
Abstract
Background:
Case-based Interprofessional Education (IPE) can help students practise their roles and responsibilities. To construct these cases, input from experts in clinical practice is essential. Consensus between these experts can be facilitated using consensus methods. In this study, a geriatric focus for the cases was chosen because of the interprofessional nature of geriatrics and the ageing population in healthcare facilities.
Methods:
By combining the 3 most commonly used consensus methods, we developed a 6-step approach to validate cases for IPE. The 6 steps include 3 expert rounds (Steps 1, 3 and 5) and 2 rounds in which discussion points were formulated by the researcher (Steps 2 and 4). The cases were piloted with students as Step 6. Four facets of a case were included: the patient description, the complemented treatment plan, the difficulty of the case and the scoring of the treatment plan. Our educational setting required constructing 4 cases with increasing difficulty. Results: Step 1: 5 typical geriatric cases were assembled. Step 2: Similar characteristics were defined; 5 cases were merged into 4. The 4 cases showed increasing difficulty levels. Step 3: The constructed cases were validated for patient description authenticity, treatment plan adequacy, difficulty and scoring of the treatment plan. Step 4: The items for further discussion were defined. Step 5: Consensus was reached for all 4 cases through a face-to-face discussion. Step 6: The student pilot for Case 1 showed no significant adjustments.
Conclusion:
We developed a 6-step consensus method to validate cases for IPE, and we constructed 4 geriatric cases based on this method. While consensus about the patient descriptions and difficulty levels was reached easily, consensus on the treatment plans was more difficult to achieve. Validation of the scoring of the treatment plan was unsuccessful. Further research on this will be conducted.
Background
Based on the premise that Interprofessional Education (IPE) improves Interprofessional Collaboration (IPC) in healthcare practice, numerous interprofessional initiatives have been established in healthcare centres and educational facilities around the world.1-3 The World Health Organisation emphasises the importance of IPE and IPC and formulates the following definitions 4 :
- ‘Interprofessional education occurs when 2 or more professions learn about, from and with each other to enable effective collaboration and improve health outcomes’.
- ‘Collaborative practice in healthcare occurs when multiple health workers from different professional backgrounds provide comprehensive services by working with patients, their families, carers and communities to deliver the highest quality of care across settings’.
IPE can be offered in different settings. An obvious setting is the so called ‘IP training ward’, where students can collaboratively perform actual patient care. Although an IP training ward may seem ideal, it is often a logistical challenge.1,2 This can result in students participating in the ward for too short a time for the training to be effective; moreover, training in this ward is time-consuming for the trainers involved. 2 Considering that students’ attitudes towards each other and their collaborative knowledge and skills improve after experiencing IPE, initiatives on IPE that occur in the classroom or simulation settings have a place in health professions’ curricula today.3,5,6 Combining several types of IPE initiatives makes IPE practices sustainable. 7 To prepare students for IPC, IPE can be offered in a classroom setting with the use of constructed cases. 8
Using cases in this way has several advantages: it can help students practise their professional roles and responsibilities, it can facilitate clinical reasoning, and case-based education is effective for students working in pairs.9-12 These can be valuable because understanding one’s own and each other’s roles is the most important aspect of effective IPE. 3
When using cases, it is essential that they are realistic.3,9 However, actual cases from clinical practice often need to be altered before applying them in an educational setting or IPE because they need to: (1) meet a particular level of competence for each group, (2) simulate a clinical setting, where students of specific professions can play their own role and (3) demand the use of interprofessional collaborative competencies.9,13 While a few articles have described tips for constructing cases, there is a lack of literature on how to construct cases using scientifically proved methods.13,14 Moreover, there is no literature on how to construct cases for IPE.
To determine the content of a constructed case, for example the symptoms, medical problems or social circumstances often seen in clinical practice, it is essential to consult with experts. However, the involvement of several experts can make it difficult to reach consensus about the content of the cases. 15 Consensus methods can facilitate this process.
