
Abstract
Objectives
This study aimed to investigate the impact of COVID-19 on the training of anesthesiologists in Hong Kong.
Introduction
COVID-19 has caused a substantial impact on anesthesiology training in multiple domains. The challenges faced by both trainees and educators remain a significant concern and adaptations in clinical teaching are warranted. We conducted this study to quantify the impact and identify learning areas in recurring pandemics.
Methods
Electronic surveys were distributed to anesthesiology trainees and fellows in Hospital Authority in Hong Kong. Data from respondents were collated and analyzed. Reliability analysis and exploratory factor analysis (EFA) were performed.
Results
A total of 97 responses were collected and analyzed. Majority (59% of trainees and 79% of fellows) agreed that the COVID-19 pandemic negatively impacted anesthesia training overall. Bag-mask ventilation and direct laryngoscopy were the 2 most affected areas in airway training; 47% of fellows observed a technical skill decline among trainees. Most respondents (64% of trainees and 71% of fellows) agreed that simulation sessions could help with residents’ training. Exploratory factor analysis indicated the following subscales: loss of educational opportunities, loss of caseload and formal training, loss of technical skills (regional and procedural), loss of technical skills (airway management), the hampering of ICU rotations, and difficulty teaching residents.
Conclusion
The COVID-19 pandemic has caused disruptions in caseload, technical skills training, work-based assessment, and continued medical education, hampering both trainees’ and fellows’ education. Measures to counter the effect of the pandemic were discussed. Our findings will help educators better understand the challenges, marshal resources, and plan to enhance trainees’ educational experience.
Introduction
The global coronavirus epidemic COVID-19 has greatly affected traditional anesthesiology training. 1 This has been multifactorial, contributed by the large reduction of elective and emergency surgeries, difficulty in teaching airway skills during intubation of COVID-19 patients, cancellation of examinations, increased stress leading to worsening mental health, as well as personal quarantine and illness. 2
Accredited anesthesiologists may feel deskilled in certain areas. In-person conferences and workshops have been canceled, leading to a reduction in hands-on training opportunities. While online webinars have replaced some in-person teaching, anesthesiology training still requires procedural skill teaching and hands-on practice. These skills have been difficult to impart to new trainees, as current guidelines for airway management in COVID-19 cases call for the most experienced clinicians to perform intubations and procedures to decrease the risk of failure and reduce the exposure of clinical staff. Along with redeployments to nonanesthetic units and reduction of caseloads, this has reduced trainees’ opportunities to perform procedures and acquire the necessary skills. This may disproportionately affect junior trainees.
The cancellation of examinations, difficulty in completing logbooks and conducting work-based assessments may lead to a delay in the graduation and accreditation of trainees. These may have important negative repercussions on trainees, on both their confidence as well as mental health.3–9 Overall the COVID-19 pandemic has seen a reduction of technical skills of surgical and anesthesia residents due to training interruptions, 6 and the gap in clinical education remains a significant concern. Pandemics are anticipated to be recurrent; it is thus important to examine in detail the challenges both trainees and educators are facing and explore solutions to preserve professional standards.
In this study, we performed the first survey of Hong Kong anesthesiologists to delineate how the COVID-19 pandemic has impacted the teaching and training of anesthesiology residents, and to identify important areas where supervisors of training, departmental heads, and other program directors might be able to marshal limited resources to improve residents’ educational experience during a pandemic, as well as share perspectives and best practices to stimulate professional growth.
Methods
This was a multicenter questionnaire survey study. Two separate surveys were designed, 1 for trainees and 1 for fellows. Content validation was performed by one of the authors, Dr Albert Chan, an expert in medical education (Master of Health Professions Education, Maastricht University). A pilot survey was conducted to collect opinions from 6 anesthesiologists on the design of questions. The final version of both surveys consisted of 30 questions each (Supplemental file 1, 2) and was constructed in Google(™) Forms. The first few questions established the demographics of the respondents. The remaining questions were 5-point Likert items ranging from “strongly disagree” to “strongly agree.” 10 Data reflecting redeployments and rotations and change in caseloads due to COVID-19 were collected. The closed-response questions addressed the impacts of the COVID-19 pandemic on anesthesia training and education. There were 3 open-text options to input personal experiences and challenges, as well as opinions on areas of improvement. Participation in the study was voluntary and anonymous. Written informed consent was taken for participation in and publication of the study. All anesthesiologists including trainee anesthesiologists (residents) working in the Hospital Authority (public hospitals) in Hong Kong were included in the study. Surveys that were incomplete were excluded.
The survey was approved by the Research Ethics Committee (Kowloon Central/Kowloon East) (Ref.: KC/KE-22-0084/ER-1). The study enrolled anesthesiologists and trainees in Hospital Authority (public hospitals) in Hong Kong via electronic methods (email and reminders via messaging). Survey respondents had to consent to publication and participation in order to proceed with the survey. Distribution of surveys was coordinated by the Trainee Committee and Young Fellow Committee in the Hong Kong College of Anaesthesiologists. The survey remained open from July 18, 2022 to November 17, 2022.
