
Abstract
OBJECTIVE
Physical inactivity is a significant contributor to many acute and chronic medical conditions. While the dangers of physical inactivity (PA) are well understood and physicians have the desire to address them, a lack of education in exercise prescription (ERx) may be a barrier to properly prescribing exercise to patients. The aim of this research was to determine the effectiveness of an ERx medical education lecture and provide evidence for the need for formal ERx education among students and physicians in training with a secondary goal of further exploring medical student and resident habits and beliefs about PA and ERx.
METHODS
A one-hour education session was developed based on the American College of Sports Medicine principles of ERx. Pre- and postsurveys were administered immediately before and after the curriculum session to Wayne State University School of Medicine medical students and residents to assess perceived ERx knowledge level and confidence levels for prescribing aerobic and resistance exercise to patients. Virtual curriculum sessions were held over Zoom.
RESULTS
A total of 144 presurvey and 119 postsurvey results were analyzed. The mean perceived ERx knowledge level significantly increased from 4.67/10 ± 1.98 to 7.35/10 ± 1.56 (P < .001). Mean confidence level discussing PA with patients, ability to answer exercise-related questions, confidence level in ability to prescribe aerobic exercise, and ability to prescribe resistance exercise significantly increased in all groups and overall (P < .001)
CONCLUSION
A one-hour session to educate medical students and residents on how to write an ERx improved perceived knowledge and confidence in this subject matter. Although further study is needed to determine long-term knowledge retention and the impact on ERx behavioral practice in a patient care setting, this study provides preliminary evidence to justify its inclusion as a regular component of the medical school curriculum.
Keywords
Introduction
Physical inactivity is a significant contributor to many acute and chronic medical conditions.1–4 It is estimated that over one-third of the world's population do not meet the minimum physical activity (PA) guidelines and 30% of the US population has no PA at all.4,5 This lack of PA has wide-ranging adverse impacts on health including increased rates of cardiovascular disease, cancer, metabolic disorder, musculoskeletal disorders, hypertension, dyslipidemia, cognitive impairment, and mortality.1–4,6 While these impacts are well recognized, and awareness around the role of PA in disease prevention and management has been increasing, there is still a significant gap in the education of exercise prescription (ERx) among medical professionals, specifically physicians. ERx refers to the specific plan of fitness-related activities designed to meet individual health and physical fitness goals within the context of individual health status, function, and the respective physical and social environment.7,8 With a properly executed ERx, the unique needs of a patient can be successfully integrated with exercise principles and behavioral techniques which can increase patient compliance and propel them towards better health and quality of life. 9
Physicians play a vital role in addressing physical inactivity and are often seen by patients as a significant source of exercise-related information.10,11 Unfortunately, many physicians report that they lack the education and skill set necessary to inform their patients on the important aspects of ERx. Lack of training is the most often mentioned barrier by physicians as to why they did not feel comfortable discussing ERx with their patients.11–16 It has been shown that formal training sessions delivered to practicing physicians can improve knowledge of ERx and increase prescribing to patients, however, these interventions fail to address implementing this education to physicians in training, both in medical school and during residency when behaviors are being developed that will be carried throughout practice.17–20 Furthermore, interventions such as these are sparse and have not been carried out in the United States where the medical education and healthcare system is different than other countries. Currently, over 87% of US medical schools offer no curriculum in ERx and only 6% have core coursework in ERx. 11 An internal curriculum review and informal needs assessment at Wayne State University School of Medicine (WSUSOM) yielded a reference to ERx but no education on how to complete it and > 1 h overall on any topics related to PA. This significant lack of education in medical education has resulted in the graduation of physicians who are not equipped to provide exercise-related information to their patients that could have a meaningful impact on their health.
The negative consequences of physical inactivity are well understood and while physicians have a desire to address them, lack of education in ERx is a barrier to properly helping their patients. By providing this education, medical schools could potentially increase the confidence and ability of physicians to give patients actionable and specific exercise programs. The aim of this research was to determine the effectiveness of an ERx education session and provide evidence for the need for formal ERx education among students and physicians in training. A secondary goal of this research was to further explore medical student and resident habits and beliefs about PA and ERx.
Methods
Education design
A formal literature review was conducted along with informal discussions with WSUSOM students and faculty to determine specific educational objectives. Following this, a one-hour education session was developed by a field expert based on the American College of Sports Medicine “Guidelines for Exercise Testing and Prescription.” 8 The education included topics on types of exercise, the basics of creating an exercise program (FITT-VP method), ERx for special patient population groups, and how to create an ERx (Table 1).
Section headings of ERx curriculum with detailed descriptions of what was included.
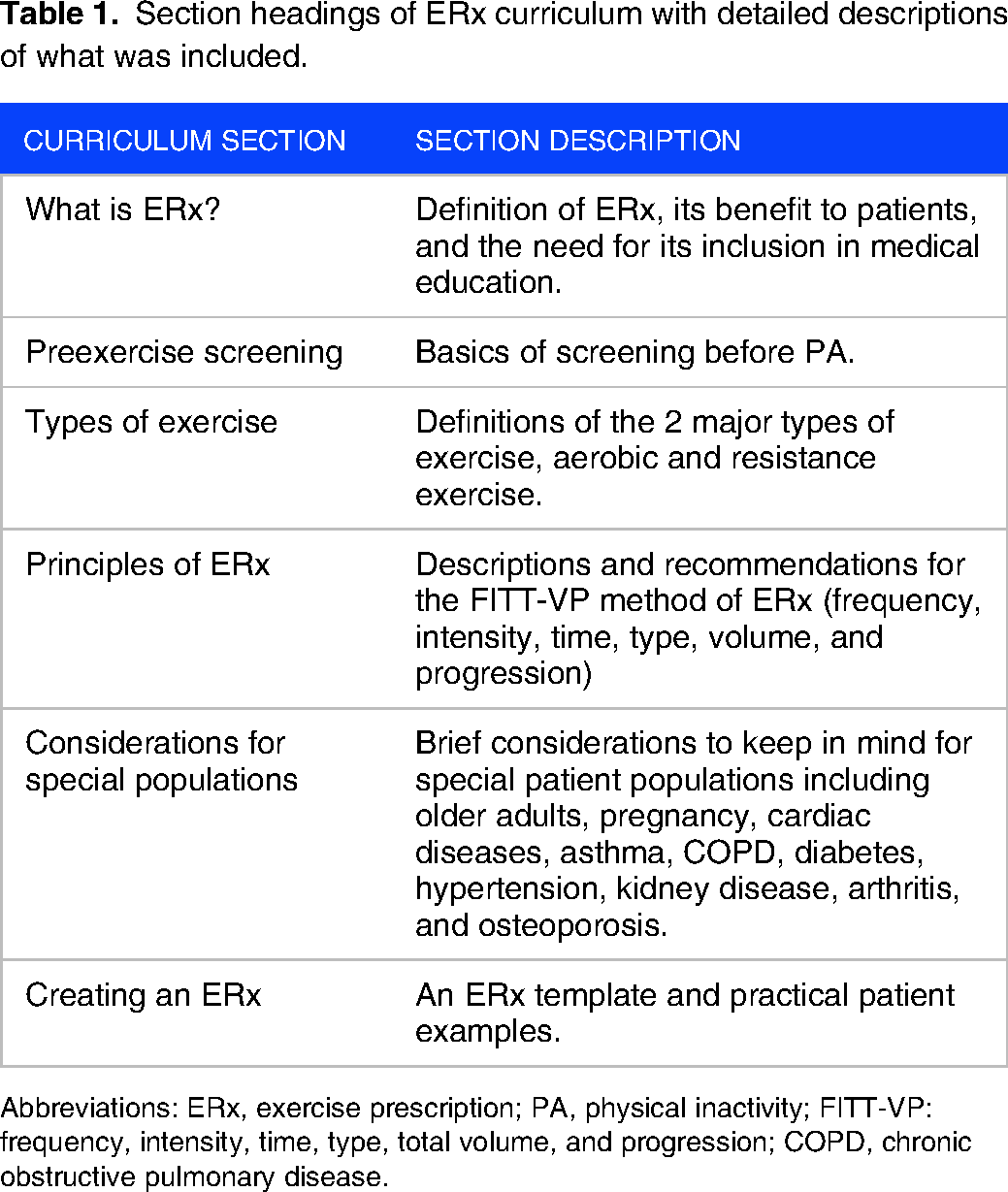
Abbreviations: ERx, exercise prescription; PA, physical inactivity; FITT-VP: frequency, intensity, time, type, total volume, and progression; COPD, chronic obstructive pulmonary disease.
The WSUSOM IRB deemed this project as an educational outcomes assessment and did not require approval from the human investigation committee and the need for obtaining informed consent for the survey was waived.
Education delivery
The curriculum was delivered by an expert in the field via PowerPoint presentation over 2, 1-hour Zoom sessions. One session was offered to all first- and second-year medical students at WSUSOM in Detroit, MI as a voluntary session students could attend. Third- and fourth-year students were not invited as participation was unlikely due to schedule differences by clerkship and clinical site. A separate session was given to internal medicine residents at Detroit Medical Center in Detroit, MI as one of the scheduled residency didactic sessions.
Participants
A total of 162 first- and second-year medical students at WSUSOM and 58 first- and second-year internal medicine residents at Detroit Medical Center. Only first- and second-year internal medicine residents were included as we wanted to include participants who were still early in their training and not functioning as almost independent attending physicians at the time of the study. Any other participants who completed the survey (senior residents, attendings, third- and fourth-year medical students, students outside of WSUSOM, etc) were excluded from statistical analysis.
Data collection
Pre- and postsurveys were administered via Qualtrics immediately before and after Zoom sessions, respectively. Information was gathered using QR code links embedded in the PowerPoint presentation. A follow-up link to the postsurvey was emailed to all participants 1 day after the presentation. Surveys contained 18 questions including 3 demographic questions and a question asking the participant's average current level of exercise. The remaining 14 questions asked about perceived ERx knowledge level on a 10-point rating scale (0 = none, 10 = expert) and confidence levels for prescribing exercise to patients and habits and beliefs surrounding PA on a 5-point Likert scale (1= strongly agree, somewhat agree, neither agree or disagree, somewhat disagree, 5 = strongly disagree) (Supplemental Table 2). Surveys were developed using validated questions from previous studies. Questions that related to the objectives of this study were selected to allow for the determination of the effectiveness of the intervention.13,21–23
Statistical analysis
Descriptive statistics were calculated for PA beliefs and habits data as mean ± SD. Analysis of pre- and postmeans for education and confidence level data were made using the Wilcoxon ranked sum test. P < .05 was interpreted as statistically significant. All statistical analyses were performed using IBM SPSS 28.0.1.1 (IBM, Armonk, NY, USA).
Study duration
The duration of the study, including education design, education delivery, data collection, and statistical analysis was approximately 4 months in length. The study took place between September 2022 and December 2022.
Results
One hundred forty-four presurvey and 119 postsurvey results were reported. Forty-three residents completed the presurvey and 27 completed the postsurvey. One hundred one medical students completed the presurvey and 92 completed the postsurvey. Overall, there was a postsurvey response rate of 63% among residents and 91% among medical students.
Perceived ERx knowledge level
Overall, mean perceived ERx knowledge significantly increased from 4.67/10 ± 1.98 to 7.35/10 ± 1.56 (P < .001, Cohen's d = 1.500). Among residents, the mean perceived ERx knowledge level significantly increased from 4.86/10 ± 1.72 to 7.56/10 ± 1.58 (P < .001, Cohen's d = 1.635). Among medical students, the mean perceived ERx knowledge level significantly increased from 4.59/10 ± 2.08 to 7.29/10 ± 1.57 (P < .001, Cohen's d = 1.465).
Perceived ERx confidence levels
Mean confidence level discussing PA with patients, ability to answer exercise-related questions, confidence level in ability to prescribe aerobic exercise, and ability to prescribe resistance exercise significantly increased in all groups and overall (P < .001) (Table 2).
Perceived ERx confidence level data. Data was reported on a 1–5 Likert scale (1 = strongly agree, 5 = strongly disagree).
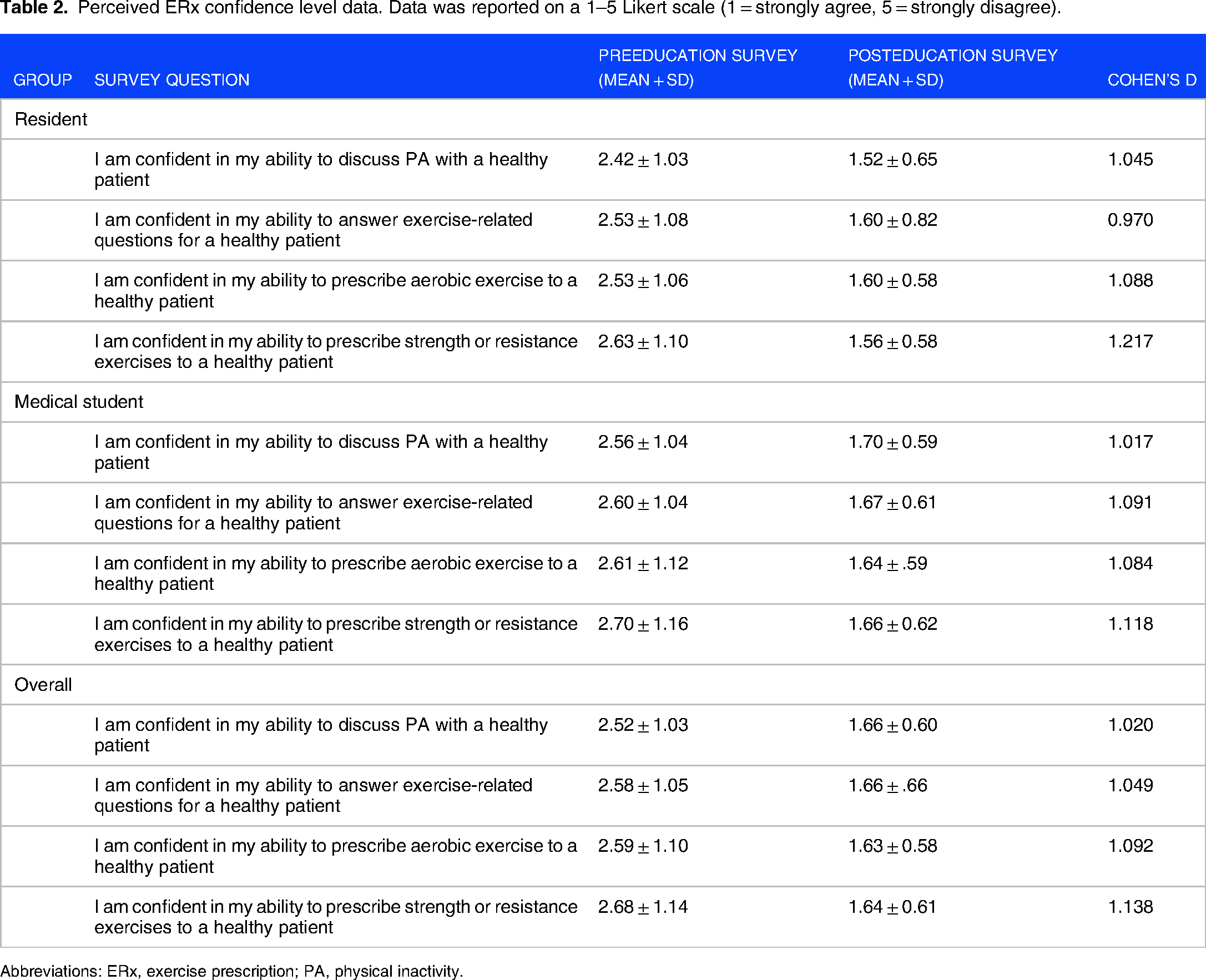
Abbreviations: ERx, exercise prescription; PA, physical inactivity.
