
Abstract
Objectives
Medical schools have sought to incorporate concepts of race and racism in their curricula to facilitate students’ abilities to grapple with healthcare disparities in the United States; however, these efforts frequently fail to address implicit bias or equip students with cultural humility, reflective capacity, and interpersonal skills required to navigate racialized systems in healthcare. The purpose of this study was to develop and evaluate an antiracism narrative medicine (NM) program designed by and for preclinical medical students.
Method
Preclinical medical students at a single center were eligible to participate from June-July 2021. Program evaluation included a postprogram qualitative interview and electronic survey. The semistructured interview included questions about program experience, lessons learned, and perspectives on antiracism curricula in medical education. Interviews were qualitatively analyzed using open and axial coding. Survey data were analyzed with descriptive statistics.
Results
A total of 30 students registered. All (100%) respondents reported “somewhat true” or “very true” in the postprogram survey when asked about their ability to reflect on their own racial identity, racial identity of others, and influence of their racial identity on their future role as a healthcare worker through the program. Qualitative analysis revealed 3 themes: (1) curricular engagement; (2) racism and antiracism in medicine; and (3) group experience. Subthemes included: meaningful theoretical content; multimodal works and unique perspectives; race, identity, and intersectionality; deeper diversity, equity, and inclusion engagement; reconstructive visions; future oriented work; close reading and writing build confidence in discomfort; community and support system; and authentic space among peer learners.
Conclusion
This virtual, peer-facilitated antiracism NM program provided an engaging and challenging experience for participants. Postprogram interviews revealed the program deepened students’ understanding of racism, promoted self-reflection and community building, and propagated reconstructive visions for continuing antiracism work.
Introduction
Medical school curricula have evolved to incorporate cultural competency1–4 and sociostructural determinants of health5–8 over past decades. Recently, topics that more directly grapple with racism have been included9–13 to address the disparities pervasive in United States healthcare. 14 Previous studies have reported on implicit biases among medical students,15–18 and the importance of addressing those biases during training.19,20 Yet, there is an ongoing need for solutions to equip future physicians with adequate knowledge, reflective capacity, and sustainable tools for navigating and improving racialized structures during and beyond medical education.21–23
Narrative medicine (NM) is a health humanities field that facilitates reflection of interpersonal and structural forces that shape a patient and provider's relationship to healthcare,24–26 while promoting self-reflection, cultural humility, and professionalism.27–33 In its most recent turn, NM methods have been applied toward understanding racism in medicine.34–37 However, there is limited literature on the use of NM methodology on educational programming that specifically focuses on antiracism in medicine.
Many previous antiracism efforts have been led by medical educators,9,12,38–40 and several have been met with the challenges of differential student needs, institutional inertia, and desire for more institutional and personal accountability.41–43 Medical students have historically played an integral role in galvanizing curricular change and promoting social justice, but the potential benefits of a medical student-led antiracism program are underexplored.43–46 Herein, the authors saw a gap in medical education that could be uniquely filled.
The goal of this study was to develop and evaluate a medical student-led antiracism program for preclinical medical students using NM methods. This program built upon a successful NM-based diversity, equity, and inclusion (DEI) program for faculty at the same institution. 35 The goal was to develop a novel curriculum in both content and facilitation that would be uniquely developed, implemented, and qualitatively evaluated by peer medical students. The authors hypothesized that a student-led curriculum would provide a distinctively meaningful experience compared to traditional DEI and antiracism programming.
Materials and methods
Setting and participants
This is a prospective single-center medical education program that was assessed through a mixed-methods survey and semistructured qualitative interviews. Medical students at a single institution in the Southeastern United States, who were between their first and second years of preclinical education were eligible to participate. Thus, inclusion criteria were (a) being a preclinical medical student at the study institution who had completed at least one year of medical school; (b) > 18 years of age; (c) have teleconferencing capabilities on a personal device; and (d) availability to attend 4 virtual hour-long sessions on predetermined dates. Exclusion criteria were (a) being a clinical phase student; and (b) inability to attend sessions on predetermined dates. The program was developed by 2 medical students (YI and SH) at the same institution who completed graduate training in NM prior to medical school.
