
Abstract
Technological advancement and improved training strategies have transformed the healthcare practice environment in the last few decades. Simulation has evolved as one of the leading training models for the next generation of healthcare professionals. Simulation-based training enables healthcare professionals to acquire knowledge and skills in a safe and educationally oriented environment and can be a valuable tool for improving clinical practice and patient outcomes. The field of healthcare simulation has been rapidly growing, and various graduate medical education programs around the world have started incorporating this modality into their curricula. In graduate medical education, simulation-based training helps implement an outcome-based curriculum that tests the trainee's actual skill level as the primary factor for the trainee's competency rather than relying on the current model of a predetermined training period. However, the major challenge revolves around developing an educational curriculum incorporating a simulation-based educational model, understanding the value of this new technology, the overall cost factor, and the lack of adequate infrastructure. Hence, embracing the full potential of simulation technology in graduate medical education curricula requires an innovative approach with participation from institutions and stakeholders.
Introduction
Medical education has undergone significant changes worldwide with the advancements in technology and teaching strategies.1,2 Although the Halsted model has worked well for the last 100 years and continues to do so in many avenues,3,4 the healthcare system's practice environment has evolved. This change requires new models for training healthcare professionals; simulation is one such model. 5 High-reliability industries such as aviation, military, nuclear, and oil industries have long emphasized the importance of human factors in understanding safety measures and made simulation-based training a prerequisite.2,6 Efforts are underway to translate lessons learned in these environments to the healthcare industry and the education of future healthcare professionals. 7
Simulation-based medical education provides a safe and controlled environment for problem-based learning where knowledge and procedural-based skills are practiced with high standards to achieve and maintain competencies. 8 In recent years, the field of healthcare simulation has grown rapidly, and these simulation-based education techniques have been included in various graduate medical education training programs.9–11 Accrediting bodies such as the Accreditation Council for Graduate Medical Education (ACGME) in the United States, 12 the General Medical Council (GMC) in the United Kingdom, 13 and the Royal College of Physicians and Surgeons of Canada 14 have included and/or recommended simulation as one of the methods of teaching, practice, and delivery of content as well as assessment of core competencies in the graduate medical education curriculum.
Although simulation-based learning has been increasingly integrated into graduate medical education, it is still not an integral part of the graduate medical education curriculum in many instances. 2 Incorporating simulation-based training as one of the possible training models in the graduate medical education curriculum could help improve the future healthcare professional learning environment and thereby promote clinical competence and patient safety.
The aims of this article are to define the principles of simulation-based training, provide a review of the historical perspectives, current status, and future directions of healthcare simulation, and elaborate on its suitability for incorporation into graduate medical education.
Principle of Simulation-Based Training
Simulation is defined as “A technique that creates a situation or environment to allow persons to experience a representation of a real event for the purpose of practice, learning, evaluation, testing or to gain an understanding of systems or human actions” (Healthcare Simulation Dictionary). 15 Healthcare Simulation is defined as “The application of a simulation activity to training, assessment, research, or systems integration toward patient safety” (Healthcare Simulation Dictionary). 15 The principle of simulation-based training in the domain of technical competence is to provide learners with an opportunity for deliberate practice to achieve a predefined benchmark.2,6,7 This allows learners to learn from their mistakes in a low-stress and safe environment and achieve proficiency in those benchmarks. 7 Although these are different from health care in many ways (humans vs machines), high-reliability industries such as aviation, military, nuclear, and oil industries build training systems based on simulation-based learning models and are more resilient to accidents and adverse events.2,6 For example, standardization, strengthening, and the introduction of various simulation-based training models of safety procedures have led to a significant reduction in aircraft accidents and improved safety. 6
In healthcare, the principle of simulation-based training applies to the acquisition of any procedural, clinical, or attitude-related skills in environments that range from low-fidelity to high-fidelity. 11 Fidelity is defined as a level of realism associated with a particular simulation activity.15,16 Low-fidelity has been defined as “not needing to be controlled or programmed externally for the learner to participate; examples include case studies, role-playing, or task trainers used to support students or professionals in learning a clinical situation or practice” (Healthcare Simulation Dictionary). 15 In health care simulation, high-fidelity refers to “simulation experiences that are extremely realistic and provide a high level of interactivity and realism for the learner and can be applied to any mode or method of simulation; for example, human, mannequin, task trainer, or virtual reality” (Healthcare Simulation Dictionary). 15 Table 1 highlights different types of simulation used in healthcare.