Statistical Analyses
A sample size of 86 was calculated by approximating members in the Hong Kong College of Anaesthesiologists to be 800 with an expected response rate 10%, and utilized a 95% confidence level and a margin of error of 10%. Statistical analysis took the form of descriptive statistics expressed in percentages. Internal consistency of the survey was measured by Cronbach's alpha with a bootstrap 95% confidence interval based on 1000 samples. An alpha of <.5 was considered unacceptable, .5 to .6 was poor, .6 to .7 was questionable, .7 to .8 was acceptable, .8 to .9 was good, and >.9 was excellent. Reliability analysis was performed to investigate the impact of individual questions on overall consistency. For the trainee survey, these were based on 12 questions (Q8, Q11, Q12, Q14, Q16, Q17, Q18, Q19, Q20, Q22, Q25, and Q26), and for the fellow survey, these were based on 12 questions (Q7, Q10, Q11, Q13, Q14, Q18, Q19, Q20, Q23, Q24, Q25, and Q27). None of the questions included were reverse-scored and the items were not randomized between respondents. A Cronbach's alpha of 1.0 would be expected if the top radio button were marked for all items by a participant. As this was the first survey of its kind, we performed a post hoc exploratory factor analysis (EFA) on both the trainee and fellow surveys. Since the data were ordinal and non-normal, we used a principal axis factor estimator to extract the variances from the data. Given that this was an educational survey and factors were likely to correlate to one another, an oblique rotation was chosen, but the data was also analyzed using orthogonal rotations for completeness. Visual inspection of the scree plot and parallel analysis (PA) was utilized to determine the number of factors. We built a correlation matrix of the results and visually inspected a scree plot and PA to estimate the number of factors. Utilizing EFA, we ran multiple factor models, increasing the number of factors by one until all models were run. The pattern matrices were examined focusing on whether the factors made theoretical sense. Low pattern coefficients were considered to be <0.40 to keep as many items as possible from the original scale. R studio (version 4.3.1) was used to perform any statistical analysis.
Results
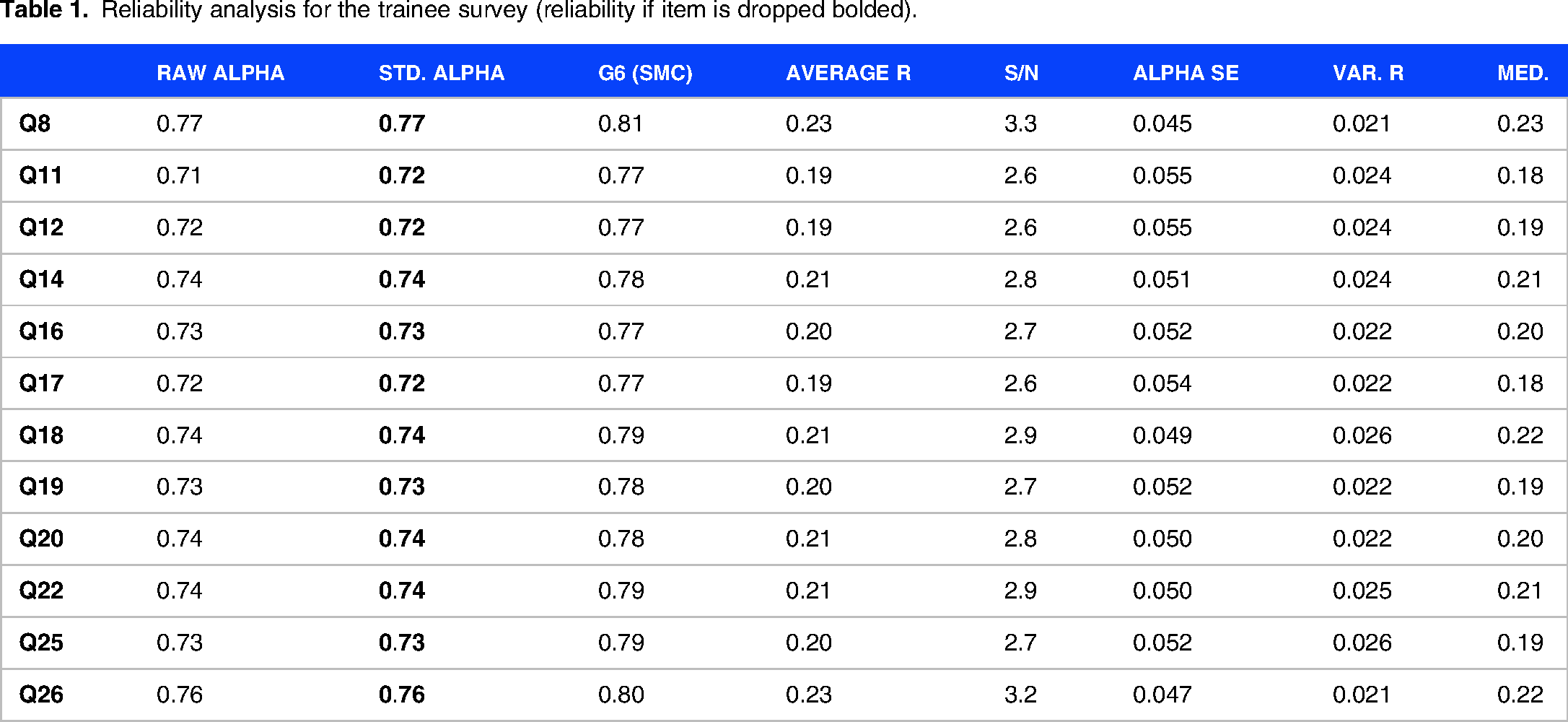
A total of 97 responses (approximately 12% of the population) were received and included in the final analysis, 59 from trainees; and 38 from fellows. There was no missing data and all surveys submitted were complete. Margin of error based on 95% confidence level was ±9%. The internal consistency of the trainee survey was acceptable. Cronbach's alpha was 0.77 (95% CI 0.63-0.83). The internal consistency of the fellow survey was questionable, with a Cronbach's alpha of 0.68 (95% CI 0.46-0.79). Reliability analyses of both surveys were performed and did not detect any outlier questions, with no improvement in the reliability if any of the items were dropped for both surveys (Table 1 and Table 2).
Reliability analysis for the trainee survey (reliability if item is dropped bolded).
Reliability analysis for the fellow survey (reliability if an item is dropped bolded).

For both the trainee and fellow surveys, the correlation matrix found weakly positive correlations between most questions. The scree plot and PA indicated a leveling out between 2 and 5 factors (Supplemental file 3).
