
Abstract
Background:
Formal goal-setting has been shown to enhance performance and improve educational experiences. We initiated a standardized goal-setting intervention for all residents rotating through a Geriatric Medicine rotation.
Objectives:
This study aims to describe the feasibility of a goal-setting intervention on a geriatric medicine rotation, the resources required, and the barriers to implementation. As well, this study aims to describe the learning goals residents created regarding content and quality.
Methods:
A pilot goal-setting intervention was initiated. A goal-setting form was provided at the beginning of their rotation and reviewed at the end of the rotation. Residents were invited to complete an anonymous online survey to gather feedback on the initiative. Goals were analysed for content and quality. Feedback from the survey results was incorporated into the goal-setting process.
Results:
Between March and December 2018, 26 of 44 residents completed the goal-setting initiative. Explanations for the poor adherence included limited protected time for faculty and residents to engage in coaching, its voluntary nature, and trainee absence during orientation. Reasons for difficulty in achieving goals included lack of faculty and trainee time and difficulty assisting residents in achieving goals when no clinical opportunities arose. Although only 59% of residents completed the intervention, if goal-setting took place, most of the goals were specific (71 of 77; 92%) and 35 of 77 (45.5%) goals were not related to medical knowledge.
Conclusions:
This pilot study outlines the successes and barriers of a brief goal-setting intervention during a Geriatric Medicine rotation. Adherence was limited; however, of those who did complete the intervention, the creation of specific goals with a short, structured goal-setting form was possible. To enhance the intervention, goal-setting form completion should be enforced and efforts should be made to engage in mid-rotation check-ins and coaching.
Keywords
Introduction
All postgraduate medical education (PGME) programmes across Canada have been mandated to deliver Competency Based Medical Education (CMBE) curricula. Tools that enhance this curriculum structure will allow for successful transitions to CMBE. 1 Goal-setting may serve as a useful tool in a CMBE, given that goal-setting improves performance in various settings and stimulates collaboration between clinician teachers and learners.2-4
Goal-setting has been applied and evaluated in many ways in undergraduate medical education (UGME). When medical students were provided a brief introduction on goal-setting, they demonstrated improved ability to set goals, and, in addition, their goals were more specific, attainable, and relevant. 5 In other studies, goal-setting led to improved behavioural change, patient counselling, better adjusted standardized test scores, higher rotation satisfaction, greater tendency towards self-directed learning, and altering learning habits to address skill deficicies.4,6,7 In surgical residents, performance on simulation tasks improved in those randomized to the goal-setting group. 8 Most of the reports on goal-setting in PGME for post-medical degree residents in non-surgical settings have involved paediatric residents or involved goal-setting as a component of a coordinated educational intervention such as resilience training.9,10 The limited PGME literature suggests that goal-setting interventions improve goal-setting skills and that resident physicians value the experience.11-13
To our knowledge, no studies have reported on a goal-setting intervention for resident physicians rotating through Geriatric Medicine. Here we describe our experience to date with a pilot goal-setting initiative on a Geriatric Medicine rotation. The objectives of this study are to discuss the feasibility, barriers, and successes of this pilot intervention, examine the content and quality of goals selected by resident physicians, and describe trainee perceptions of a goal-setting process on a Geriatric Medicine rotation.
Methods
This educational intervention is still ongoing and this study reports on our initial findings from the pilot phase. Since March 2018, all residents rotating through Geriatric Medicine at Sunnybrook Health Sciences Centre (SHSC), Toronto, receive goal-setting sessions and are asked to complete a standard goal-setting form (Appendix 1). The goal-setting form takes approximately 10 minutes for residents to complete and 10 minutes for the faculty to review. Although other studies report on more longitudinal (often annually) goal-setting interventions, given the lack of longitudinal coaching in the pre-CMBE curriculum, at this point goals have been restricted to the 1-month rotation. 14
Residents are encouraged to create 3 learning goals personal to them. This number of goals was felt to be a manageable time commitment and is the number of goals that other interventions have used. To assist in the development of actionable learning goals, a structured process is recommended. 15 Thus, residents are instructed to follow the SMART (Specific, Measurable, Accountable, Realistic, and Timely) goals framework when setting learning goals.15,16 Residents are also asked to outline a process to achieve their end goal. Residents select CanMEDS roles, the Canadian framework of physician abilities, related to the goal. 17 Goal-setting sessions are initiated by D.G., the education director for Geriatric Medicine at SHSC. Following the rotation, residents are invited via a secure email account to complete an anonymous online survey (Appendix 2) to gather information on how they perceived the goal-setting initiative.
For this study, 2 reviewers (J.A., E.C.) independently reviewed all goal-setting sheets to date. Goal quality was categorized as specific or general. Based on the I-SMART criteria proposed by Reed et al, 16 a goal was specific if the resident clearly outlined terms of their statement and provided a specific topic. Goals were also assessed for the presence of process goals. Process goals were considered present if the resident broke down their goal into steps and outlined a realistic plan to attain the goal while on the rotation. 16 The reviewers also coded the general content topic of the goals and whether medical knowledge versus non-knowledge goals were identified. A comparison was made and disagreements were solved through discussion between the 2 reviewers. In case of disagreement, a third reviewer (D.G.) would decide the final input. This study received Research Ethics Board approval.
Results
Over a 12-month period (March 2018 to February 2019), 26 of 44 (59%) residents completed the goal-setting form. There were 19 internal medicine trainees and 5 Geriatric Medicine trainees; 2 residents did not disclose their training level.
Feasibility
Only 26 of 44 (59%) residents completed the intervention. Reasons for poor adherence include the voluntary nature of the intervention, other competing priorities for trainee time, lack of a reminder system for form completion, and lack of administrative support to follow-up with form completion. Another reason for poor adherence is the high frequency of residents missing the orientation session when the form was provided. Reasons for missing the orientation session vary, but include vacation, post-call days, conferences, and sick days.
The structured goal-setting process was not too onerous. It was feasible to distribute structured goal-setting forms with an orientation package. Administrative support required was minimal; however, in the future, a tracking progress for form completion should be undertaken.
Goal content and quality
Overall, 71 of 77 goals created were specific (92%) (Table 1). Of 77 goals, 65 provided a process for achieving the goal (84%) (Figure 1). The top 3 content themes were (1) Delirium (n = 15), (2) Community Resources (n = 13), and (3) Prescribing and Pharmacology (n = 11). Non-medical knowledge goals were relatively common (35/77 [45.5%]). For example, many residents identified improving counselling skills, goals-of-care conversations, and interprofessional collaboration as goals. Several goals outlined an overlap between Geriatric Medicine and other specialties, such as learning about the management of rheumatological conditions in frail older adults. Residents identified a variety of CanMEDS criteria, which were Medical Expert (35), Communicator (29), Health Advocate (24), Scholar (21), Collaborator (19), Professional (13), and Leader (10).
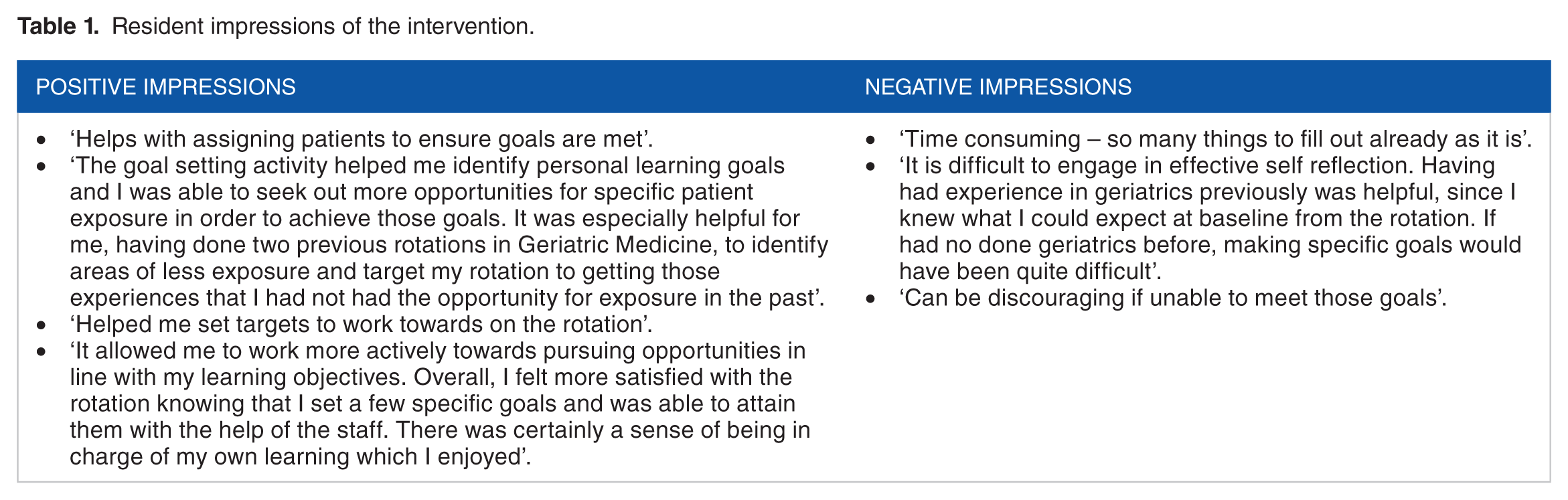
Resident impressions of the intervention.

Percent of goals that were specific and that had a process goals identified
Goal-setting resident experience
Of the 26 residents completing the goal-setting form, 8 of 26 completed the online survey. Of the 8, 4 (50%) felt the goal-setting initiative increased the value of the rotation (Figure 1). Three had used goal-setting in previous rotations, and 6 thought goal-setting should be incorporated in all rotations. Only 2 said they were likely to incorporate into other rotations if it were not required (Figure 2).

