
Abstract
CONTEXT
Little research exists to determine if medical students experience symptoms of depression after examinations and if symptoms vary by gender.
OBJECTIVES
Determine if is there a difference between male and female medical students in the number of symptoms of major depressive disorder (MDD) experienced after exams, as well as which coping strategies are used by students to alleviate depression symptoms.
METHODS
An anonymous and secure survey was sent via university email to first, second, and third-year medical students after exams for 2 consecutive exam periods. Surveys that were not fully completed were excluded from the analysis.
RESULTS
A total of 162 out of 550 students completed the survey for a response rate of 30%. Overall, a greater proportion of female students experienced more symptoms of depression compared to males. This was statistically significant for the Diagnostic and Statistical Manual of Mental Disorders 5th Edition symptoms of MDD: depressed mood, anhedonia, changes in sleep, fatigue, and difficulty with concentration after exams compared to their male counterparts. Male first-year medical students experienced higher rates of depression compared to their third-year counterparts. Most students exhibited coping strategies that helped them feel less depressed. The 3 most common coping strategies reported were: reaching out to social support networks, physical activity/exercise, and engaging in hobbies.
CONCLUSIONS
Both gender and year in a medical school play a role in the number of symptoms of depression experienced after medical school exams. Recognizing that examinations can be a trigger of depressive symptoms in medical students, particularly female and first-year students, has important implications on student mental health. Helping students recognize these symptoms and employ healthy coping strategies may further help alleviate these symptoms. Long-term consequences of experiencing symptoms of depression after recurrent exams in medical school are unknown and require further research.
Introduction
Estimates vary, but well over a quarter of all medical students experience depression during their medical training.1–6 Additionally, around half of all medical students experience symptoms of distress or burnout, defined as “work-related syndrome involving emotional exhaustion, depersonalization, and a sense of reduced personal accomplishment” 7 at some point during their education.1,8–10 Burnout is often associated with depression or psychiatric illness and in recent years has been noted to be a global phenomenon affecting students and health care providers alike. Therefore, student mental health is an important and pertinent topic of research and discussion, to identify triggers of destabilization and thus combat both mental illness and burnout in our future health care providers.1,7,8 Multiple studies show that medical students experience higher rates of depression compared to the general population,11–14 with gender being a major factor that impacts depressive symptoms.3,15–17 However, the true incidence of depression in medical students compared to the general population remains unknown, as some studies show conflicting data, where medical students were found not to have higher rates of depression compared to students studying business or humanities.18–20 The relationship between gender and depression in medical students is also mixed with some data supporting that female medical students experience more depression,5,13,21–24 while other studies find no difference in symptoms between genders.6,25,26 Most of the above-cited studies are cross-sectional and look at depression at 1 point in time in medical school. This makes it challenging to find the true incidence as many different factors, including life stressors, can impact a student's emotions. The topic of depression in medical students is further complicated as the above-cited studies are taken from multiple different countries. Not only do different cultures likely play a role in the development of symptoms of depression, but in countries outside the USA, medical education often begins immediately after high school, whereas in the USA medical school begins after at least an undergraduate education has already been completed. Additionally, most studies compare medical students to students in other professions, not individuals who are nonstudents, adding to the complexity of this topic. Regardless, across most studies, alarmingly high rates of depressive symptomatology were found in medical students. Understanding precipitating factors and identifying methods to alleviate the mental burden endured by our future health care providers is both timely and imperative.
As of 2019, 17.3 million Americans (7.1% of the population) suffer from major depressive disorder (MDD). 27 According to the National Institute of Mental Health, female adults suffer from MDD at higher rates (8.7%) than their male counterparts (5.3%), and adults aged 18 to 25 years make up the largest group of individuals diagnosed with MDD at 13.1%. 28 These findings were confirmed by many other studies.29–31 Notably, the median age of female and male adults entering medical school is 23 and 24 years old, respectively, with both genders falling into the age group most vulnerable to developing symptoms of MDD. 32 Yet, other data suggests that the emergence of depressive symptoms in medical students is not affected by age. 15 Whether or not medical students develop these symptoms because of their age or other factors surrounding being in medical school is not known. Having a diagnosis of MDD as a medical student was found to be an independent predictor of burnout later in training, jeopardizing the longevity of future physician's careers and leading to potential job dissatisfaction. 33 Additionally, residents with burnout and depression make statistically more errors compared to their nondepressed peers. 34 These facts highlight the importance of identifying factors contributing to depressive symptoms in medical students and provide an opportunity for early intervention and an integral step in preventing burnout and fostering physician well-being, starting in the formative years of medical education.
One longitudinal study aimed to identify possible predictors of psychiatric morbidity in medical students and found that “high levels of performance-based-self-esteem, depressive symptoms, and disengagement” in first-year medical students led to an increased risk of being diagnosed with psychiatric conditions, including MDD and generalized anxiety disorder, as third-year students. 27 Previous research from a cross-sectional study has noted consistent stressors for medical students, including excessive workload, difficulties with time management, conflicts in work–life balance, administrative failures (unsupportive learning environment, inefficient scheduling, and communication problems), concerns about career planning, and performance pressure, including “constant assessment, subjective grading, and high stakes exams.” 35 Other studies have identified major factors contributing to student examination anxiety, such as extensive and intensive course load, inadequate rest, sleep disturbance, and inability to relax physically. 36 Increasing performance pressure is understandable as medical school and residency selection have become increasingly dependent upon examination scores, with many residency programs ranking medical board examination performance as the top factor in determining whether to interview an applicant. 37 While research shows that medical students do not feel that examinations accurately reflect their knowledge, 28% of students still believe that examination performance is directly related to future success. 36 With increasing emphasis on examination performance impacting future career options, the weight of academic performance on medical students may take its toll on mental health. Previous research has shown that medical students use a variety of coping strategies. One study found social supports to be the most popular coping strategy, with substance use having the lowest prevalence. 38 In the current study, the researchers chose to look at positive coping strategies as well as substance use.
