
Abstract
Among medical students, neurosceince is considered a notoriously difficult subject. This challenges faculty to teach preclinical neurology in more engaging, efficient, and prioritized ways. Traditional approaches to neuroscience instruction typically begin with neuroanatomy and advance to clinical problem solving after this foundation of knowledge is in place. Over the past 45 years, neurology faculty at Mayo Clinic Alix School of Medicine have developed and iteratively refined an inverted approach called The Basic Four. The Basic Four uses authentic clinical scenarios as the basis for neuroscience instruction and incorporates principles from cognitive load theory to calibrate load on students’ working memory. This perspective describes The Basic Four and illustrates how cognitive load theory can be used to enhance case-based learning.
Keywords
Introduction
Introducing preclinical medical students to neuroanatomic localization poses challenges to learner and teacher alike. Novice learners often perceive neuroscience to be complex, esoteric, and formidable—so much so that the term “neurophobia” has been coined to describe the apprehension with which they approach it.1-6 Students often have little neuroscience background, and retention of neuroscience knowledge into the clinical years is poor. 7 For these reasons, the task of teaching neuroanatomy has been called “difficult and unenviable.” 8
Compounding these challenges are trends in medical education, including initiatives to shorten medical school training, 9 incorporate new content into medical school curricula,10-12 and undertake various other curricular reforms. Current and projected shortages of neurologists also highlight the need to recruit more students into the specialty. 13 Thus, faculty are compelled to teach neuroscience in more engaging, efficient, and prioritized ways.
Over the years, neurology faculty at the Mayo Clinic Alix School of Medicine have responded to these challenges by developing an innovative approach to clinical neuroscience instruction called The Basic Four. The original version of this approach was conceived in 1972 by Dr Burton Sandok, a Mayo Clinic neurologist, later department chair, then medical school dean, known for his ability to teach and simplify complex concepts. 14 It has since been iteratively refined and revised by numerous neurology faculty and used to teach neuroscience to more than 1700 preclinical medical students in both small and large group settings. In this perspective, we aim to describe The Basic Four approach and illustrate how cognitive load theory (CLT) can be used to enhance case-based learning. This is not a one-size-fits-all approach, but rather an example of how learning theory can enrich and inform neuroscience instruction.