PA habits and beliefs
PA habit and belief data were assessed during the presurvey (Table 3).
PA habit and belief data. Data was reported on a 1–5 Likert scale (1 = strongly agree, 5 = strongly disagree).
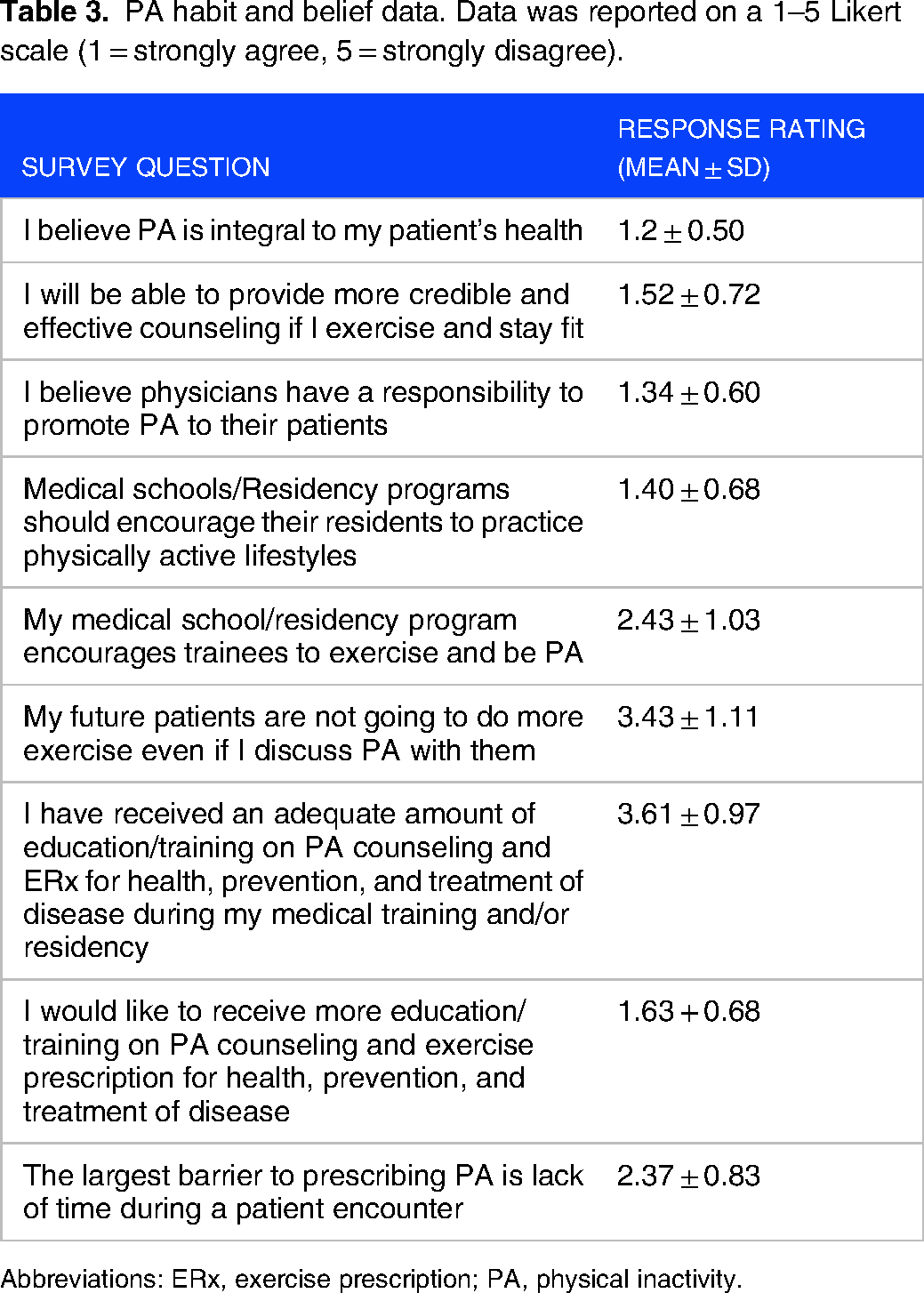
Abbreviations: ERx, exercise prescription; PA, physical inactivity.