The ability to identify and address factors that increase medical student predilection for depression or burnout may lead to better student and physician mental well-being in both the short- and long-term. The researchers in this study aimed to look at 1 particular potential trigger of depression symptoms in medical students by examining depressive symptoms of medical students after examinations. There is a notable lack of information regarding student experiences with depressive symptoms after examinations, which is an important factor in understanding how high-intensity examinations relate to student mental health, burnout, and future well-being. Understanding the interplay between medical school examinations and depression in medical students is complex. In this study, the authors aimed to assess whether medical students experience symptoms of depression after exams and if there is a difference between male and female students. In doing so, the authors hypothesized that: (1) medical students experience high rates of depressive symptoms after exams; (2) female medical students experience higher rates of depression than their male counterparts; and (3) most medical students use coping mechanisms to deal with such symptoms of depression. Collecting this data is the first step in understanding if medical school exams may be a contributing factor to medical student mental health. Understanding coping mechanisms used by medical students is also important information that could help alleviate depressive symptoms in students.
Method
A survey was distributed via email using the secure REDcap platform to first-, second-, and third-year medical students at the University of New England College of Osteopathic Medicine (UNECOM) in Biddeford, ME, after taking school examinations (for first- and second-year medical students) or Comprehensive Osteopathic Medical Achievement (COMAT) examinations for third-year medical students. The survey was sent to a total of 550 students after medical students received their grades from their most recent exam. The same survey was sent to students after 2 different exam periods, and students were asked to only respond once. This was done to achieve a wider sample size and to allow students who had not responded to the survey after the first exam period to participate in the survey after a second consecutive exam period. The difference between exam periods ranged from 2 to 6 weeks depending on the year in medical school, this was due to the fact that at UNECOM, first-year students are tested the most often, typically in a week-long block exam format, second-year students are tested less often usually, every 3 to 6 weeks and third-year students are tested the least frequently, every 6 to 12 weeks. All exams were computerized multiple-choice examinations. Exams in the first year are based on material learned in the past 2 weeks in an integrated curriculum, exams in second-year are summative and given at the end of each body system block, and exams in third-year are standardized across all osteopathic medical schools and given at the end of each core rotation and are specific to the rotation each student is on (COMAT examination). An initial email was sent out immediately after scores were released, and a second email was sent several days later to recruit more participants. Scores were sent out to students within a week of taking the exam.
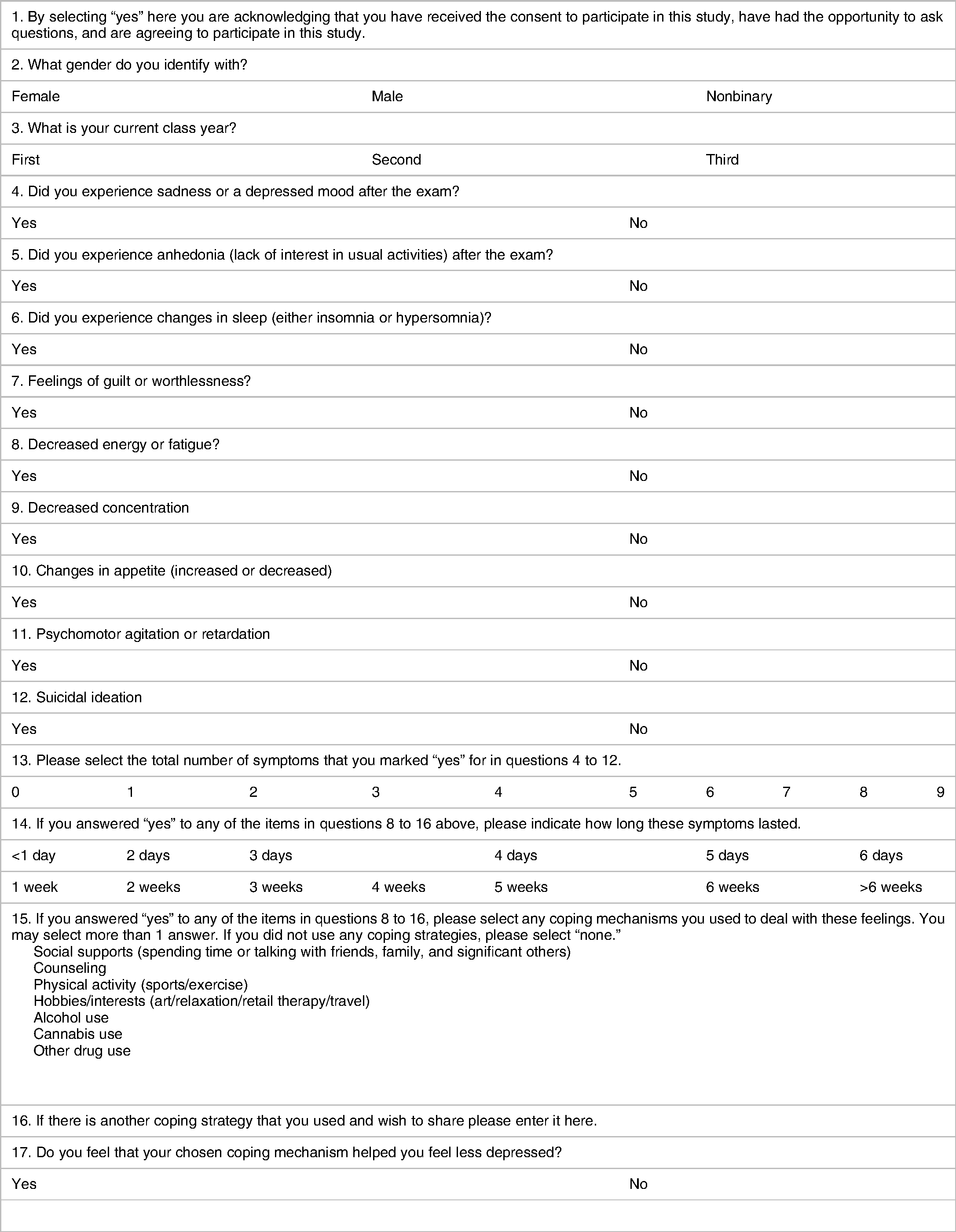
