
Abstract
Objective
The social contract mandates that in return for the government-funded labor of residents and fellows, the medical profession trains, to the best of its ability, the physicians of our future. This contract obligates graduate medical education (GME) to utilize all available information to create an optimal learning environment for its trainees. Business research has determined that a clearly defined mission statement is associated with improved employee engagement, retention, and wellness. Given that GME trainees are situated at the intersection of at least two institutions, each with its own separate mission, trainees could potentially be hindered by incongruent missions in the learning environment. The literature on mission statements has analyzed medical schools and hospitals separately; however, investigations comparing the statements of these affiliated institutions have not been conducted. Therefore, we plan to compare the content and assess the consistency of mission statements from affiliated medical schools and hospitals to determine if incongruencies exist.
Methods
In 2023, the mission statements from the Association of American Medical Colleges (AAMC) medical schools and affiliated teaching hospitals (n = 163) were aggregated from their public websites. The content of each mission statement was thematically analyzed to assess variation.
Results
According to content analysis of the mission statements from 163 AAMC medical school members and affiliated teaching hospitals, less than half of their top priorities are shared by their affiliated hospitals (45%). Additionally, themes of diversity, religion, and global care were found to be contrasting priorities between affiliated institutions.
Conclusion
Given the precedence within the business and the observed discrepancies in mission, further research is needed to determine whether collaborating medical schools and hospitals could provide a more favorable graduate training environment by uniting their priorities and identifying shared goals.
Keywords
Introduction
The pathway through graduate medical education (GME) is strife with challenges that force trainees to perfect their knowledge and skills within the medical field. Providing favorable learning environments to students should be a main priority within GME. The social contract of GME is made explicit by heavy governmental subsidies to hospitals for fellow and resident training with strict criteria from the Accreditation Council for Graduate Medical Education for measuring physician competency. 1 As students transition through stages of their medical careers, they are guided by numerous individuals from various institutions, namely medical schools and hospitals. To be successful through this transition, trainees must navigate effectively between the school and affiliated teaching hospital, suggesting the need for a learning environment unified in its priorities. Therefore, an initial investigation is necessary to identify any discrepancies and where they may occur.
Clinical and academic medicine hold multiple internal tensions with respect to their priorities. 2 Excellent patient outcomes, superb teaching, innovative research, and stewardship of precious resources are all common organizational priorities that coexist well in the abstract, but conflict easily in practice. 3 When members of an organization are bound by multiple duties, a cohesive mission statement serves as the backbone of the institution's value system and it provides strategic alignment. 4 It has been observed within business practices that a clear cohesion of organizational purpose within their mission statement boosts employee engagement, augments wellness, and increases retention.5,6
Medical schools and hospitals alike implement mission statements as a method of producing this organizational unity. 7 The thematic analyses of medical school mission statements identify a unified emphasis on health, research, and education, highlighting the homogeneity of their priorities. 8 In contrast, hospital mission statements were found to have substantial differences in their content and are based on the guiding principles of the hospital. 9 This lack of unity could be elicited from nuances in the way each hospital balances its obligation to patient care, community needs, and economic management. The mission statements of hospitals and medical schools have been analyzed individually10,11; however, the correlation between the mission statements of medical schools and their affiliated hospitals has received little attention, raising the question to what degree these institutions share priorities and goals.
Graduate medical education is often situated at the intersection of at least two institutions (eg, a medical school and a hospital), each with its own priorities and mission. An example of this overlap is when medical students perform their clinical rotations within their school's affiliated teaching hospital. The students are exposed to a learning environment imbued with the qualities of both institutions’ mission statements. An environment with contrasting priorities has the potential to impede graduate training, given how a clear mission statement is shown to increase retention, wellness, and engagement.
Therefore, we set out to assess the concordance of the mission statements of the top medical schools in North America and those of their corresponding teaching hospitals. We hypothesized there would be a noticeable variance between the priorities of affiliated institutions.
Methods
Using the publicly available list of medical schools membered with the Association of American Medical Colleges (AAMC) in 2023, we identified the top 163 medical schools and their respective teaching hospitals within North America. 12 In the same year, we obtained the respective mission statements from each school and institution's home website. We used an inductive-qualitative analysis to extract themes and compare mission statements between corresponding institutions to establish the degree of congruency. After reviewing all mission statements, four research assistants developed an initial codebook with mission statement themes; to maximize consistency with coding, the definition of each theme was discussed and agreed upon. The mission statements were then divided among the four research assistants and coded for each theme.
