
Abstract
Medical students who underperform or find they are not a “good fit” for medicine have limited options. A terminal master's degree represents an exit alternative that recognizes students’ completed coursework and acknowledges their commitment to the medical sciences. Although medical educators have called for the creation of such programs, termed “compassionate off-ramps,” the prevalence of degree offerings in US programs is unknown. In the fall of 2020, a survey was sent to Student Affairs Deans at 141 LCME-accredited MD programs; 73 institutions responded (52%). Terminal master's degrees were offered by 19% of respondent institutions (n = 13). While 85% of those without a terminal master's (n = 48) endorsed degree benefits, only 36% (n = 21) had plans to create the degree. This study demonstrates that few US medical schools offer a terminal master's degree, leaving students who exit medicine with high levels of debt without an avenue for a degree to support employment or future academic pursuits. The authors identify implications for students, particularly those who are at a higher risk of failing Step 1, such as students who are underrepresented in medicine, socioeconomically disadvantaged, or who have a disability and are unaccommodated. Potential barriers to terminal master's program creation are identified and mitigating strategies are recommended.
Introduction
After completing the first 2 years of coursework, some medical students cease pursuit of a medical degree, often due to poor fit with the profession, extenuating personal or health-related circumstances, or inability to pass the USMLE Step 1 examination. Medical education stakeholders have advocated for the creation of “compassionate off-ramps” in the form of master's degrees for coursework completed.1–3 Terminal master's programs vary in format, but generally involve students applying completed preclinical coursework to a medical sciences master's degree, usually in conjunction with the submission of a thesis, capstone project, or literature review.
Students who repeatedly fail Step 1 are often dismissed or asked to withdraw from their programs, regardless of prior academic accomplishments.1,2 For these students, exiting medical school is driven by high stakes standardized exam results or lack of exam access,4–6 as opposed to course failure or insufficient professional interest. The National Board of Medical Examiners reported that 3% of first-time test takers failed Step 1 in 2019, 7 some of whom applied for, but were denied, accommodation. 4 While a small percentage fail Step 1, the consequences of Step 1 failure can be dire,4,8 and many of these students will be forced to leave medicine without a degree.
Exiting medicine after the preclinical years has considerable consequences and may create a tripartite challenge for learners: debt, no degree, and potential adverse impacts on wellness.1–3 For 2020 graduates, the average medical school debt was US$207 003. 9 At year 2, this would amount to an average of over US$100 000 with no earned degree to support employment or future academic pursuits. The drivers of medical school withdrawal (eg, poor academic performance, Step 1 failure, poor fit, extenuating personal or health circumstances)1–4 place significant stress on students, a group already at higher risk for depression.10,11 Students in this position may feel overwhelmed with feelings of failure, loss of social networks, and disappointment from family. These challenges may be further exacerbated by a student's loss of access to supportive institutional resources once withdrawn (eg, counseling, advising, health insurance, and housing).1–3 Lack of degree, and the resulting gap in a student's resume, may make it difficult to apply to another academic program or to find employment.
It is important to acknowledge that some groups are more likely to be impacted by Step 1 failures. This was demonstrated within a cohort that took an earlier iteration of Step 1 between 1993 and 2001:Students underrepresented in medicine URiM, racial and ethnic populations that are underrepresented in the medical profession relative to their numbers in the general population, represented 48% of Step 1 failures 12 while the percentage of URiM students was well below 20%. 13 Another study demonstrated that graduates from one of 6 midwestern medical schools in the Classes of 1997 to 2002 who failed Step 1 on their first attempt were significantly more likely to be women, URiM, first-generation college graduates, and nontraditional students. 8 More recently, using data from more than 45 000 examinees that took the exam between 2010 and 2015, researchers reported that students from underrepresented racial and ethnic groups had lower mean scores on USMLE Step exams, 6 a trend that has been shown across other standardized exams.14–19 Studies demonstrate that, in the aggregate, students who are underrepresented in medicine URiM have lower mean scores on the MCAT, an exam that has been utilized by medical school admissions officers.17–19 Recent data demonstrate that students with disabilities also have lower mean scores on the MCAT than students without disabilities. 20 Collectively, these trends suggest underrepresented and marginalized groups of students are more likely to be overrepresented among those who fail Step 1.