The University of North Carolina Institutional Review Board (#20-3548) reviewed and deemed this study exempt. While informed consent was waived, all participants were notified of the risks, benefits, and goals of the study through a standardized research information form before participating in the program. The program was co-sponsored by the medical school's Office of Diversity, Equity, and Inclusion, Columbia University's Narrative Medicine Program, and the medical school's local Gold Humanism Honor Society (GHHS) chapter.
Program description
The program curriculum, including learning objectives, are outlined in Table 1. Four sessions were held in sequence for each group of students. Participants completed required presession readings that were discussed in the first 20 min of each session. The remaining 40 min were reserved for an NM workshop, which included close reading of a creative work, discussion, a prompt-driven writing exercise, and sharing of individual writing. Creative works included poems, multimedia audio work, and a visual art exhibit.
NM antiracism program curriculum.

Abbreviation: NM, narrative medicine.
The curriculum and facilitation materials were developed in discussion with expert scholars in NM and race. Specifically, the creative works and NM prompts were selected in consultation with NM faculty who had extensive teaching experience in narratives of social justice, activism, embodiment, and abolition at the graduate level. The theory-based texts were selected in consultation with a local cultural sociology and race scholar (AMR) at the medical students’ home institution. This faculty member's expertise is in diversity discourse in education, Black feminist thought, and non-normative Black masculinity and sexuality. The curriculum was curated by the lead medical students and iteratively revised with the aforementioned NM faculty members, cultural sociology faculty, and a supervising health humanities faculty member at the host institution.
Program sessions covered topics including the history of racism in US healthcare, deconstructing whiteness as the “transcendental norm,” 47 policing in medicine, abolition medicine, and re-imagining medicine as an antiracist practice. The fourth workshop on re-imagining antiracism in medicine was held in conjunction with the Ackland Art Museum, which has a history of educational programming with the medical school. 13 An art educator from the museum co-facilitated this session and provided sociohistorical context for the artwork that was discussed. This art educator has extensive experience in medical education, including facilitation of a workshop series on race that had been hosted at the medical school previously. Participants had the opportunity to engage with the sculpture through the museum's virtual viewing platform.
Participant recruitment and incentives
Participants were recruited through the medical school's listserv using a standardized script in March 2021. An additional announcement was made at a mandatory class meeting. Medical students were sent a survey link to express interest in the program. To maximize participation, all students who met inclusion criteria were registered for the series. No formal power calculations were made for statistical purposes.
Program incentives were 2-fold. Participants who attended at least 3 of the 4 sessions and completed associated evaluation tools received a hard-copy and electronic certificate of completion co-signed by the sponsoring organizations: Office of Diversity, Equity, and Inclusion, Columbia University's NM Program, and local GHHS chapter. Students could also have their participation in the program be included in their Medical Student Performance Evaluation for residency applications. Students were informed of these incentives when the program was advertised. There was no cost associated with program participation.
Additionally, participants who completed the 30 to 60min qualitative postprogram interview had the option of receiving a $10 gift card or having a $10 donation in their name to a community organization advocating for housing justice, civil rights, and local history education.
Program facilitation
Participants were divided into 4 groups. Each group had no more than 8 participants. Group assignments were random except for students with scheduling conflicts. Each group was assigned 2 facilitators. One facilitator was a medical student at the home institution (YI and SH) and the second facilitator was an NM graduate student from an outside institution (FGL). The facilitators intersectional identities and experiences include the following: YI is an Asian woman with graduate training in narrative medicine, teaching experience in the carceral system, and research experience on the intersection of incarceration and health; SH is a white woman with graduate training and multidisciplinary teaching experience in narrative medicine and qualitative research experience within the maternal and child health and medical education fields; FGL is an Afro-Latinx queer man with graduate training in narrative medicine and psychology, with specific research experience on the psychological benefits of safe online spaces for Black same-gender loving men, and the impact of systematic white supremacy and policing on suicidality across race and sexual identities.
Four 60min sessions were held over a videoconferencing platform (Zoom Video Communications Inc, San Jose, CA). The program was administered from June-July 2021 over a 2-month period when students had no required coursework. There were 4 total groups (each with 4 sessions) that were staggered: 2 groups began in the third week of June; 2 groups began in the fourth week of June. One group met in the morning, one during lunch hours, and 2 groups during the evening to maximize engagement.
