
Abstract
Purpose:
The aging population in the United States poses a substantial challenge to our health care system, and particularly affects the training of physicians in geriatric care. To introduce undergraduate medical students to a variety of clinical skills and concepts emphasized in geriatrics, we created an interprofessional geriatric workshop and examined changes in student perceptions of working in interprofessional teams, knowledge regarding geriatric concepts, perceptions of the pre-work material, and suggestions for curricular improvement to enhance the workshop for future students.
Methods:
Second-year medical students participated in a 4-hour workshop with tasks that emphasized activities of daily living, geriatric physical assessment, end-of-life discussions, Beers Criteria, and a home health assessment. Pre- and post-surveys were administered including the Students Perceptions of Interprofessional Clinical Education–Revised (SPICE-R) survey and a knowledge assessment. Student perceptions of pre-work and overall program assessment were captured after the workshop. Descriptive statistics and paired t tests assessed for significant differences. Emerging themes were analyzed using the Glaser constant comparative method.
Results:
Of the 186 medical student participants, 178 students completed the SPICE-R survey, demonstrating significant increases in students’ perceptions of the value of interprofessional education (P < .001). In addition, 111 students completed the pre- and post-test for the knowledge assessment, demonstrating significant gains in geriatric concepts (P < .001). Overall, most students perceived the pre-work as useful and felt prepared to evaluate geriatric patients. Open-ended question analysis supported results, in which 34 students indicated that they felt most comfortable performing a home health assessment and emphasized the usage of the home health simulation.
Conclusions:
Introducing medical students to a variety of geriatric assessments and concepts in an interprofessional environment early in their career positively influences their perceptions of working as an interprofessional team member to deliver comprehensive care to older adults.
Introduction
Many have recognized the critical need for increasing the number of geriatricians in the United States, especially considering that there were 37.8 million older adults in 2017, and by 2060, the number of older adults is projected to be over 94 million.1,2 As of 2017, there were 7279 certified geriatricians and only half are practicing full-time in the United States. 3 Although pursuing certification as a geriatrician follows an internal or family medicine residency, it is imperative that we ensure that medical students receive exposure to the complexities of health care delivery to older adults. As emphasized recently by Flaherty and Bartels, 4 our primary care workforce requires increased attention to geriatric training to improve care for older adults. Such experiences will not only increase interest toward the field but also prepare all medical students regardless of their specialty as most will care for an older adult.
In addition, the Association of American Medical Colleges (AAMC) has endorsed the minimum geriatric competencies for medical students, which include the ability to manage medications, develop a self-capacity management plan evaluating functional abilities, assess safety risks in home environment, and conduct gait assessments. 5 Recent literature has discussed the inclusion of home evaluations, simulation cases, and real-life patient encounters during the clerkship years of medical school (third and fourth year) or residency as means to meet the geriatric assessment standards outlined by AAMC.6-11 Although several studies have described activities and indicated improvements in students’ perceptions of the geriatric population, many have occurred outside the United States12-15; thus, comprehensive, geriatric workshops have not been emphasized or evaluated in medical students during pre-clerkship years.
In addition, interprofessional teamwork is essential for patient-centered care in older adults. The World Health Organization has emphasized the significance of training professionals in health care, stating that “[i]nterprofessional education occurs when students from 2 or more professions learn about, from and with each other to enable effective collaboration and improve health outcomes.” 16 Complex medication regimens, referrals to physical therapy, occupational therapy or other specialties, and in-home nursing in older adults have required the need for professionals across the spectrum of health care to improve patient outcomes. Recently, calls for expanded interprofessional opportunities to train the next generation of health care providers has been emphasized for the geriatric population. 4
As such, our objective of this study was to introduce and apply geriatric care competencies by designing and evaluating an interprofessional workshop as part of the Physical Diagnosis course curriculum for second-year medical (M2) students. Our primary aim evaluated M2 students’ perceptions of interprofessional team interactions before and after a 4-hour geriatric workshop. Secondary outcomes included medical students’ knowledge of geriatric topics, perceptions of self-confidence regarding geriatric patient assessment, drug-related problems, and students’ evaluations of the pre-work content.