The survey can be found in Table 1. The survey employed was created by the authors and included all of the criteria for MDD as delineated in the Diagnostic and Statistical Manual of Mental Disorders 5th Edition (DSM-5); DSM-5 criteria were used as this is the criterion used to diagnose MDD in the USA where the medical school in which this study was conducted is located, and therefore would be the criterion for which such students would be diagnosed with MDD by a health care provider. Additionally, the coping strategies assessed in the survey were chosen by the researchers, with question 16 being free-response to allow participants to add additional strategies. A statement of informed consent was presented at the start of the survey. The REDcap platform allowed data collection to be collected anonymously and free of identifiers. The study was approved by the University of New England Institutional Review Board. Incomplete surveys were excluded from the analysis. In this survey, gender was assessed in the context of social construct versus biological sex, as students were asked what gender they “identify with” in the survey, not what gender they were assigned at birth. Gender in the social construct versus the biological context was chosen by the authors as they felt this was most representative of the student population. One person reported identifying as nonbinary; because a sample size of 1 was not enough to run statistics on, and due to the potential of identifying this individual in the data set, this survey was excluded from the analysis.
Survey.
Data was compiled and stratified by gender and year of medical school education. All statistical analysis was run using IBM SPSS Statistics. All participants who responded to the survey in full, regardless of answering “yes” or “no” to questions in the survey, were included in the final data analysis. Two-sided chi-square tests were used to determine differences between categorical groups. P < .05 was considered statistically significant. Of note, in the data tables, only the percentage of students who responded “yes” is shown, but the statistical analysis was performed between those who responded “yes” and those who responded “no.” A “*” next to a data point in the below tables denotes a statistically significant difference at P < .05.
Results
Survey Participants
A total of 169 participants (out of 550 surveys distributed) completed the survey in full for an overall response rate of 30.7% (169 of 550). Forty-nine (49) first-year medical students (28.0%), 42 second-year medical students (24.8%), and 78 third-year medical students (46.2%) made up the population of this study (Table 2).
Participant demographics.

*Surveys that were not completed in full were not included in this number.
Numbers are shown as fractions and the percentage of participants per group.
Symptoms of MDD in Medical Students After Exams
In examining depressive symptoms experienced by medical students after examinations, with symptoms lasting <2 weeks, the chi-square test indicated that females experienced more depressive symptoms than their male counterparts (Figure 1 and Table 3). In each MDD symptom investigated, female medical students experienced the symptom at an increased frequency compared to males. Statistical significance was found between genders for the symptoms of depressed mood (P = .017), anhedonia (P = .047), sleep disturbance (P = .019), fatigue (P < .001), and difficulty concentrating (P < .001) (Table 3). For the symptoms of fatigue and difficulty concentrating, nearly 70% of females experienced these symptoms. Males experienced fatigue and difficulty concentrating at a rate closer to 30%, revealing a large difference in symptom expression between genders, albeit still a large proportion of students (Figure 1).