The themes of each mission statement were listed and compared with the respective affiliated institution (eg. Washington University School of Medicine's mission statement was analyzed with Barnes-Jewish Hospital's mission statement). The number of shared themes was divided by the total number of unique themes between both institutions to obtain the fraction of congruent themes. A percent breakdown was obtained by counting the themes within each category of institution—medical school and teaching hospital—as well as the themes shared between each affiliated school-hospital pair.
Given that all the data was collected from publicly available websites published by the respective institutions, the study is exempt from IRB assessment. Ethics and consent statements are also not applicable.
Results
Following a review of the mission statements, the following 9 themes were identified: Global Care, Community Care, Diversity, Education, Ethics, Patient Care, Professionalism, Religion, and Research. All 163 affiliated medical schools and hospitals contained mission statements that were incorporated into the thematic analysis.
The majority of themes were expressed nearly verbatim within the mission statements, making identification simple. However, a few of the themes were commonly expressed in a more indirect manner. For example, the theme of Ethics was identified if the mission statement contained elements that prioritized the beneficence and equal treatment of people. Since only a few themes were expressed indirectly, they were determined following deliberation among the coders.
Using the identified themes, we found a 45% (M = 0.449 ± 0.019, SD = 0.25) congruency between the missions of medical schools and those of their respective hospitals (Figure 1). This finding means that less than half of the themes reported in the medical school's mission statements were also present in the mission statement of the affiliated hospital, suggesting a lack of shared principles.
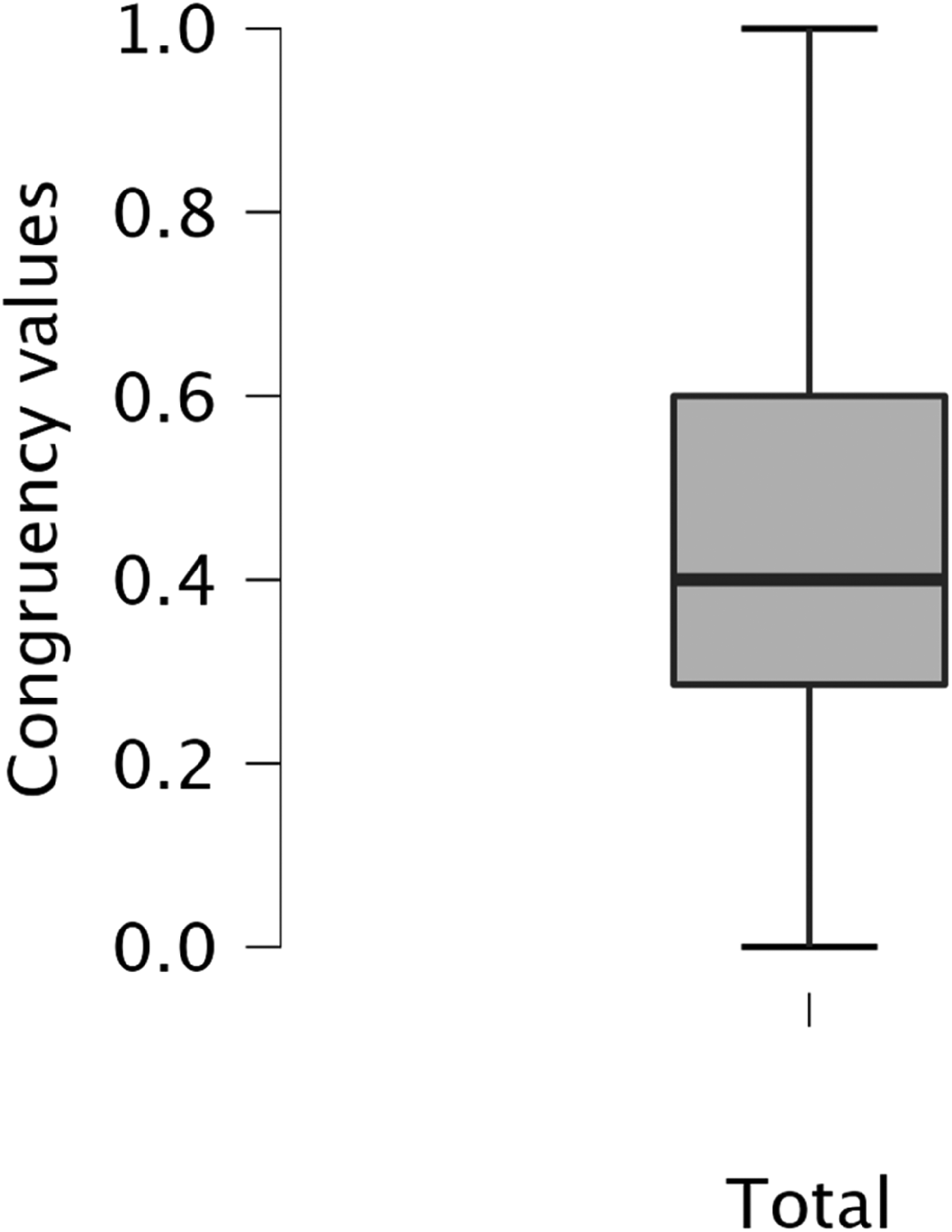
Contains a boxplot which conveys the distribution of congruency values between the mission statements of affiliated school–hospital pairs. M = 0.449 ± 0.019, SD = 0.25, 25th Percentile = 0.286, 75th Percentile = 0.600.
