
Abstract
Introduction
Malaria is a potentially life-threatening infectious disease caused by protozoan parasites of the genus Plasmodium. Plasmodium falciparum causes the most severe disease. The parasites are vectored by Anopheles mosquitoes and trigger symptoms when they multiply in human red blood cells (erythrocytes).
Malaria is characteristically an acute febrile illness. The symptoms of uncomplicated malaria are nonspecific and include fever, chills, headache, and vomiting. If not treated within 24 hours, malaria can progress to severe illness and can be fatal. In children, severe malaria can include symptoms such as severe anemia, respiratory distress in response to metabolic acidosis, or convulsions and coma in cases of cerebral malaria. Long-term neurological abnormalities such as ataxia, palsy, speech impairment, deafness, and blindness may persist after cerebral malaria, especially in children.
Interventions to prevent malaria include vector control methods (mainly the use of insecticide-treated nets and indoor residual spraying), chemoprevention, and potentially vaccination. Artemisinin-based combination therapies (ACT) are recommended by the World Health Organization (WHO) for the treatment of uncomplicated malaria caused by P. falciparum, and have been shown to reduce malaria mortality by 97% to 99% in children aged <5 years.
Despite the increase of prevention and control methods, malaria is still a major public health burden in sub-Saharan Africa, being in the top three causes of childhood death. In 2015, there were an estimated 191 million cases of malaria and 394,000 malaria deaths in the WHO Africa region. The malaria burden is concentrated in young children. In 2015, there were an estimated 292,000 malaria deaths in children aged <5 years in the WHO Africa region, accounting for 74% of malaria deaths.
Malaria is therefore associated with a high economic and social burden. Malaria costs may be substantial in relation to household income in sub-Saharan Africa, especially in poorer socioeconomic groups. 1 After taking into account factors such as initial poverty, economic policy, and tropical location, the rate of economic growth per capita in countries with malaria was estimated to be 1.3% per year slower between 1965 and 1990, compared with countries without malaria. 2 The long-term effect of this lower growth rate is an income per capita, in a country with intensive malaria, that is only around one third of that in a country without intensive malaria. 2
The objective of this study is to conduct a systematic review of information available from the peer-reviewed literature on health system costs, health care resource use, and household costs for the management of malaria episodes in children aged <5 years in sub-Saharan Africa. It should help identify information that can be applied to improve understanding of the economic burden of malaria to health systems and households, and to help assess the potential economic impact of malaria prevention.
Methods
Search Strategy
Three electronic databases, Medline, EMBASE, and the Cochrane Library, were searched to identify studies reporting information on economic impact and resource use associated with malaria management in children aged <5 years in sub-Saharan Africa. For example, search terms in Medline for disease included ‘Malaria (MeSH),’‘plasmodium (MeSH),’ or ‘“plasmodium falciparum” (MeSH),’ search terms for economics included ‘budgets (MeSH)’ or ‘economic (MeSH),’ and search terms for the geographical area included ‘sub-Saharan Africa (MeSH)’ or ‘West Africa (MeSH)’ together with individual country names. Detailed search terms are presented in Supplementary Material: Search terms. The searches were limited to studies published in English or French, and added to the database between January 1, 2006, and September 1, 2016. In addition, hand searches were conducted to identify relevant conference abstracts from key conferences between 2014 and 2016.3–14
Study Selection
Studies before 2006 were excluded. Studies were selected according to the predefined PICOS (Population, Intervention, Comparison, Outcome, Study type) framework. As this was a review of information on cost of illness, “Intervention” and “Comparison” were not applicable, and the “Outcome” of interest was cost data. Full details of the PICOS criteria used are presented in Supplementary Material: PICOS criteria. Studies were included if they met the following criteria:
Population: children aged <5 years with malaria (including uncomplicated, severe, or other manifestations of malaria, with or without laboratory/rapid diagnostic test [RDT] confirmation), living in sub-Saharan Africa.
