
Abstract
Objective:
There is recent evidence that exercise referral schemes (ERSs) are beginning to permit self-referral access. Notwithstanding this, to date it is unknown whether key referral characteristics, such as age, gender and socioeconomic status are associated with a greater likelihood of self-referring to an ERS, and whether self-referral participants are more or less likely to complete schemes, than traditional healthcare referrals.
Design/Setting:
This study presents an evaluation and cross-sectional exploration of key participant referral characteristics of those (n = 647) who signed up to ‘Active West Lancs’; a 12-week ERS in the northwest of England.
Methods:
Chi-square analysis, tests of difference and binary logistic regression were conducted to explore associations between key referral characteristics and (1) the likelihood of accessing Active West Lancs via a self- or healthcare-referral and (2) the likelihood of completion.
Results:
About 56% of participants accessed the scheme via self-referral. These participants were more likely to be women, to report a musculoskeletal primary health condition, to access a specific site and to do so during spring. The scheme had an overall completion rate of 42.2%. Participants who were older, resided in less socioeconomically deprived neighbourhoods, and accessed a specific site were more likely to complete. Self-referral participants were not more or less likely to complete than those who enrolled via healthcare-referral.
Conclusion:
These data do not directly identify a clear benefit or detriment to Active West Lancs’ incorporation of self-referral participants. Notwithstanding this, enabling self-referral ERS access may widen scheme participation opportunities among those reluctant to seek referral from a healthcare provider and reduce the administrative burden for healthcare providers themselves.
Keywords
Introduction
Exercise referral schemes (ERSs) are physical activity (PA) interventions for adults (18+ years) with long-term physical and/or psychological health condition(s) who do not engage in ⩾ 150 minutes per week of moderate-to-vigorous PA (National Institute for Health and Care Excellence (NICE), 2014). ERSs provide approximately 12 weeks of free or discounted access to a community-based PA environment (Rowley, 2019), where participants adhere to bespoke PA programmes under the supervision of a qualified exercise professional (Rowley et al., 2018). ERSs continue to be delivered nationally and internationally (Arsenijevic and Groot, 2017; Morgan et al., 2020) despite modest and variable effectiveness for facilitating meaningful health outcomes (Wade et al., 2020). In this regard, poor rates of ERS completion, varying between 12% and 93% (Pavey et al., 2012) remain a long-standing and pervasive challenge (Campbell et al., 2015). As a response, previous and ongoing research has sought to identify referral characteristics that are positively associated with ERS completion (Hanson et al., 2021; Mills et al., 2012). Better understanding of these factors will enable modification of future schemes in ways that (1) focus promotion of ERSs towards those most likely to achieve meaningful health enhancing outcomes and/or (2) facilitate the embedding of additional support for those who present the highest dropout risk.
Multiple evaluations have explored the associations between ERS completion and age, primary health condition, gender and socioeconomic deprivation (Kelly et al., 2017; Mills et al., 2012). Age is the most consistent predictor of ERS completion, with older adults more likely to complete schemes than their younger counterparts (Kelly et al., 2017; Oliver et al., 2021). ERS completion is also frequently higher among those referred due to a cardiovascular-related health condition (Campbell et al., 2015; Mills et al., 2012), and lowest among those referred due to a mental health condition (Kelly et al., 2017; Moore et al., 2013). Associations between ERS completion and gender and socioeconomic deprivation status are more equivocal (Hanson et al., 2021; Pavey et al., 2012). Women are less likely to complete some ERSs (Kelly et al., 2017; Moore et al., 2013), but not others (Hanson et al., 2021; Shore et al., 2021), while lower socioeconomic deprivation status is similarly positively associated with ERS completion in some schemes (Hanson et al., 2021), but not others (Shore et al., 2021). Despite some exceptions (Gidlow et al., 2007; Hanson et al., 2013; Kelly et al., 2017), mode of ERS entry is a referral characteristic that has received comparably less attention. Gidlow et al. (2007) identified a positive association between ERS uptake and referral from a primary healthcare provider (e.g. a general practitioner), whereas Kelly et al. (2017) found referral from a secondary care provider to be positively associated with scheme completion. Accessing ERSs following a referral from a primary or secondary care provider is consistent with the ‘traditional’ format of ERS provision (NICE, 2014). However, there have been growing calls for ERSs to embrace self-referral participants in recent years (Din et al., 2015) and evidence that this is occurring in practice (Hanson et al., 2020; Oliver et al., 2021).
To date, self-referrals have accounted for only a small percentage of participants within ERS evaluations (e.g. 3% in Taylor et al. (2020)). As such, it is currently unknown whether certain referral characteristics are associated with an increased likelihood of participants accessing ERSs via self-referral, and whether there is an association between ERS completion and participants’ mode of ERS entry via referral from a healthcare provider or self-referral. This study documents the evaluation of Active West Lancs; a novel ERS due to its widespread inclusion of self-referrals. This study investigated associations between ERS participants’ referral characteristics and (1) the likelihood of accessing Active West Lancs via healthcare- or self-referral and (2) the likelihood of completion.