Methods
Study design
Our study involved a pre- and post-study design with data initially gathered for curriculum evaluation. Data from M2 student participants were collected through a series of survey instruments and activity worksheets. Data from fourth-year pharmacy (P4) students were not collected for 2 reasons: (1) the pharmacy students were invited as guests from another university system and (2) all data were gathered as a component of curriculum evaluation of the medical students for our required Physical Diagnosis course.
Setting
Second-year medical students at the Medical College of Georgia (MCG) and P4 students from the University of Georgia (UGA) attended and participated in a geriatric workshop in the Spring 2019 that was embedded in the medical curriculum Physical Diagnosis course. As aforementioned, this a required course that takes place in the first and second year of medical school and is designed to teach medical students the fundamentals of taking a comprehensive medical history and performing an accurate and comprehensive/focused physical examination, discussing the differential diagnoses and formulating a management plan. Students are oriented to upcoming sessions using flipped classroom methods, in which students have access to online material before each session to prepare adequately as a means to apply acquired knowledge and skills in a simulated environment. This study’s intervention is the first exposure to geriatric patient care in the pre-clerkship curriculum for medical students at MCG. Fourth-year pharmacy students have taken a similar applications-based course, occurring in years 1 and 2 of UGA’s College of Pharmacy curriculum and been familiarized with polypharmacy, geriatric pharmacokinetics/pharmacodynamics, and the Beers Criteria.
Participants and eligibility criteria
All M2 students (N = 186) at MCG were eligible and required to participate in the geriatric workshop as a requirement for the Physical Diagnosis course. Pre- and post-session evaluations and surveys were voluntary for M2 students to complete. Pharmacy students were eligible to participate in the geriatric workshop if they were P4 students on rotation at the Augusta UGA campus. Fourth-year pharmacy students were not eligible to complete the pre- and post-session surveys due to their status as UGA students.
Procedure
In total, 186 M2 students participated in the geriatric workshop over a 4-day period. Students were divided into 6 groups each day, and the groups were named after one of the Activities of Daily Living (ADLs). Due to the limited number of P4 students who participated (n = 4), 1 group from each day was assigned a P4 student for all the workshop activities. For purposes of analyses, 32 M2 students experienced the workshop activities with a P4 student (interprofessional group), and 154 M2 students experienced the workshop activities without a P4 student (non-interprofessional group). On average, there were approximately 8 students per group.
Intervention
Similar to other sessions in the Physical Diagnosis course, students accessed pre-work resources including 2 videos demonstrating the Timed Up & Go (TUG) test and end-of-life discussion as well as handouts explaining the Montreal Cognitive Assessment (MoCA), the Mini-Mental State Examination (MMSE), and Beers Criteria, and the Home Health CDC (Centers for Disease Control and Prevention) booklet.17-20
Table 1 provides details regarding the 6 activities and respective learning objectives. The first activity involved an interactive video with a student-driven game, with the goal to introduce and understand the concept of functional assessment. The video incorporated a standardized patient performing the 6 ADLs: eating, bathing, dressing, toileting, transferring, and hygiene. 21 After each ADL presented in the video, the video was paused and student groups competed to identify the appropriate assistance equipment the patient could use. The second activity centered on a geriatric assessment, in which a geriatrician guided the students through the basics of how to perform a TUG test and MoCA test on a live geriatric patient. Next, students witnessed a live end-of-life discussion between the geriatrician and geriatric patient. The concepts of Beers Criteria, anticholinergic effects, and polypharmacy were emphasized with the students by discussing 3 clinical vignettes as an entire class, then breaking down into smaller groups to evaluate simulated cases within an educational electronic health record. For the latter activity, several groups teamed up with a pharmacy student to discuss the medication management of their respective simulated cases. Groups without a pharmacy student had the opportunity to request a clinical consult from a PharmD faculty member. The final activity involved a home assessment for safety risk in a simulation room, which was outfitted with several dozen possible risks. Student groups were tasked with identifying risks in a small apartment that included a living room area, kitchen, and bedroom.
Description of activities and learning objectives.

Abbreviation: ADLs, activities of daily living.
Run simultaneously.
