
Abstract
Leadership training is a necessary component of undergraduate medical education. Our group successfully implemented a student-led organization starting from 2016 (Student Leadership Development Initiative; SLDI) that aimed to provide medical students with exposure to physician-leader career paths in an informal, organic, interactive setting. The COVID-19 pandemic necessitated a shift to online programming, and given the high prevalence of ZOOMTM fatigue, we incorporated monthly, freely available, self-directed modules as an additional leadership training opportunity. The goals of this study are to assess the (1) feasibility of and participation in a virtual student organization focused on leadership training, (2) whether students’ perceptions of the importance of leadership were associated with participation in SLDI, and (3) lessons learned from transitioning to virtual modalities. An anonymous, retrospective cross-sectional survey with 13-items was distributed through an email listserv and a 6-question survey was sent to attendees following each virtual group-discussion. A Fisher's exact test was conducted to assess whether the number of modules completed was associated with students’ perception of leadership importance. Survey results showed that 85% strongly agreed or agreed that SLDI helped them develop professional goals and career paths, and 74% reported benefits in becoming more compassionate physician leaders and valuing wellness. All respondents completed ≥1 self-directed module, and the students’ perception of leadership importance did not influence the number of self-directed modules completed (p > .05). Most participants (63%) attended ≥67% of virtual events, and postevent feedback was positive; however, only 46% of respondents reported meeting someone new at events and 32% reported that they intended on connecting with new contacts. Our results suggest that virtual leadership student-organization, involving small-group discussions and self-directed modules, is feasible and beneficial for medical students. However, the inability to promote meaningful networking opportunities is a major limitation of a virtual training model.
Keywords
Introduction
Leadership training is a necessary component of undergraduate medical education (UME), with numerous studies highlighting improved clinical outcomes and team-dynamics following dedicated leadership training.1,2 But, lack of dedicated curricular time, implementation costs, and disinterest in methods of teaching/activity have limited large-scale implementation of leadership curricula in UME.3,4
Student Leadership Development Initiative (SLDI) is a student-led organization at the Medical College of Wisconsin (MCW) founded in 2016. Previously, up to 20 students met with physician leaders monthly for dinner discussions about physician-leaders’ career paths, experiences, and opportunities. This curricular design is based on the principles of “Situational Leadership Theory,” and as such highlights to students the wide breadth of leadership styles that physician leaders use based on their unique careers. 5 Importantly, in line with the “Social Learning Theory,” 6 these speaker interactions provide students with role models they can observe and imitate. The informal setting further promoted organic conversations and personalized learning, 7 and 93% of year-end survey respondents reporting they learned specific ways to improve their leadership skills. 8
When in-person meetings were suspended due to the COVID-19 pandemic, SLDI pivoted toward virtual platforms. Given high prevalence of ZOOMTM fatigue, 9 we incorporated monthly, freely available, self-directed modules as additional leadership training opportunities for SLDI members. Self-directed learning provides additional benefits in allowing students to develop life-long, independent learning skills (Self-Directed Learning Theory 10 ) that are critical within healthcare10,11; it also allows students to work asynchronously and participate in leadership training regardless of scheduling conflicts. In this study, we assessed (1) feasibility of and participation in a virtual student organization focused on leadership training, (2) whether students’ perceptions of the importance of leadership were associated with participation in SLDI, and (3) lessons learned from transitioning to virtual modalities.
Methods
The virtual SLDI curriculum was implemented between September 2020 and February 2021. Three ZOOMTM events with physician leaders were held; the speakers were given the option to use presentation slides, and students asked questions throughout the event. In addition, 6 modules were shared with members (Table 1). Module topics were selected based on prior leadership curricula for medical students (systematically reviewed in Sadowski et al’s study
12
), and the sources were selected based on reliability and ease-of-access. An anonymous, retrospective cross-sectional survey with 13-items was distributed using REDcap software in March 2021 via the SLDI email listserv (Supplemental Document 1). Inclusion criteria for this survey included (1) currently being enrolled at MCW as a medical student or resident and (2) being listed on the SLDI listserv. Additionally, a 6-question anonymous Qualtrics survey was sent to attendees following each virtual event
Summary of SLDI sessions and modules.
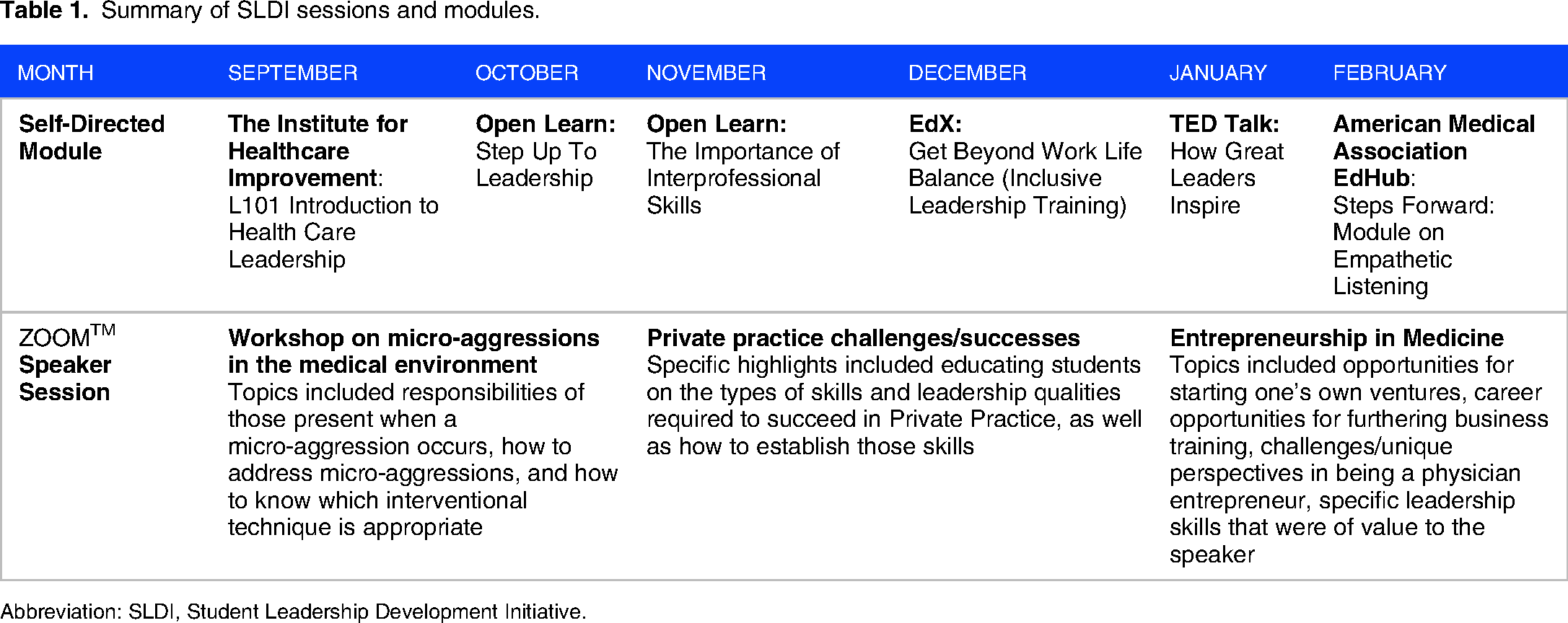
Abbreviation: SLDI, Student Leadership Development Initiative.
Results
The survey was distributed to 192 students on the SLDI listserv with 27 (14%) students responding. Of the respondents, 85% held a leadership role when surveyed, and 52% were past SLDI participants (Table 2). And 63% of respondents were M1s, and no responses were received from residents. All respondents completed ≥1 self-directed module and 19% completed >4 modules. The majority (63%) of respondents attended 2-3 virtual events with physician leaders.
Demographics of respondents and their participation in SLDI.
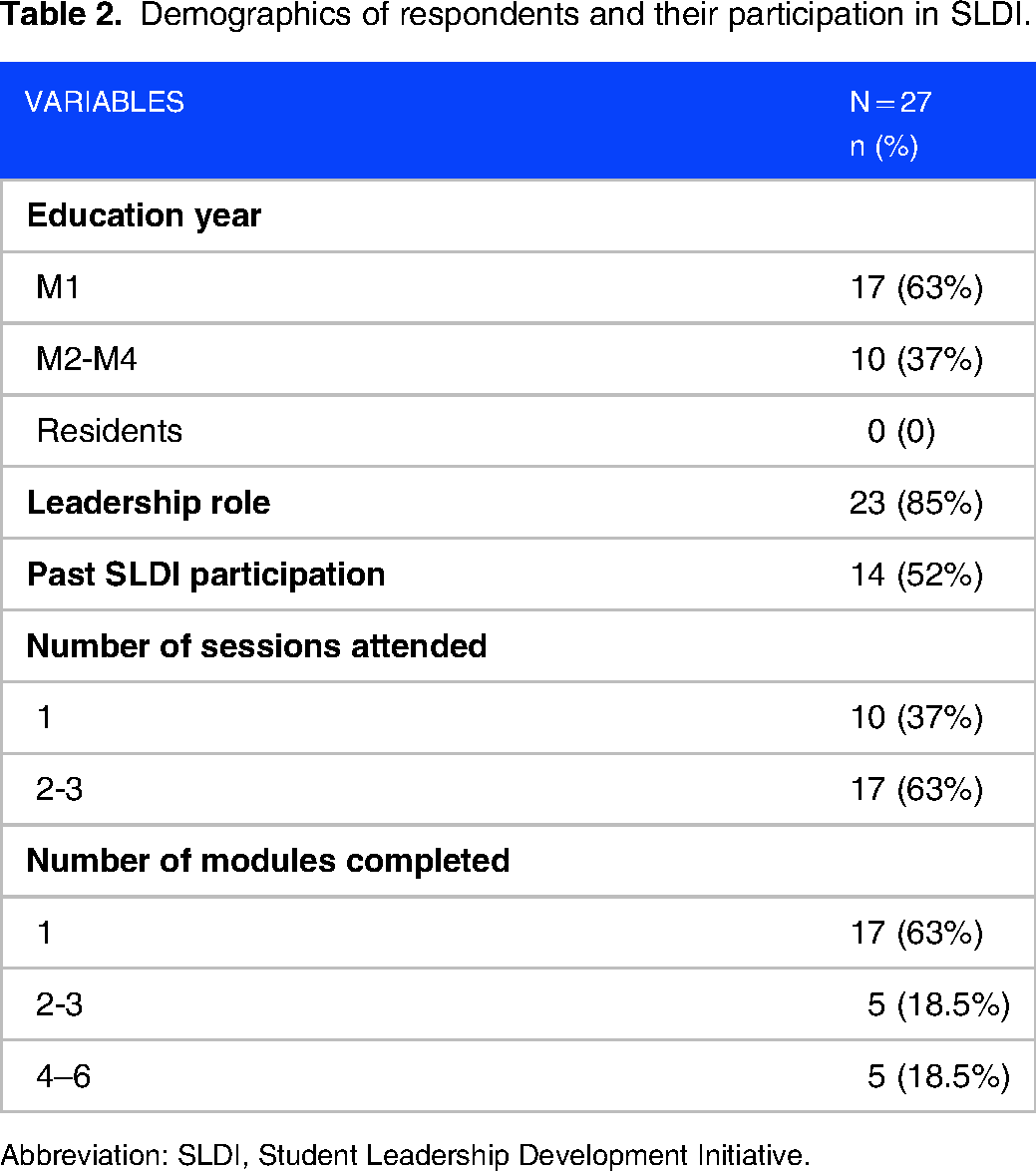
Abbreviation: SLDI, Student Leadership Development Initiative.
Furthermore, 82% of the respondents felt that leadership skills were of similar importance to clinical knowledge and skills for being an exceptional physician, while 7% felt leadership skills were more important (Figure 1). The students’ perception of leadership importance did not influence the number of self-directed modules completed (p > .05).

Respondent's self-reported perception of the importance of leadership skills in comparison to clinical skills.
And 85% strongly agreed or agreed that SLDI helped them develop professional goals and career paths (Figure 2). And 74% reported benefits in becoming more compassionate physician leaders and valuing wellness. And 63% reported benefits in identifying specific ways to improve leadership skills and 56% reported benefits in building confidence to lead a team.

Benefits of virtual SLDI. Abbreviation: SLDI, Student Leadership Development Initiative.
Twelve out of 21 attendees (57%), 7 out of 20 attendees (35%), and 4 out of 8 attendees (50%) responded to each respective postevent survey, with written feedback being overwhelmingly positive. Out of these 23 respondents, 97% and 91% reported they probably or definitely intended on applying what they learned to their work and sharing their learnings with others, respectively; however, only 46% reported meeting someone new at events and 32% reported that they intended on connecting with new contacts.
Discussion
Our results suggest that implementation of extracurricular, virtual leadership training that involves both small-group speaker events and self-directed modules are feasible and beneficial for medical students. This is in line with other elective/extracurricular student-led leadership initiatives. Recent work by Richard et al reported that student participation in 6, in person 90 min sessions led by a variety of healthcare leaders as part of an elective course improved participants’ self-reported confidence and leadership skills. 13 Our study similarly showed that 60% of respondents stated an improvement in their leadership skills and confidence after participation in SLDI, with the added benefit of being held via a virtual environment that requires less resources and is more cost-effective. There are many other differences in the curricula between our study and Richard et al's work, however there are some key similarities: (1) sessions led by current healthcare leaders who can serve as role models for attendees, (2) elective/optional participation, and (3) emphasis on student-led discussions. These key elements have been incorporated by other student-led initiatives as well,14,15 which report largely positive feedback from students and improvements in leadership skills. One of the main additional takeaways from these other studies is the importance of supporting experiential learning not only through self-directed modules but also through student-driven projects14–16; we hope to incorporate such opportunities in future iterations of SLDI. Importantly, we hope to develop virtual modalities to support student projects to maintain the cost-benefits and flexibility-benefits provided by our current structure.
Key differences and similarities between our study and prior studies on in-person SLDI events were noted. In both virtual and in-person SLDI, the majority of participants held leadership positions, 17 questioning whether voluntary, extracurricular leadership training is only utilized by those who self-identify as leaders. Prior studies received responses predominantly from upperclassmen (66% M2-M4s) as well as residents (20%), 17 compared to the high proportion of first year medical students in our study. This suggests a potential shift in demographics of student involvement with the virtual transition. Additionally, ~60% of respondents felt that virtual SLDI improved their leadership skills and built confidence, compared to 80% and 71%, respectively, with in-person programming. 17 The underlying cause of this difference is unclear; however, a recent systematic review noted that major disadvantages of virtual learning for medical students included lack of networking opportunities, suboptimal communication skills, poor motivation, decreased student engagement, and lower confidence levels in skills. 18 These critical influencers of leadership development have been noted as shortcomings from other leadership programs that shifted to virtual environments. 19 Similarly, the low proportion of students that reported meeting new people at events also reflects the limitations of virtual environments in fostering meaningful networking opportunities. 18
Our results contribute to a growing body of literature that report that medical students recognize the importance of leadership competency in becoming a successful clinician.4,20,21 Given that only 3 events were held secondary to COVID-19 challenges, we were unable to ascertain whether the number of events attended was associated with students’ perception of leadership importance as reported with in-person SLDI sessions. 17
Response rates ranged between 35% and 57% for postevent surveys administered to those who attended the events. However, only 14% of those in our listserv responded to our one-time survey, and thus the results may not reflect opinions of all SLDI participants. This is similar to the 17% survey response rate from past studies. 17 We suspect this is due to a large number of medical students that signed up for the SLDI listserv and thus received the survey, but only a small proportion of them actually participated consistently in events. The lack of involvement within SLDI does not currently result in the removal of students from listserv. While this is a key limitation of our study, the results are in line with prior studies reporting that in almost 50% of the existing elective leadership training at medical schools, <20% of students participated in them. 22 Future studies that survey only those who consistently participated in SLDI are needed for ascertaining the true response rate and improving the generalizability of our results.
Our study is limited by the retrospective nature of our surveys and lack of a control group that did not participate in SLDI. Thus, our respondents may be affected by recall bias, and our results are not broadly applicable to medical student populations. Additionally, while the questions from our survey are similar to prior work, 17 they were not validated or pilot-tested. A sample size/power analysis was also not performed for this study. Nonetheless, our study supports the feasibility and potential benefits of a virtual, voluntary, student-driven leadership program for medical students already holding leadership positions. While we discussed differences compared to past in-person events, changes in program leaders, the speakers invited, and total number of events held resulted in our inability to draw statistical comparisons and conclusions regarding the impact of virtual transitions.
Conclusion
Our results suggest virtual leadership training, involving small-group discussions and self-directed modules, is feasible, inexpensive, and beneficial for medical students. Virtual sessions are easier to integrate within curricular time and having multiple training modalities may help cater toward different learning styles among students, helping to overcome current barriers for implementing leadership training within UME. Notably, the inability to promote meaningful networking opportunities is a major limitation of a virtual training model.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231200731 - Supplemental material for Student Leadership Development Initiative for Medical Students: Lessons Learned From Transitioning to Virtual Modalities
Supplemental material, sj-docx-1-mde-10.1177_23821205231200731 for Student Leadership Development Initiative for Medical Students: Lessons Learned From Transitioning to Virtual Modalities by Gopika SenthilKumar, Kelli C. Sommers, Yizeng He, Katarina Stark, Taylor Craig, Aliyah Keval, Neemit Shah, Kahaan Patel and John Meurer in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors acknowledge Ezzeddine Elmir for his contribution as part of the SLDI leadership team.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Advancing a Healthier Wisconsin Endowment (grant number Learning Event Support).
Author contributions
GSK was involved in conception and design of the study, data collection and interpretation, drafting the manuscript, and critical revision of the manuscript. KEC was involved in conception and design of the study, data collection, and critical revision of the manuscript. YH was involved in data collection, analysis and interpretation, and critical revision of the manuscript. KS, TG, AK, NS, and KP were involved in design of the work and critical revision of the manuscript. JM was involved in conception and design of the study, data interpretation, and critical revision of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.