
Abstract
Sport participation is an important part of the development, both physically and mentally, of children and adolescents in the United States. Illness and injury associated with sport and physical activities may occur in the school setting. Although most sport-related illness and injury in students are considered minor emergencies, life-threatening illnesses or injuries may occur. It is important for the school nurse to recognize potential life-threatening emergencies associated with sport and physical activity, to initiate stabilization of the student with life-threatening symptoms, and to triage these students to an appropriate level of care (back to the classroom, home with their guardian with follow-up at their primary healthcare provider’s office, or directly to the closest emergency department [ED] via Emergency Medical Services [EMS]). This article specifically describes the initial assessment and management of shortness of breath in an adolescent athlete during a track event.
Who Is the ER Pediatrician?
Dr. Robert Olympia, MD, is a pediatric emergency medicine physician with more than 20 years of experience, currently working in an emergency department in the Sweetest Place on Earth (Hershey, PA). He is a professor in the Departments of Emergency Medicine and Pediatrics at the Penn State College of Medicine. His research interests include emergency and disaster preparedness for children in the setting of schools and school-based athletics, as well as in sport-related illness and injuries. He has presented his research both regionally and nationally and has lectured on a variety of topics pertaining to pediatric emergency medicine, such as fever and infectious diseases, trauma, sports-related injuries, and disaster preparedness.
Who Is Dr. Olympia’s Coauthor?
Dr. Thomas Swaffield, MD, is currently a third-year General Pediatrics resident physician at the Penn State Hershey Children’s Hospital and will be starting a Pediatric Sports Medicine fellowship at the Children’s Hospital of Philadelphia in the summer of 2022.
What Is the Purpose of the “School Nurses on the Front Lines of Healthcare” Series?
The “School Nurses on the Front Lines of Healthcare” series presents cases reflecting emergencies commonly encountered in the school setting, focusing on an evidence-based approach to the initial management, stabilization, and disposition of the ill or injured child.
Special features unique to each article are Extra-Credit Points and Report Cards. Extra-Credit Points are trivia questions or clinical pearls scattered throughout the article related to the topic at hand. Report Cards are concise tables summarizing key points in each article that you can photocopy and laminate, or photograph and keep on your smart device, for easy access.
Case 1
You are helping out the medical team for a spring weekend track event. Abigail, a 15-year-old participant in a long-distance race, is brought into the medical tent by her father who saw her struggling to breathe and coughing during the race. Abigail, who had “reactive airways” as a toddler but hasn’t had issues since then, complains of chest tightness, difficulty breathing, and chest pain when taking a deep breath. You notice that her breathing is labored and fast, and that she is unable to speak in full sentences. Upon auscultation of her lungs, you notice that she has poor air movement, especially at the lung bases, with scattered wheezing. What do you think is going on, and what do you do next?
What Should You Consider When a Pediatric Athlete Is Having Difficulty Breathing: Remember Taking Some “BREATHS”?
You quickly take out your laminated card with the mnemonic for causes of respiratory distress in a child or adolescent student: “BREATHS,” which stands for “Brain, Respiratory, Entrails (gastrointestinal tract), Airway, Trauma, Heart, and Shock” (Loaec & Olympia, 2018). Based on your history and initial assessment, you believe that the most likely etiology for Abigail’s respiratory distress is “Respiratory.”
In healthy children and adolescents, exercise-induced bronchospasm (EIB) is often the most common cause of respiratory distress during or after physical activity (Bhatia et al., 2019) However, other etiologies for shortness of breath during physical activity should be considered. Deconditioning, vocal cord dysfunction, exercise-induced hyperventilation, and chest wall abnormalities can all contribute to shortness of breath in the exercising pediatric athlete. Deconditioning is common and results in hyperventilation (fast breathing) due to accumulation of lactate (a chemical produced during strenuous exercise) at a lower exercise threshold. Vocal cord dysfunction is associated with inspiratory stridor (high-pitched sound when taking a deep breath indicating an upper airway obstruction) or wheeze, common in athletes with upper chest or throat symptoms. Exercise-induced hyperventilation, typically associated with anxiety, can lead to shortness of breath and feelings of chest tightness. Finally, mild pectus deformities (anatomic deformities of the chest wall) or scoliosis (anatomic deformities of the spine) can cause restrictive lung physiology, therefore affecting the expansion of the lungs on inspiration and contributing to shortness of breath.
What Is Exercise-Induced Bronchoconstriction (EIB)?
EIB, also known as exercise-induced asthma (EIA), describes airway narrowing that occurs during exercise (Klain et al., 2022). EIB can occur in individuals with or without a diagnosis of asthma or reactive airway disease. Approximately 90% of people with asthma or reactive airway disease can experience EIB, while the incidence of EIB in people without a previous diagnosis of asthma or reactive airway disease is 20%. Sports associated with an increased risk of EIB include those that require a long duration of exercise, especially in colder environments, such as cross-country running, cycling, downhill/cross-country skiing, ice hockey, swimming, and triathlons.