A board-certified geriatrician led the first 3 activities of the workshop, the pharmacy-related activities were led and facilitated by a registered pharmacist, and the final activity was facilitated by the aforementioned geriatrician and an internal medicine physician for the remainder of the workshop (Table 1).
Instruments
Students’ perceptions of interprofessional team-based care were assessed using the validated Students Perceptions of Interprofessional Clinical Education–Revised (SPICE-R) instrument. 17 The SPICE-R is a 10-item instrument that assesses interprofessional teamwork (6 items), the roles and responsibilities of health care disciplines (2 items), and patient outcomes due to collaborative practices (2 items) using a 5-point Likert-type scale (1, strongly disagree and 5, strongly agree). 17 All instruments measuring secondary outcomes were developed by the authors. Items were finalized through consensus among W.J.-R., S.P.B., and N.R.-W., and peer-reviewed by a member of our Educational Innovation Institute (E.A.W.) for accuracy and appropriateness. Second-year medical student knowledge was assessed using the pre- and post-workshop test consisting of 8 single-correct, multiple-choice questions evaluating 4 areas of content: transitions of care, geriatric pathophysiology, Beers Criteria, and end-of-life discussions. During the session, student groups were also asked to identify drug-related problems and recommend changes for geriatric patient cases, which were collected and evaluated for accuracy. And finally, on the post-survey, the M2 students evaluated pre-work online content (3, very useful, 1, not useful), perceptions of their abilities (4, strongly agree, 1, strongly disagree) and overall satisfaction with the workshop. The pre- and post-workshop knowledge assessment and post-workshop evaluation responses were captured using the Qualtrics platform, while the SPICE-R pre- and post-workshop responses were distributed via paper before and after the workshop and responses were transcribed into SPSS v25.
Statistics
Descriptive statistics were used to describe means and respective standard deviations for primary and secondary outcomes. Paired t tests were used to evaluate pre- and post-study data collected from the SPICE-R instrument and the knowledge assessment. Differences between groups with a pharmacy student regarding SPICE-R data and correctly identifying drug-related problems were calculated using the Welch t test of unequal variance due to sample size variation. A P value <.05 was considered statistically significant. The effect size for SPICE-R was calculated as the mean difference divided by the standard deviation of the differences (Cohen d). All analyses were calculated using SPSS Version 25 (IBM Corp. Armonk, NY). Themes from open-ended questions were developed using the Glaser 22 constant comparative method.
Ethical issues
This study was approved by Augusta University Institutional Review Board. Data were collected as a component of regular curriculum evaluations, and M2 students submitted all data voluntarily. Anonymity of the data were maintained through de-identification and stored over a secure server.
Results
For the SPICE-R survey (Table 2), 178 students submitted completed results, and post-session scores demonstrated a significant (P < .001) increase in M2 students’ perceptions of the value of interprofessional education (pre-session, 4.05 vs post-session, 4.25). In addition, each element within the SPICE-R survey demonstrated significant increases across all medical students, and the statement regarding the roles of health professionals within a team increased the most overall (0.5 increase). Although the differences between these 2 groups were significant, the effect size was small to medium (Cohen d = 0.43). The difference between groups with a pharmacy student (pre-test mean = 4, SD = 0.51; post-test mean = 4.34, SD = 0.48) trended toward significance (P = .08). On the contrary, interprofessional groups identified and recommended significantly more drug-related problems in the patient cases, identifying an average of 8.7 correct drug-related problems as compared with 4.1 in groups that did not include a pharmacy student (P < .001).
SPICE-R results (n = 178).