Costs reported: costs per disease episode; costs of antimalarial treatments; diagnosis and treatment of uncomplicated or severe malaria, including late manifestations of severe malaria; treatment of symptoms attributable to malaria (e.g., fever). Studies on the cost of management of febrile illnesses without malaria confirmation were included only if indirect costs associated with productivity loss and opportunity costs (travel time and waiting time) were reported. The selected studies reported costs from either the health care sector or household perspective. Health care sector costs were defined as the direct cost of malaria per episode or total cost of malaria over a known number of episodes. Household costs included direct and indirect costs associated with episodes of malaria including out-of-pocket payments, transportation, self-medication, and traditional therapy.
Study type: observational studies, pragmatic trials, and clinical trials of therapeutic interventions were included. Model-based studies were included only if they estimated costs of treatment provision for diagnosed malaria cases.
Studies were excluded as follows:
Studies in North Africa or South Africa, or studies in populations not receiving treatment in the context of routine health care delivery (e.g., displaced populations) were excluded.
Studies on disease recurrence, reinfection, incorrect treatment administration, screening and mass administration of interventions, or studies reporting information that could not be attributed to a uniquely identifiable disease episode were not included.
Case reports, letters, comments, and historical articles were excluded.
Publications identified by the electronic searches were first screened for relevance by reviewing the title and abstract. Studies that were eligible after primary screening underwent full-text review against the selection criteria above. Two reviewers conducted the screening and full-text review. Any discrepancies were resolved by discussion or the involvement of a third reviewer.
Data including country, study period, population, study type, and reported costs were extracted from studies meeting the selection criteria. All costs were inflated and converted to 2016 US dollars using the CCEMG-EPPI Centre online cost converter tool using the International Monetary Fund dataset for purchasing power parity values and the year of data collection if available, otherwise the year of study publication. 15
Risk of Bias Assessment
A risk assessment was performed by one reviewer on the studies reporting resource use and cost data. The included studies in this review were analyzed separately, and potential limitations in the methods (i.e., study design, data collection, and data entry) were flagged as well as potential self-reported biases.
The PRISMA checklist completed for this literature review can be found in the supplementary material.
Results
Search Results
A total of 1846 publications were identified from the searches and screened using title and abstract. Of these, 101 underwent full-text review, and 16 met the selection criteria.16–31 One additional study was identified from the hand searches of conference abstracts, 32 resulting in a total of 17 studies included (Figure 1). The most recent publication date was 2016. 29

Search results and study selection.
The studies covered nine countries, the Democratic Republic of Congo (DRC), Ghana, Kenya, Malawi, Mozambique, Nigeria, Tanzania, Uganda, and Zambia.
Studies on Malaria Costs to Health Systems
Characteristics of Included Studies
Seven studies16–22 estimated health care costs for episodes of malaria in a range of settings. Five studies were costing studies,16,17,19–21 one analyzed the pattern of medicine prescribing in the community, 18 and one was an expenditure study. 22 In addition, a model-based study estimated health care system costs and private expenditure in three countries (Ghana, Kenya, and Tanzania). 30 Table 1 summarizes the study characteristics.
Characteristics of Included Studies on the Cost of Malaria Episodes to Health Systems

HC, health care; OPD, outpatient department.
Cost of Health Care Associated With an Episode of Malaria
Five studies16,19,20,22,30 reported data on inpatient costs for an episode of malaria, and three17,18,20 reported data on outpatient costs (Table 2). Health care costs included the costs of diagnostics and treatment, drug costs, administration costs, and hospitalization costs.
Inpatient and Outpatient Costs per Episode of Malaria to the Health Systems

ACT, artemisinin-based combination; ART, artesunate; CI, confidence interval; DRC, Democratic Republic of Congo; NA, not applicable; NR, Not reported; QNN, quinine; US, United States.
Public health hospital (Institut Médical Evangélique, Kimpese, Bas Congo); one medium-sized, nonprofit, missionary hospital (St Luc Kisantu); and a medium-sized, government hospital (Centre Hospitalier Roi Baudouin). In addition, five rural health centers were selected within the same Health Zones (HZs; Health Centre Bita, Health Centre Menkao, Health Centre Ngeba, Health Centre CECO, and Health center La Famille).
Mean cost for oral quinine and Artesunate-Amodiaquine (AS-AQ).