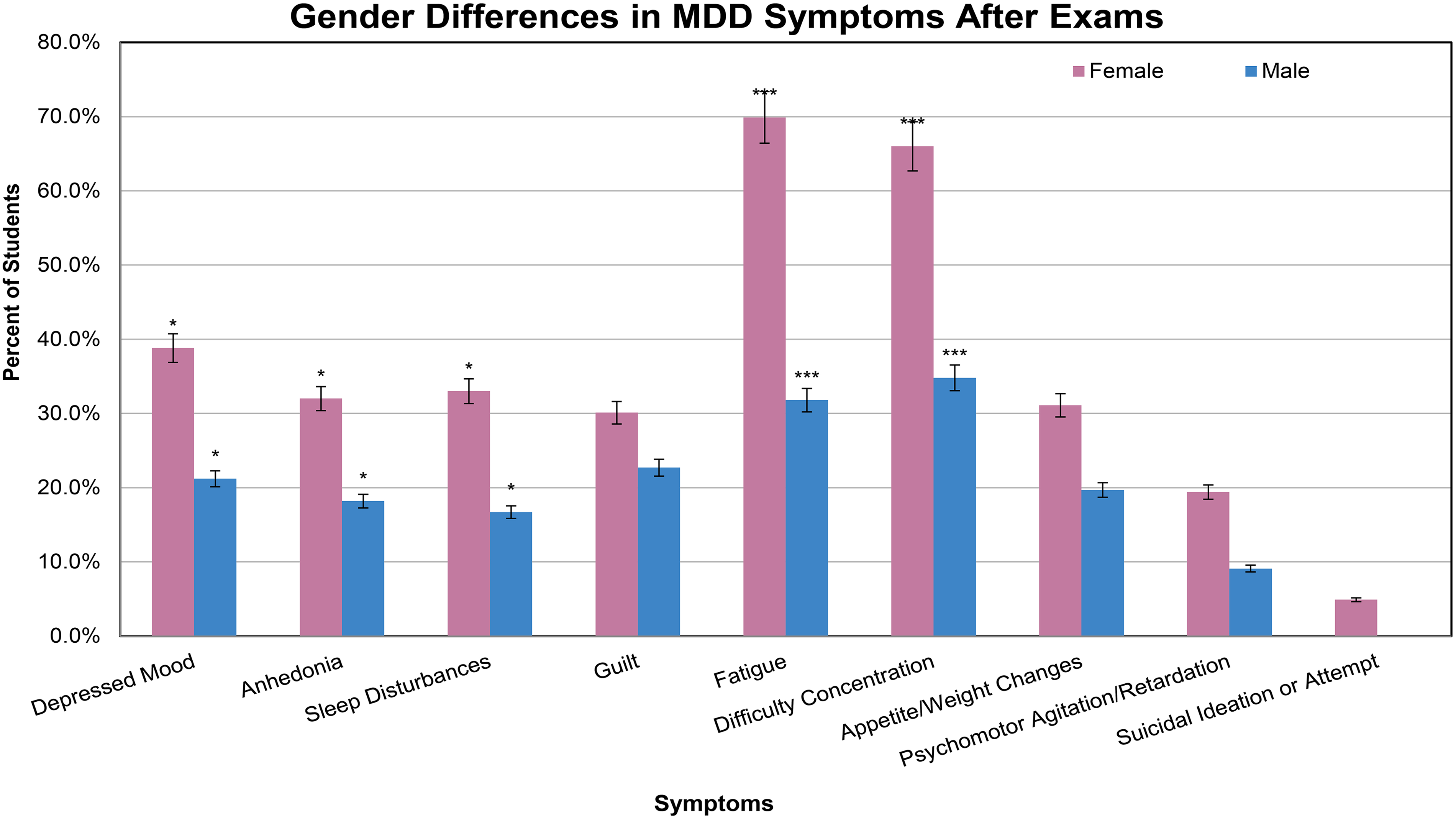
Major depressive disorder (MDD) symptoms experienced for <2 weeks by male and female medical students with first- through third-year medical students grouped together and separated by gender. *Represents P < .05 ***Represents P < .001.
Gender differences in major depressive disorder (MDD) symptoms after exams.

*Represents statistical significance, P < .05.
In examining symptoms of depression across different classes (class years in medical school) divided by gender, significant differences were observed between male first-year and third-year medical students across multiple different symptoms of depression (Figure 2). First-year male medical students experienced a statistically greater incidence of depressed mood (P = .045), sleep disturbances (P = .045), fatigue (P = .034), difficulty with concentration (P = .009), and psychomotor agitation/retardation (P = .032). The same trend was observed for anhedonia (P = .088), guilt (P = .207), and appetite and weight changes (P = .276), although not statistically significant (Figure 2 and Table 4). No males in any year of medical school experienced suicidal ideation. No difference was found between second-year male medical students and males in the other class years, or between females in any year in medical school.
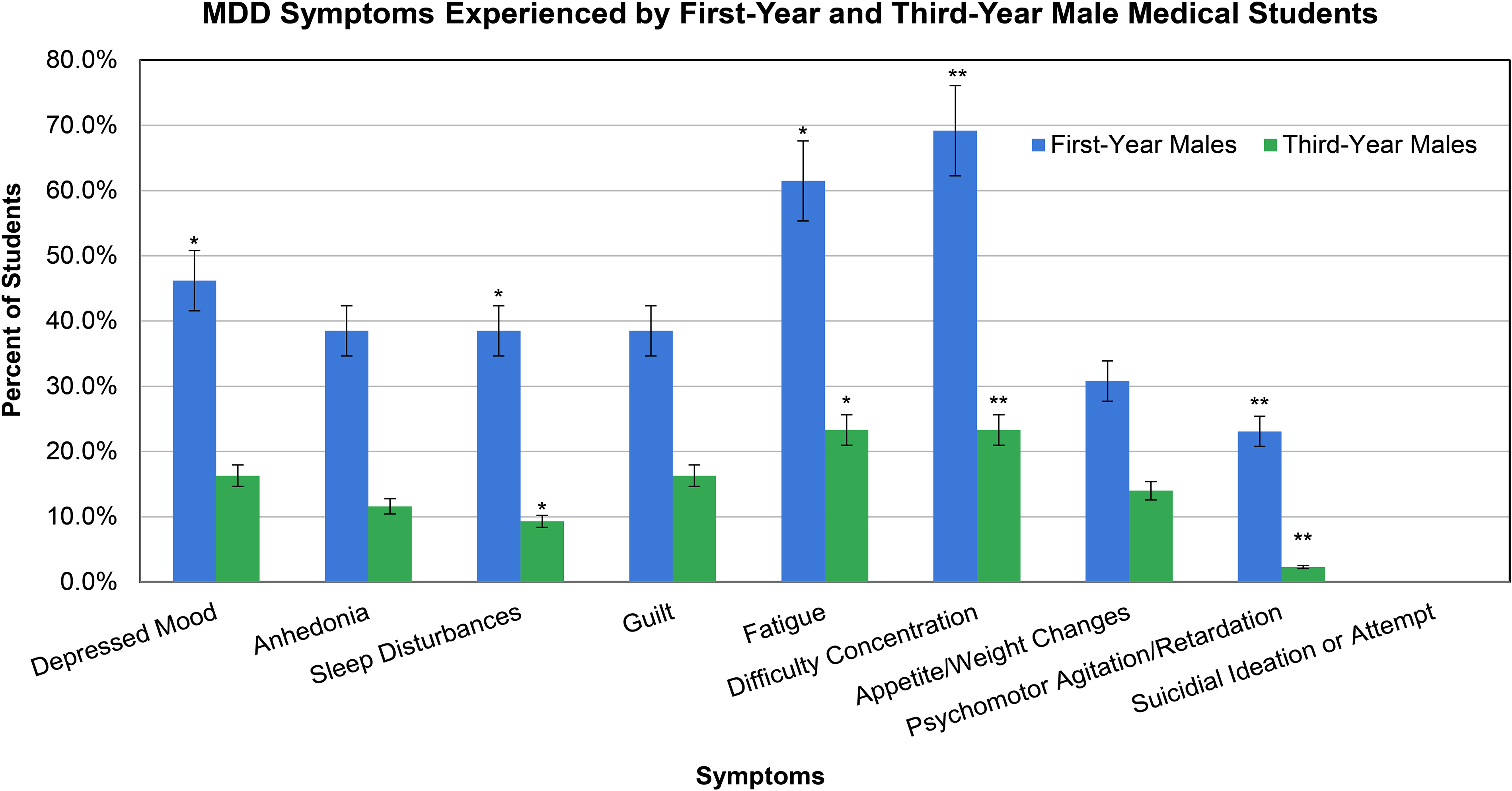
Percent of first-year males experiencing major depressive disorder (MDD) symptoms is significantly more than the percentage of males experiencing MDD symptoms in the third year. Significantly more first-year males experienced 5 or more symptoms of depression (including depressed mood or anhedonia, postexamination) compared to the third-year males. *Represents P ≤ .05 between first and third-year male medical students. **Represents P ≤ .01 between first and third-year male medical students.