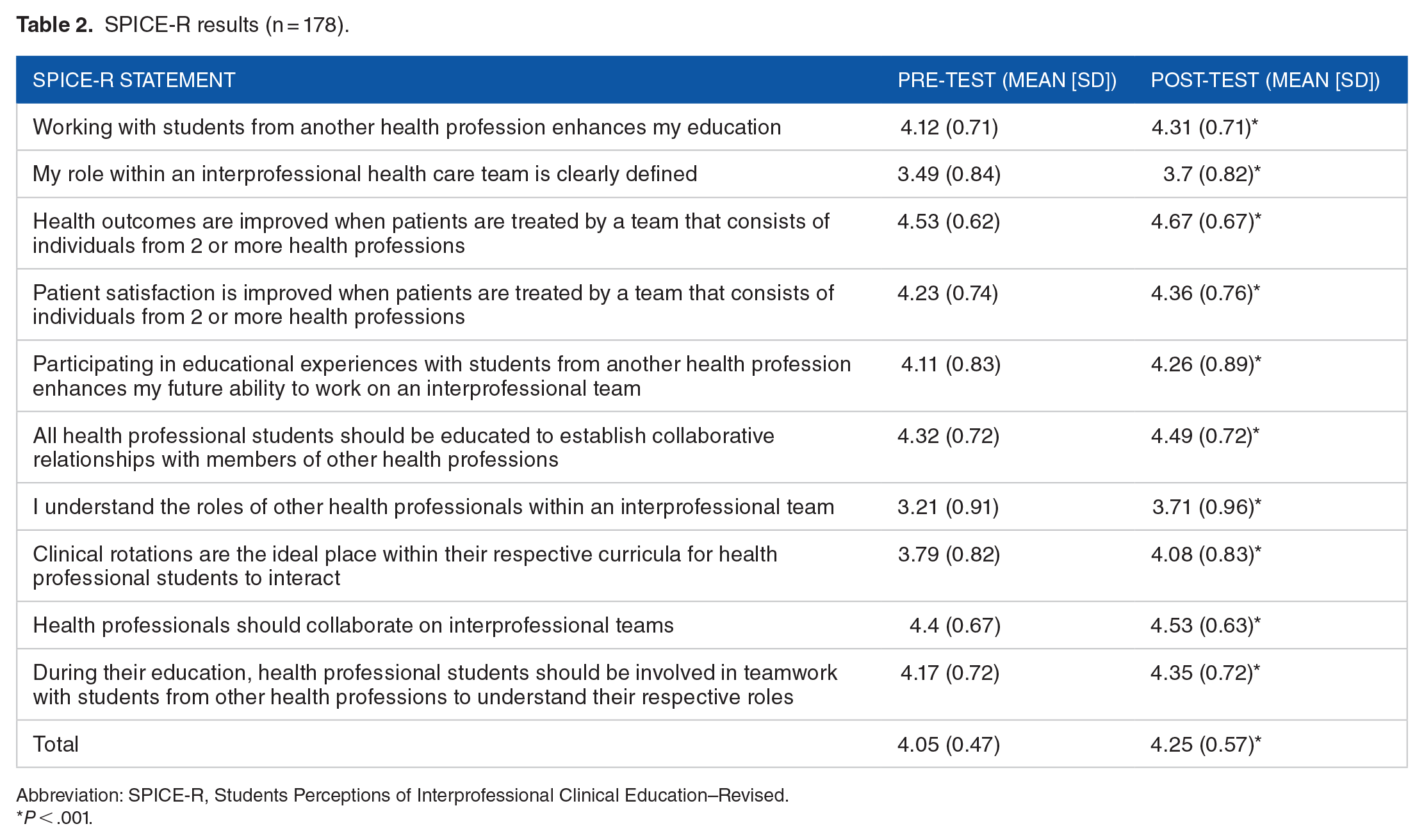
Abbreviation: SPICE-R, Students Perceptions of Interprofessional Clinical Education–Revised.
P < .001.
In total, 111 (60% response rate) students completed both the pre- and post-test knowledge assessment. Post-test results demonstrated a statistically significant (P < .001) improvement compared with pre-test scores, as illustrated in Table 3 (71% correct vs 68% correct, respectively). Questions related to the topic to the Beers Criteria demonstrated the most significant gains (pre-test 0.62 vs post-test 0.66, P < .001).
Geriatric knowledge assessment (n = 111).

P < .001.
Overall, most students reviewed pre-work material and perceived the content as useful, as demonstrated in Table 4. Of those who viewed the Beers Criteria guidelines, they felt this resource as the most useful for the activities. After the session, students felt prepared to perform a variety of geriatric assessments and evaluations and indicated they felt most comfortable performing a home health visit (Table 5). This was reflected in our open-ended question analysis, in which 34 students indicated how the home health visit simulation was very useful and well received.