Overview of The Basic Four Approach
The Basic Four represents a type of case-based learning 15 in which students are presented with authentic clinical cases (in a variety of formats) and prompted to answer four questions (Q1-4, Figure 1A). This standardized set of questions guides students through the tasks of neuroanatomic localization (Q1-2) and differential diagnosis (Q3-4), allowing novice students to reach possible diagnoses with relative ease. This process serves as a springboard for subsequent inquiry into basic and clinical neuroscience concepts. Figure 1B shows the shorthand version of The Basic Four as it appears in all course materials. Because the same set of questions is applied to every clinical scenario, students quickly internalize these abbreviated question-and-answer groupings.

The Basic Four.
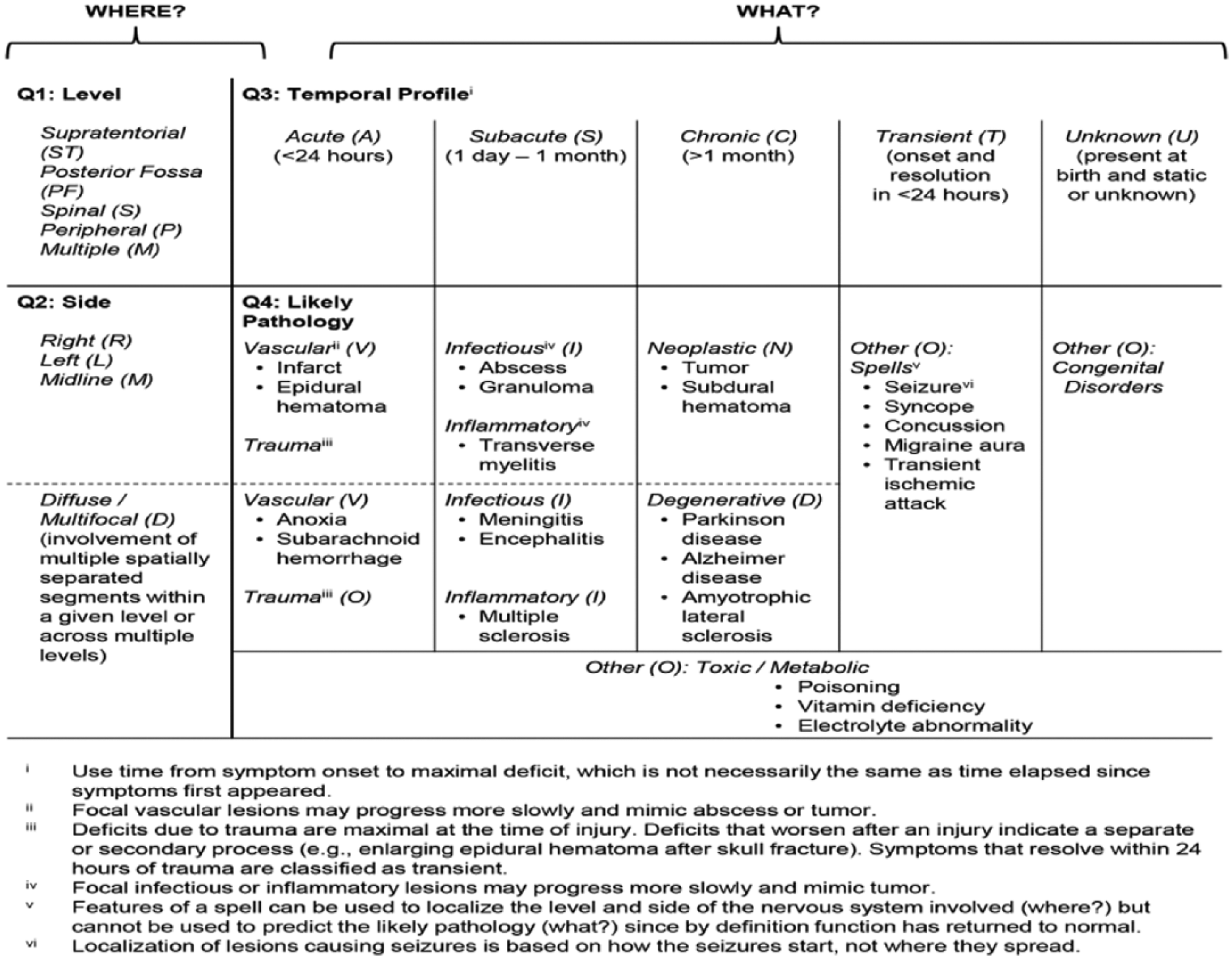
Table 1 provides six illustrative clinical scenarios, their Basic Four formulations, and a possible diagnosis for each. Guidelines for applying The Basic Four are provided in Figure 2, which can also serve as a handout for learners. These guidelines summarize “first principles” of neuroanatomy 8 (eg, ipsilateral face and limb involvement suggests a contralateral supratentorial lesion) and physiology (eg, a process that starts acutely is likely to be vascular in nature), which can be learned and applied without any previous neuroscience training. Initial cases are very simple (Table 1, case 1) but increase in complexity (Table 1, case 6) and fidelity (through the use of video clips and a simulated patient encounter) as the course progresses and students’ knowledge base grows.
Examples of The Basic Four applied to clinical scenarios to localize a lesion and generate a possible diagnosis.

In this fashion, The Basic Four approach uses clinical reasoning as the starting point for neuroscience instruction, encouraging students to develop cognitive schemata from worked examples. Notably, Basic Four problems are intended to be the means by which students learn neuroscience, rather than simply an opportunity for students to apply previously learned concepts. This represents an inversion of more traditional approaches, which typically begin with neuroanatomy and advance to clinical problem solving after this foundation of knowledge is in place.
Rationale for The Basic Four Approach
Case-based learning has been shown to positively impact a number of relevant learning outcomes across a variety of subject areas, 15 including neuroanatomy16-19 and neurologic reasoning.20,21 Case-based learning is also recognized as a way to foster interest in neurology. 22 The Basic Four method seeks to further optimize this approach by incorporating principles of CLT.