The 3 most commonly used consensus methods are: the Delphi Technique (DT), the Nominal Group Process (NGP) and the Consensus Development Panel (CDP). 16 These 3 methods have different characteristics, which are explained in Table 1. DT is widely used for reaching consensus among the opinions of different experts. 17 The data are collected using a series of questionnaires, which are sent to a selected group of experts. NGP is a consensus method based on a face-to-face meeting with the experts involved. 18 During the face-to-face meeting, experts can discuss each other’s ideas about 1 or more problems. CDP is also based on face-to-face interaction; it was developed by the National Institutes of Health to formulate guidelines and statements. This technique allows a multidisciplinary approach of different experts; therefore, it can be useful in healthcare policy making. 16
Aspects of the different consensus methods.

Abbreviations: DT, Delphi Technique; NGP, Nominal Group Process; CDP, Consensus Development Panel.
In a comparative study, Waggoner et al found that none of these methods is preferred over the other; they summarised the characteristics of the different methods by reviewing the current literature. 16 Table 1 presents an overview of the different aspects of the 3 methods. 16
The objective of the present study was to use consensus methods to construct and validate patient cases that are suitable for IPE in undergraduate nursing and medical education.
We chose a geriatric focus for our cases because of the different professions involved in caring for geriatric patients. IPC between these different stakeholders is important for adhering to a good standard for the quality of care. 19 Furthermore while there has been a substantial increase in the number of elderly patients in the countries in northern and western Europe, few medical students are interested in working with these patients. 20 It has been reported that geriatric IPE programs help motivate students to work with geriatric patients, since students are able to expand their knowledge, and deliberate with each other about geriatric problems. 21
Methods
The 6 steps based on the consensus methods
To reach consensus about and validate the content of the cases, we used a combination of the 3 consensus methods. We did this because none of the methods covered all the aspects that are relevant to the construction of cases. We chose the best aspects and the aspects that are most applicable to this research topic. Table 2 provides justification for these different aspects, and how and why they were implemented in our study.
Justification for the different consensus methods and an explanation for their application in this research study.

Abbreviations: DT, Delphi Technique; NGP, Nominal Group Process; CDP, Consensus Development Panel.
The cases and setting
In our setting it was logistically easy to include medical and nursing students, so we focused on these 2 groups in this study. In future studies, other professions, for example, physical therapy and social work, can be included following the same methodology. We constructed 4 cases to be used in our nursing and medical curriculum in a classroom setting, during a 1-year training period. Since skills and knowledge increase over time, the 4 cases needed to have different levels of difficulty. To determine on which prior knowledge and competencies the cases could be built on, we consulted nursing and medical educators on the geriatric content of both curricula. The problems that were discussed needed to be recognisable and frequently occur in clinical practice. For each case, the students worked in pairs of medical students and nursing students to develop treatment plans. The students’ treatment plans were assessed by comparing them to a standard validated treatment plan formulated by the experts.
Figure 1 presents an impression of the items that needed to be validated for each case. In the 6 steps, we validated:
- The content of the cases (patient description and treatment plan);
- The scoring (difficulty and scoring of treatment plan).

Visual impression of a case.
Integral, interdisciplinary and medical (INTERMED) for the elderly
To define the difficulty of each case, in the first round we asked the experts: What makes a case like this (not) difficult? We compared their responses with the information in the literature about the tools that measure case complexity, especially in geriatric patients. We found that INTERMED for the elderly best resembles the items named by the experts.
INTERMED was developed originally to facilitate the description of case complexity for clinical and educational purposes. 22 Wild et al stated that INTERMED for the elderly could be used to identify elderly patients in need of interdisciplinary care. 23 The validity of the constructed cases is unknown. INTERMED delineates caring needs into 4 domains: biological, psychological, social and healthcare. Each domain has a maximum total score of 15. These 4 domains are structured based on time: history, current state and prognosis. The INTERMED for the elderly score ranges from 0 (not complex patients) to 60 (very complex patients).
Based on the aspects presented in Table 2, we formulated 6 steps (Figure 2):
- Three expert rounds (Steps 1, 3 and 5);
- In between, the information is summarised by the researcher (Steps 2 and 4);
- We added a pilot testing with students to assess the constructed cases (Step 6).