In the trainee survey, the 2-factor solution consisted of one factor that had high pattern coefficients for items that represented the loss of learning opportunities for specific technical skills as well as opportunities for work-based assessment, explaining 18% of the variance in the data, and a second factor that had high pattern coefficients for the negative impact in formal-training, eg, caseload and postponement of courses, explaining 13.6% of the variance in the data. The total variance explained by the 2-factor model was 31.6%. In the 3-factor solution, the third factor only included one item with pattern loadings greater than 0.40 and was deemed unsuitable. The 4-factor solution split apart the loss of technical skills items and opportunities for work-based assessment. The 5-factor solution (Table 3) further parsed the subscales into loss of educational opportunities, loss of caseload and formal training, loss of technical skills (regional and procedural), loss of technical skills (airway management), and the hampering of ICU rotations. The total variance explained by the 5-factor solution was 53.4%, and all the items were accounted for. In the 6- and 7-factor solutions, the sixth and seventh factors included only one item with pattern loadings greater than 0.40 and were thus deemed inappropriate.
Five-factor solution of the trainee's survey. a

Abbreviation: WBA, work-based assessment.
Bolded numbers indicate pattern coefficients >0.40.
In conclusion, the EFA indicated a 2-factor or 5-factor solution. We chose a 5-factor solution as it allowed us to retain all of the original items and made theoretical sense, and was a further parsing of the original 2 scales. The items seemed to fit on 4 subscales that were represented by items related to (1) loss of opportunities for technical skills (which can be split into airway skills and procedural skills), (2) loss of educational opportunities, (3) loss of caseload and training, and (4) hampering of ICU rotations.
For the fellow survey, the 2-factor solution consisted of one factor that had high pattern coefficients for the items related to the negative impact of COVID-19 on the residents’ training, explaining 20% of the variance in the data, and another for difficulty in teaching during COVID-19, explaining 12.4% of the variance in the data. The total variance explained by the 2-factor model was 32.4%. The 3-factor model did not make any improvements to the 2-factor model and split the difficulty in teaching regional anesthesia into a separate factor. The 4-factor model (Table 4) included the majority of the items and consisted of one factor that had high pattern coefficients for items related to the decline of technical skills of residents during COVID-19, another factor for items related to COVID-19's negative impact on formal training, another factor for items related to difficulty teaching residents during COVID-19, and another factor for fewer opportunities for residents during COVID-19. In the 5-, 6-, and 7-factor models, the several factors only had one item with pattern loading greater than 0.40 and were thus deemed unsuitable. Question 23 “Do you find difficulty in conducting teaching during the COVID-19 pandemic overall?” had cross-loading for multiple factors, which was likely due to the overly generalized nature of the question.
Four-factor solution of the fellow's survey. a

Abbreviation: WBA, work-based assessment.
Bolded numbers indicate pattern coefficients/pattern coefficients >0.40.