CLT posits that learning is most effective when instruction is aligned with human capacity for information processing. According to CLT, information processing is most acutely constrained by the limited capacity of working memory, which can hold only a few discrete elements at any given time. 23 If the elements being held in working memory interact (requiring simultaneous processing), working memory becomes further constrained. 24 In this fashion, the capacity of working memory varies between learners and within the same learner at different times.
Neuroanatomic localization and neurologic clinical reasoning are complex tasks that can easily exceed the processing capacity of novice learners, resulting in cognitive overload. 25 Three types of cognitive load can strain working memory: extraneous load (effort required to cope with factors not directly related to the task at hand, such as interruptions or dense lecture slides), intrinsic load (effort required to process the inherent complexity of new information, such as lateral medullary syndrome), and germane load (effort required to build cognitive schemata through which one understands new concepts, such as upper versus lower motor neurons). For novice learners without preexisting cognitive schemata or mental representations (eg, first-year medical students learning neuroanatomy), intrinsic load is particularly hefty. 22
When total cognitive load exceeds working memory capacity, learning is impaired. 24 CLT can inform strategies to prevent working memory overload and optimize allocation of cognitive resources during case-based learning by reducing extraneous load, titrating intrinsic load to the learner’s level, and optimizing germane load. 24
The Basic Four approach aims to reduce extraneous load by providing a consistent approach to neuroanatomic localization that is maintained throughout the entire neuroscience course, including large group lectures, small group sessions, weekly tests, the final examination, and a simulated patient encounter. In each setting, The Basic Four is presented in the same format and order with consistent abbreviations (Figure 1). Thus, no cognitive load is wasted deciphering new formats or harmonizing discrepant structures, and students’ working memory can be more fully devoted to learning. Table 2 outlines additional ways in which The Basic Four tries to reduce extraneous load.