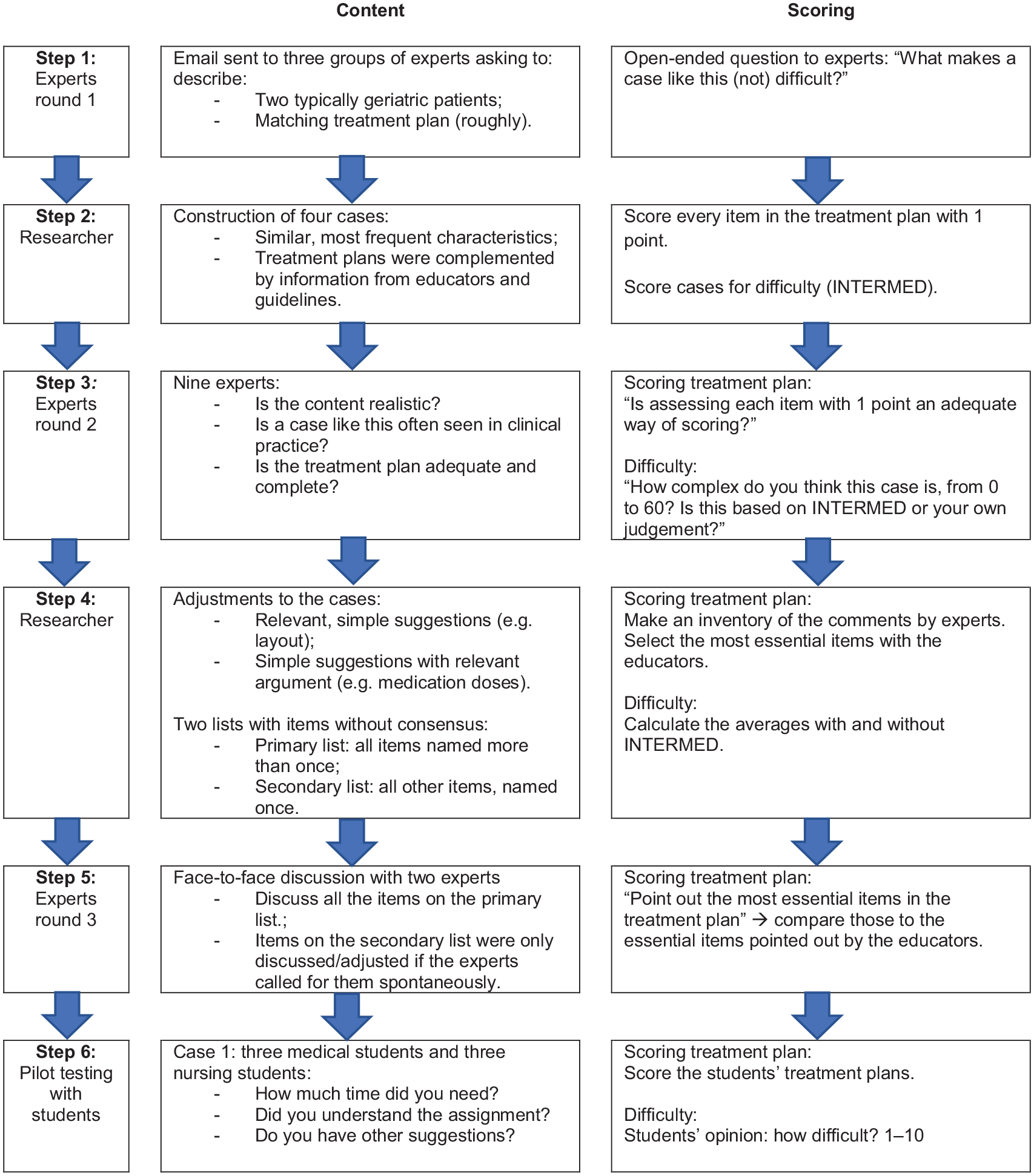
Description of the 6 steps for validation of content and scoring of each case.
Figure 2 shows what we did in each step to validate the content and scoring of each case.
Results
Using the 6 steps, we constructed and validated the content and scoring of the 4 cases. Consensus was achieved after Step 5. The results of each step are specified in Figure 3.

The results of each step.
Discussion
We developed a 6-step process to create geriatric cases that can be used for classroom IPE. The 6 steps are based on the characteristics of 3 consensus methods (DT, NGP and CDP), so the content of the cases could be validated. We chose a geriatric focus and an interprofessional setting, but the 6 steps can also be used in a variety of other settings.