History of Simulation in Medicine
Simulation-based medical training has been practiced since ancient times. The Sushruta Samhita, an important treatise produced during the golden age of medicine in India (also called Bharat) from 800 BC to 1000 AD, may be one of the earliest treatises to describe simulation.23,24 The treatise described how disciples practiced surgical skills by performing mock operations on various experimental models, such as incising watermelon, gourd, clay pots, and reeds and probing on a worm-eaten wood akin to present-day skills workshops.23,24 Ancient clay and stone models used to demonstrate the clinical features of various diseases were also found across the globe. 25 Historical data also document the use of animals in teaching surgical skills since the middle ages through modern times. 26 With the passage of time and the advancement of technology, medical education has evolved considerably and has become more sophisticated. The earliest simulator in the history of medicine was an obstetrical mannequin named Phantom, made of a human pelvis and a dead baby, developed around 1700 in Paris by father and son Grégoire.26,27 Phantom enabled obstetricians to teach delivery techniques, resulting in the reduction of maternal and infant mortality rates.26,27
The modern era of medical simulation is believed to have originated in the second half of the 20th century. 28 In the early 1960s, resuscitation pioneers Drs James Jude, Guy Knickerbocker, and William Kouwenhoven at Johns Hopkins University, Dr Peter Safar at Baltimore City Hospital, and Dr James Elam at the University of Buffalo School of Medicine were the first to combine chest compressions with mouth-to-mouth breathing to create cardiopulmonary resuscitation (CPR) technique, the modern-day CPR.29–31 The creation of the CPR technique led to the development of Resusci-Anne, a realistic simulator used to teach mouth-to-mouth ventilation by Laerdal Corporation under the leadership of Ausmund Laerdal. 32 This development was the origin of one of the most widely used CPR mannequins of the 20th century. 33 Another significant milestone in healthcare simulation was the development of Harvey, the Cardiology Patient Simulator, by Dr Michael Gordon at the University of Miami in 1968.34,35 Resusci-Anne and Harvey represent the beginning of the modern-era medical simulation, and many other simulators were developed for education and training after this.5,36 Concurrently, the concept of standardized patients was first reported by Howard Barrows in 1964, using actors to portray patient encounters. 37
As technology improved during the 1980s and 1990s, software and computerized systems that mimic physiologic responses and provide real feedback were produced. 38 At Stanford University, a group led by David Gaba developed the Comprehensive Anesthesia Simulation Environment (CASE). 38 The rationale of the CASE simulator was to incorporate the aviation model of crew resource management for teamwork training in a realistic environment. 38 After the success with CASE, simulation-based medical education was implemented into the anesthesia crisis resource management curriculum of graduate medical education, leading to significant advances in team-based training.5,39,40 In the last 2 decades since the CASE simulation model's development, the simulation technique has grown to encompass a variety of tools to provide an augmented learning experience.21,38–40 For example, Anesthesia SimSTAT, a high fidelity, avatar-based online training system developed by the American Society of Anesthesiologists, replicates complex anesthesia emergencies in real-time and can be completed anywhere, anytime. 41 As the capabilities of computer systems continued to evolve, the complexity and capabilities of simulators simultaneously evolved, and new advanced technologies such as virtual reality, mixed reality, and augmented reality have been incorporated into simulation-based medical training.17–19
Importance of Simulation-Based Medical Training
Simulation-based training techniques have been widely applied in the training model of high-reliability industries such as aviation and military, and these industries dictate that trainees must pass numerous simulation exercises before engaging in real-life situations. 6 This rigorous technique allows these industries to achieve the desired aim with minimal accidents and adverse events. 6 Since the last century, increasing efforts have been underway to translate lessons learned in these environments to the healthcare industry. 7 As a result, simulation-based medical training that began with life-like mannequins now encompasses an entire range of systems, from synthetic models to high-fidelity simulation suites.
Currently, simulation-based medical training is incorporated into both undergraduate and graduate medical education. The tremendous increase in the incorporation of simulation-based training in healthcare is highlighted by the creation of multiple committees and interest groups focused on simulation within different medical specialty organizations worldwide. The Society for Simulation in Healthcare (SSH), established in January 2004 as an umbrella organization of all medical specialties, is the largest accrediting body in the United States and operates worldwide. 42 The American College of Surgeons-Accredited Education Institutes (ACS-AEI) was launched in 2005 by the ACS Division of Education and continues to set standards for simulation-based surgical education and training. 43 The American Society of Anesthesiologists (ASA), 44 the Royal College of Physicians and Surgeons of Canada, 45 and the Association for Simulated Practice in Healthcare in the United Kingdom 46 also endorse and/or accredit simulation centers.
To appraise the status of simulation-based medical learning worldwide, we reviewed the number of simulation centers registered/accredited by these four major organizations: SSH, ACS-AEI, ASA, and the Royal College of Physicians and Surgeons of Canada. As of 2023, 1114 simulation centers are registered; of these, 415 are accredited centers (Table 2). The United States has the highest number of accredited healthcare simulation centers, followed by Canada, Europe, and Asia (Table 3).

Abbreviations: SSH, Society for Simulation in Healthcare; ACS-AEI, American College of Surgeons-Accredited Education Institutes; ASA, American Society of Anesthesiologists.
aSome of the simulation centers have overlapping registration/accreditation in the four accrediting bodies

Abbreviations: SSH, Society for Simulation in Healthcare; ACS-AEI, American College of Surgeons-Accredited Education Institutes; ASA, American Society of Anesthesiologists.
Some of the simulation centers have overlapping registration/accreditation in the four accrediting bodies
Current Status of Incorporation of Simulation in Graduate Medical Education
Simulation can be a powerful tool in the training and assessment of residents and fellows enrolled in graduate medical education programs. Different accrediting bodies, such as ACGME, 12 GMC, 13 and the Royal College of Physicians and Surgeons of Canada, 14 have incorporated/recommended simulation-based training in different areas of the curriculum of graduate medical education. ACGME listed simulation as one of the critical assessment tools for a number of the core competencies. 49 For example, ACGME Common Program Requirements state that simulation should/must be incorporated into the structured core didactic activities curriculum where residents or fellows are provided with protected time. 12 The requirement also states that programs could use simulation to conduct interprofessional clinical patient safety activities, such as root cause analyses or other activities that include analysis, formulation, and implementation of actions for the learners. 12 The Royal College of Physicians and Surgeons of Canada also incorporated simulation as one of the teaching and assessment tools for patient-centeredness in the Patient–Physician Relationships section of the CanMEDS Medical Expert. 14 Simulation-based learning will ensure that programs meet the requirements of their respective accrediting bodies and ensure that learners achieve competence and gain the ability to enter independent practice.
To understand the current status of the incorporation of simulation-based learning in graduate medical education, we analyzed the survey responses from the simulation centers accredited by the ACS-AEI from 2018 to 2021. The survey response rate ranged from 23% in 2018% to 95% in 2021. Table 4 shows the ACS-AEI annual reports from 2018 to 2021 focused on learners’ registration, expenses incurred, income generated, curricula implemented, type of simulators used, and research or scholarly activities reported by the participating centers. 50 A total of 156 000 to 882 000 learner encounters were documented in 2018 and 2021, averaging 7400 to 9300 learners per AEI (Table 4). Of these, 34 000 learners in 2018 and 156 500 learners in 2021 were residents’ learners, averaging 1619 to 1701 per AEI (Table 5). The average number of original/adopted simulation-based curricula introduced in the centers ranged from 1 to 5 from 2018 to 2021, and ∼85% to 100% of these curricula were implemented successfully (Table 4). The number of simulators in these AEI centers increased from 2018 to 2021, but the average number of simulators per AEI is 6 (Table 4). The types of simulators used in these AEIs range from general-use to specialty-specific simulators and are highlighted in Table 6. The total number of research or scholarly activities also increased from 2018 to 2021, but the average remains at 5 to 6 per AEI (Table 4). Interestingly, the annual reports did not show a significant difference between the income earned and expenses incurred per AEI from 2018 to 2021 (Table 4). These findings indicate the increasing incorporation of simulation-based training in graduate medical education and the potential for expansion in the future.
Number of ACS-AEIs, affiliations, learners numbers, course hours, CME credits, curricula type, simulator numbers, research or scholarly activities, expenses, income.

Type and number of learner encounters (participants attending multiple activities are counted multiple times).

Types of simulators and number of AEIs with availability/supporting use of them effectively to meet learner and curricular needs.

AEI, Accredited Education Institutes.
Benefits of Simulation-Based Medical Education
Simulation-based medical education enables healthcare professionals to acquire knowledge and skills in an educationally oriented, safe, low-stress environment. Skills acquired through simulation-based activities can be cross-pollinated into clinical practice, resulting in improved patient outcomes. 7 Evidence suggests improved performances in clinical settings after the use of simulation.9,51,52 For example, in a study by Ali et al that focused on the simulation-based assessment of trainees’ performance in postcardiac arrest resuscitation, trainees with critical care simulation training performed better overall than those without critical care training. 52 In graduate medical education, simulation-based training helps implement an outcome-based curriculum that focuses on competencies, which is different from the established system based on a time-based construct. 9
With the use of immersive simulation in graduate medical education to recreate the operating room environment, the technique of simulation has grown to encompass a variety of tools to provide an augmented learning experience. For example, the high-fidelity Anesthesia SimSTAT replicates complex anesthesia emergencies in real-time and can be completed anywhere and at any time. 41 Furthermore, a simulated operating room can be modeled as a real patient environment that requires cognitive and professional skills and enables trainees to receive feedback about their technical and nontechnical performance. 53
Type of Simulation Commonly Included in Graduate Medical Education
The simulation methods used in graduate medical education can range from computer-based clinical simulations, task trainers, and role play and games to full-scale life-like versions of virtual clinical environments using trained individuals and technology to mimic clinical problems, conditions, and events in medicine. 11 Table 7 highlights the type of simulator commonly included in graduate medical education programs.

Comparison of Simulation Effectiveness With Other Teaching Methods
Studies have reported that simulation-based medical education with deliberate practice can be, at times, more effective than traditional clinical medical education in achieving some of the clinical education skills.59–63 Simulation-based learning is unique because it can design scenarios to include and evaluate all six ACGME core competencies. 64 With the integration of simulation-based training in graduate medical education, various procedural, communication, leadership, and team-working skills can be learned and measured. This, in conjunction with other well-established methods, can be used as another pathway for the assessment of competency prior to entering independent practice.65,66 Simulation can also create models for improving patient safety when such innovations are translated into clinical environments. With simulation-based learning, trainees can acquire and retain clinical skills with repetitive practice. Debriefing after simulation-based learning can help understand how learners make medical decisions by evaluating medical knowledge and interpersonal and communication skills by asking open-ended questions. 67 Simulation can also be helpful for leadership training. Furthermore, learners who participated in the simulation demonstrated better communication skills compared to the passive didactic training method. 68
Although simulations alone cannot improve the quality of health care, a combination of enriched curricular and educational environments, such as virtual operating suites, can significantly advance clinical education, leading to enhanced clinical reasoning and professionalism. 2 Some of the benefits of simulation-based learning in medical education compared to other teaching methods are highlighted in Table 8.

Barriers and Limitations of Simulation-Based Medical Education
Although graduate medical education programs should incorporate simulation into the training pathways, several challenges abound. These challenges can be grouped into two categories: barriers to simulation-based medical education and limitations of simulation-based medical education.