Prompt treatment and prevention of EIB is vital for optimal patient outcomes. Short-acting beta agonists (such as albuterol) are the preferred first-line medication for the treatment of shortness of breath associated with EIB. The American Thoracic Society also recommends the use of albuterol 5 to 20 minutes prior to exercise or sport, citing strong evidence that this can help prevent bronchoconstriction episodes. Inhaled corticosteroids can also be beneficial to prevent exacerbations; however, these medications take roughly 1 month to see optimal benefit and therefore should be initiated a few months before the season starts. Other preventive strategies include increasing general exercise endurance and lowering body weight in obese athletes.
The ABC’s of Shortness of Breath
The initial management of a pediatric athlete with shortness of breath includes the ABC’s: assessment of A (Airway), B (Breathing), and C (circulation) (Loaec & Olympia, 2018). Let’s focus on Airway and Breathing:
Is the athlete able to speak to you? If he or she is able to speak, then his or her airway is open.
If the athlete is unconscious or cannot speak, open their airway with simple positioning (head tilt–chin lift) and clearing any secretions or vomitus from their airway, if present.
Suspicion of an obstructing foreign body (an athlete who is gagging or drooling, presenting with stridor [a high-pitched sound that can be heard without a stethoscope on inspiration], or in the “tripod” position [athlete leaning forward, neck is hyperextended, mouth is open, and both arms extended forward in front of them, as in a camera tripod]) may require immediate use of the Heimlich maneuver.
Severe allergic reactions can result in airway edema and loss of airway, as well as involvement of the cardiovascular, pulmonary, and gastrointestinal systems, and therefore immediate recognition and administration of an epinephrine autoinjector, if available, is of paramount importance.
Finally, in an athlete with airway compromise, it is important to keep them as comfortable as possible. Crying, screaming, or hyperventilation may compromise their airway even further.
What is the athlete’s respiratory rate? The normal respiratory rate is 20 to 30 breaths per minute for elementary school-age children and 12 to 20 breaths per minute for older children and adolescents. Are their lips blue (consistent with cyanosis, or lack of oxygen in their blood)? Does the athlete have evidence of respiratory distress (fast or labored breathing, shallow breaths, absent chest rise, suprasternal or intercostal retractions)? If you have a stethoscope readily available, listen for breath sounds in all lung fields. There should be good aeration in all lung fields without crackles, rales, or wheezing. Athletes experiencing an exacerbation of asthma or lower airway obstruction will often have an increased respiratory rate and may have either decreased lung sounds or abnormal breath sounds, most commonly wheezing, on auscultation. Wheezing is often heard most clearly at the end of expiration and is described as a high-pitched whistling sound. In more severe cases (lack of air movement), there will be an absence of breath sounds in occluded airways, resulting in an absence of auscultated wheezing. In athletes with pneumonia, you may be able to auscultate crackles/rales (high-pitched sounds on inspiration) and/or rhonchi (low-pitched sounds on inspiration).
Extra-Credit Point: When Should an Athlete With Respiratory Distress Be Transported to an Emergency Department (ED)?