Differences in major depressive disorder (MDD) symptoms between the first and third-year male students.

*Represents statistical significance, P < .05.
Gender Differences in Medical Students Experiencing 5 or More Symptoms of MDD for <2 Weeks Including Either Depressed Mood or Anhedonia Postexamination
A greater number of females (29.1%) compared to males (19.7%) experienced 5 or more symptoms of depression, for <2 weeks after exams (Figure 3 and Table 5); however, this was not statistically significant (P = .170). When examining the differences between female and male students who experienced 5 or more symptoms of MDD, broken down by each year of medical school, a statistically significant difference was found between males and females in the third-year class (P = .027) (Figure 4 and Table 5), this difference was not seen in the first- (P = .311) or second-year classes (P = .909).

First through third-year medical students who experience 5 or more symptoms of depression (including depressed mood or anhedonia, and postexamination) for <2 weeks separated by gender.

Medical students who experience 5 or more symptoms of major depressive disorder (MDD) for <2 weeks after exams, separated by class year and gender. *Represents P ≤ .05 between females and males in the same year of medical school. ***Represents P ≤ .001 between the same gender in different years of medical school.
Gender differences in students who experience 5 or more symptoms of major depressive disorder (MDD) for <2 weeks after exams, broken down by year in medical school.
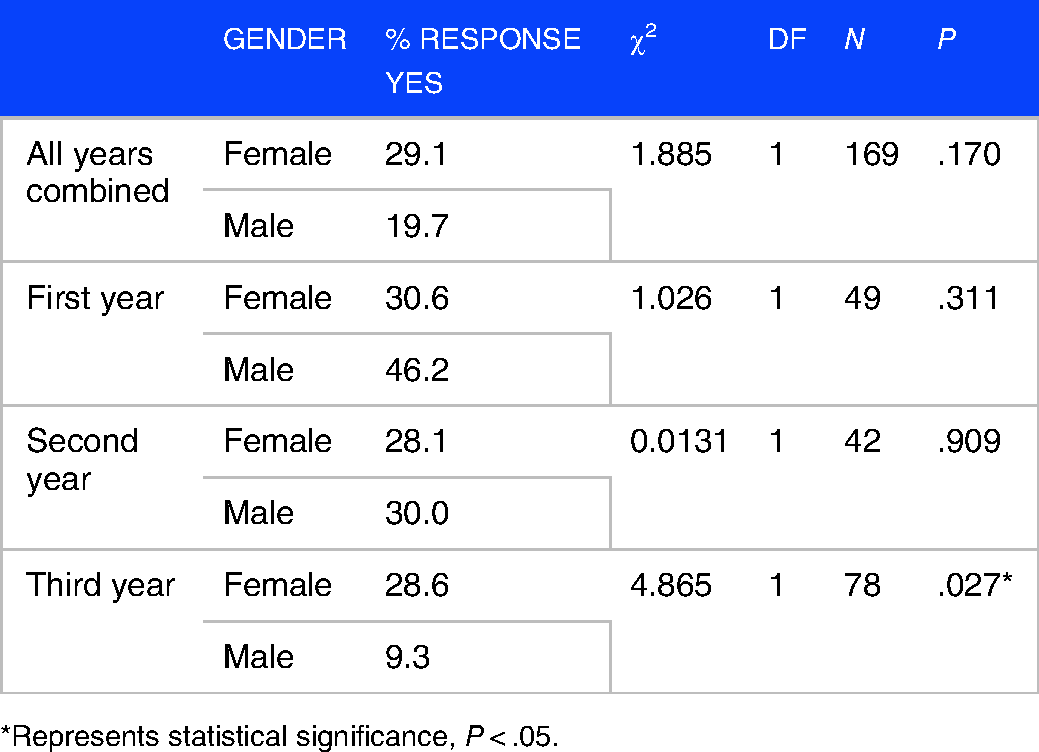
*Represents statistical significance, P < .05.