Barriers to Stimulation-Based Medical Education
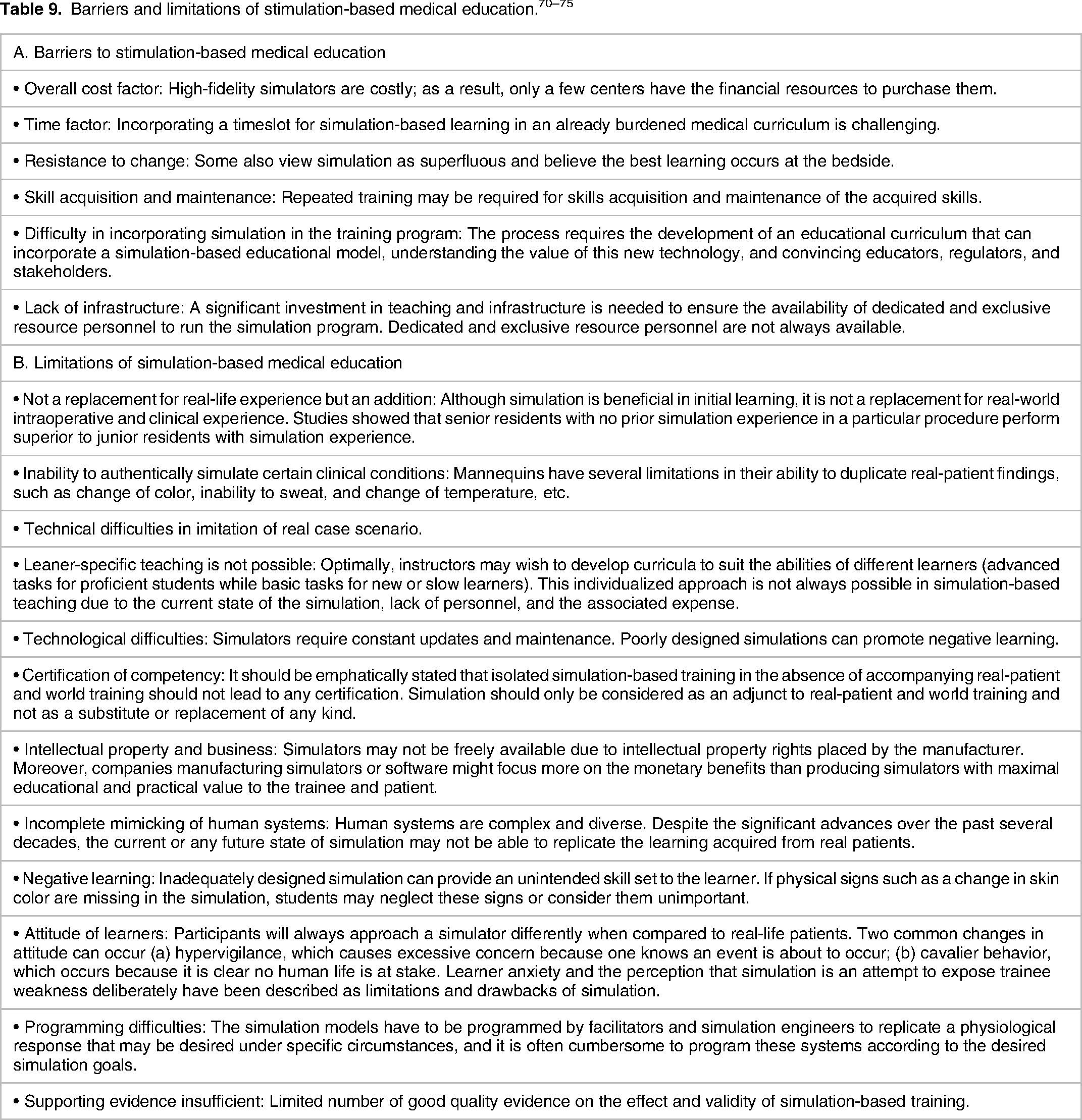
The major challenge revolves around developing an educational curriculum incorporating a simulation-based educational model and understanding the value of this new technology. In addition, simulation-based assessment should produce reliable, valid, affordable, and practical results for the trainee and institution. 28 However, simulation centers and simulation equipment can be costly. A single high-complexity simulator may cost up to $200,000, with additional costs required for maintaining warranties for any malfunction. 69 Moreover, simulation does not always lead to a successful learning outcome or translate into better patient outcomes. 70 Simulation-based educational curricula may need more clinical validity to enhance the benefits of the activity. 71 Simulation centers also need dedicated personnel, including simulation technicians, to set up, operate, and break down scenarios, oversee the standardized patient program, and instruct learners (students, residents, fellows, etc). 72 Many training programs have no or limited access to simulation centers to conduct these activities. 72 Table 9A highlights the common barriers to simulation-based medical training.