Program evaluation
A mixed-methods approach was undertaken to evaluate the program. Participants were asked to complete a preprogram and postprogram survey (Supplemental Appendix 1). The preprogram survey primarily included questions regarding past health humanities experience, past DEI or antiracism programming experience, and participant demographics. Only gender identity was collected and 3 categories (“male,” “female,” and “other”) were ultimately used for analysis to avoid potential identification of participants. The postprogram survey included Likert scale and free response formats. Likert questions queried participants’ ability to reflect on their own racial identity, racial identity of others, and influence of their racial identity on their future role as a healthcare worker. Free responses included questions about how the program differed from prior DEI program.
These surveys were intended to collect basic participant demographic and educational information and assess their general experience of the program prior to the formal qualitative interviews. These surveys were not validated. However, survey experts at the Odum Institute for Research in Social Science were consulted and the survey was tested by the study team for language, flow, and accessibility prior to distribution. Surveys were formatted into an electronic platform (version XM; Qualtrics, Provo, Utah; 2020) and emailed 1 week before and after the program with one interval reminder email.
Postprogram qualitative interviews were conducted to evaluate participants’ experience. The Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines were used for the qualitative interview and analysis process (Figure 1 and Supplemental Appendix 2). 48 One-on-one interviews were selected to capture the embodied experience of participating in these workshops and to allow a space for participants to process their growth and provide feedback on the program. All participants who completed the program were eligible to participate in interviews. Interview questions were developed by the research team in consultation with a qualitative expert at the Odum Institute for Research in Social Science. A standardized interview script was established after iterative edits (Supplemental Appendix 3). Interviews were conducted by a medical sociologist at the host institution (ARB). The interviewer was not present for the workshops and was not affiliated with the medical school. An outside interviewer was selected to eliminate the risk of bias associated with the peer-facilitators conducting the interviews. This also allowed participants to share unfiltered feedback on the program. Recruitment for interviews was completed by the interviewer, who reached out via email to all participants who completed the program.

Consolidated Criteria for Reporting Qualitative Research studies (COREQ) flow diagram.
Qualitative interviews were held over a videoconferencing platform (Zoom Video Communications Inc, San Jose, CA). Interviews were one-on-one and scheduled for 60 min. Each interview was recorded and transcribed using Temi (Rev, Ausitn, TX). Transcriptions were manually reviewed and edited by a research team member.
Data analysis
Interviews were formatted into Dedoose 9.0.62 (Sociocultural Research Consultants, LLC, Los Angeles, CA). A deductive analytical approach was determined appropriate to gain insight into participants’ experiences with the current workshop compared to prior DEI experiences and to gather pertinent feedback for curricular improvement. 49 Two researchers (YI and SH) used conventional content analysis, supplemented with open and axial coding and constant comparison to analyze the data. 50 Preliminary codes were determined after each researcher coded 2 interviews selected at random. A codebook was generated and used to code a third randomly selected interview. Intercoder agreement was calculated in the coding software and a kappa statistic 51 of 75% was achieved. Disagreements were resolved through discussion and the codebook was finalized. Interviews were coded independently, and themes were decided between the lead authors (YI and SH). To address reflexivity, lead authors reflected on their personal connections to the work and their own journeys with antiracism throughout data analysis. Illustrative quotes were selected and summarized in table form.
All students were asked to complete the qualitative interview after participating in the program. Thematic saturation was determined to have been achieved by the independent coders after roughly half of interviewers were coded. No additional interviews were deemed necessary at this point. Results from content analysis of interviews were then triangulated with survey Likert-scale and free-text responses to compare findings across objective and subjective research tools.
Descriptive statistics were used to analyze participant characteristics and quantify Likert responses in the postprogram survey. These results were summarized as No. (%) and reported in table form.
Results
Participants
Thirty medical students registered for the program with a 93.3% (n = 28/30) attendance rate (ie, individuals who attended at least 3 of 4 sessions). Response rate for the preprogram survey was 96.7% (n = 29 of 30) and 70.0% (n = 21 of 30) for the postprogram survey. Preprogram data were used for summarizing participant characteristics (Table 2). Participants were 75.9% female with a mean age of matriculation into medical school at 23.4 years (standard deviation 1.7). Participant sex was not collected. Racial demographic breakdown was: 51.7% White, 31.0% Asian or Asian American, 3.4% Black or African American, 10.3% multiple races, and 3.4% other. Most participants (65.5%) had participated in a DEI educational activity before and one participant (3.4%) had participated in an NM workshop.