In conclusion, the EFA indicated a 4-factor solution. It retained the majority (10 of 12) of the original items and made theoretical sense. The items fit on 4 subscales that were represented by items related to (1) the decline of technical skills of residents, (2) COVID-19's negative impact on formal training, (3) difficulty teaching residents, and (4) the loss of learning opportunities for residents.
Respondent demographics including age, gender, years of experience, training post occupancy, and working hospital are displayed in Table 5.
Respondent demographics.

Abbreviations: PMH, Princess Margaret Hospital; PWH, Prince of Wales Hospital; PYNEH, Pamela Youde Nethersole Eastern Hospital; QEH, Queen Elizabeth Hospital; QMH, Queen Mary Hospital; TKOH, Tseung Kwan O Hospital; UCH, United Christian Hospital; NDH/AHNH, North District Hospital/Alice Ho Miu Ling Nethersole Hospital; KWH, Kwong Wah Hospital; TMH, Tuen Mun Hospital.
As seen in Figure 1, 32% of trainees and 24% of fellows underwent redeployment to another department due to COVID-19 pandemic, with Intensive Care Unit being the most frequent site. Among those 39% had been redeployed for 1 to 2 weeks; 28% redeployed for 3 to 4 weeks; 28% redeployed for more than 6 weeks. 42% of trainees and 58% of fellows agreed that COVID-19 pandemic had hampered trainees’ interhospital or ICU rotations.

Number of respondents with redeployment during COVID-19 pandemic.
More than 90% of the respondents reported a decrease in average elective caseload during COVID-19 pandemic. Around 20% of the respondents reported a decrease in average elective caseload of more than 50% (Figure 2). For emergency caseload, around half of the respondents reflected a similar caseload to pre-COVID era (Figure 3). 29% of trainees were concerned about inadequate caseload due to the pandemic for their anesthesia training and logbook fulfillment. 45% of fellows had the same concern for trainees.
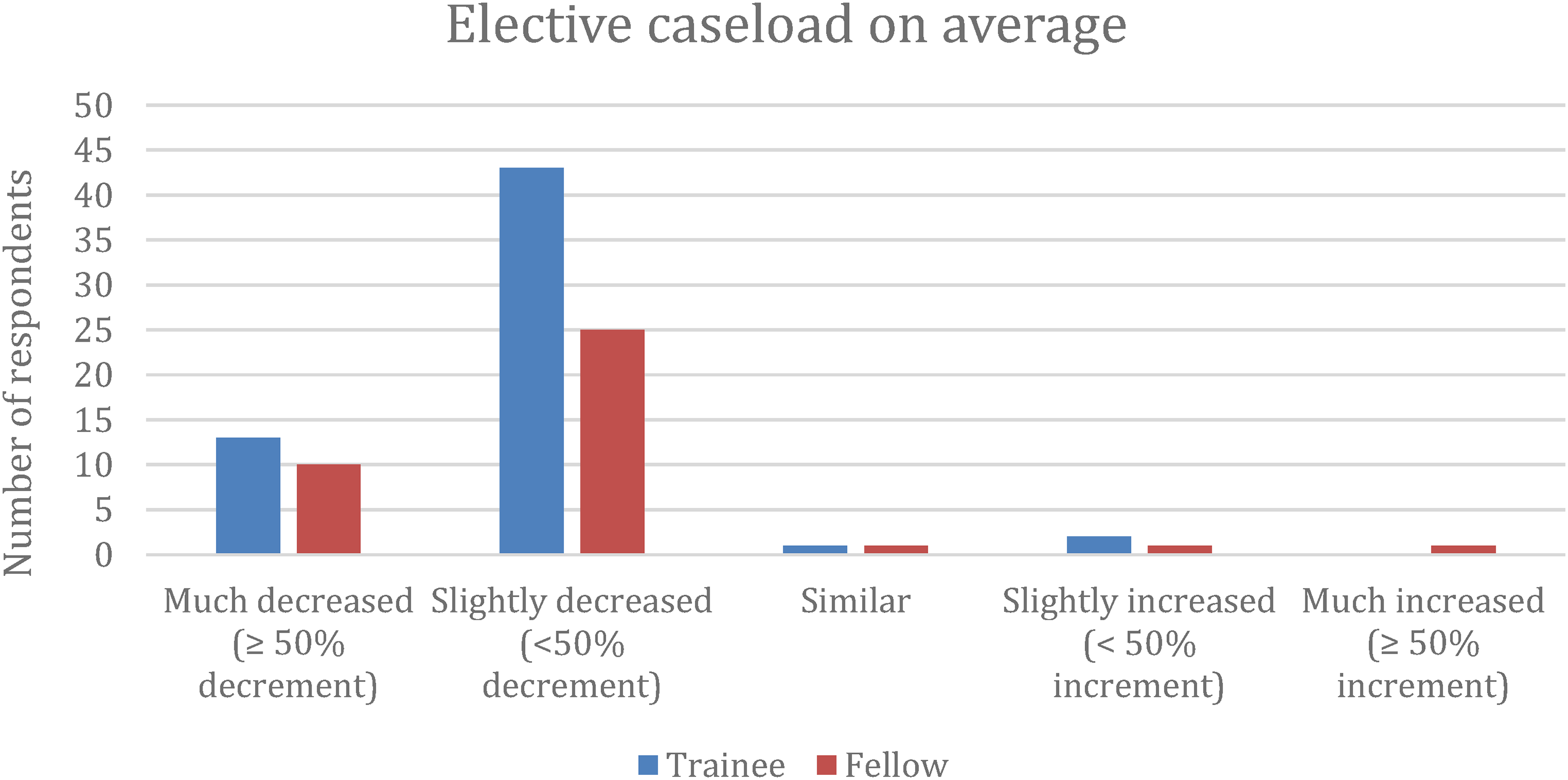
Elective caseload on average during COVID-19 pandemic.