Discussion
Our study found that ERx education delivered in a single-hour session led to a significant increase in perceived ERx knowledge, confidence in discussing and answering aerobic and resistance exercise-related questions, and confidence in prescribing aerobic and resistance exercise immediately following the session. We also found that medical students and residents believe that PA is integral to patient health, that they have not received adequate education on PA counseling and ERx training, and that they want to receive more education in these areas.
Exercise prescription
It is well documented that there is a gap in ERx education in medical schools and recently there has been more of a push for inclusion of this type of curriculum.6,11,13,15,21,24–26 Connaughton et al 13 reported that only 10% of medical school deans felt their students could design an ERx for a patient and Cardinal et al 27 found that many medical students receive no formal education in PA. Radenkovic et al 16 found that final-year medical students lacked knowledge of any physical activity guidelines. Vallance et al 23 found that while medical students thought that ERx prescription was important, they indicated less than moderate competence at actual ERx. This significant lack of education has resulted in physicians who are not equipped to provide adequate exercise-related information to their patients.11,13,27 This is a serious problem as physicians are expected to answer questions and offer guidance on all health-related topics, including exercise.10,11 Our findings point to potential improvements in the ability of future physicians and internists to prescribe exercise programs to their patients. While these findings cannot be generalized to actual changes in patient health or physician prescribing behavior, they model that this type of intervention can be integrated into medical education and deserves a space within the curriculum at medical schools and residencies in internal medicine.
Recently, several medical schools have implemented interventions to increase knowledge of PA in medical students. These programs resulted in an increase in student's belief that PA was important for health and treating disease, 21 their understanding of PA guidelines, 28 their comfort in counseling patients on PA,22,29,30 as well as the importance of being physically active themselves.17,31 These results show that educational programs have the potential to increase physician and medical student knowledge of PA. However, none of these programs looked specifically at increasing knowledge and application of ERx. Our study focused on this specifically and demonstrated that a single session was successful at increasing perceived knowledge and confidence levels around prescribing exercise. While our study only looked at the effects of one session, it is likely that a longer and more in-depth curriculum could have larger effects on education, confidence, and potentially ability to prescribe exercise to patients.
There have been few interventions focused specifically on increasing ERx prescribing behavior. Windt et al 20 and Fowles et al 18 found that physician prescribing activity increased following short ERx education sessions. O'Brien et al 19 found that the prescribing activity of physicians with prior ERx training was higher than their counterparts with no training. These results demonstrate that ERx education can increase prescribing activity in practicing physicians. While our study did not test for prescription behavior, these results support a further study to determine whether ERx education has longer-term results and impacts ERx prescribing behavior. While the aforementioned studies showed increased ERx activity, they were only carried out in countries outside of the United States and only with currently practicing physicians. They did not investigate the impact that ERx education has on physicians in training and the specific effects of this training on physicians in the United States. Furthermore, they did not look at knowledge retention related to ERx. Our study, which found increased knowledge gained after an ERx education session, was done within the United States, and performed with medical students and residents. Further research is needed to determine if similar results can be achieved within the US medical system and examine the effect of providing this education to medical students and residents.
Further investigations should focus on long-term knowledge retention and assessment of prescribing ability after education to determine ERx competency in physicians in training in US medical schools and residencies. Research should also be done to examine behavioral change in physician ERx practice and patient exercise practices under the care of physicians undergoing this type of training to understand the applicability and impact of this education in practice.
PA habits and beliefs
Research has consistently reported that medical professionals, including students and residents, believe PA is important for their patients.10,22–24,30 Hébert et al 24 found that providers and students feel they have a role in promoting PA and believe that it is important to their patient's health. Similarly, a study from Jadczak et al 30 found that perceptions among medical students indicated a belief in the importance of prescribing exercise to older patients. Also, several studies have cited that lack of training is the largest barrier that providers and students mention as the reason they do not feel comfortable discussing ERx with their patients.11,13–15 Similar to previous research, our study found that medical students and residents believe PA is important to their patients’ health. They also believe they will be able to provide more credible PA advice if they are physically active themselves and somewhat disagreed with the statement “My future patients are not going to do more exercise even if I discuss PA with them.” Both these statements point to the importance of PA knowledge and participation for both patients and providers, but there are likely many important constructs, including but not limited to task efficacy, 32 body image,33,34 imposter syndrome, 35 and various social determinants of health,36–39 that relate to these beliefs as well. Further research is needed to explore these factors and how they affect both patients and providers. It is also important to acknowledge these multifactorial elements in any type of formal ERx education as it has the possibility to effect ERx behavioral outcomes. Medical students and residents also felt that they had not received enough education on ERx at this point in their education and wanted to learn more about the subject. Our results show that this type of education session is desired by students. Based on all these factors, it seems reasonable that medical schools should consider incorporating ERx education in their curriculum for students.
Limitations
This study is not without limitations. It was conducted at a single medical school and residency program and therefore may not be generalized to all medical schools and residency programs. This was a convenience sample of students and residents who attended the educational session; a power analysis was not performed. Pilot testing of the questionnaire was not completed on the study population. Long-term educational retention was not tested so we are unable to determine if any long-term benefits were gained from the education session. Additionally, student and resident behavioral change was not tracked so the impact on ERx behavior cannot be determined. Lastly, the medical student session was offered as a voluntary session so outcomes may have related to the self-selection of individuals who had an interest in the subject matter.
Conclusion
A one-hour session to educate medical students and residents on how to write an ERx improved perceived knowledge and confidence in this subject matter. Although further study is needed to determine long-term knowledge retention and the impact on ERx behavioral practice in a patient care setting, this study provides preliminary evidence to justify its inclusion as a regular component of the medical school curriculum.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231217893 - Supplemental material for The Application of Exercise Prescription Education in Medical Training
Supplemental material, sj-docx-1-mde-10.1177_23821205231217893 for The Application of Exercise Prescription Education in Medical Training by Thomas Sprys-Tellner, Diane Levine and Asim Kagzi in Journal of Medical Education and Curricular Development
Footnotes
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributorship
TST designed research, performed research, analyzed data, contributed unpublished reagents/analytic tools, and wrote the manuscript. DL designed research, contributed unpublished reagents/analytic tools, and wrote the manuscript. AK designed research, performed research, contributed unpublished reagents/analytic tools, and wrote the manuscript.
Data Sharing Statement
The collected data of this article are available upon reasonable request to the corresponding author
Ethical Approval Information,Institution(s),and Number(s)
This study was exempted from IRB by Wayne State University Institutional Review Board; WSU IRB Number/HPR Determination Number: 2021 107.
TYPE
Original Research Article
Patient Involvement
No.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.