Participant characteristics.
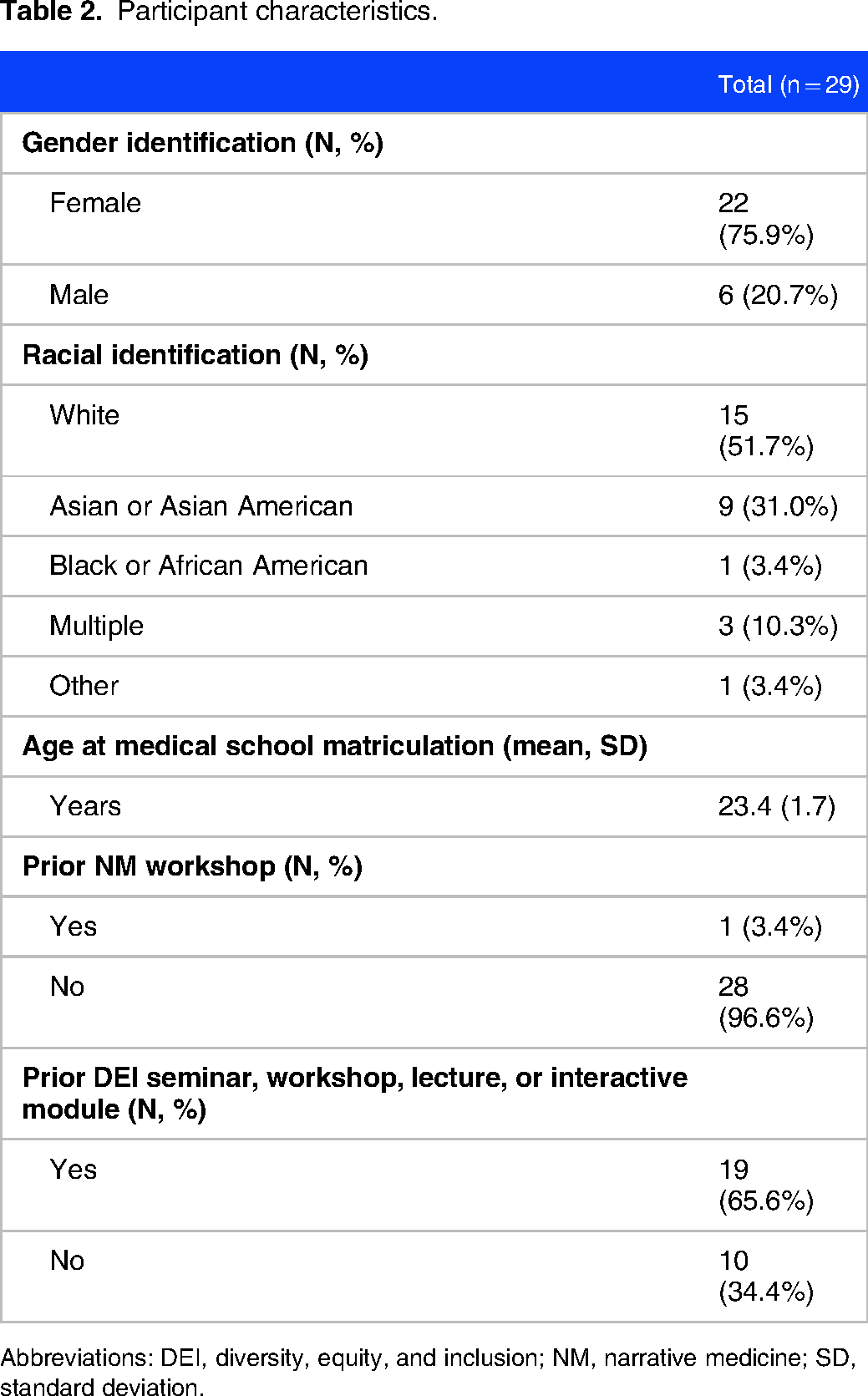
Abbreviations: DEI, diversity, equity, and inclusion; NM, narrative medicine; SD, standard deviation.