Medical Students who met Full Criteria for MDD According to DSM-5
Results revealed that 5 medical students overall met full DSM-5 MDD criteria, including symptoms for >2 weeks, all of which were female. This made up 4.9% of the females in this study. No male respondents were found to meet the full criteria for MDD with symptoms lasting >2 weeks. Statistical analysis was not performed on this comparison due to a small samples size (N = 5), which would result in a lack of statistical power 39 (Figure 5).
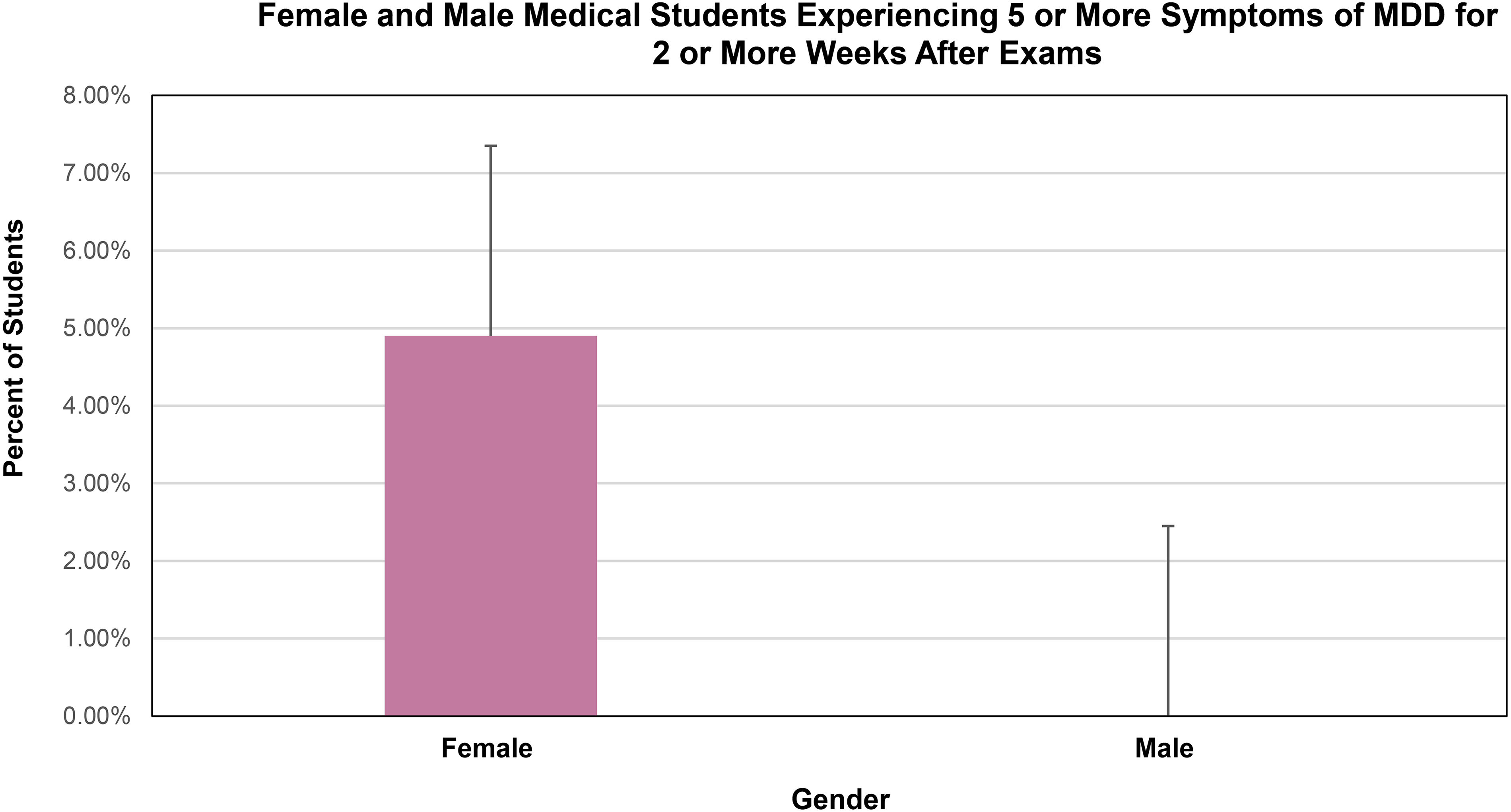
Female and male medical students who meet DSM-5 criteria for MDD. First- through third-year medical students are grouped by gender.
Coping Strategies of Medical Students
When respondents were asked to identify their coping strategies to combat symptoms of depression after exams, most chose social supports (spending time or talking with a friend, family, or significant others) at 80.8%, physical activity (sports/exercise) at 66.9%, or hobbies/interests (art/relaxation/retail therapy/travel) at 53.8%. Less common coping strategies included alcohol use (25.4%), counseling (8.5%), cannabis use (5.4%), other drug use (0.8%), and 10.8% of students said they had no coping strategies. Other coping strategies that respondents submitted included: mediation (3 respondents), TV/movies (3 respondents), refocusing on more schoolwork (2 students), spending time on their phone (1 respondent), mindfulness/stretching (1 respondent), going outside (1 respondent), and sleeping (1 respondent). Interestingly, 90.2% of students said that their chosen coping mechanism helped them feel less depressed, whereas 9.8% did not feel that their chosen coping mechanism helped them feel less depressed (Table 6).
Coping strategies used by medical students.
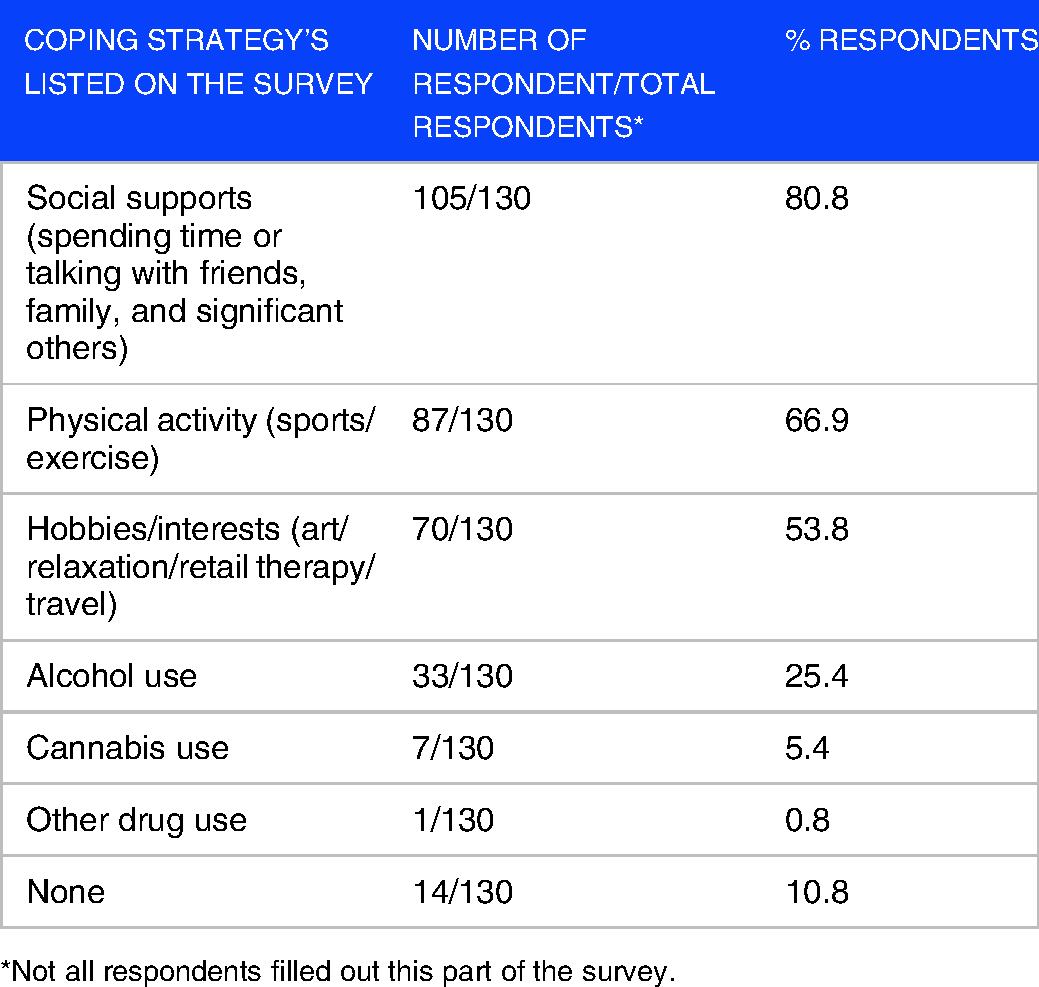
*Not all respondents filled out this part of the survey.
Discussion
There is a great deal of research surrounding medical students and depression,1–4,8,40 as well as how medical school exams cause anxiety and distress.27,35,36,41 There is, however, little research investigating whether medical school exams cause symptoms of depression directly after exams. In the present study, the number of depressive symptoms experienced after exams differed by gender and year in medical school, with females overall experiencing more symptoms of depression compared to males (Figure 1), and male first-year medical students experiencing more symptoms of depression compared to male third-year medical students (Figure 2). Of note, students in this study tended to have fewer depressive symptoms after exams as they advanced chronologically through medical school. Prior research has shown that medical students as a group tend to become more depressed as they progress 42 ; however, in the present study, depressive symptoms immediately following exams were examined, and not general depressive symptoms in medical students. Further work to investigate if there is a true difference between depressive symptoms after exams versus overall depressive symptoms is warranted.
As hypothesized, females experienced higher rates of symptoms of depression after exams compared to male medical students overall (Figure 1 and Table 3). This is similar to what has been found in the general population, where females experience more symptoms of depression and anxiety compared to males.28–30,43 However, given the stresses of medical school, and frequent high-stakes exams that are part of the medical education process in the USA, the researchers suspect that some of the factors driving the development of depressive symptoms in medical students may be different than those affecting the general population. While not the full explanation for the development of depressive symptoms in medical students, results from this pilot study show that exams could be a contributing source of such symptoms in medical students, as they are also known to contribute largely to anxiety,16,27,35,36,41 which is often linked to depression. 44 A previous study by Thiemann et al 16 showed that medical students with imminent exams were more likely to experience depression; however, symptoms were only looked at before exams and not afterward. The authors suggested that students may require more support during exam periods; that correlates well with this study's finding that students experience symptoms of depression after exams. Overall, the driver of the striking differences between male and female experiences of depression after exams is not fully understood (similar to the drivers behind symptoms in the general population); however, lack of self-esteem, imposter syndrome, or lack of female role models in medicine could be contributing factors.45–47 Further work is needed to better understand the etiology of these findings in medical students and the general population alike to find ways to alleviate these symptoms. The authors suspect that there will be overlap between many drivers of symptoms of MDD between medical students and the general population, but also suspect there to be differences given the high stakes surrounding performance-based assessments that medical students’ experience, which differs from the general population.