The Basic Four application of cognitive load theory principles to decrease extraneous load.

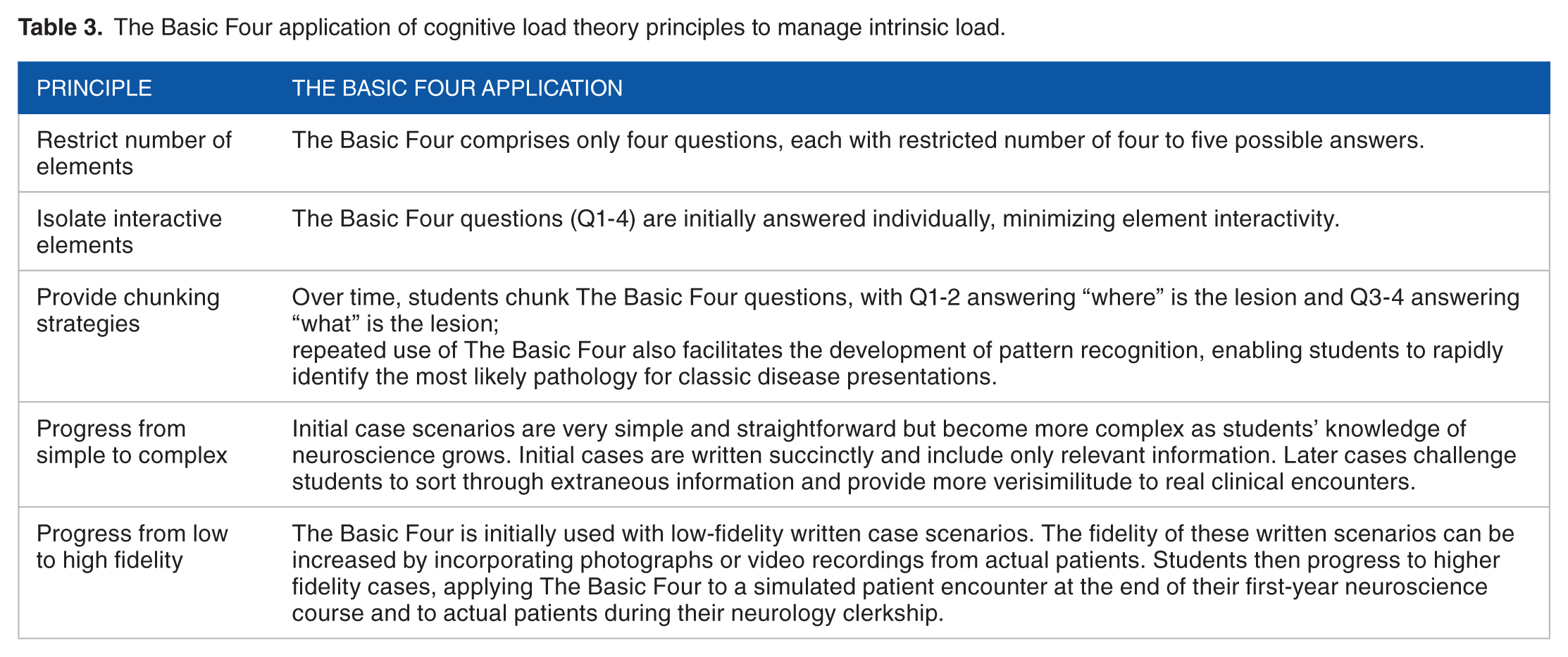
The Basic Four approach seeks to manage intrinsic load by simplifying and constraining the tasks of neuroanatomic localization and differential diagnosis generation. Notably, the number of interacting elements is restricted to four, the maximum capacity for simultaneous manipulation by working memory. Isolating these elements initially is intended to manage intrinsic load for novice learners. Over time, intrinsic load may be further reduced by viewing The Basic Four as two pairs of questions, with Q1 and Q2 answering “where” and Q3 and Q4 answering “what.” This is an example of “chunking,” which reduces interactivity and thereby lessens intrinsic load. 26 Table 3 outlines other ways in which The Basic Four seeks to manage intrinsic load.
The Basic Four application of cognitive load theory principles to manage intrinsic load.
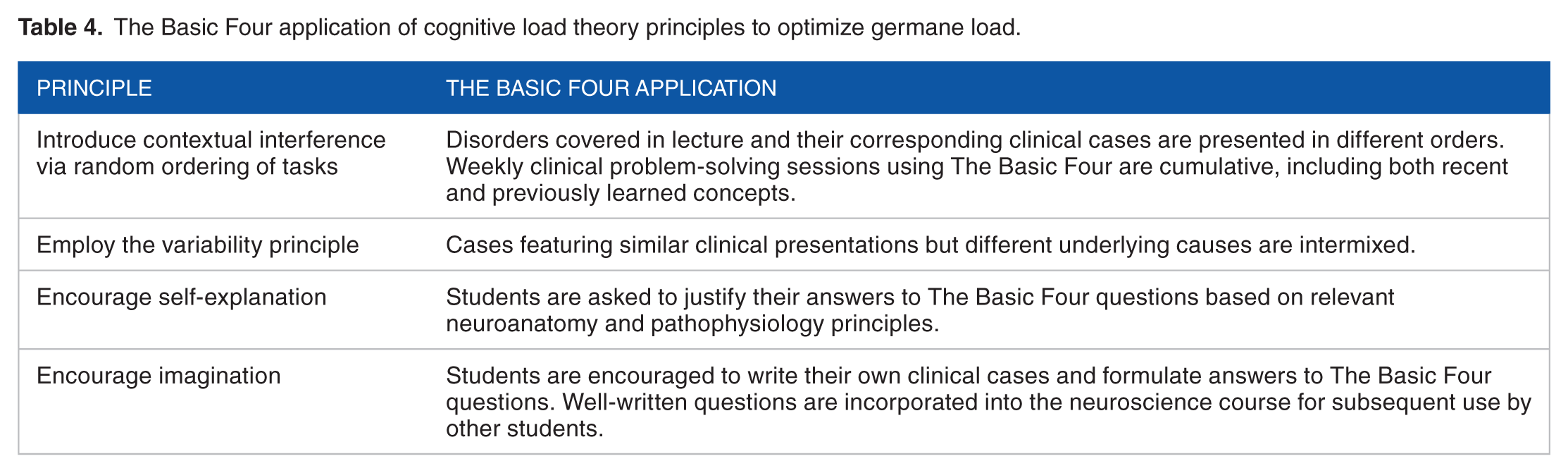
Once extraneous load has been minimized and intrinsic load titrated, newly liberated working memory capacity can be allocated to germane load. The Basic Four approach attempts to optimize germane load by varying clinical problem-solving tasks, which has been shown to enhance learning. 24 Course instructors can apply this “variability principle” 27 by interweaving clinical cases with similar presentations but different causes (eg, progressive myelopathy due to infection, disk herniation, or spinal meningioma) and different presentations of the same cause (eg, cerebral ischemia). This optimizes germane load and encourages students to maintain a broad differential diagnosis. Table 4 outlines additional ways in which The Basic Four approach can optimize germane load.