When conducting this research study, we experienced some difficulties. First, the process was time-consuming, especially for the coordinator, that is, the researcher. However, we see this as a 1-time investment. A constructed case can be re-used in an educational setting for many years. Furthermore, this approach involved minimum effort from the experts, so they were willing to participate. In the last round, both the medical resident and the nurse reported that they found that reviewing the cases was ‘a nice thing to do, because they did it together’. During the validation process, an online questionnaire for experts can result in further distributing the workload, but that will need to be developed.
Secondly, the consensus process for the case content was also difficult. The results indicate that experts may easily agree upon the content of frequently seen cases. In Step 1, several of the characteristics were similar. In Steps 3 and 5, there were a few items that needed to be discussed. There was a lot more diversity in the experts’ opinions of the treatment plans. Almost every expert in Step 3 had a unique opinion about the items that should be included in the treatment plans, for example, whether or not to consult an occupational therapist or to order a chest X-ray. The number of ‘secondary items’ in Step 4 demonstrates this diversity: 45 about the treatment plan versus 3 about the content.
It was possible to score the case complexity using INTERMED for the elderly. All the experts in clinical practice scored the cases similarly. Differences were seen by the experts that scored the complexity using their own judgment, not INTERMED. Case 1 was estimated to be more difficult and Case 4 was estimated to be less difficult when INTERMED was not used in comparison to when it was used. It is possible that the experts focused on the diagnosing dilemma more heavily than when using INTERMED. For example, in Case 1, the symptoms were vague, which can make diagnosing more difficult; therefore, difficulty of Case 1 was rated higher when experts used their own judgement instead of INTERMED. In contrast, in Case 4, there was a clear description and no diagnosing dilemma, but the background, comorbidity and severity of the symptoms made it complex. This case was rated less difficult by experts’ own judgements. The literature confirms the biopsychosocial strength of the INTERMED: it focuses on social and psychological problems as much as on diagnosing dilemmas. 23 Scoring based on the experts’ own judgment has not been validated in previous research. The increasing difficulty of the INTERMED scores of the 4 cases is of specific relevance to our study. The difficulty the students reported was not consistent with their performance. This could possibly be explained by the fact that the students could not grasp the complexity of the case.
The most important limitation of this study is the unsuccessful validation of the treatment plan as an assessment tool. We found discrepancies between what clinical experts versus educational experts found to be ‘essential’. The clinicians’ vision was often unrealistic for the students’ capabilities. For example, a clinical expert can insist that all geriatric laboratory examination is essential, but if students have not been taught this in their knowledge classes, we cannot expect them to include it in their treatment plans. One expert commented on the format of handling all the items of the treatment plan simultaneously. In clinical practice, some diagnostic research depends on previous test results. This is a valid statement. Consequently, we tried to include only primary items. It was possible to score the treatment plans of the students and collect a range of scores; however, further validation of the scoring system is necessary and will be continued. Other limitations of this study are that we had a geriatric focus and only nursing and medical students were involved. A different focus and involving more disciplines could require a validation process with more experts and/or more steps. The validation of the 6 steps in different settings should be studied further. Finally, due to time constraints, our student pilot testing was conducted with individual students and only for Case 1. Our research will proceed with a pilot study with all 4 cases and with interprofessional pairs of medical and nursing students. A study investigating the influence of IPE with cases on non-structured workplace learning will also be conducted.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Authors’ contributions
CT conducted the research, collected the data, ordered the data, formulated the 6 steps, framed the topic in known literature and theory and wrote the article. RK contributed to the design of the work (eg, how and which experts to approach), the analysis and interpretation of the data related to the known literature, and made adjustments according to that knowledge. HS contributed to the design of the work (eg, how and which experts to approach, which questions to formulate) and how to order data, the analysis and how to present the data. HD contributed to the analysis and interpretation of the data and how and which points to formulate for the discussion. SP contributed to the design of the work (eg, how to design the 6 steps, which experts to approach), the analysis and interpretation of the data. All authors read, corrected and made suggestions on several versions of the article. All authors state that all questions about accuracy and integrity are appropriately resolved and give their final approval of the version to be published.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.