Athletes with significant respiratory distress should be transported by Emergency Medical Services (EMS) to your local ED (Table 1).
REPORT CARD: Life-Threatening Presentations of Respiratory Distress Requiring Immediate Transport to an ED
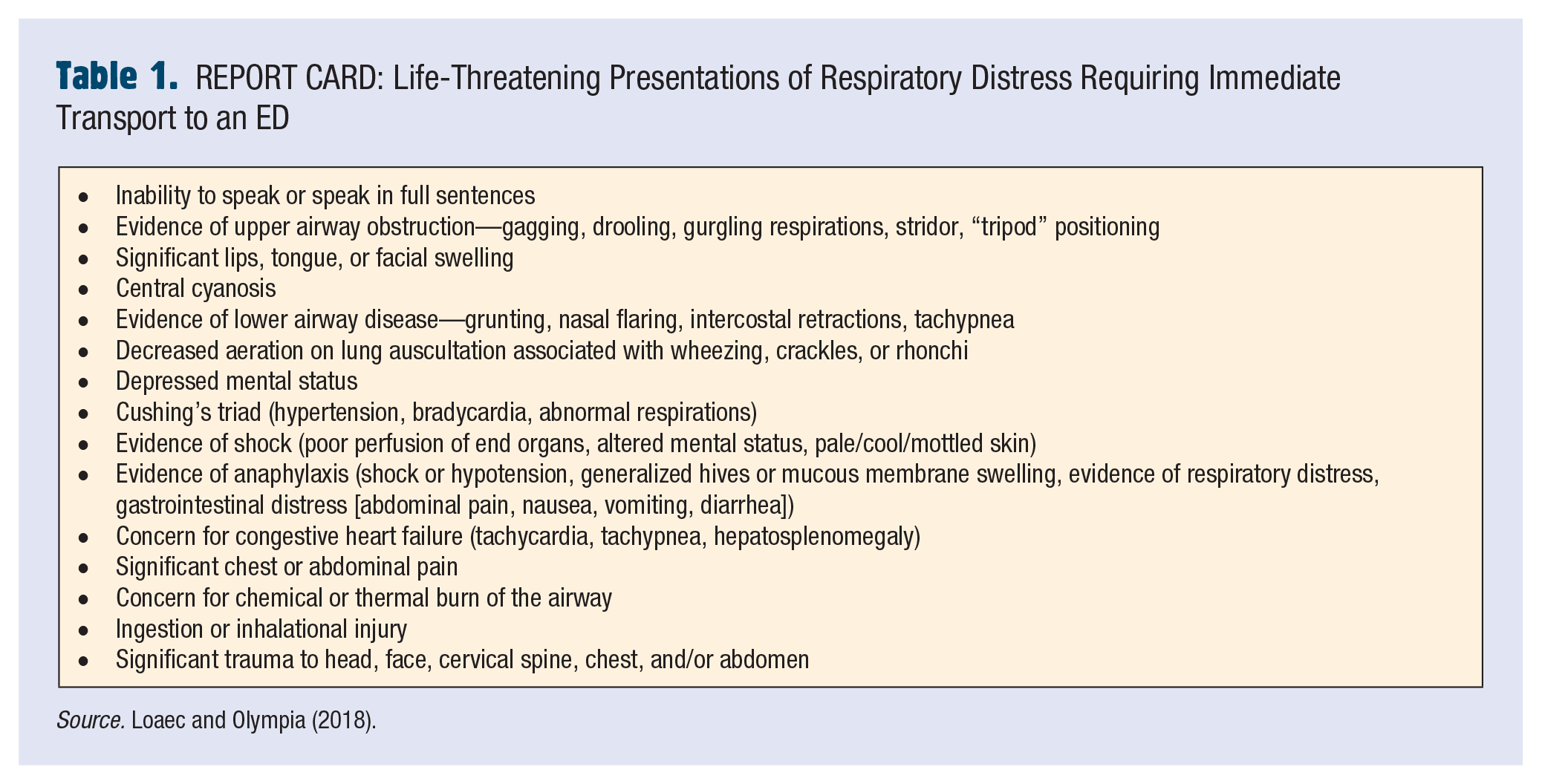
Source. Loaec and Olympia (2018).
The Other ABC’s of Shortness of Breath
In a pediatric athlete with shortness of breath due to EIB, the “A” of ABC’s may be albuterol and in severe cases, the “E” may be epinephrine (regular or pediatric dosage based on the student’s weight). Prompt administration of albuterol initiates bronchodilation of the small airways and improves oxygenation and ventilation (Patel & Teach, 2019). In a pediatric athlete with a previous diagnosis of asthma or reactive airway disease, close attention should be directed to the athlete’s Asthma Action Plan, if available, to determine acute management based on severity of symptoms. For pediatric athletes without a diagnosis of asthma or reactive airway disease, or if their Asthma Action Plan is not readily available, administration of albuterol via an inhaler with spacer, four to eight puffs every 15 minutes is appropriate until EMS arrives. If available, intramuscular epinephrine may be used in a pediatric athlete with significant signs of respiratory distress (depressed mental status, cyanosis, slowed breathing after a period of fast breathing [“tiring out”], or no movement of air on lung auscultation). Epinephrine administration results in immediate opening of constricted airways while you wait for the bronchodilation effects of albuterol to work. School nurses must be aware of state laws related to stock albuterol and stock epinephrine in the school setting and around school-sponsored athletic events prior to their administration for athletes without a history of or action plan for asthma or anaphylaxis.
Case 1 Resolution
After recognizing EIB, you promptly call EMS for transport and administer four puffs of an albuterol inhaler with a spacer. In route to the ED, despite continuous albuterol nebulizer therapy, Abigail is noted to be hypoxic with an oxygen saturation of 88%. In the ED, Abigail is placed on continuous albuterol treatment with ipratropium (Atrovent), given intravenous methylprednisolone, and supplemental oxygen. After an hour of respiratory treatments, Abigail feels better with less chest tightness and cough, although she remains hypoxic on room air. She is admitted to the ED observation unit, receives supplemental oxygen and albuterol treatments every 4 hours, and discharged home the following day.
Conclusion
Shortness of breath is a common complaint of pediatric athletes during or after physical activity. Quick assessment of the athlete’s ABC’s is important to determine treatment and disposition. EIB can occur in pediatric athletes with or without a diagnosis of asthma, and treatment of the athlete by the school nurse should be based on predetermined action plans or state laws regarding stock albuterol and epinephrine.
Footnotes
Robert is a physician boarded in both Pediatrics and Pediatric Emergency Medicine with more than 20 years of clinical experience. His research interests include emergency and disaster preparedness for children in the setting of schools and school-based athletics.
Dr. Thomas Swaffield, MD, is currently a third-year General Pediatrics resident physician at the Penn State Hershey Children’s Hospital and will be starting a Pediatric Sports Medicine fellowship at the Children’s Hospital of Philadelphia in the summer of 2022.