Limitations of Stimulation-Based Medical Education
Although simulation-based medical training is increasingly incorporated in graduate medical education curricula, simulators and task trainers cannot replace real-life experience, and there is technical difficulty in imitating real case scenarios.70,73 Furthermore, it is challenging to attribute improved patient care outcomes solely to simulation when other confounding factors, such as time, fatigue, and clinical experience, are present. 74 A study reported that senior residents with no prior arthroscopy simulation experience continued to perform superior to junior residents with arthroscopy simulation experience. 69 This study demonstrated that although simulation is beneficial, it is not a replacement for intraoperative and clinical expertise. 69 Table 9B highlights the common limitations of stimulation-based medical education.
Future Directions
The goal of graduate medical education programs is to train competent physicians. However, determining the most efficient way to evaluate a particular competency can be challenging at times due to various factors.76,77 Standardized testing assesses a learner's clinical knowledge but does not assess the application of that knowledge in a clinical setting. Simulation-based testing has the capacity to assess the application of this knowledge in clinical settings, holds great promise in developing competency-based assessments, and should continue to be validated as a grading model. As simulation gets adopted into graduate medical education training programs with demonstrated benefits to education and patient care, we anticipate it will become more accepted as a learning modality by the healthcare community. We also expect that simulation-based learning will enhance resident training that can be objectively measured through milestones, especially in surgical specialty programs. Moreover, advanced robotics and VR or AR will expose trainees to real-life examination findings rarely encountered in short clinical rotations.
Creating and implementing a simulation curriculum requires expertise in case creation and production and familiarity with debriefing techniques. Medical education-focused platforms such as MedEdPORTAL, 78 which publish program-focused peer-reviewed simulation cases that include resources and checklists, can be adapted to meet educators’ objectives. As more educators embrace simulation, developing a standardized case repository would enable educators to help facilitate simulation-based education. These collaborative efforts will assist in adequately measuring clinically meaningful simulation training.
With the rapid advancement in technology and the adoption of simulation-based training in graduate medical education, there is a demand for more simulators to complement and provide training. Cost and limited access to specialized simulation centers are primary barriers to the adoption of simulation. However, expanding access to technological advances may provide workarounds to these problems. For example, old and expired medical equipment from healthcare industries can be used and reused in simulation. 3D-printed simulation models and low-cost do it yourself (DIY) models could significantly lower costs for a task trainer and improve procedural skills acquisition by facilitating sustained, deliberate practice, even in remote and low-resource settings. Moreover, the development of adaptive trainers that do not require expert instructors, sharing simulation space among multiple residency programs and healthcare organizations, and partnering with equipment vendors may allow trainees to practice procedures with little cost.67,79 Advances in virtual and hybrid simulation models will also help bypass the cost of a simulation center and promote healthcare simulation beyond highly resourced academic centers. Furthermore, leaner-centered approaches of a simulation-based program can help learners actively develop their knowledge and skills instead of passively receiving expert didactic lectures. This often allows senior residents or fellows to substitute for faculty in some roles. In addition, choosing the appropriate level and type of fidelity and scenario, as well as providing appropriate instructions and team planning before starting a scenario, can help maximize learning. Providing an immersive learning experience using smell, sounds, visuals, and movement components in a simulator could also help in providing a realistic experience to the learners.
Although not without limitations, simulation offers learners a flexible range of learning and assessment formats at the bedside and virtually and will continue to play an integral role in the world of graduate medical education. Hence, additional research, validation and participation from stakeholders and institutions are warranted to facilitate the growth of simulation-based training in graduate medical education programs worldwide.
Conclusion
Simulation-based training holds enormous potential to revolutionize medical education in the future. Still, more studies are needed to validate the translational benefits of simulation and to identify skills that are most effectively acquired through simulation. Further work remains to be done to define the best modalities of simulation and its application to the world of graduate medical education. Through innovation and research, we should identify the best simulation paradigms for incorporation into graduate medical education. This will help train competent physicians who can enter independent practice to help address healthcare needs.
Footnotes
Author Contributions
Conceptualization: PDL, CA; literature search: PDL, PRA, and CA; manuscript preparation and critical revision: PDL, PRA, and CA. All authors read and approved the final manuscript.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.