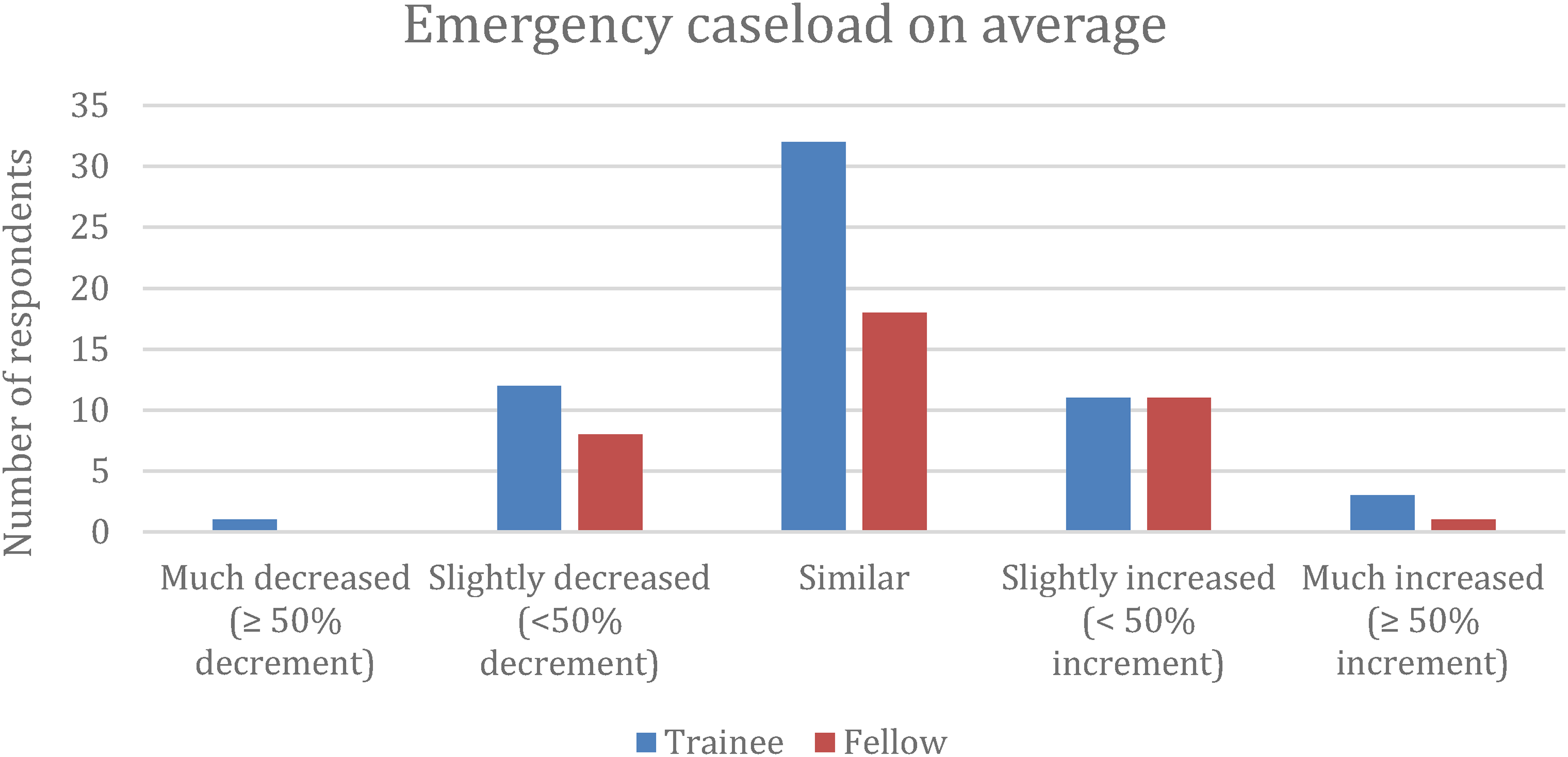
Emergency caseload on average during COVID-19 pandemic.