The Basic Four application of cognitive load theory principles to optimize germane load.
Clinical reasoning is a complex, iterative task that involves both analytic and non-analytic strategies and is influenced by contextual cues. 28 The Basic Four aims to introduce novice learners to this process by facilitating the creation of initial hypotheses about the nature of a patient’s problem. It answers the questions “where?” and “what?” but does not aim to answer the question “why?” (ie, by providing a specific diagnosis or definitive explanation for the patient’s problem). Instead, The Basic Four guides students to a disease category from which to generate a list of diagnostic possibilities. This exemplifies the use of nonspecific goals, which reduce cognitive load for novice learners, improve their problem-solving strategies, and facilitate transfer of learning to new contexts (the “goal-free principle,” Table 2).29,30
Discussion
The Basic Four is a practical, clinically oriented approach to teaching neuroanatomy and neuroscience that seeks to optimize case-based learning by incorporating principles of CLT. This approach illustrates how educators can apply evidence-based learning theories to common pedagogical strategies to increase their effectiveness—a recommended strategy for combatting neurophobia and promoting neurophilia. 31
The Basic Four approach is particularly well-suited for novice learners, allowing them to engage in part-task practice with increasing complex written case scenarios. 32 Importantly, The Basic Four is suitable for use with a variety of instructional modalities (eg, large group lectures, small group sessions, face-to-face teaching, online learning modules, and other digital learning tools) and can also be used in simulated or real clinical settings, such as those encountered during clerkships. In this fashion, The Basic Four accommodates increasing task complexity and fidelity, which allows for vertical integration of neurology curricula 31 and may facilitate transfer of knowledge from classroom settings to subsequent patient care. 25 Repeated use of The Basic Four may also improve retention, an important initial step toward ensuring students acquire the essential neurologic skills needed for high-quality patient care. 33
The nervous system is a highly complex and nuanced biological entity, and The Basic Four, like any conceptual framework, presents only a partial view of reality. 34 Seasoned neurologists will recognize its shortcomings and identify exceptions. For example, carpal tunnel syndrome often presents as a focal, chronic lesion but is rarely caused by a neoplasm (the resulting Basic Four diagnosis). However, it is important for medical educators to recognize oversimplification as an asset to early learners. Instructors tend to underestimate the difficulty of assimilating new information because they have the benefit of existing cognitive schemata, 35 whereas learners face the more demanding task of schema construction. 24 Strategic simplifications, such as those offered by The Basic Four, aid in this process by teaching students the “rules” before they learn the “exceptions.”
Conclusions
Traditional approaches to preclinical neuroscience instruction typically begin with neuroanatomy and advance to clinical problem solving after this foundation of knowledge is in place. The Basic Four inverts this approach by first providing a scaffold or cognitive schema for solving clinical problems, then populating this scaffold with relevant knowledge of neuroanatomy, physiology, and pathology. The Basic Four illustrates how CLT can be used to enhance case-based learning in an effort to make the process of learning neuroscience more efficient, effective, and enjoyable. This, in turn, may foster interest in neurology and help combat neurophobia. Further study is needed to measure the impact of The Basic Four approach on relevant outcomes such as performance on standardized tests, clinical clerkship evaluations, and recruitment of medical students into neurology.
Footnotes
Acknowledgements
The authors wish to acknowledge the late Dr Burton Sandok (1937-2011) for developing the original version of The Basic Four, the faculty of the Mayo Clinic Alix School of Medicine first-year neuroscience course for their dedication to teaching clinical neurology, and the hundreds of medical students whose enthusiasm for learning and insightful questions have inspired ongoing refinements of The Basic Four approach.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
KES, JKC-G, and ANLH contributed to the study concept, study design, and drafting of the manuscript. All authors approved the final manuscript.