Methods
Study design
This evaluation comprised a cross-sectional exploration of key referral participant characteristics by mode of scheme entry and likelihood of scheme completion. Ethical approval was granted by the Sport and Physical Activity departmental research ethics committee at Edge Hill University(SPA-REC-2017-008). Participants referred to Active West Lancs’ ERS between May 2018 and January 2020 were presented with a participant information sheet and provided written consent for their data to be included in this evaluation, upon scheme sign-up.
Participants
Scheme eligibility criteria stipulated that participants were aged 18+ years, resided within the West Lancashire region of northwest England, and were experiencing or recovering from a long-term health condition. Scheme exclusion criteria were as follows: (1) unstable or uncontrolled angina, (2) uncontrolled asthma, (3) hypertension (blood pressure > 180/100 mm Hg), (4) hypotension (blood pressure < 100/60 mm Hg) and (5) pregnancy.
The ERS context
The scheme took the form of a 12-week gym-based intervention delivered free-of-charge across four community leisure centres in the West Lancashire region of northwest England. The scheme was advertised via flyers distributed through local community facilities (e.g. libraries, healthcare centres and social clubs) and promoted by healthcare providers during appointments with eligible prospective participants. Participants’ willingness to uptake the scheme was identified following referral from a primary or secondary healthcare provider (e.g. general practitioner, social prescribing link-worker), or via self-referral, with healthcare- and self-referrers noting the primary health-related reason for seeking referral and providing a mechanism of contact.
A project support officer contacted referred participants to (1) confirm their scheme eligibility and (2) arrange an exercise referral officer–led physical health assessment at the participant’s closest community leisure centre. During this assessment, exercise referral officers recorded participants’ demographic information including age, gender, postcode and primary long-term health condition on a paper-based referral form. Referral forms were stored in a secure filing cabinet within the central ERS office. Following their assessment, participants received an exercise referral officer–led gym induction and a bespoke PA training programme. Training programmes consisted of cardiovascular endurance or resistance-based exercises including the use of treadmills, cross-trainers and fixed weight machines. Participants also received a timetable of available exercise referral officer–supervised drop-in sessions and encouraged to attend at least two drop-in sessions per week. Drop-in sessions comprised neither group-based nor strictly one-to-one-based provision, with exercise referral officers sporadically and simultaneously supervising multiple scheme users throughout. All participants repeated the initial physical health assessment upon scheme completion at week 12. Participants who completed the scheme could subsequently sign-up to a 6-month gym membership at a significantly discounted rate. Provision and data recording were consistent among the four community leisure centres (sites A, B, C and D), with exercise referral officers operating across multiple sites. However, site A was located in an area of higher socioeconomic deprivation relative to sites B, C and D.
Data recording
Participants’ data were extracted from referral forms by the first author acting in the capacity of an embedded researcher involved as part of a wider evaluation and intervention design research project. Participants’ age, gender, primary health condition, postcode, site of referral, mode of referral and dropout reason were extracted directly from the referral forms on site at the central ERS office. Season of referral was generated by extracting the date of participant’s initial physical health assessment. Postcodes were used to generate indices of deprivation according to the English Index of Multiple Deprivation (Office for National Statistics, 2019). Socioeconomic deprivation status was re-categorised into quintiles of deprivation (1 = most to 5 = least deprived). Scheme uptake was classified as participants attending a physical health assessment at week 1. Participants were classified as ‘completers’ if they attended a physical health assessment at weeks 1 and 12.
Data analyses
IBM Statistical Package for the Social Sciences version 25 (IBM Corp, 2019) was used to conduct all analyses. Descriptive statistics (means and standard deviations) were calculated for continuous variables and normality distributions were assessed via inspection of histograms and q–q plots. Counts and percentages were calculated for gender, deprivation quintile, primary health condition, season of referral and presented separately according to mode of referral. Independent t-tests were used to investigate age differences in mode of referral and scheme completion. Effect sizes are presented in accordance with Cohen’s guidance where 0.01 = small, 0.06 = moderate and 0.14 = large effect (Cohen, 1988). Chi-square tests for independence (χ2) explored the associations between referral characteristics and mode of referral and scheme completion and mode of referral. Phi coefficients (2 × 2) or Cramer’s V and adjusted residuals (Z scores) are presented for 2 × ⩾ 3 analyses for effect size estimates. Z scores ± 2.0 indicate observed scores that are significantly higher or lower than expected (Agresti, 2002). Binary logistic regression analyses were conducted to investigate whether referral characteristics predicted the likelihood of (1) accessing the scheme via self-referral, and (2) scheme completion. Groups containing the largest number of participants were used as the reference categories for each predictor variable. Nagelkerke scores (r2) are presented to describe the variance and Hosmer and Lemeshow to assess goodness-of-fit for each respective model. Odds ratios (OR) and 95% confidence intervals (CI) are presented to demonstrate effect size. Statistical significance was set at p ⩽ .05.