The perceived value of the goal-setting intervention
Resident feedback
Residents who believed the goal-setting intervention added value commented that the goals helped identify learning goals, tailored resources, and assignment of patients, improved satisfaction with the rotation, and allowed them to be in charge of their own learning. One commented that it was time-consuming and another highlighted difficulty engaging in self-reflection. One resident was discouraged by unattained goals (Table 1).
Six residents provided insights to improve the process. This included providing more examples (2), completing the goal-setting form prior to the rotation (2), having a coaching session around goals (1) and reviewing the goals midway through the rotation (1).
Improvements to process
During the pilot period, several improvements were made. Originally, residents were only provided the form in hard-copy version during the orientation session. Due to low adherence and survey feedback, we developed an electronic version that was provided prior to the rotation orientation. This may improve adherence for those missing the orientation session and allows time for trainees to review goals with the faculty during the orientation session. It also limits timely steps that might be barriers to form completion such as needing to remember to return or scan-in the hard-copy form.
This electronic version is sent a week prior to the rotation with enhanced instructions and examples. It has also been modified to better fit a goal-quality rubric. 18 A mid-rotation email check-in was adopted to provide more assistance to work towards completing goals. Due to competing time priorities, adopting formal coaching sessions has not been feasible.
Discussion
Our pilot goal-setting intervention had a number of challenges. First, there was a relatively low adherence rate (59%). An electronic version of the form sent prior to the rotation may aid in improving adherence from those trainees that miss the orientation session. In addition, to improve adherence, the form could be made mandatory and a follow-up system could be developed to track forms that are not completed.
Trainee time to set goals was less than 10 minutes; however, as noted, this was a perceived burden to 1 resident on the survey. Although the initial time with the preceptor to review goals is minimal (less than 10 minutes) and occurs conveniently during rotation orientation, there is no protected time for faculty to provide ongoing coaching around individual goals and no means of monitoring progress. Incorporating a mid-rotation goal progress inquiry via email instead of a face-to-face encounter mitigated this. If residents were having difficulty achieving goals, time and effort was required to create encounters to help reach them. With the transition to CMBE underway during the 2019-2020 academic year, residents will now be linked with a faculty advisor. This presents an opportunity for goals to be communicated with the advisors to provide a mechanism for longitudinal coaching.
From those that did participate, it appeared that specific, individualized learning goals were set with a brief introduction and a simple, structured goal-setting form. Many residents created goals unrelated to medical knowledge. This contrasts with the other PGME goal-setting literature and reflects the comprehensive nature of the practice of Geriatric Medicine. 4
Low completion rates of the survey limit the utility of its data. Despite most residents suggesting goal-setting be included in all rotations, only 50% of residents valued goal-setting which is less than that reported by other PGME goal-setting interventions.12-14,19 There are a few potential explanations for this. Other goal-setting interventions often occurred in conjunction with other educational interventions, such as coaching and learning plans that were outside of the scope and resources of this intervention.9,20 It is possible that goal-setting will be more welcomed with the adoption of CMBE, as residents will be provided coaching by academic advisors. As this was a pilot intervention, improvements were made iteratively based on feedback from the residents, which might increase the value.
Engaging internal medicine trainees in Geriatric Medicine to build competency for caring for older adults is critical given the ageing population and shortage of physicians with specialization in caring for older adults.21-24 It is not possible to train the number of geriatricians necessary to satisfy societal needs, but ensuring competent Geriatric Medicine knowledge and skill among health care practitioners as a whole has previously been described as a more attainable goal.25-28 As internal medicine trainees constitute most of the trainees rotating through Geriatric Medicine at the study institution, goal-setting is theorized as an attractive way to engage potentially disinterested resident physicians and improve their performance in caring for older adults.26,29,30
After adjustments are made to the initiative, we plan to scale the structured goal-setting process to another academic institution and complete a more in-depth qualitative study with trainee focus groups to further evaluate their reasons for non-adherence, the perceived value of the initiative, and how it impacts engagement on the rotation.
Footnotes
Appendix 1
Appendix 2
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A grant from Post Graduate Medical Education, University of Toronto, for the development of the pilot. The funding source was not involved in the evaluation of the pilot program, nor was the funding source involved in the development of the manuscript.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author’s Note
Dov Gandell is also affiliated with Department of Medicine, Sunnybrook Health Sciences Centre, Toronto, Canada.
Author Contributions
JA was responsible for the conception and design of the pilot program. She contributed to the abstraction, analysis and, interpretation of data. EC was responsible for abstraction, analysis and, interpretation of data. DG was responsible for the conception, design and, implementation of the pilot program. He contributed to the analysis and interpretation of the data. All of the authors contributed to the drafting and revising of the manuscript and approved the final version submitted for publication.