After counting the themes within the mission statements, we compared the various themes that were favored and disfavored among the various types of medical institutions to determine the frequency of each theme within each institution category (Table 1, Figure 2). Medical schools were found to discuss considerably more themes within their mission statements (n = 804) than teaching hospitals (n = 535) and contained twice as many themes than were shared between affiliated institutions (n = 409).

Bar graph compares the number of occurrences of each theme between the AAMC Medical School Members and the affiliated teaching hospitals.
Table presents the percent theme breakdown for each institution category of AAMC medical school members and their affiliated teaching hospitals which compares theme prevalence within institution categories. The “Affiliated school–hospital pairs” category denotes the frequency of themes shared between a medical school and its respective affiliated teaching hospital. The “Total” column presents the number of themes identified within each institution category.

There are several interesting relationships that can be observed from the theme breakdown between medical schools and hospitals. Generally, it was very common for mission statements to include the themes of Patient Care, Research, and Education. This trio prevailed as the basic format to the majority of mission statements with most institutions presenting them either in a list or as guiding principles. Therefore, those three themes held around the largest percentage in both medical school and hospital mission statements; however, Community Care was more frequent than research within teaching hospitals (17.4% vs 14.6%). Community Care overall was a theme that also occurred consistently within the mission statements of both institutions.
Given its common prevalence in both medical schools and hospitals, the theme trio—Patient Care, Education, and Research—were appreciably the most common themes shared between affiliated school-hospital pairs (33.5%, 20.0%, and 17.8% respectively). Despite the high congruence of the theme of Patient Care within the medical school and teaching hospital mission statements, there was an appreciable disparity in its respective frequency between each institution (17.5% vs 28.8%). Community Care was also found to be a commonly shared theme in the mission statements (16.9%). The rest of the themes were greatly under shared between the affiliated institutions.
The theme of religion held a relatively large percentage (2.6%) in hospital mission statements compared to the notably lower occurrence (0.4%) in medical schools. Conversely, diversity and global care were moderately common within medical schools (8.8% and 6.5%) but did not have a large prevalence within hospital mission statements (2.6% and 3.7%, respectively). To better appreciate the differences in theme prevalence of religion, diversity, and global care between medical schools and teaching hospitals, pie charts were created to isolate the variation in theme prevalence between institutions (Figure 3). From these data, the disparities can more clearly be observed as each theme has one institution which represents the majority of theme usage.