Medical center is a health care facility which provides outpatient services. Teaching hospital is a tertiary health care facility providing a variety of specialized clinical and teaching services. It is the main referral public health facility in the state run by the federal government. Patients pay for services and their drugs at the point of delivery.
Artemether-pyrimethamine was the most used antimalarial drug (50.6%), followed by monotherapy sulphadoxine-pyrimethamine (18.8%). For all study age groups, total cost of medication (including co-medications) with artemisinin-based combination (ACT) averaged US$4.10 per prescription about twice the mean cost of treatment with monotherapy US$2.06 but the average medication cost varied noticeably across age categories. While it was highest for children under 5 years at US$3.74 (95% CI; US$3.11 to US$4.35), the lowest was observed for children aged between 5 and 12 at US$2.75 (95% CI; US$2.43 to US$3.06) per case.
The mean cost of medication (including co-medication such as antibiotics) per patient at the two public health facilities for children under <5 years was 1062 Naira. Costs data were standardized with US dollars, as calculated for the 2014 price year (Nigeria) [US$1= 158.553 Naira (2014)]. Exchange rates were obtained from the World Bank Data.
Most studies reported cost for severe malaria or malaria hospitalization with a total cost ranging from US$18.35 to US$136.35 per patient depending on the type of facility (health center or hospital) and complication to be treated (cerebral malaria, anemia) (Figure 2). If a patient was treated in a national hospital, the costs were higher (US$115.18) than if that same patient was treated in a mission hospital (US$106.26). 22 Treatment per inpatient episode of malaria was more expensive in hospitals compared with health centers. 16 The type of malaria was an important cost driver. Treatment for cerebral malaria with anemia or neurological sequelae was more expensive than uncomplicated and severe malaria in Kenya, Ghana, Tanzania, and Zambia.19,30
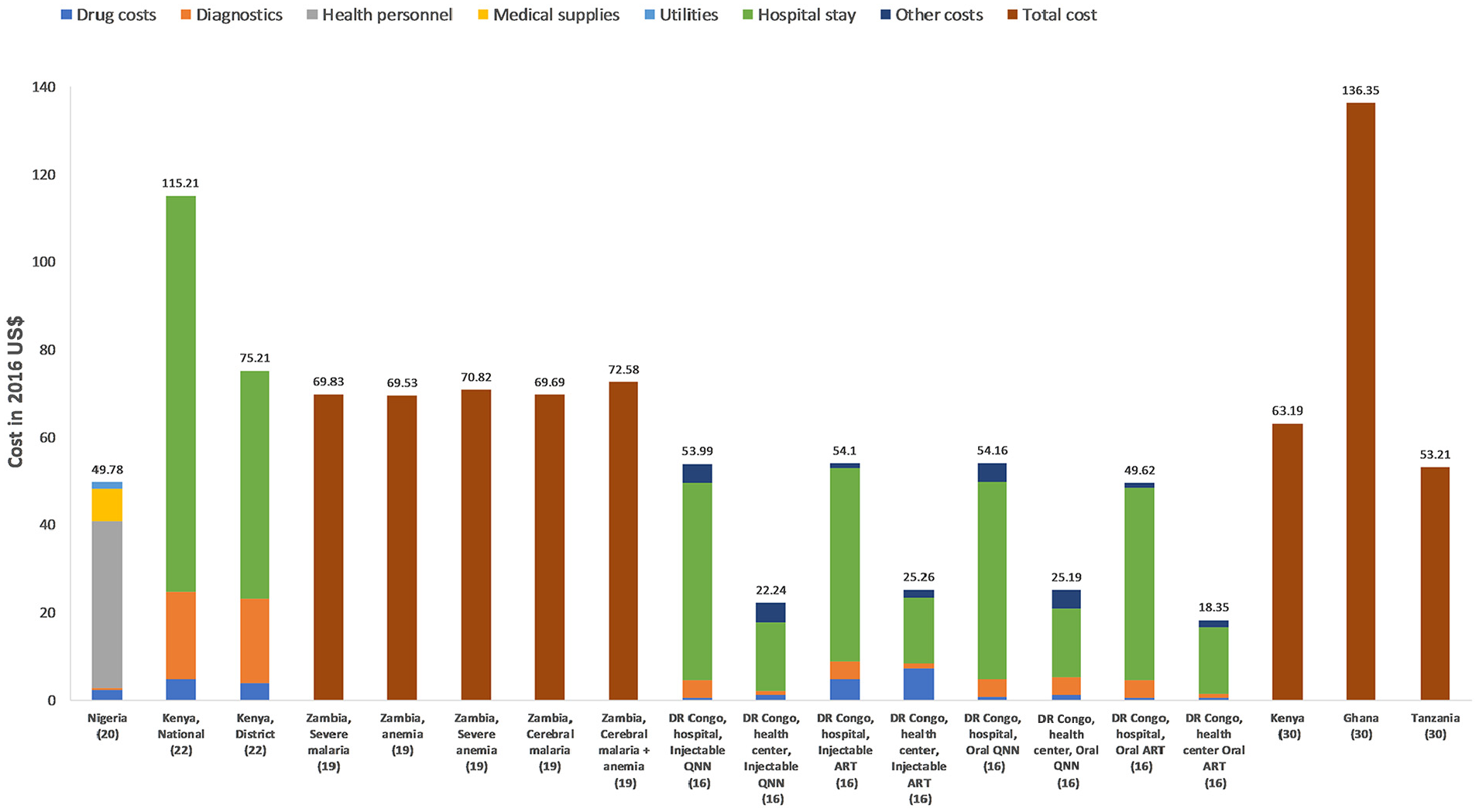
Cost per inpatient malaria case with cost components when available. QNN, quinine; ART, artesunate.