Results
A total of 973 participants were referred to Active West Lancs between May 2018 and January 2020. The scheme had a 78.1% uptake rate (n = 760). Data for 113 participants were omitted as these participants were still enrolled when data collection for the study ceased. From this analytical sample of 647 participants, 42.2% completed the scheme (n = 273). Participants had a mean age of 55.84 ± 16.39 years and were predominantly women (60.4%, n = 391). Data for 10 participants were removed due to unknown mode of referral. Of the remaining 637, 282 (44.3%) accessed the scheme via a healthcare referral (56.18 ± 16.57 years) and 355 (55.7%) via self-referral (55.70 ± 16.41 years). Further descriptive characteristics are presented below according to participants’ status as a healthcare- or self-referral (Table 1).
Descriptive characteristics of participants by mode of referral.
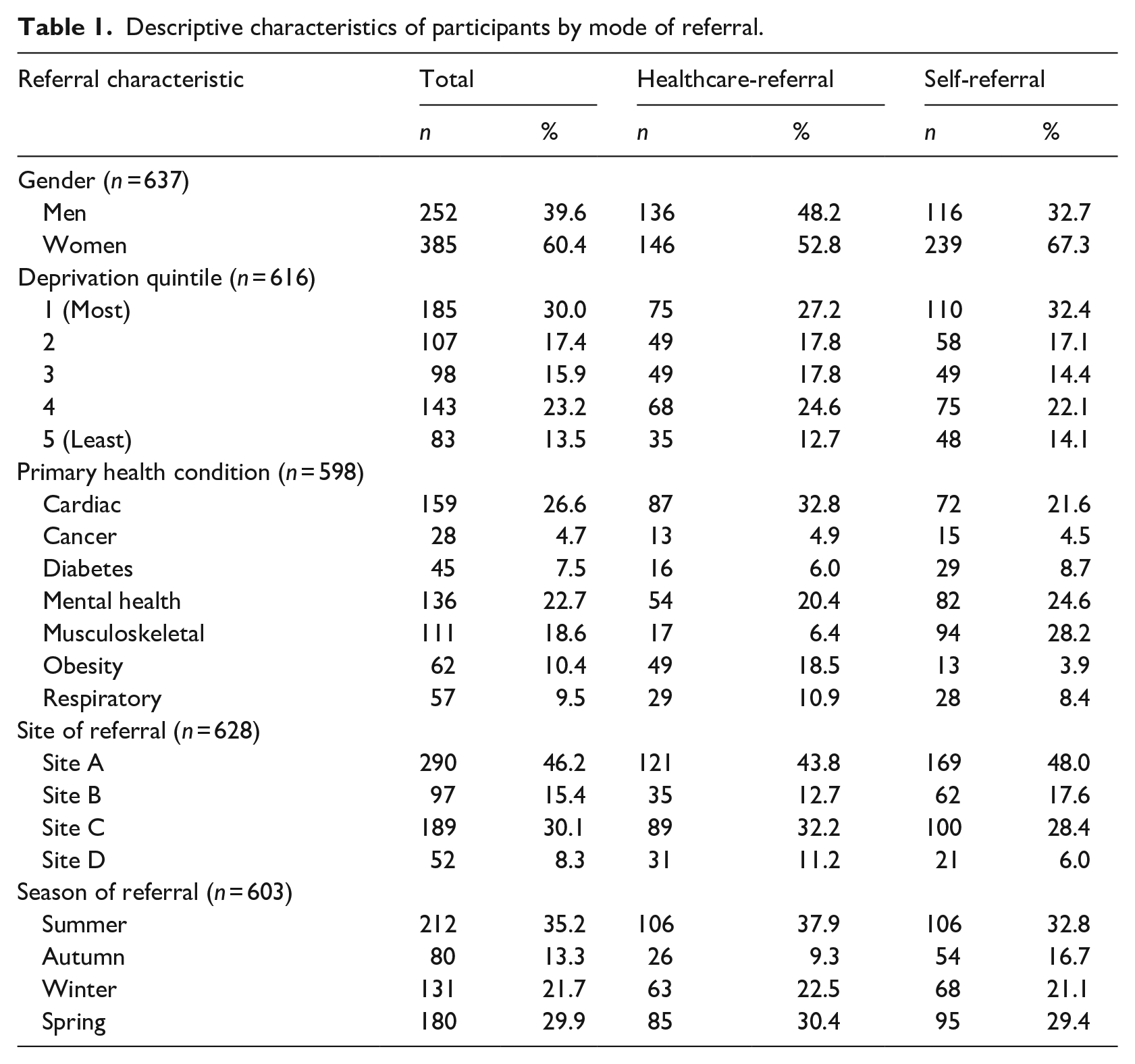
Healthcare- versus self-referrals
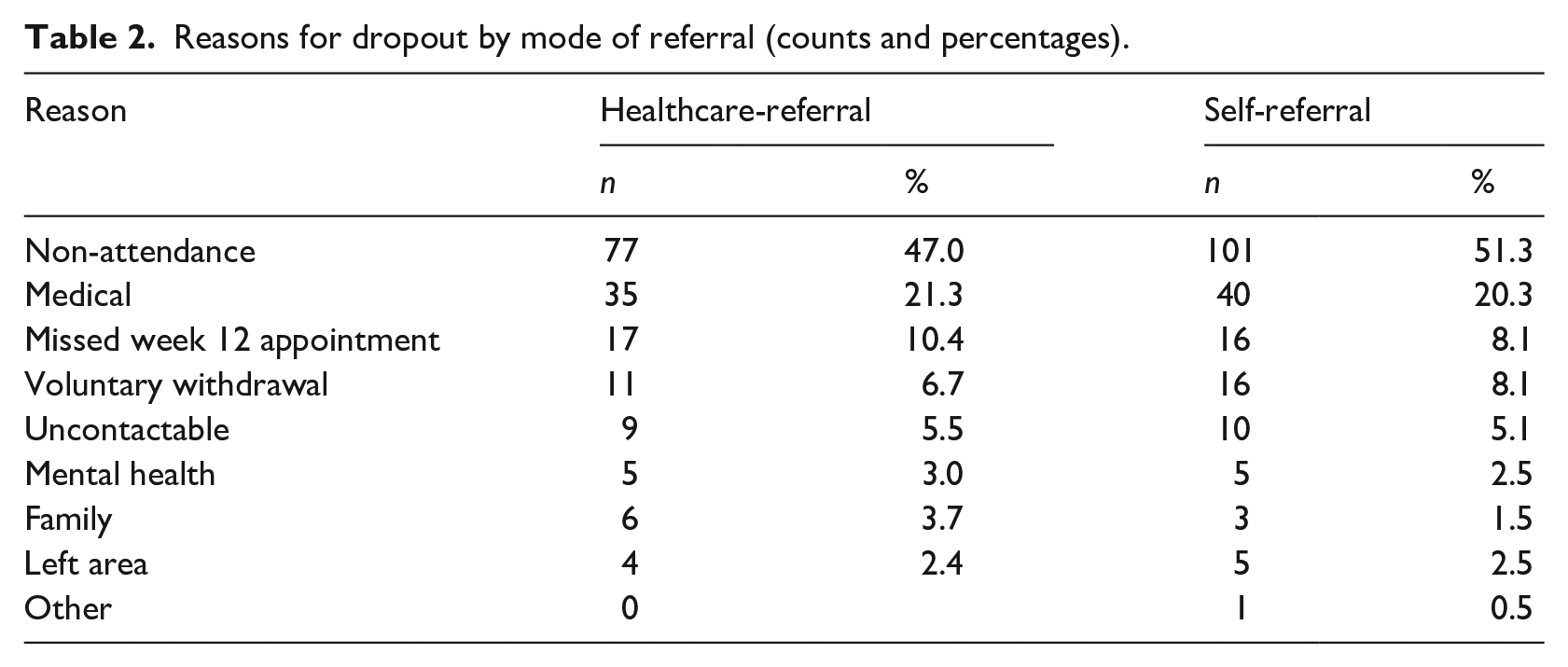
Chi-square analyses revealed significant associations between the mode of referral (healthcare- vs self-referral) and gender, χ2(1, n = 637) = 15.25, p < .001, phi = 0.16, primary health condition, χ2(6, n = 598) = 78.70, p < .001, Cramer’s V = 0.36, and site of referral, χ2(3, n = 628) = 8.96, p = .030, Cramer’s V = 0.12. Self-referrals were more likely to be women and to have reported a musculoskeletal health condition as their primary health condition (Z = 6.8). They were less likely to have reported a cardiac health condition (Z = −3.1) and to have attended site D (Z = −2.4) compared to healthcare-referral participants. There were no significant associations between mode of referral and deprivation quintile, season of referral, reason for dropout or scheme completion. There were also no significant differences in age between healthcare- and self-referral participants. Non-attendance was the primary reason for dropout across both healthcare- and self-referrals (see Table 2).