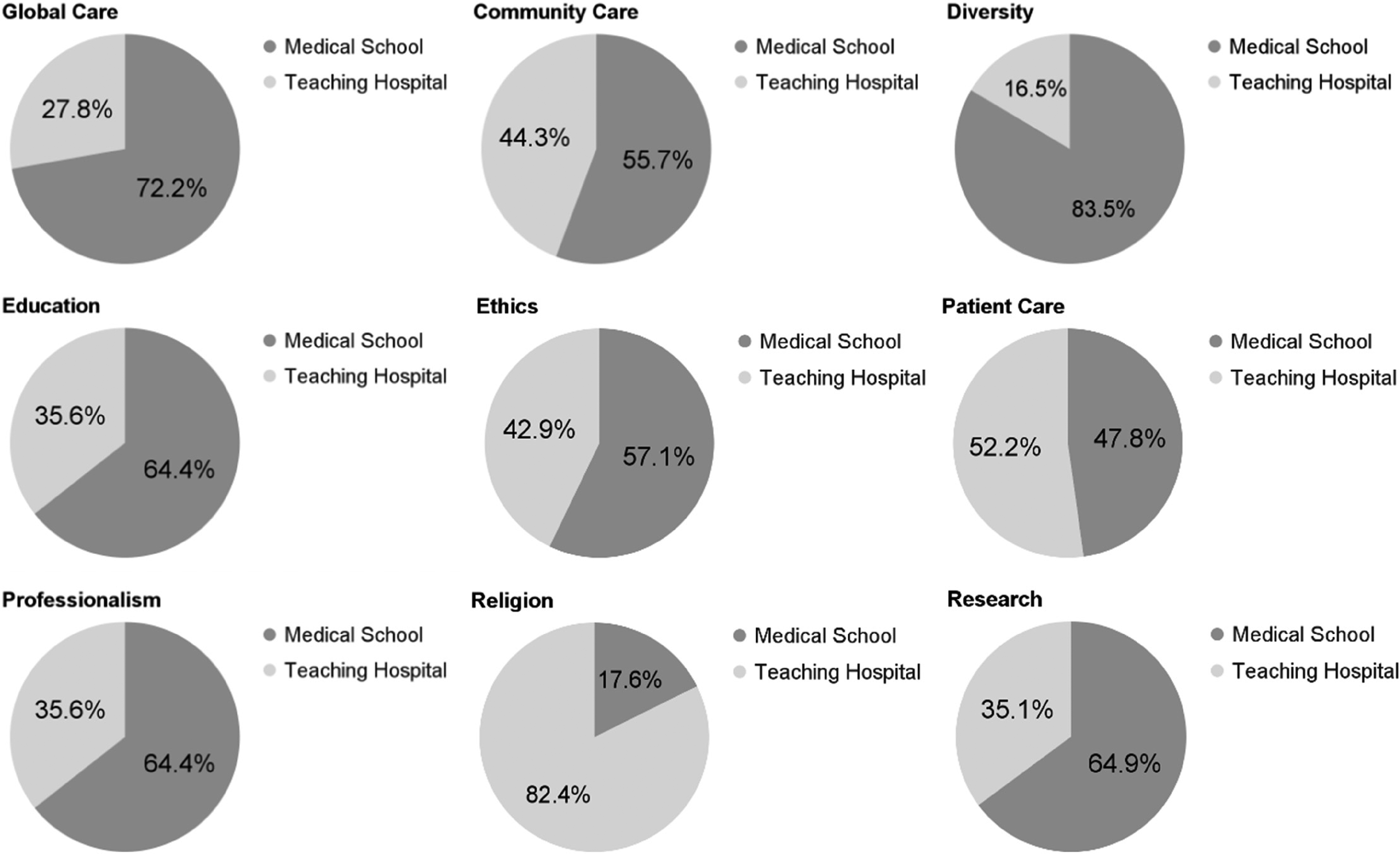
Set of pie charts that describe the percent frequency of occurrence for each theme within the AAMC Medical School Members and the affiliated teaching hospitals, comparing theme prevalence between institutions.
Discussion
When examining the mission statements of the top 163 North American AAMC medical school members and those of their affiliated teaching hospitals, our results indicate only a 45% overlap between them. This means that, on average, more than half of the priorities and ideals promoted by the medical schools are not similarly endorsed by their affiliated hospitals. The low level of congruency within the mission statements raises possible concerns about the characteristics of GME learning environments. Trainees who are located within the border of the medical school and hospital could be met with conflicting ideas and principles regarding their work and training. It is unlikely that these discrepancies will cause direct conflicts in teaching, given that mission statements are broad pursuits rather than strict protocols, but the incongruence could cause deviations in the working culture, leading to subtle differences in the minutia of organizational frameworks as observed in the business field.
However, this lack of congruency is not spread equally among the themes, the themes that are shared between affiliated school-hospital pairs are centralized to Patient Care, Research, and Education. These findings suggest that the affiliated medical schools and hospitals predominantly share the basic tenets of GME but differ crucially in the nuances that make them unique based on location and community. These results are not surprising given the relationship between medical schools and teaching hospitals. Both institutions are directly involved in GME but provide different services to society. Therefore, the combination of similarities and differences identified are logical; however, differences among nuances in regional circumstances can potentially prevent a cohesive purpose from being achieved, raising concern for the quality of GME.
Furthermore, our findings suggest that the theme of Diversity is relatively underrepresented in teaching hospitals compared to medical schools and is rarely observed at the same time within affiliated school–hospital pairs. This relationship introduces a discrepancy within the levels of GME which is corroborated in other studies. A 2020 survey by the AAMC identified that 99% of respondents were implementing strategies to recruit students from diverse backgrounds, highlighting a clear commitment to diversity. 13 Whereas, a lack of commitment to diversity was identified within general surgery residency websites, suggesting a decreased adherence to these principles in the higher levels of medical education. 14 This finding potentially suggests that as trainees transition through GME, they could be met with less inclusive and diverse learning environments which has been shown to decrease creativity and potentially produce lower work performance.15,16
In the reverse direction, Patient Care is a theme that is relatively underrepresented in medical school's mission statements compared to teaching hospitals. This finding makes sense given the purpose each institution has within society and the communities they are located in. Hospitals are directly involved with patient care whereas medical schools maintain a degree of separation from patients as trainees develop their medical knowledge and skill. This theme suggests a possible incongruence between medical schools and teaching hospital mission statements that cannot be removed because of the fundamental nature of each institution. An inherent challenge to trainees as they progress through GME is the transition from student to patient-facing roles. 17 Ultimately, these data most likely capture a sign of this transitional period through the incongruent theme of Patient Care.
To continue, the theme of Religion was also found to be predominantly present in teaching hospitals and maintains a low level of congruency in affiliated school–hospital pairs. Religion was a rare theme within all the mission statements; however, when it was identified within an institution it was the predominant theme promoted by the mission statement. This observation presents some concern regarding the potential for conflicting mission statements leading to poor GME because of the degree of significance it holds in certain teaching hospitals. If the affiliated medical school does not hold similar religious values, then students could be met with conflicting messages throughout their training, raising concerns about education quality.
Literature from the fields of leadership and business confirms that a unifying mission statement that is supported by institutional practice has many advantages, including employee wellness, retention, engagement, and overall cost reduction. Evidence suggests that mixed messaging to residents is counterproductive. 18 The Social Contract that obligates us to train our future physicians to the best of our ability also mandates that we set our trainees up for success. Success, however, could potentially be made difficult with the inclusion of conflicting guiding principles impressed upon trainees. To alleviate this obstacle, medical schools and their associated hospitals should identify and align their combined priorities to take a step in the right direction to improve graduate training.
The limitations of this study are concentrated in the method of data collection and the vague nature of mission statements. Persistent communication and agreement among the coders were utilized during the inductive-qualitative analysis to achieve the highest level of consistency and objectivity possible, but variation in interpretation undoubtedly led to some unwanted variation in the data. Ultimately, this brings into question the precision and reproducibility of the results, presenting the need for further iterations to be conducted. Other studies have performed network text analysis to bypass this issue and identify more complex relationships in the data which could lead to more nuanced thematic relationships in future studies. 19 Another limitation is within the nature of mission statements and their influence on work environments. It is unknown the extent to which mission statements accurately reflect the goals furthered by the administration of medical schools and teaching hospitals. Thus, there could be a large variation in the accuracy of congruency values between affiliated school–hospital pairs.
The next steps for this research should dive further into the relationship of how confusion and inconsistency in mission statements affect learning and work outcomes. It is evident that differences in mission exist, but it is still unknown how this affects the realm of GME. Additionally, other dimensions of institutional cohesion such as statements of value and strategic action plans should be analyzed to assess whether incongruencies are similarly observed.
Conclusion
According to the mission statements of the top 163 medical schools in North America, the majority of their main priorities are not shared by their affiliated teaching hospitals, specifically regarding Diversity, Religion, and Global Care. These data, in combination with research in the business field that identifies the negative effects of incongruent mission statements, raise concern about how mission statements could affect GME. Therefore, further research must be performed to elucidate the significance of mission statement incongruency on the quality of training environments and whether collaborating medical schools and hospitals could provide a more favorable graduate training environment by uniting their priorities and identifying shared goals.
Footnotes
Acknowledgments
Maura Kepper, PhD, Research Assistant Professor at Brown School Administration.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.