Students from underrepresented groups experience multifactorial, historical, and systemic inequalities that precede medical education14–24 and may contribute to increased risk for Step 1 failure and are also more likely to encounter financial barriers,22–24 which may prevent them from purchasing cost-prohibitive educational preparatory materials. 25 Students with disabilities share similar struggles to accessing the Step 1 exam in the form of accommodations. Without the accommodations necessary to fully engage with the material, these students are also at increased risk of failure.4,5 For students who identify as disabled and URiM and/or socioeconomically disadvantaged, the barriers associated with taking Step 1 may be exponential including increased difficulty obtaining the often costly documentation required to support strong Step 1 accommodation applications. 26
Some institutions acknowledge and address these systemic barriers by providing funding for students to obtain commercial exam preparation programs, 4 offering in-house exam preparation programs,27–29 and/or purchasing commercial programs for all students,30–32 while others mitigate barriers for students with disabilities by providing funding to obtain clinical evaluations, such as neuropsychological evaluations, that are required to support students applications for accommodations on USMLE examinations. 33 While MCAT accommodation applicants who qualify for the Fee Assistance Program can apply for a subsidy to support expenses related to obtaining updated clinical evaluations 34 no such supplementary funding opportunities are offered for USMLE examinees. 35 Without widespread and nationally consistent measures to address financial barriers within medical education, the effects of systemic inequalities are perpetuated and disproportionately impact certain students, placing them at risk for failure on the Step 1 exam, potentially thwarting their ability to persist in the program.36–38
A call for compassionate off-ramps
Recent literature calls for medical education stakeholders to create “compassionate off-ramps” whereby students who leave medical school may achieve a terminal master's degree.1,2 This represents an option to address one of the multifaceted issues associated with students who leave medicine: providing recognition of students’ successful completion of basic science coursework and acknowledging their commitment to medical sciences.1–3
A study of 12 terminal master's programs suggests that requirements in current “off-ramp” programs varied considerably with many requiring a capstone or thesis in addition to coursework completed; few students utilized the degree option; and that the degree helped reduce overall institutional student debt statistics, honored student effort, and improved career options. 3 However, there is a gap in the literature on the availability of, or institutional plans to create, a terminal master's degree at US allopathic medical schools. Given the potential financial, vocational, psychological, and social consequences of leaving medical school without a degree, more information is needed to identify options for these students. This study aims to understand the number of US allopathic medical schools that offer terminal master's programs or plan to create them in the near future, as well as program beliefs regarding the potential benefits of a terminal master's degree.
Methods
Between June and October 2020, an online Qualtrics survey was sent to Student Affairs Deans at all fully accredited Liaison Committee for Medical Education (LCME) allopathic medical schools (n = 141). Responses were collected from June to October 2020, with email reminders sent in July, August, and September. The University of Michigan Institutional Review Board reviewed the study and assigned a “non-regulated” status (E-study ID: HUM00175997). This study sought to understand the availability of a terminal master's degree program for students who are unable to continue their studies as part of a larger study on the institutional impact of accommodation denial on USMLE Examinations.
Survey
A 10-question survey was designed by the authors [LMM and KHP] as part of a larger survey on the impact of nonaccommodation on medical school operations. 4 The 3 questions used in this study focus on the availability of a terminal master's degree for students who do not wish to persist to the MD, or for whom this is not an option academically.
The primary question asked, “Does your institution offer a terminal Master's degree for students who do not wish to, or are ineligible to continue studies beyond the pre-clinical years (Y/N)?” For programs that did not have a terminal master's option, 2 additional yes/no questions were asked: (1) Do you believe that a terminal master's degree would be beneficial for students who choose to withdraw or are ineligible to continue beyond the preclinical years because of a Step 1 failure (Y/N)? and (2) Is your program planning to add a terminal Master's Degree (Y/N)? The survey content was pilot tested by 3 medical school student affairs deans who were not institutional respondents for the final survey. The survey was refined for content and clarity following their feedback.
Statistical analysis
Response percentages were obtained using basic counts and were linked to the 2018 AAMC Organizational Characteristics Database. 39 Data included: medical schools’ region, ownership, financial characteristics, and class size. All organizational data, except class size, were categorical. One investigator (BC) developed categories for class size using national medical school cohort means and ranges as a guideline. Class size categories were defined as small (< 100 students), average (100-200 students), and large (> 200 students). To assess the representation of survey data, respondents were compared with nonrespondents using Pearson's chi-square and Fisher's exact tests. Data analysis was conducted using IBM SPSS Statistics Version 26.
Results
Seventy-three of the 141 schools completed the survey (52%). No associations were found between answers to the questions pertaining to terminal master's degree availability and the 2018 AAMC database of institutional characteristics or class size. Of the 73 responding schools, 13 (19%) reported having a terminal master's degree option. The majority of programs (n = 57; 81%) did not offer a terminal master's, yet 85% of these respondents (n = 48) agreed that such a degree would be a beneficial addition to their program. Despite this high endorsement of a terminal master's degree, only 36% (n = 21) planned to add one to their program (Figure 1).