Reasons for dropout by mode of referral (counts and percentages).
Binary logistic regression was used to assess whether mode of referral was predicted by gender, age, deprivation quintile, primary health condition, referral site and season of referral for all participants who engaged in scheme uptake. The regression model was statistically significant, χ2(18, n = 542) = 126.25, p < .001, explaining 28.0% of the variance in mode of referral and correctly classifying 67.3% of cases overall (Healthcare = 61.9%; self = 72.1%). The Hosmer and Lemeshow test indicated excellent model fit (p = .941). As shown in Table 3, gender, primary health condition, site of referral and season of referral were significantly associated with mode of referral. Participants who reported a musculoskeletal primary health condition were over seven times more likely than those with a cardiac primary health condition to have accessed the scheme via self-referral (odds ratio [OR] = 7.18, [95% confidence interval [95% CI]: 3.57, 14.46]). Participants referred due to their diabetes were twice as likely to have accessed the scheme via self-referral (OR = 2.15, [95% CI: 1.03, 4.47]), whereas those with obesity as their primary health condition were nearly six times less likely to have self-referred (OR = 0.20, [95% CI: 0.09, 0.45]). With respect to the location of the sites, participants who attended site D were almost three times less likely to have accessed the scheme via self-referral than those at site A (OR = 0.36, [95% CI: 0.15, 0.89]). Self-referral participants were also more likely to be women (OR = 2.05, [95% CI: 1.37, 3.07]) and were almost three times more likely to have accessed the scheme in spring rather than in the summer (OR = 2.91, [95% CI: 1.51, 5.61]).
Binary logistic regression predicting the likelihood of self-referral.
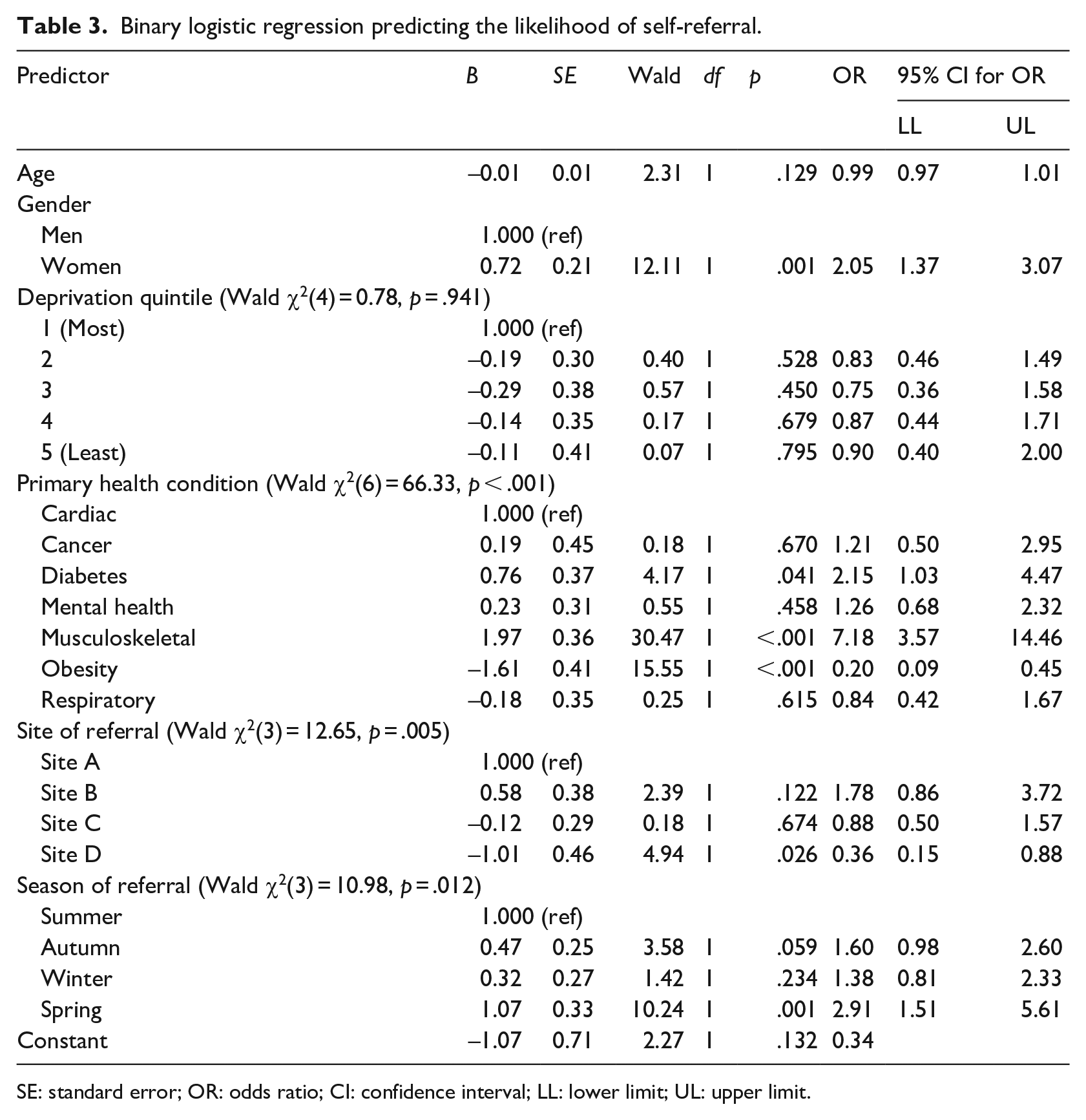
SE: standard error; OR: odds ratio; CI: confidence interval; LL: lower limit; UL: upper limit.
Completers versus non-completers
Scheme completers were significantly older (M = 60.00 ± 15.21) than non-completers (M = 53.00 ± 16.75; t(635) = −5.50, p < .001, d = 0.43). Significant associations were observed between scheme completion and gender, χ2(1, n = 637) = 4.33, p = .03, phi = −0.09, primary health condition, χ2(6, n = 598) = 16.86, p < .001, deprivation quintile, χ2(4, n = 616) = 44.39, p < .001, Cramer’s V = 0.27, and site of referral, χ2(3, n = 628) = 48.18, p < .001, Cramer’s V = 0.28. Completers were more likely to reside within the least deprived quintile (D5; Z = 5.7) and to have attended site B (Z = 6.8). Non-completers were more likely to be women (Z = 2.2), to report a mental health condition as their primary health condition (Z = 3.6), to reside within the most deprived quintile (D1; Z = 4.6) and to have attended site A (Z = 3.8).
Binary logistic regression was used to assess whether completion was predicted by gender, age, deprivation quintile, primary health condition, referral site and season. The regression model was statistically significant, χ2(19, n = 542) = 83.62, p < .001, explaining 19.2% of the variance in scheme completion and correctly classifying 68.6% of cases overall (non-completers = 85.6%; completers = 44.6%). The Hosmer and Lemeshow test indicated very good model fit (p = .884). As shown below in Table 4, age, deprivation quintile and site of referral were associated with an increased likelihood of scheme completion. Participants who attended site B were over three times as likely (OR = 3.22, 95% CI: 1.58, 6.56) to complete the scheme compared to those who attended site A. Older age significantly contributed to the increased likelihood of scheme completion (OR = 1.02, 95% CI: 1.00, 1.03) and completers were three and a half times more likely to reside in the least deprived area (OR = 3.67, 95% CI: 1.68, 7.99) than the most deprived area. Season of referral, primary health condition and scheme completion did not significantly predict scheme completion.
Binary logistic regression predicting the likelihood of scheme completion.
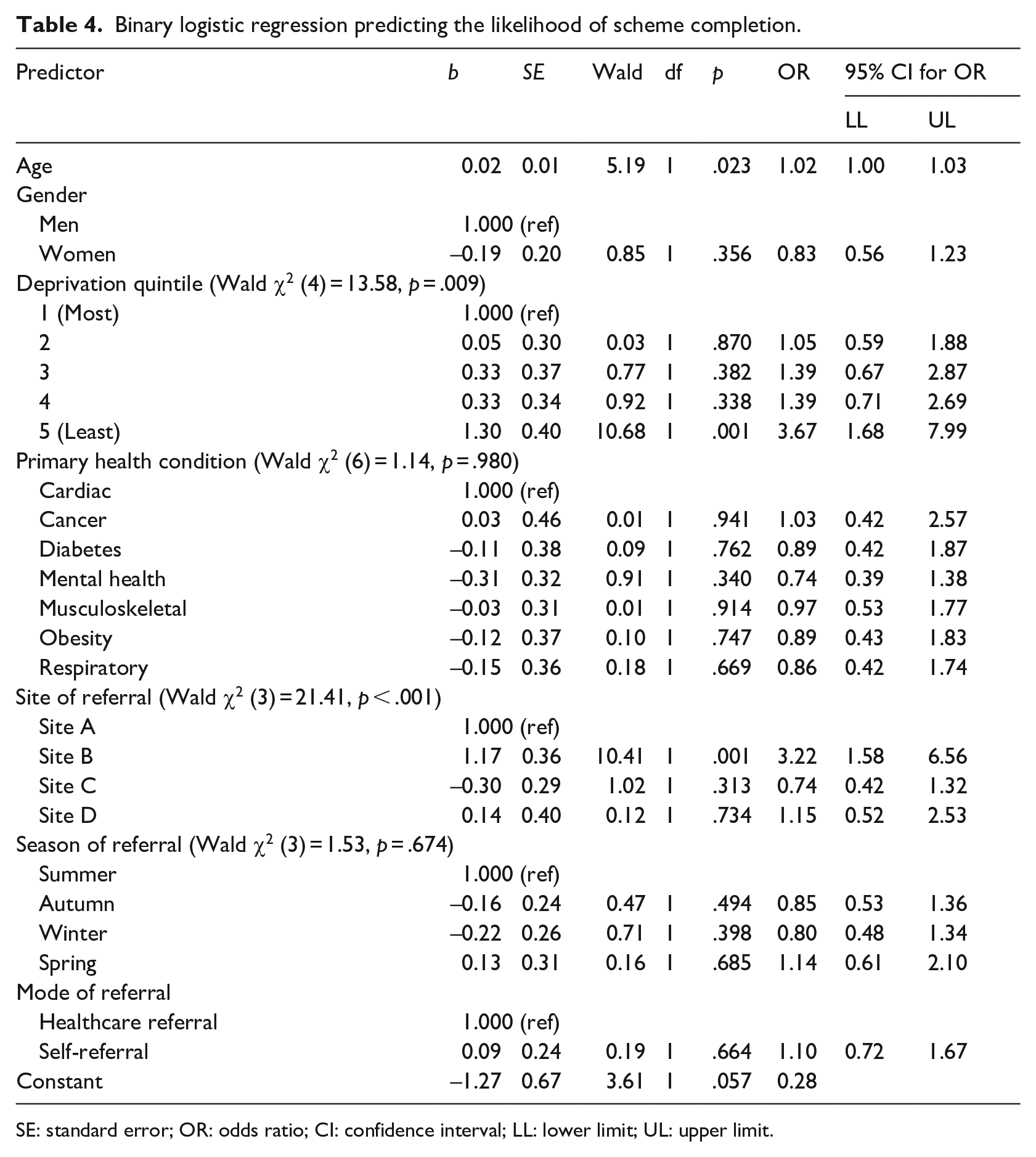
SE: standard error; OR: odds ratio; CI: confidence interval; LL: lower limit; UL: upper limit.