59% of trainees and 79% of fellows agreed that COVID-19 pandemic negatively impacted anesthesia training overall. Among the various subspecialty training, day surgery was the most affected category, with pediatrics and nonoperating theatre anesthesia being the next (Figure 4). 70% of trainees reported fewer opportunities in practicing airway management skills. Correspondingly, 84% of fellows selected airway management skills as the most impacted area among trainees. Bag-mask ventilation (90% and 95%) and direct laryngoscopy (71% and 68%) were the 2 most affected areas (Figure 5).

Subspecialty training most affected by COVID-19 as reported by trainees.

Most affected area(s) in airway management training as reported by trainees and fellows.
Majority (70% of trainees and 76% of fellows) disagreed that COVID-19 pandemic had hampered learning or teaching of regional anesthesia skills. 76% of fellows commented that there were areas positively affected by the pandemic, with regional anesthesia and infection control being the most mentioned ones. As for other procedural skills such as arterial line and central venous catheterization, 61% of trainees disagreed with fewer opportunities in learning or practicing these skills. 25% of trainees felt that their technical skills had decayed since COVID-19 outbreak, while 47% of fellows observed such decline (Figure 6); 37% of fellows found difficulty in conducting teaching during the pandemic overall, and 29% felt less confident in residents’ competence in practicing independently after the pandemic (Figure 7).

Technical skill decay among trainees as reported by trainees and fellows.

Percentage of fellows feeling less confident in residents’ competence in practicing independently.
A minority of respondents (14% of trainees and 8% of fellows) felt that WBA was less valuable during COVID-19 pandemic. Inadequate caseload, inadequate manpower, and lack of case varieties were the difficulties in conducting WBA during the pandemic. 42% of fellows found difficulty in performing direct observation of procedural skills (DOPS) for trainees.
64% of trainees and 71% of fellows agreed that organizing simulation sessions during the pandemic could help with residents’ anesthesia training (Figure 8); 15% of trainees and 26% of fellows disagreed that their units had been organizing adequate simulation sessions; 25% of trainees and 50% of fellows felt that changes in educational activities had hampered continued medical education; 66% of trainees expressed concern about cancellation or postponement of mandatory courses held by the college.

Helpfulness of simulation sessions on anesthesia training during COVID-19 pandemic as reported by trainees and fellows.
In the open text questions, trainees and fellows expressed that clinical teaching had changed in the way of hampered airway skill training, reduced caseload, and face-to-face interaction. As for methods to improve education during the pandemic, most respondents commented that simulations, tele-education, and online resources could be utilized.
Discussion
The COVID-19 pandemic has posed unprecedented challenges to postgraduate medical training. Anesthesiology is one of the most impacted specialties as technical skills and procedural competency are essential in everyday practice. A study has shown that reduced caseload, subspecialty experience, and supervised procedures among anesthesia trainees due to COVID-19 impaired learning. Cancelled educational activities, postponed examinations, and altered rotations also threatened training progression. 11 Our survey is the first interhospital study investigating the impact of COVID-19 pandemic on anesthesiology training in Hong Kong. As seen in the statistical analyses, internal consistency of the trainee survey was acceptable (0.77) and that of the fellow survey was questionable (0.68). The reliability of both surveys was excellent.
The impact of COVID-19 on anesthesia training was multifactorial. One of the subscales found in the EFA of both the trainee and fellow survey was the loss of learning opportunities. Caseload is crucial in anesthesia training as teaching of clinical management and technical skills relies heavily on adequate exposure and experience, and inadequate caseloads may impede training progression. COVID-19 pandemic has caused reductions in elective operation lists. Compared to a nationwide survey in Canada where only 1% of respondents reported >50% reduction in procedure volume, 12 the situation in Hong Kong during the peak of a COVID wave was worse, with 20% of respondents in our survey reporting >50% reduction.