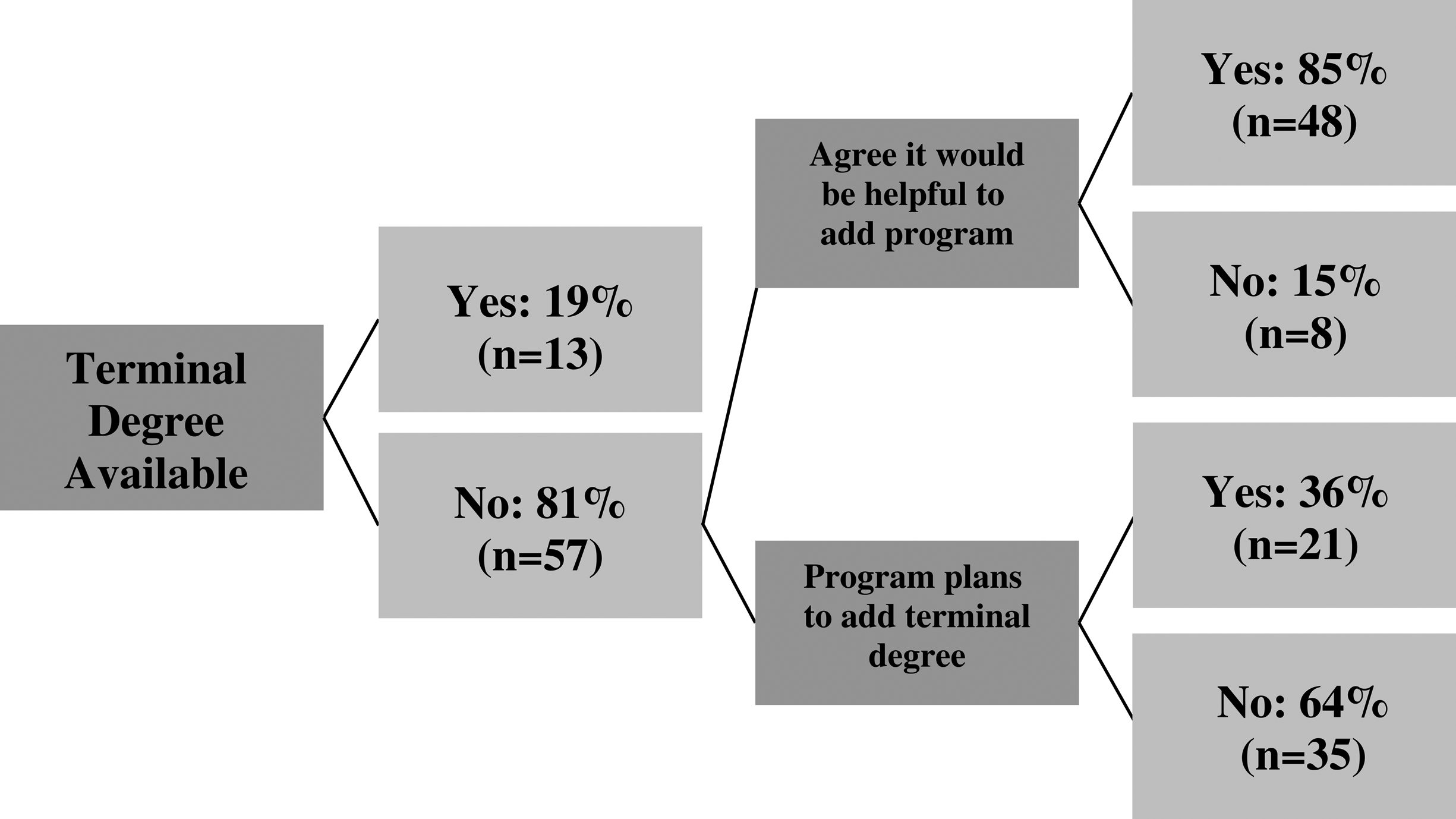
Availability, plans, and perceptions of terminal master's in allopathic medical schools.
Discussion
This study demonstrated that, despite literature supporting the potential benefits,1–3 a small number of medical schools offer a terminal master's degree for students who cannot continue past the preclinical curriculum. There is a considerable gap between the number of medical schools that acknowledge the value of offering a terminal master's degree and those with plans to offer one. We propose that 3 institutional barriers may be perpetuating this gap: lack of cross-school coordination, lack of tangible incentives, and bureaucratic inertia.
First, barriers pertaining to cross-school coordination may prevent partnerships with the institution's graduate school, hindering program approval and establishment. Furthermore, implementation often requires the development of new academic elements (eg, capstone project, courses, thesis), 3 which may be costly and time consuming to develop and administer.