Discussion
This study explored associations between Active West Lancs participants’ referral characteristics, mode of scheme entry and scheme completion. The majority of participants were self-referral and these participants were more likely to be women and to report a musculoskeletal primary health condition or diabetes rather than a cardiac primary health condition. Self-referrals were less likely to report obesity as their primary health condition than a cardiac primary health condition. Self-referral participants were also less likely to refer to site D compared to site A, and to initiate referral in spring rather than summer. However, self-referral participants were not more or less likely to complete than healthcare referrals. Overall, 42.2% of participants completed Active West Lancs. Completers were older, resided within a less socioeconomically deprived and more likely to have attended site B than site A. Non-completers were more likely to be women and to have reported mental health as their primary health condition.
Age did not predict mode of entry, although increasing age did predict an increased likelihood of completion. Fewer time constraints (James et al., 2008), an increased desire for social interaction (Tobi et al., 2012) and easier incorporation of ERS-related activities into daily life (Campbell et al., 2015) may account for increased completion rates among older adults. Women accounted for 60.4% of the overall sample, supporting previous evaluations identifying an increased prevalence of women among ERSs relative to men (Hawkins et al., 2019; Morgan et al., 2020). James et al. (2008) postulated that this may reflect women being more likely to access a healthcare service and thus having a greater probability of receiving a referral. Here, women were also more likely than men to self-refer. Women participants’ increased likelihood of accessing Active West Lancs via self-referral may indicate that they perceived the scheme as representing a health-enhancing opportunity akin to other healthcare services. However, as elsewhere (Kelly et al., 2017; Pavey et al., 2012), women were less likely to complete. Collectively, there remains little consensus regarding gender differences in ERS engagement as other researchers have found no association between gender and ERS completion (Hanson et al., 2013, 2020) or higher rates of completion among women (Oliver et al., 2021). It remains unclear why women are less likely to complete some ERSs but not others.
Most participants reported a cardiac-, mental health– or musculoskeletal-related primary health condition. This is consistent with longitudinal evaluation of ERS participant referral characteristics by Morgan et al. (2020). In this study, participants who reported a musculoskeletal primary health condition or diabetes were more likely to access the scheme via self-referral than those with a cardiac primary health condition. Those reporting obesity as their primary health condition were less likely to access the scheme via self-referral than those with a cardiac primary health condition. Musculoskeletal primary health conditions, including joint pain and restricted movement, are easier to identify and self-diagnose than a cardiac-related health condition and thus may be more likely to trigger a self-referral-seeking response. In contrast, experience of a cardiac-related health incident is more likely to have resulted in a referral to Active West Lancs from a healthcare professional, with scheme uptake following prior completion of a dedicated cardiac rehabilitation programme. The existence of standardised rehabilitation pathways for those with a cardiac primary health condition may explain the observed differences in healthcare- and self-referral participants. The reduced likelihood of self-referral participants reporting obesity as their primary health condition may reflect a minor discrepancy between healthcare- and self-referral forms at the initial point of referral. Healthcare-referral forms included obesity as a distinct primary health condition, whereas self-referral forms did not. This does not indicate that participants here were less likely to be obese than in other ERSs, or that those who reported cardiac or musculoskeletal primary health conditions were not also obese. However, it may reflect a lower inclination for participants to self-report obesity relative to the reporting of a healthcare referrer. This also reflects the challenges of accurately categorising participants according to their primary health condition (Rowley et al., 2018), with many ERS participants presenting multi-morbidities (Prior et al., 2019). Referral due to a mental health primary health condition was associated with a lower likelihood of ERS completion. This is consistent with previous ERS evaluations (Kelly et al., 2017; Murphy et al., 2012) indicating that those with physical primary health conditions are more amenable to current forms of ERS provision. However, referral due to a mental health condition did not negatively predict ERS completion relative to referral due to a cardiac primary health condition.