Postprogram survey results
The postprogram survey included Likert scale questions about participants’ ability to reflect on their own racial identity, racial identity of others, and influence of their racial identity on their future role as a healthcare worker. Distribution of responses is summarized in Table 3. Of the participants who completed the postprogram survey, all respondents (100%) reported “somewhat true” or “very true” for all questions.
Postprogram survey responses.

For the free text question, “Was this workshop different from other DEI workshops, lectures, and modules you’ve engaged with in the past?” all participants (100%) provided a response. One-third (33.3%) of participants commented on the value of active engagement and self-reflection. Five (23.8%) participants commented on the intimacy of the small group setting. Six (28.6%) wrote about the value of the program's narrative component, and 3 (14.3%) wrote about multimedia use. The following responses illustrate these elements. Yes, I’ve never experienced a DEI workshop that has as many creative and self reflective elements. I think both the creative piece analysis and writing portions of the workshop were really great for humanizing this topic further as well as thinking more deeply about ones own role in anti racism (which is a piece that I feel is often minimized in a lot of DEI trainings). (Participant 34) (1) More questioning, openness, soul-searching, etc—very engaged in complexity, which I appreciated. The facilitators did an awesome job letting us all think expansively about how we relate to one another, and I didn't feel like I walked away with a cookie cutter way in which I was supposed to engage in anti-racism work, which is both challenging and emboldening. (2) more imagination and finding inspiration in art, which I think helps humans grapple with really difficult social challenges in a way that “here's a to-do list” does not. (Participant 47) Yes, this workshop was different than others. I really appreciated the small group format, as I feel it allowed for deeper engagement. I also enjoyed engaging with pieces of art or creative work, then writing about a unique prompt. The prompts included ideas that I had not before truly sat and written down or put my thoughts about into words, so it was really beneficial. (Participant 17)
Qualitative results
Sixteen (53.3%) individuals participated in a postprogram interview. Interviews ranged from 18 to 59 min with most lasting approximately 30 min. Interviews had 11 to 33 codes with a mean of 21 codes per interview. Three major themes emerged: (Theme 1) curricular engagement; (Theme 2) racism and antiracism in medicine; and (Theme 3) group experience.
Curricular engagement
Participants described their experiences participating in the NM antiracism curriculum. Participants discussed the value of assigned readings, including the theory-based texts that were required before sessions (Meaningful Theoretical Content). One participant said: “I thought it gave a good foundation for some of the scholarly work in this field. And then I think a lot of what we read was written 15 to 20 years ago, so that also was a light bulb moment—that this is something people have been talking about for a while and some of the stuff I read I'm like, duh, right … but also it's been 20 years and what has changed? I think it underscored, again, how common this experience for a lot of people is and how quickly it can become invisible if it's not something you personally experienced on a day-to-day basis or your family experiences on a day-to-day basis.” (Participant 41) “It was not challenging to talk about how militarized we are in terms of ‘fighting disease’ and ‘the frontlines.’ We could come up with examples all day, but then I thought it was challenging to say, okay, well then now what? And yeah, I think I felt a little more challenged.” (Participant 18) “We all come from different backgrounds and experiences, so whether we were interacting with an art piece from the Ackland Museum or reading a poem or talking about the readings that we had read previously for that session, everyone interprets it in different ways. So, what I might've thought on first glance, some of my classmates might have had different first impressions.” (Participant 16)
Through listening to others’ perspectives on the creative works, participants began to consider the lived realities of minoritized groups more deeply. One said: “I think that hearing people's different emotional and artistic response to that piece … made me appreciate not only stereotypes, but also historical context for how we portray different groups of people and the characteristics that we expect of them. And yeah, there's a lot of complexity in how we celebrate different, not only cultural, but historical parts of various groups’ histories.” (Participant 18)
Additionally, participants reported the readings and activities included in the curriculum helped them gain a more nuanced understanding of race (Race, Identity, and Intersectionality). Several non-White participants spoke about the opportunity to explore racial dynamics among minority groups: “As a minority it's easy to kind of group myself in as like, ‘oh, I’m a minority.’ I’m oppressed in every way the other groups are and be on the side of the oppressed, but [the curriculum] made me realize that as minorities we end up oppressing other minorities as well. It was a change of perspective in the sense like, ‘hey, yes, I might be a minority, but … I can be the oppressor,’ or I am actively tolerating oppression of other groups so my work is nowhere close to done.” (Participant11) “I think the nicest part about this workshop was how much I felt personally engaged. I’m just not a big proponent of lectures so I appreciated a context where I was asked a lot more questions, where I was asked to do something and then share it, versus I sit here and listen to someone talk for an hour about diversity and inclusion. And I think that surpassed a lot of the previous experiences I’ve had.” (Participant 26)
Others noted that the curriculum was targeted at helping participants understand their personal journeys with racism, while typical DEI programming is not. One stated: “This workshop has made me challenge [myself] … Why do I have this reaction? Why do I feel that way? Why do I imagine a black man when all the narrative does is just describe a noose around his neck. Right? I don't think those DEI programs that I have attended have gotten to that level of, well, why do you feel that way? How does that manifest in your life?” (Participant 44)
Racism and antiracism in medicine
While 66% of students reported prior DEI course participation, many commented on a new or refined “reconstructive” (not just recognizing unjust systems but building more just systems in their place) approach to antiracism (Reconstructive Visions). One participant gave the following definition of antiracism: “I think being anti-racist means acknowledging my privilege as a white person who was raised in a pretty privileged community. And then, now educating myself and working to change my internalized racism and then working to change the culture in the systems that I’m a part of. And I think lastly interrupting racism when I see it.” (Participant 16) “I think the idea of using imagination to tap into those things like, what do you want the work to look like? And why? What is our vision going forward? And what a more just and fair society looks like? I think the idea that that was worthwhile, dwelling in those ideas and dwelling in those thoughts, was really, really helpful.” (Participant 47)
Finally, some participants discussed their aspirations for the future of medical education that were shaped or reinforced by the program. One said: “Hopefully one day [I’ll] be teaching a generation of medical students or younger people who maybe are still working towards the same goal, but don't face the same barriers that people do today in some way. I would like to make progress, be part of progress.” (Participant 41) “I think, for me, trying to understand what I can do specifically as a doctor versus specifically as a human being are two important things because they are different. Like ultimately, I am still a human when I am a doctor, but as a doctor, I do have a lot more impact and that is a good and a bad thing sometimes.” (Participant 26) “[The facilitator] asked us to show up bravely, like this is not a safe space, this is a brave space. And that, just that one line made me feel like I could engage a lot or like I could engage a lot more with like, oh yeah, I'm having a really racist thought right now. I'm like, wow, that's interesting. I didn't notice that before. Or wow, I don't know anything about this, let's explore that.” (Participant 25) “Every time someone shared something of theirs, I feel like I was very challenged to think about where they were coming from. I think as a society, we're very used to being able to absorb media or stories so quickly. I'll scroll through articles, scroll through thousands of comments in a day, right? So, when I do get to engage with this person and their story, I'm critically being like, ‘oh, where are they coming from?’ ‘What do they mean when they wrote this sentence?’ Especially with this being such a spontaneous activity it makes it feel a lot more real or, I guess, internal. I don't know if ‘challenge’ is the right word, but it feels difficult sometimes to not necessarily respond to it but engage with it in some fashion.” (Participant 26)
Group experience
The group experience in this program proved to be critical to its success. Many participants spoke about their ability to build a community of peers who they could rely upon to do the challenging work of antiracism with (Community and Support System). One participant said: “This is my favorite way to learn, being in small groups of people, where we share thoughts and feelings where there's space to, not even push back, but be very vulnerable and open and transparent and to talk about the ways that intellectual things and emotional things intersect.” (Participant 47) “People actually shared genuine thoughts and takeaways. And it wasn't like people were just trying to act like, ‘oh, this is how I'm the biggest ally’ and whatnot. I thought it was really great, everyone shared things we took away from it and what we could do better and ways we can advocate for anti-racism.” (Participant 35)
Further, peer facilitation was well received by most, as it created a safe space while still feeling educational (Authentic Space Among Peer Learners). One participant said: “The peer part was super important because it didn't feel like this authority figure, like a professor or some expert in the field, was looking [or] watching this whole thing. I think having a peer facilitator who knew about this issue, but not to the point that I had to be scared of what I say was extremely helpful in generating conversation and generating thoughts and speaking my mind and seeing what other people think.” (Participant 11) “I think the fact, too, that we were all not necessarily similar ages but in a similar position helped. I think sometimes having more of a teacher or a professor as a facilitator does create this power dynamic where people aren't as open to saying anything. I think it was very unfiltered, which was helpful.” (Participant 41)
Discussion