Second, financial and reputational incentives may be lacking, as additional requirements may be viewed as a potential financial liability by administrators. Tuition for the MD coursework was paid to the medical school, disincentivizing the graduate school from conferring a degree. Medical school stakeholders may fear a decreased graduation rate with students electing the terminal master's; however, previous research suggests that a small number of students elect this option. Given the low overall attrition rate in medical education (∼ 3%) 40 and the low number of students who engage in the existing terminal master's programs, 3 it is reasonable to surmise that the students who elect the “off-ramp” are likely the same students who would have exited the program regardless of degree options, hence not impacting MD graduation rates.
Third, schools may suffer from bureaucratic inertia, the tendency for organizations to stay on the same path. 41 Given the small number of individuals impacted and the investment of time and resources required, administrators may justify inaction.
Notwithstanding these potential barriers, Bellini and colleagues argue for the “moral imperative” to create terminal degree options for students. 1 This moral imperative is further strengthened by the current conditions, where marginalized and underrepresented groups seem to be more likely to fail Step 1 and more likely to leave medicine, often without any tangible outcome for their efforts.4,6,8,42 Debt without a degree can be catastrophic for those who are unable to complete an MD program. A terminal master's degree allows medical students to demonstrate their knowledge of and commitment to the medical sciences. 2 This option shifts the focus from penalizing students for what they were unable to achieve (eg, unable to pass Step 1, complete third and fourth year) to acknowledging their accomplishments in the preclinical curriculum. Subsequent benefits include opportunities for employment or further training and a pathway to pay off acquired debt. Offering such a degree may also remove pressure from students who do not want to continue to pursue a medical career but may contribute to the biomedical workforce in other ways. Finally, providing a compassionate “off-ramp” may reduce the social stigma of being a medical school “dropout” within a population that is at increased risk of depression compared to same-aged peers.1–3,10,11
Compassionate off-ramps alone are not the solution. The striking differences between performance and persistence in underrepresented groups suggest that systemic and cultural barriers exist within medical education that are long-standing and deeply ingrained. Given the disproportionately higher number of students from marginalized backgrounds who leave medicine, 40 a need to address systemic racism, colonialism, ableism, classism, and sexism in medicine is clear.4–6,17,18,25,36–38,43–46 The added stress of navigating these marginalizing forces takes a toll, creates conditions that inhibit thriving in medicine, and may create conditions wherein barriers are so high and seemingly insurmountable that leaving is a desirable outcome—at a time when medicine desperately needs more diverse physicians.36–38,42–46 Therefore, it is critical to creating compassionate off-ramps for those who desire to leave medicine, while simultaneously examining the structural and systemic barriers that may force an exit for students who wish to stay. This will require an equity evaluation of supports for Step 1 preparation and applications for Step 1 accommodation so that maximum support is provided to all students.
This study has limitations. First, these findings only represent half of the medical schools and may underrepresent the availability of terminal master's degrees. Second, response bias may lead to an overrepresentation of schools that have an interest in developing a terminal master's degree or have experienced student dismissals where a terminal master's could have provided support. Third, we did not seek further elaboration regarding the disjuncture between a perceived benefit and plans to create a terminal master's degree.
Conclusion
To our knowledge, this is the first study to examine the current and planned availability of terminal master's degrees in MD programs. A terminal master's may present a “compassionate off-ramp” for students unable to continue medical school, positively impacting their well-being and career possibilities. To date, few schools offer these degrees and, despite many seeing the utility, most do not plan to add this degree option. Future studies should examine the long-term impact for students who elect a terminal master's degree, including well-being, career trajectory, and experiences of students who leave medicine. Efforts should be made to retain students following an initial Step 1 failure through academic and disability support.
Supplemental Material
sj-pdf-1-mde-10.1177_23821205231164022 - Supplemental material for Compassionate Off-Ramps: The Availability of Terminal Master's Degrees in US Medical Schools
Supplemental material, sj-pdf-1-mde-10.1177_23821205231164022 for Compassionate Off-Ramps: The Availability of Terminal Master's Degrees in US Medical Schools by Kristina H Petersen, Neera R Jain, Ben Case, Sharad Jain, Sarah L Solomon and Lisa M Meeks in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors would like to thank the student affairs deans at participating medical schools for their partnership in collecting the data, thus facilitating this study. No one received any financial compensation for this work.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Partial financial support was obtained through a diversity grant from the University of Colorado Anschutz Medical Campus Office of Diversity Equity Inclusion and Community Engagement. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conceptualization: Kristina Petersen and Lisa Meeks; Methodology: Lisa Meeks, and Ben Case; Formal analysis and investigation: Ben Case and Lisa Meeks; Writing – original draft preparation: all authors. Writing – review and editing: all authors; Funding acquisition: Lisa Meeks; Resources: Lisa Meeks; Supervision: Lisa Meeks. All authors read and approved the final manuscript.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.