Participants who entered via self-referral were less likely to access site D relative to site A. Referral to site A was associated with higher rates of non-completion, though only referral to site B positively predicted ERS completion. The underlying reasons for between-site differences in ERS engagement are complex and multifaceted (Hanson et al., 2013), however, contextual differences in how sites promote and operate their schemes can contribute to variable rates of between-site engagement (Din et al., 2015). At a surface level, the Active West Lancs delivery model remained consistent across all sites and the same exercise referral officers delivered drop-in sessions across multiple sites. In this regard, wider community-level contextual differences may be responsible for the observed patterns. For instance, it is possible that the healthcare services surrounding site D had lower awareness of Active West Lancs and thus were less likely to instigate a referral than those surrounding site A. In contrast, the healthcare services surrounding site D may have been efficient and proactive in promoting the ERS, thus reducing the need for self-referral. Notably, considerable disparity of socioeconomic deprivation status existed across the four sites, with participants who attended site A reporting the highest levels of deprivation. Socioeconomic deprivation status did not predict mode of entry. Higher socioeconomic deprivation has been previously associated with lower ERS uptake (Hanson et al., 2013). It is possible that participants’ ability to self-refer to Active West Lancs may have mitigated against the impact of key deprivation-related uptake barriers identified elsewhere (Hanson et al., 2013; Murphy et al., 2012). As in the study by Hanson et al. (2021), lower socioeconomic deprivation positively predicted completion. This contrasts with recent evaluations to report no association between socioeconomic deprivation and ERS completion (Shore et al., 2021), or high ERS engagement among the most socioeconomically deprived participants (Bell et al., 2021).
Mode of entry, healthcare- versus self-referral, did not predict scheme completion. As such, Active West Lancs’ incorporation of self-referral participants was not directly beneficial nor detrimental to participants’ likelihood of completing the scheme. Moreover, those who accessed Active West Lancs via healthcare- or self-referral shared largely similar referral characteristics. This potentially represents the existence of an equivalent susceptibility to scheme dropout due to shared exposure to the same myriad of organisational and interpersonal-related barriers, which ERS participants face (Morgan et al., 2016). Notwithstanding this, wider incorporation of self-referral participants may have positive implications for the long-term sustainability of ERSs. Foremost, permitting self-referral access enables schemes to exhibit greater control and ownership over the ways in which they operate. Previous ERS participants have cited a lack of communication between referral sites and ERSs as a barrier to uptake (Birtwistle et al., 2019). Schemes that afford self-referral access may be able to navigate beyond poor or inconsistent communication links with healthcare referrers by taking a more active role in promoting scheme awareness within their own communities.
In addition, enabling self-referral access can benefit schemes and prospective scheme users by enhancing the ease in which schemes can be accessed and accelerate the speed at which eligible participants can gain access to ERSs. ERSs which predominantly rely on referrals from primary and secondary care providers are dependent on prospective participants’ initial willingness to engage with these services. Demographic sub-populations such as men, who may be more reluctant to access healthcare services (James et al., 2008), may benefit from the option to self-refer to ERS as it affords them the opportunity to bypass these services. Finally, wider incorporation of self-referral ERS participants may alleviate unnecessary burden from healthcare services by eliminating the need for self-referral-seeking individuals to first engage with a healthcare provider. The current wide inclusion criteria means that the majority of those seeking referral to ERSs are highly likely to be eligible, often reducing the healthcare-referrer role to that of gatekeeper acting to prevent schemes from becoming overwhelmed (Din et al., 2015; Moore et al., 2013). The Active West Lancs model demonstrates that ERSs can modify their delivery practices to accommodate self-referral participants without becoming overwhelmed.
Collectively, widespread incorporation of self-referral ERS participants can have notable research and policy implications. Poor cost-effectiveness is a pervasive and salient critique against the promotion of ERSs (Campbell et al., 2015). Permitting self-referral access can lessen the economic cost of ERS delivery by alleviating prospective scheme users’ need to access healthcare services prior to uptake. Future research can further explore the economic viability of self-referral ERSs relative to traditional models of ERS delivery.
Limitations
A limitation of this study was its inability to discriminate between distinct types of healthcare referrers. There is evidence to suggest that variable rates of ERS completion exist in accordance with the mode of healthcare referral (Hanson et al., 2013; Kelly et al., 2017). However, it was not possible to discriminate between different modes of healthcare referral in this study and thus, there remains scope for further investigation of rates of ERS completion by mode of referral. In addition, this study did not collect data on attendance. As such, while participants could be classified as completers or non-completers based on their attendance of physical health assessments at weeks 1 and 12, this does not account for how many sessions participants attended between these time points, which is likely to be a key factor in determining ERSs effectiveness for facilitating health enhancing outcomes (Shore et al., 2019).
Conclusion
This study demonstrates positive associations between discrete referral characteristics, including gender and primary health condition, and mode of ERS entry, healthcare- versus self-referral. Women, and those with primary referral reasons of a musculoskeletal primary health condition and diabetes were more likely to have accessed the scheme via self-referral. Men, and those who had a primary referral reason such as obesity or cardiac condition were more likely to access the scheme via healthcare referral. Mode of referral did not predict completion. Because of this, while this study’s findings cannot provide inference for if, or how, rates of ERS completion may directly benefit from wider incorporation of self-referral participants in the future, the inclusion of self-referral participants is unlikely to be directly detrimental to ERS completion rates. Moreover, permitting self-referral ERS access can yield additional community- and organisational-level benefits. These may include increasing the accessibility of ERSs within the wider community and alleviating undue burden from local healthcare services traditionally responsible for administering referrals.