This antiracism NM program, developed and facilitated by medical students for medical students, provided a unique opportunity for participants to grapple with concepts of antiracism. The successful implementation and engagement of this program is consistent with successes of prior student-driven initiatives, particularly around social justice in medicine.44,45 These findings are important, especially as antiracism becomes an integral part of medical education and more rigorous, thoughtful programming is desired by students.52–55
The potential implications of this program are far-reaching. Program evaluation revealed the value and need for antiracism education that is engaging, interactive, and appropriately challenging. NM methods have been previously applied to increase empathy, cultural competence, professionalism, and reduce burnout in healthcare.27,30,31,56,57 The findings of this study suggest a new and important direction that NM can move toward in addressing racism and unmet DEI programming needs in medical education. Qualitative analysis revealed that many participants found the narrative element of the program to promote self-reflection of their own racial identity and of larger social structures. While writing has been utilized in medical schools to foster self-reflection and wellbeing,58–60 the unique structure of the NM workshop (eg, close reading of a text/artwork, discussion, prompt-driven writing, sharing of writing) may lend itself to grappling with topics of racism/antiracism which can be inherently personal and structural. The use of multimedia was also raised as an innovative element that encouraged participant reflection of complex issues that may not have otherwise been accessible. NM opens channels for bringing multimedia into medical education, and antiracism programming is an area that may uniquely benefit from this. 61
Evaluation of this program revealed the importance of embracing antiracism as both a deconstructive (ie, breaking down racist structures) and reconstructive process (ie, rebuilding more just systems in place). Over recent years, programming efforts have encouraged students to take an active role in addressing workplace bias.62–64 These programs have often focused on specific clinical scenarios without providing historical context in which bias, microaggressions, and mistreatment take place. 23 One strength of this curriculum was its breadth in providing sociopolitical and historical context, while providing space for practical and visionary discussions to navigate racial injustices along professional and patient relationships. Future programs may benefit from developing curricula that encourage deconstructive and reconstructive approaches to address the complexities of racism in medicine more holistically.
Peer facilitation was an essential and novel element of this program. Participant interviews revealed a common theme of comfort, rigor, and authenticity that was fostered by having medical student facilitators. Specifically, the lack of an authority figure and pressure to perform or receive a good grade allowed for a different type of vulnerability than what students had experienced in traditional DEI programming. The literature on peer education and near-peer facilitation is most robust in professional development, mentorship, and clerkship preparation; yet, even in these studies, peers are often a year or more ahead in the curriculum or involve residents and junior faculty.65–68 Identity-based peer support has also been shown to be effective, but the role that peers can play in antiracism and DEI engagement is largely underexplored.69,70 What is perhaps most unique about this program is the true peer-to-peer facilitation (ie, same academic year students) without the presence of any senior medical students, trainees, or faculty. We anticipate that peer facilitation may be similarly useful for residents, fellows, or junior faculty and should be considered as institutions try to incorporate more antiracism in their professional development and promotion guidelines. However, as faculty become more senior, further deconstructing the traditional hierarchy may also be beneficial. Prior to the administration of this current study, the authors developed an NM antiracism faculty program which involved medical students facilitating workshops for faculty at the same institution. 35 The results from the faculty program suggested that reversing the power dynamics was effective for discussing antiracism at the more senior faculty level. Thus, considering not only the content of antiracism and DEI programming, but how the content is delivered is crucial for ongoing growth and engagement from different types and levels of learners.
This program also revealed challenges in developing and evaluating an antiracism program facilitated by and created for medical students. Consistent with prior literature, institutional support was essential for operationalizing the program. 44 While sustainability was outside the scope of this study, ongoing faculty and institutional support and availability of student-facilitators with adequate NM training are potential barriers. Like other NM programs, time constraint was an anticipated challenge.33,56 The summer months were chosen for the program to mitigate course conflicts, but several topics were omitted from the curriculum to avoid increasing session duration and total number. Time pressure also contributed to the decision to focus on anti-Black racism; however, racism does not exist in binaries or in siloes, and future iterations of this program would benefit from more inclusive discussions of antiracism.71,72 In the qualitative interviews, many students reported on their desire to continue the program's antiracism work in the academic year, but several raised concerns about competing priorities and engaging other students who would not be readily interested. The successes of this program may be partially attributable to engagement from a self-selected group of individuals and navigating how to promote this work in medical school is an ongoing challenge.