Overall, the majority of respondents in both trainee and fellow surveys felt that COVID-19 pandemic has a negative impact on anesthesia training, which was another subscale identified by the EFA. Airway management training was the most affected aspect in our results. The recommendations for intubation of COVID-19 patients place an emphasis on strategies to minimize aerosolization of virus from airways. Modified rapid sequence induction has been advocated and manual bagging is discouraged. 13 Videolaryngoscopy has broadly replaced direct laryngoscopy to increase first-attempt success rate. This practice is observed to extend toward non-COVID-19 patients in the operation theatre. Correspondingly, most of the survey respondents reflected hampered training on bag-mask ventilation and direct laryngoscopy, which are fundamental skills in anesthesia. This corresponded to a subscale (loss of technical skills) found in the EFA for both surveys. In our study, 25% of trainees self-reported technical skill decay since the COVID-19 outbreak, compared to a 64% perceived reduction in technical skills among surgery and anesthesia residents in a survey study conducted in New York. 6 Lack of airway skill training remains a great concern to trainees’ competency, the effect of which will be evident even after the end of pandemic. Similar impact has been reflected in a study conducted in Cairo University Hospital which found that the training in technical skills was less in during-pandemic resident group than that in before-pandemic group. 14 Trainees across 6 continents from British Journal of Anaesthesia's partner organizations similarly reported reduced caseload and less complex case mix, reduced subspecialty experience and supervised procedures. Opportunities in practicing aerosol-generating procedures including bag mask ventilation, tracheal intubation, and tracheostomy are particularly lessened. 11
As shown by the EFA, difficulty teaching and loss of formal training and learning opportunities were subscales identified in both the trainee and fellow survey. This corresponds to the fact that traditional time-based or volume-based measures of progress may not be fully achievable in the COVID-19 era. 15 Face-to-face courses and conferences were largely canceled or postponed. Continued medical education in the COVID-19 era has to be modified. Teleplatforms and virtual learning for medical education have been advocated by the Accreditation Council for Graduate Medical Education. 15 In Plymouth, trainee meetings organized weekly have gained more importance. Combining onsite and remote access increases participation. 11 Majority of our respondents agreed that simulation sessions would be beneficial for training. CME meetings and Annual Scientific Meeting have been organized via teleplatforms. Regarding continuation of training and progression, temporary flexibility is offered in the United Kingdom's anesthesia curriculum to facilitate training progress. 11
The challenges from COVID-19 pandemic have called for innovations beyond traditional teaching methods. Medical education in response to COVID-19 pandemic has been increasingly studied. 16 Online learning is one of the most deployed developments. Success from both synchronous and asynchronous teaching relies on promoting engagement via teaching strategy modifications 17 and well-designed online learning modules with combination of webinars, group discussions, and practice questions. 18 Faculty and college are encouraged to make adaptations by means of resources curation and online teaching delivery.19,20 Trainee preparatory courses, procedural videos, meetings, and conferences can be recorded and uploaded to online platforms for educational purposes. Simulation and virtual reality can be employed for airway and regional skill training, crisis management in COVID-19 patients, echocardiography, and interventional procedures. The importance of physical teaching with patient contact is still emphasized in postgraduate training, the risk of which can be mitigated with the use of personal protective equipment and appropriate distancing. 21 Besides knowledge and skill acquisition, mental health protection is another highlighted area in the COVID-19 era. 22 Strategies to promote psychological well-being include providing psychologically safe environment for staff, encouraging communication, preventing social stigmatization, and peer support. 21
The impacts demonstrated in this study are observed worldwide and across various medical specialties. A systematic review on medical and surgical education challenges in the COVID-19 era has pinpointed the adversities of both undergraduate and postgraduate training. 23 Our results are especially generalizable to specialties with high dependency on hands-on training as reduction in experience translates plausibly to weakened skills. In a survey conducted in 2 large academic medical centers in New York, a majority of faculty respondents perceived a reduction in technical skill among surgical and anesthesiology residents. Residents shared a similar concern about returning to the operating room with worse skill and impaired ability to practice independently. 6
Although to date COVID-19 pandemic has started waning, its impact on anesthetic residents’ training remains due to lost training opportunities that cannot be recovered. Recurrent pandemics are almost a certainty. It is believed that COVID-19 may develop into possible scenarios including persistent outbreaks of severe disease, transition into an epidemic seasonal disease or endemic disease with lower morbidity and mortality, 24 and continue to exert negative impacts on anesthesia training. This study quantifies the impacts of a pandemic on anesthesia training and can guide educators to develop alternative approaches to ensure the continuity of education during similar pandemics. This should include planning for clinical rotations and examination formats, support for online and simulation training, safety measures for clinical teaching, as well as strategies to maintain mental well-being. An example of a structured program is Self-isolAting Virtual Education (SAVEd) project described by anesthetists in the North West School of Anaesthesia, UK. It incorporates prerecorded and live online tutorials, with addition of live MCQ polls and informal conversation among trainees. 25 Additional training should be provided to junior trainees on bag mask ventilation and direct laryngoscopy, which were the most affected skills from our findings.
Limitations
Our study has several limitations intrinsic to survey study design. Respondents were subject to recall bias. This was reduced by distributing the survey just following the peak of a COVID wave. Objective data such as logbook information were not obtained since trainees’ logbooks are not consistently updated. Perceived technical skill decay was self-reported and there was no objective measure for evaluation. The strength of our study is that the questionnaire was validated by a subject matter expert, and trainees’ and fellows’ opinions were collected separately for direct comparison. The scales used in our study were original and not yet validated, so pilot surveys were performed. We were unable to obtain extra actual demographic data of the population studied due to privacy rules, which hampered the comparison of our respondent demographics to the population demographics. The respondent population was mostly doctors in public and government practice, who were in training or were trainers, compared to a nonrespondent population which included doctors in private practice who were not likely involved in teaching. While we performed a sample size calculation of 800 which is the total number of anesthesiologists (fellows and trainees) in Hong Kong, this number includes anesthesiologists who are in private practice and are not trainees nor trainers. The actual number of trainees and trainers is likely half that number (approximately 400), and the demographic data of the survey respondents were estimated to be similar to that of the population studied. The respondents are therefore a good representation and proportion of the studied population.