In addition, the current study revealed that there were fewer symptoms of depression after examinations in third-year male medical students compared to first-year male medical students. With 46.2% of first-year male medical students and 9.3% of third-year male medical students experiencing symptoms (Figure 2). This finding may be due to the placing of less emphasis or consideration on examinations in the calculation of final grades in year 3 compared to the first 2 years of medical school at the UNECOM; this finding may be school-specific, as other medical schools and other countries differ in how they weight examination scores in final grade determination across the continuum of education. Additionally, this study looked at students in the first 3 years of medical education, and not the fourth year, as medical students in the USA often do not take exams in their fourth and final year of school.
Data from this study revealed that 90.2% of student respondents felt that their chosen coping strategy after exams helped them feel less depressed. Interestingly, the 3 most common coping strategies in this study included healthy positive outlets, including using social supports, physical activity, and participating in hobbies/interests (Table 6). However, examinations in medical school are recurrent and frequent, even biweekly at times; this study found a high rate of symptoms of MDD after medical school exams, potentially putting students at repeated risk for experiencing these symptoms multiple times throughout a semester, school year, and the entire duration of medical education. Recurrent experiences of such symptoms can potentially lead to cumulative negative effects on students’ overall well-being and lead to burnout or the development of mental health pathology. Prior studies have postulated that mental health status can worsen as medical students continue through the continuum of medical education. Therefore, it is reasonable to question whether recurrent high-stakes examinations may be contributing to mental health concerns as students’ progress through their education. 48 Additionally, in light of recent COVID-19 restrictions on social gatherings, limiting students’ coping strategy of using social supports may be compounding depressive symptoms in medical students at this time.
Additionally, medical students who experience depressive symptoms are less likely to seek help, with previous research showing only 22% of students who met the criteria for MDD using the Beck depression inventory (BDI) were utilizing mental health services. 49 Another similar cross-sectional study showed that 26.5% of medical students found to meet criteria for MDD using the BDI were receiving treatment with counseling, medication therapy, or both. 45 Although the current study looked at depressive symptoms in a discrete-time point after exams and does not address whether or not the students surveyed received treatment for these symptoms, it is worth noting that, as mentioned above, medical students in general often do not receive treatment for such symptoms, and understanding factors that may contribute to such symptoms is important. The findings from this current study highlight the importance of awareness and open discussion about emotions that can be triggered by examinations, with the hope that this will encourage students to seek help early on. With the knowledge that many medical students experience depressive symptoms at some point in their training,1,8,21–23,33 incorporation of psychosocial resources or services as part of medical education may reduce the stigma of seeking help and develop a culture where mental well-being is emphasized. Students have cited “lack of time, lack of confidentiality, the stigma associated with using mental health services, cost, fear of documentation on academic record, and fear of unwanted intervention” as reasons for not seeking help 49 ; as such, medical students who experience depressive symptoms are often undertreated. Understanding the factors that contribute to such depressive symptoms, including medical school examinations, and reducing stigma around mental health, are important conversations to implement within medical schools and at the national level.
Limitations
Data presented here is limited by the number of respondents, willingness for participants to be fully honest on the survey, and the context in which these symptoms were asked (immediately postexamination). Another limitation involved the differing percentages of students from each class year, as well as between male and female participants, who answered the call to the study. A lack of preexamination data for comparison of pre- and postexamination symptoms is a limitation. It is unknown if any of the participants had prior mental health diagnoses, or if they had undergone a recent stressor outside of exams (eg, death of a loved one, breakup, accident, or disease), which could have also spurred symptoms of depression; clearly, it is difficult to account for all the various types of stressors in 1 survey. Additionally, a validated questionnaire was not used in this study, making it challenging to compare to other research. However, employing criteria for the diagnosis of MDD using the DSM-5 provides a good representation of the burden of MDD symptoms in medical students after exams. Another limitation was that the number of coping strategies assessed was limited, and included mostly avoiding strategies. Examining students from multiple medical schools, and potentially multiple countries, would better show what students experience. Despite its limitations, this study supports further research into gender and year in medical school differences in the development of depression symptoms surrounding medical school exams.
Conclusion
Female medical students experienced more symptoms of depression after exams compared to their male counterparts across the first 3 years of medical school. In addition, male first-year medical students experienced more symptoms of depression compared to male third-year medical students. Most students reported possessing coping strategies that helped them feel less depressed, yet due to recurrent testing in medical school, the cumulative effects of these symptoms on student mental health are yet to be fully understood. The data presented here warrants further studies analyzing the development of pre- and postexam symptoms of depression and how this affects medical student mental health longitudinally.
Footnotes
Acknowledgements
The authors of this manuscript would like to acknowledge Hwyda A. Arafat, MD, PhD, MSc. MedL, for her edits of this manuscript.
Authors Contributions
TJA, JM, MA, CS, and RS provided substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; all mentioned authors helped drafted the article or revised it critically for important intellectual content; all mentioned authors gave final approval of the version of the article to be published; all mentioned authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.