Assessing internal bias over time was another challenge to this program's development. The race Implicit Association Test (IAT) 73 was initially distributed to participants with the goal of serially evaluating changes in student bias; however, IAT data was ultimately not included in the analysis due to low participation and poor data quality. To date, there are limited tools for evaluating bias and changes in perspectives after an exposure (eg, workshop). The validated race IAT included a version with photographs of Black/White faces for assessing anti-Black bias and cartoons of Asian faces for assessing anti-Asian bias. While the possibility of combining IATs to capture implicit bias more broadly was discussed by the research team, this was ultimately determined to be infeasible with the existing IAT structure at the time of the study period. Further studies are needed to evaluate this program with instruments that can meaningfully characterize bias. Additionally, validated instruments that may better evaluate racial bias are important considerations for future research.
Limitations
This program was conducted at an institution with a history of health humanities and social justice education. It is unclear how reproduceable the program is in its current state. Nonetheless, the development and evaluation of this program revealed key themes around the effectiveness of NM methods in antiracism programming, peer facilitation as a useful structure for discussing race and racism with medical students, and the depth of reflection that a virtual antiracism series could yield among its participants. Elements of this program may be reproducible in other settings and similarly be evaluated to validate this study's findings.
The program was relatively small (approximate 16% of the medical school class participated) and predominantly female and White. We were unable to assess why students did not participate and the generalizability our findings are thus difficult to ascertain. The program survey and qualitative interviews were subject to response and recall bias. To mitigate against these, students could pause the survey and schedule the interview at their convenience. Future directions include increasing the scope of antiracism, increasing participant numbers, and expanding to additional institutions and health professional programs.
Conclusion
This virtual, peer-facilitated antiracism NM program provided an active, engaging, and challenging experience for participating students. Postprogram interviews revealed the program deepened students’ understanding of racism and intersectionality, promoted self-reflection and community building, and propagated reconstructive visions for continuing antiracism work. Future directions include expanding the program curricula and including more medical schools to assess reproducibility.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241261238 - Supplemental material for By Medical Students, for Medical Students: A Narrative Medicine Antiracism Program
Supplemental material, sj-docx-1-mde-10.1177_23821205241261238 for By Medical Students, for Medical Students: A Narrative Medicine Antiracism Program by Yoshiko Iwai, Sarah Holdren, Alyssa R. Browne, Nicholas R. Lenze, Felix Gabriel Lopez, Antonia M. Randolph and Amy B. Weil in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241261238 - Supplemental material for By Medical Students, for Medical Students: A Narrative Medicine Antiracism Program
Supplemental material, sj-docx-2-mde-10.1177_23821205241261238 for By Medical Students, for Medical Students: A Narrative Medicine Antiracism Program by Yoshiko Iwai, Sarah Holdren, Alyssa R. Browne, Nicholas R. Lenze, Felix Gabriel Lopez, Antonia M. Randolph and Amy B. Weil in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors wish to thank Columbia University's Narrative Medicine Program and the Office of Diversity, Equity, and Inclusion at the University of North Carolina at Chapel Hill School of Medicine for co-sponsoring this program, and the Gold Humanism Honor Society for their support. The authors also thank Elizabeth H. Manekin from the Ackland Art Museum for her collaboration, Dr Sayantani DasGupta and Professor Zahra H. Khan for their guidance, and the scholars and artists whose texts were instrumental to our curriculum.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Columbia University Narrative Medicine Post-Graduate Fellowship.
Author Contributions
YI, SH, AMR, and ABW were involved in concept and design; YI and SH in drafting of the manuscript and obtained funding; NRL in statistical analysis; ARB, AMR, and ABW in administrative, technical, or material support; and ABW in supervision. All authors contributed to acquisition, analysis, or interpretation of data, and critical revision of the manuscript for important intellectual content.
Ethics and Consent
The University of North Carolina Institutional Review Board (#20-3548) reviewed and deemed this study exempt. While informed consent was waived, all participants were notified of the risks, benefits, and goals of the study through a standardized research information form before participating in the program.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.