We did not perform follow-back surveys due to potential recall bias as it was approaching one year post epidemic and due to the long collection period. Although the internal consistency of the fellow's survey was questionable, the reliability was good and the EFA made theoretical sense. While EFA is generally used in larger sample sizes, studies have shown that it can yield reliable results for sample sizes below 50, even in the presence of small distortions. 26 However, as the chosen models had multiple factors with 3 or 4 items per scale and pattern coefficients of >0.4, a larger sample size would have provided more confidence with our results. 27 One of the questions on the fellow survey (Q23) was overly general and resulted in cross-loadings for multiple factors. We did not run a confirmatory factor analysis as any confirmatory factor analysis run on the same data would lead to confirmation bias. 28 As the data set was small, we were unable to split the data into 2 parts to perform separate exploratory and confirmatory factor analysis. Performing a second survey for a confirmatory factor analysis was likely to have a lower response rate and may be hampered by recollection bias.
As the response rate was suboptimal (12%), there is a risk of nonrespondent bias and this is an important limitation. We minimized nonresponse bias through pretesting the survey with a pilot survey. We kept the survey short and simple to keep responding time within 10 to 15 min, and targeted the survey audience through the Hong Kong College of Anaesthesiologist's updated database. We improved the reach of the survey through both e-mail and mobile-phone messages, and the survey could be completed on a mobile web-browser. Reminders were sent to complete the survey and we maintained a collection period of 5 months. However, as nonresponders were likely anesthesiologists who were neither in training nor trainers, nonresponse bias analyses were not performed. While our results are generalizable to procedural specialties and those involved in airway management such as Emergency Medicine and Intensive Care, they may be less generalizable to nonprocedural specialties, such as Internal medicine.
Conclusion
The COVID-19 pandemic has posed a major impact on anesthesiology training in Hong Kong. Factors identified by the EFA included loss of educational opportunities, loss of caseload and formal training, loss of technical skills (regional and procedural), loss of technical skills (airway management), the hampering of ICU rotations, and difficulty teaching residents. This hampered both trainees’ and fellows’ professional development. Measures to counter the effect of the pandemic have to be undertaken to sustain professional training in the field. These involve supplementing traditional teaching with online learning, simulation with virtual reality, and mental health protection. In the face of recurring pandemics, our findings will help educators better understand the challenges, marshal resources, and plan ahead to enhance trainees’ educational experience.
Supplemental Material
sj-pdf-1-mde-10.1177_23821205231216264 - Supplemental material for The Impact of COVID-19 on the Training of Anesthesiologists in Hong Kong: Overcoming the Challenge
Supplemental material, sj-pdf-1-mde-10.1177_23821205231216264 for The Impact of COVID-19 on the Training of Anesthesiologists in Hong Kong: Overcoming the Challenge by Kevin Kai Wai Chan, Timothy Xianyi Yang and Albert Kam Ming Chan in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-2-mde-10.1177_23821205231216264 - Supplemental material for The Impact of COVID-19 on the Training of Anesthesiologists in Hong Kong: Overcoming the Challenge
Supplemental material, sj-pdf-2-mde-10.1177_23821205231216264 for The Impact of COVID-19 on the Training of Anesthesiologists in Hong Kong: Overcoming the Challenge by Kevin Kai Wai Chan, Timothy Xianyi Yang and Albert Kam Ming Chan in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-3-mde-10.1177_23821205231216264 - Supplemental material for The Impact of COVID-19 on the Training of Anesthesiologists in Hong Kong: Overcoming the Challenge
Supplemental material, sj-pdf-3-mde-10.1177_23821205231216264 for The Impact of COVID-19 on the Training of Anesthesiologists in Hong Kong: Overcoming the Challenge by Kevin Kai Wai Chan, Timothy Xianyi Yang and Albert Kam Ming Chan in Journal of Medical Education and Curricular Development
Footnotes
Authors’ Contribution
KKWC conceived and designed the analysis, collected the data, performed data analysis, interpreted the data, and wrote the paper. TXYY and AKMC also conceived and designed the analysis, performed data analysis, interpreted the data, and wrote the paper. All authors approved the manuscript.
Availability of Data and Materials
The dataset supporting the conclusions of this article is available from the corresponding author upon reasonable request.
Consent for Publication
Written informed consent for participation and publication was obtained from all participants before accessing the survey.
Ethics Approval and Consent to Participate
The survey was approved by the Research Ethics Committee (Kowloon Central/Kowloon East) (Ref.: KC/KE-22-0084/ER-1). All methods were performed in accordance with the relevant guidelines and regulations. Written informed consent for participation and publication was obtained from all participants before accessing the survey. Aside from demographic data, no personal data were recorded.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.