Use and value of pre-work material (n = 111).

Students’ perceptions of abilities (n = 111).

Discussion
To our knowledge, this research study is the first to design and evaluate an interprofessional geriatric workshop in pre-clerkship medical students that integrated pharmacy concepts, including the Beers Criteria. As the literature has indicated, an interprofessional team approach is crucial for patient-centered care that provides continuity throughout the stages of aging. Providing the opportunity to pre-clerkship medical students to experience the merits and value of other health professions, and in the case of our study, pharmacy students, will train students to seek out these professionals in such settings. Our study demonstrates an increase in geriatrics knowledge and efficiency in identifying drug-related problems in older adults. In addition, M2 students perceived themselves as having effective skills to perform an initial evaluation, functional assessment, lead an end-of-life discussion, and perform a home health visit for older adult patients. Despite having a high baseline value, our study demonstrated an increase of interprofessional skills. We expected our students to score relatively high at baseline regarding interprofessional education due to previous sessions with dental students and prior volunteering experiences with interprofessional student-led clinics.
Our findings build on previous work that has demonstrated improvements in knowledge, clinical skills, and empathy among undergraduate and graduate medical trainees.6-15 In particular, studies designed to evaluate the perceptions of medical and pharmacy students have demonstrated a positive influence of interprofessional activities with respect to geriatric medicine. Shrader et al 23 described an in-home interview and medication history activity with local volunteers, in which students were assessed on attitudes toward other health professionals before and after the experience, demonstrating gains in the importance in collaboration. The impetus for medical students to understand the complexities of geriatric patients, especially medication management, is crucial, particularly because a recent systematic review revealed a median of only 2 hours dedicated to geriatric pharmacology and a lack of overall effectiveness in medical schools. 24 With respect to pharmacy education literature, studies have similarly reported increases in knowledge and positive attitudes toward geriatric patients after interprofessional experiences, and programs here in the United States and abroad have indicated that geriatric topics are included across the curriculum.25-27
As the population of the United States continues to age and life expectancy increases, introducing clinical skills crucial for caring for geriatric patients early in the career trajectory of medical students is essential in influencing their future professional tracks. Providing opportunities to medical students to develop these critical skills should translate not only into trainees excelling in residency competencies but also positively influence their future expertise. End-of-life discussions (advance directives), medication management, and maintaining collaborative interprofessional relationships are foundational for all medical specialties. Based on our experience, the team should include 1 pharmacist, 1 geriatrician, and 1 or more internists to run the hands-on experience successfully. In addition, collecting pre- and post-study data should be distributed among in-class (SPICE-R and drug-related problem identification) and outside of the workshop (knowledge assessment, workshop evaluation).
Although this study demonstrated significant differences in knowledge and attitude toward interprofessional education, there are several limitations. The study did not include evaluation of attitudes toward geriatric patients. Furthermore, we had planned to include more pharmacy students but due to scheduling changes, not all groups were able to collaborate with pharmacy students. In addition, post-evaluations survey response rate was 60% as these were sent out by email and were not mandatory. Thus, our results should be interpreted with caution as students who have favorable perceptions of geriatric medicine may have been more likely to answer the post evaluations and our effect size was small to medium (Cohen d = 0.43). In addition, limitations of our study include evaluating 1 academic year of M2 students at a single institution, which limits the generalizability. Although we had hoped to include other health professions, scheduling conflicts limited our Spring 2019 session to pharmacy students. As such, we have planned a revised geriatric session, incorporating occupational and physical therapy students, and will increase the number of pharmacy students who will be involved. This upcoming session will also be designed and led by the faculty from the various professions to improve understanding of the roles of different health care professions. Upcoming future sessions will evaluate attitudes toward geriatric patients and empathy through hands-on clinical stations.
Conclusions
Our findings demonstrate that a workshop integrating activities that encompass geriatric care results in significant improvement in perceptions of the value of interprofessional education and knowledge, perceptions, and confidence in performing geriatric assessments.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
WJ-R, SPB, EAW, and NR-W contributed to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript.