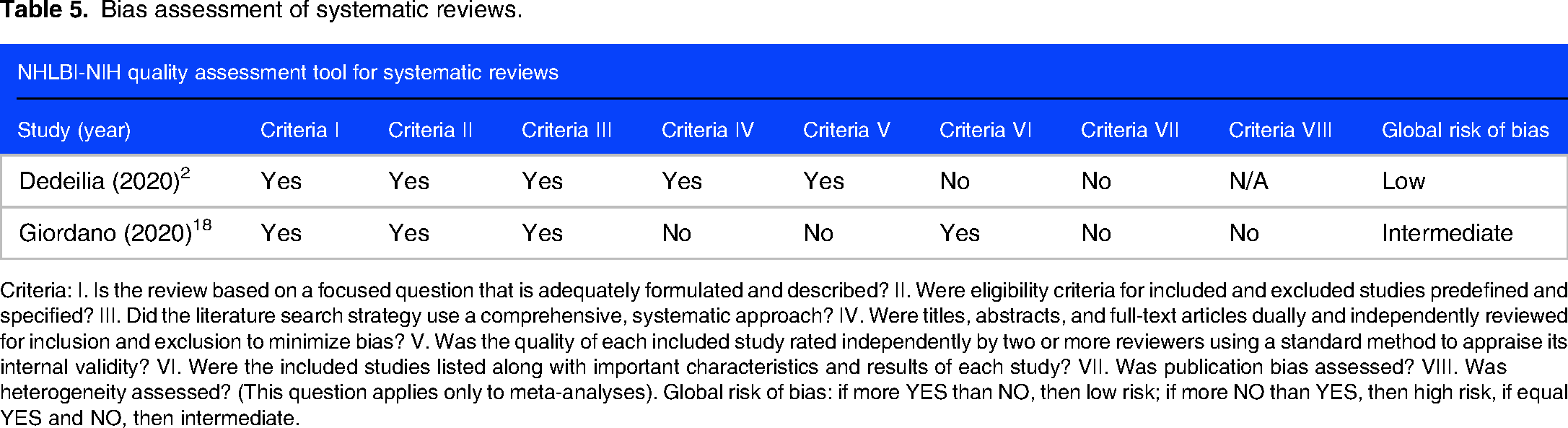
Criteria: I. Is the review based on a focused question that is adequately formulated and described? II. Were eligibility criteria for included and excluded studies predefined and specified? III. Did the literature search strategy use a comprehensive, systematic approach? IV. Were titles, abstracts, and full-text articles dually and independently reviewed for inclusion and exclusion to minimize bias? V. Was the quality of each included study rated independently by two or more reviewers using a standard method to appraise its internal validity? VI. Were the included studies listed along with important characteristics and results of each study? VII. Was publication bias assessed? VIII. Was heterogeneity assessed? (This question applies only to meta-analyses). Global risk of bias: if more YES than NO, then low risk; if more NO than YES, then high risk, if equal YES and NO, then intermediate.
Of the four qualitative studies included, two have a low risk of bias.10,22 Two have a high risk of bias.16,20 Hilburg et al have a risk because ethical issues were not taken into consideration and the date was not sufficiently rigorous. Dhillon et al have a high risk because the recruitment strategy was not appropriate to the aims of the research, the relationship between researcher and participant was not adequately considered, ethical issues were not taken into consideration, the data analysis was not sufficiently rigorous and there was no clear statement of findings. Table 6 shows a summary of the analysis of these 4 studies.
Bias assessment of qualitative studies.

Questions: I. Was there a clear statement of the aims of the research? II. Is a qualitative methodology appropriate? III. Was the research design appropriate to address the aims of the research? IV. Was the recruitment strategy appropriate to the aims of the research? V. Was the data collected in a way that addressed the research issue? VI. Has the relationship between the researcher and participants been adequately considered? VII. Have ethical issues been taken into consideration? VIII. Was the data analysis sufficiently rigorous? IX. Is there a clear statement of findings? X. How valuable is the research? Global risk of bias: if more YES than NO, then low risk; if more NO than YES, then high risk, if equal YES and NO, then intermediate.
Syntheses of results
In the first search, the most common academic impact was the suspension of in-person activity, depicted in 6 articles.2,9,10,13,22,35 There was an online shift of didactic material.9,10,13,22 Deployment and rotation incompletion was also reported in 4 articles of the 16.2,13,30,35 Other, less frequently detailed repercussions included decreased clinical exposure due to lack of personal protective equipment (PPE), cancelation of elective surgeries, and telework.2,9,13,27
The most common personal impact was anxiety related to working in a high-risk environment depicted in 4 articles.15,20,22,35 This was closely followed by anxiety secondary to the above academic changes in 3 papers.21,22,35 Depression secondary to isolation and burnout due to changes at work also came up.11,20–22,25 Another, less frequently mentioned consequence was anxiety due to the financial burden of the health crises. 30
Common solutions proposed were the promotion and adoption of healthy lifestyle and didactic innovation.11,18,20,21,25 Other initiatives went from check-in emails to instilling accessible mental health resources and PPE.13,22
In the second search, the most common academic impact was limited clinical exposure, depicted in 4 articles.3,18,23,29 Suspension of in-person activities and online shift of didactic material were mentioned in 3, as well as the cancelation of elective surgeries.3,17,18,33 Less supervision was detailed in three papers.3,18,23 Other, less frequently detailed repercussions included were delayed rotations and graduation, lack of professional identity formation, and increase in work hours and telework.3,18,23,29,33,34
The most common personal impact was anxiety depicted in 8 articles.3,4,23,24,26,28,34 This was followed closely by insomnia or changes in sleep patterns and depression.4,23,24,26,28,34 Other, less frequently mentioned consequences were fear related to virus exposure and infection of loved ones and worry about career development.4,12,28,29,34
Common solutions proposed were having accessible mental health resources and training in telehealth precepting.3,18,19,26,29 Other initiatives went from professional development programs to ensuring technological support and training.18,26
Reporting biases
The screening process of articles generated initially in each search was undertaken by a sole reviewer (M.C.) to exclude those failing to fulfill inclusion criteria. Those meeting them were assessed by the same reviewer to eliminate those suiting the exclusion criteria. Provided this undertaking was performed by a sole person, subjectivity in the initial selection process remains an important bias in our methodology. Furthermore, the qualitative report of this study dilutes objectivity as the reviewers’ opinions are involved.
Discussion
The current COVID-19 pandemic continues to strain the healthcare system and its workers as well as test their adaptability. Notably, physicians-in-training have seen their academic development bothered and their personal life, challenged. In this narrative review, we intended to describe the effect of COVID-19 and past epidemics and pandemics on the academic and personal lives of medical students and residents. To this effect, an automated search was performed on two occasions: one during the first wave of COVID-19, and the other, during its second wave, each of which 14 and 16 articles, respectively, were included for qualitative synthesis. This review confirmed and recognized the academic and personal impact of the sanitary crisis on junior healthcare workers and identified solutions to alleviate the burden they bestow.
Academic repercussions common to articles yielded from both searches were the suspension of in-person academic activities, online teaching, examination postponement, cancelation of elective procedures, disruption of rotation and telemedicine. This suggests the perpetuation of guidelines minimizing in-person interactions to curtail infection propagation. The need for appropriate distancing measures as well as the shortage of PPE has forced hospitals to minimize nonessential staff in the workplace, which means medical learners now lack bedside teaching and direct observation of their clinical ability in both assessing a patient and elaborating their management.2,13 Dedeilia et al further emphasize the greater impact on surgical education as urgent and emergency procedures solely are performed, most of which are not usually performed by trainees, further precluding their training. 2
The personal impact raised in both searches was anxiety, depression, and worry related to academic changes, social distancing guidelines, and work in a high-risk environment. Anxiety in the time of COVID-19 sees itself exacerbated by life and work in an urban area, gaps in social support or lack thereof due to social distancing guidelines alongside living with parents who may have comorbidities and thus, may be at higher risk of either contracting the virus or displaying a more serious presentation of it. 17 Those relocated to busier centers are further isolated, and potentially further burdened financially.17,22 Once more, this underlines the persisting, and perhaps worsening, psychological state of residents as the infection rate worsens and rules and regulations tighten in response.
The 14 articles initially generated reported emphasis on acute and emergency medicine and limitation of clinical exposure because of lack of PPE as further academic changes. Staff deployment aimed to saturate emergency medicine and intensive care services. 2 The articles generated from the secondary search detailed concerns with professional identity formation, decrease in supervision, increase in working hours and innovation of virtual educational tools as other academic impacts of major health crises. The difference between the results of these searches may be explained by chronology. Loss of professional identity may be endowed by the diminishing time spent outside of work, thus blurring the line between personal and professional identity, but also steering learners away from their program objectives in an effort to concentrate on helping hands to alleviate the COVID-19 strain. 34 The second search conducted nearly 6 months after the first produced results affected by time; that is, pandemic time length. It is reasonable to see long-term effects, such as didactic innovation and worry about professional identity formation, develop as the crisis lengthens. Such consequences may not have time to evolve in an otherwise acute situation. Educational innovation proving efficient span from maximizing the use of video conference tools (ie whiteboard function and breakout rooms), telehealth precepting, and surgical platforms accessible from home including virtual operation room simulations, laparoscopic box training, and intraoperative videos.3,18,27
In regard to the personal impact, the main differences uncovered between both searches were changes in sleep patterns and mental health issues exacerbated in urban and lower-income households or having an underlying psychiatric condition, in the second search.17,19 Once more, this may be elucidated by the long-term effects of a pandemic as a more serious toll is taken on well-being and income as it progresses. Sleep disturbance, particularly, including falling asleep late or not at all, has led to further psychological distress.24,28,34 Torun et al identified exacerbated sleep impairment since the onset of the COVID-19 pandemic in a third of its participants (n = 275), while Saraswathi et al points out an association between poor sleep quality and an increase in stress, anxiety and depression.24,28
The secondary goal of this paper was to identify solutions within the literature that tackled the academic and personal problems sparked by the health crisis. All were suggestions found within articles pertaining to the unfolding COVID-19 pandemic. Both searches recommended solutions addressing mental health and the availability of its resources as well as encouraged the development of online learning tools. Particularly, anticipation of the reverberations of a sanitary crisis in both academic and personal spheres would undoubtedly alleviate them. 36 Ways of doing so include mulling over previous crises to stay ahead of future ones, prioritizing the safety of the staff, learners and patients by ensuring access to protective gear, being attentive to burnout within the healthcare team and further asseverate the need for mental health support prior to and during tumultuous times. Another suggestion was an innovation of platforms through which learners can participate remotely, complement their education and prepare to catch up when normalcy resumes. 36 The main difference in regard to solutions lies within the perspective of longevity taken by each search. The first search focused on addressing issues in the earlier stages of the pandemic, or in a more acute setting (ie following up on resident experience shortly after tough clinical interactions), ensuring PPE availability and tending to their basic needs, that is need for water, food, sleep and proper shelter.13,25,30 The second search further emphasized long-term solutions, such as telemedicine as a permanent implementation in medicine and guaranteeing technological support and training for the long-term use of virtual platforms.
This is the first narrative review, to our knowledge, pooling the literature pertaining to SARS-CoV-1, H1N1 and SARS-CoV-2 and their respective impacts on medical trainees. The strengths of this narrative review lie in the explanation of divergent results and in the reproducibility of the systematic search, especially as the COVID-19 pandemic continues to unravel. Moreover, articles generated were from North America, South America, Europe, Asia and Oceania, revealing a relative idea of the impact of recent health crises in a substantial portion of the world. Nonetheless, because of the nature of this study, as a qualitative narrative review, it reflects our judgment, and thus, involves selective and subjective bias, in both the selection and interpretation of articles. 31 The search media were MedLine, PubMed, and EducationSource, only. Further limitations include the lack of articles discussing H1N1 and the few discussing SARS-CoV-1 in comparison to those addressing SARS-CoV-2. Perhaps this discrepancy is explained by the length of the SARS-CoV-2 pandemic and its associated mortality and healthcare burden. 1 However, academic and personal repercussions of both SARS viruses seem similar. The evidence suggested in each article included must be considered within the bias each inevitably has. Lastly, we did not examine specific causality and the results we detailed are not statistically representative. Implications of this review remain mostly in the solutions proposed in most of the articles analyzed in an attempt to remedy the distress induced by such health crises. Checking in on learners frequently, encouraging virtual didactic innovation and increasing vigilance regarding mental health are seemingly the easiest and quickest solutions to implement and may provide some prompt aid and relief to residents. Supplementary research would, however, be needed to investigate the impact of countries’ level of development on trainees, as well as the impact of their specialty.
Conclusion
The current narrative review has explored the impact current and past health crises have had on the academic and personal lives of medical trainees. It has highlighted some of the issues with isolation and virtuality implicated by such situations and proposed solutions to help learners better adapt to these new realities, all the while supporting them throughout their academic journey. As the COVID-19 pandemic continues, it is critical that future research addresses the long-term impact of this disease on trainees, their professional development and personal wellbeing. It is up to individual institutions to implement strategies to both support and enhance the medical learner's experience during trying times and assess whether those strategies are effective and sufficient or rather, need revision and innovation.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231217897 - Supplemental material for Impact of SARS, H1N1, and COVID-19 on Medical Trainees’ Academic and Personal Experience: A Systematic Search and Narrative Review
Supplemental material, sj-docx-1-mde-10.1177_23821205231217897 for Impact of SARS, H1N1, and COVID-19 on Medical Trainees’ Academic and Personal Experience: A Systematic Search and Narrative Review by Megan Cipro, Lyne Pitre, Salomon Fotsing and Marjorie Pomerleau in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-2-mde-10.1177_23821205231217897 - Supplemental material for Impact of SARS, H1N1, and COVID-19 on Medical Trainees’ Academic and Personal Experience: A Systematic Search and Narrative Review
Supplemental material, sj-pdf-2-mde-10.1177_23821205231217897 for Impact of SARS, H1N1, and COVID-19 on Medical Trainees’ Academic and Personal Experience: A Systematic Search and Narrative Review by Megan Cipro, Lyne Pitre, Salomon Fotsing and Marjorie Pomerleau in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-3-mde-10.1177_23821205231217897 - Supplemental material for Impact of SARS, H1N1, and COVID-19 on Medical Trainees’ Academic and Personal Experience: A Systematic Search and Narrative Review
Supplemental material, sj-pdf-3-mde-10.1177_23821205231217897 for Impact of SARS, H1N1, and COVID-19 on Medical Trainees’ Academic and Personal Experience: A Systematic Search and Narrative Review by Megan Cipro, Lyne Pitre, Salomon Fotsing and Marjorie Pomerleau in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
We thank the Francophone Affairs Office of the University of Ottawa and Association médicale universitaire de l’Hôpital Montfort for their assistance and support as well as Marie-Cécile Domecq for her assistance and expertise in database search.
DECLARATION OF CONFLICTING INTERESTS
The authors declare that there are no conflict of interest.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Association médicale universitaire de l’Hôpital MontfortStudent Bursary.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.