Two studies reported data covering Kenya. Costs reported by Ayieko et al. 22 (National: US$115.18, District: US$75.22) were slightly higher than those reported by Sicuri et al. 30 (range US$3.07–63.19). This could reflect limitations in the cost-analysis methodology used by Ayieko et al., 22 which reported a bed-day cost of hospitalization based on results of two studies each representing a single hospital. Bed-day costs vary significantly between hospitals especially due to differences in occupancy rates. The study authors mentioned that overcoming this limitation was difficult given the expense of conducting multiple formal hospital costing studies. In addition, a high level of presumptive malaria treatments (due to lack of accurate diagnosis) may have encouraged the use of the wrong drug, so total treatment costs could have been overestimated. Fewer studies reported cost for outpatient or uncomplicated malaria with a total cost per episode from US$1.94 to US$7.47 mainly based on drug cost (Figure 3). One study in Nigeria reported higher costs of US$ 31.53 per outpatient case due mainly to personnel costs. 20

Cost per outpatient malaria case with cost components when available.
In Uganda, antimalarial drugs delivered at health facilities were free for children aged <5 years with a diagnosis of uncomplicated malaria, thus placing the economic burden on the health care system rather on households. 27
Inpatient care of an uncomplicated episode (US$5.15) was more expensive than outpatient care (US$2.65), 20 with health personnel and medications being the major cost drivers. Limited data on outpatient delivery were reported.
Length of Stay in Hospital
Only two studies reported data on hospital length of stay.16,22 Ferrari et al. 16 reported that the average length of stay for patients with severe malaria ranged from 1.7 to 7.1 days, depending on treatment and type of health facility. Ayieko et al. evaluated patients with an unspecified malaria diagnosis, and reported an average length of stay ranging from 3.1 days in a mission hospital to 4.8 days in a district hospital. 22
Studies of Malaria Costs to Households
Characteristics of Included Studies
Ten studies20,23–31 reported malaria costs to households (Table 3). Two of these20,30 also reported costs to health systems. In addition, one abstract 32 reported some information on hospitalization costs associated with severe malaria to households in Malawi. Two publications20,23 reported results from the same study, a cross-sectional survey of household expenditure for children with malaria in Nigeria. Similarly, two publications28,29 reported data from the same sample in Uganda. Only one study provided data on the distance to the closest health facility, 27 and only one reported data on the average household income. 25
Characteristics of Included Studies on the Cost of Malaria Episodes to Households
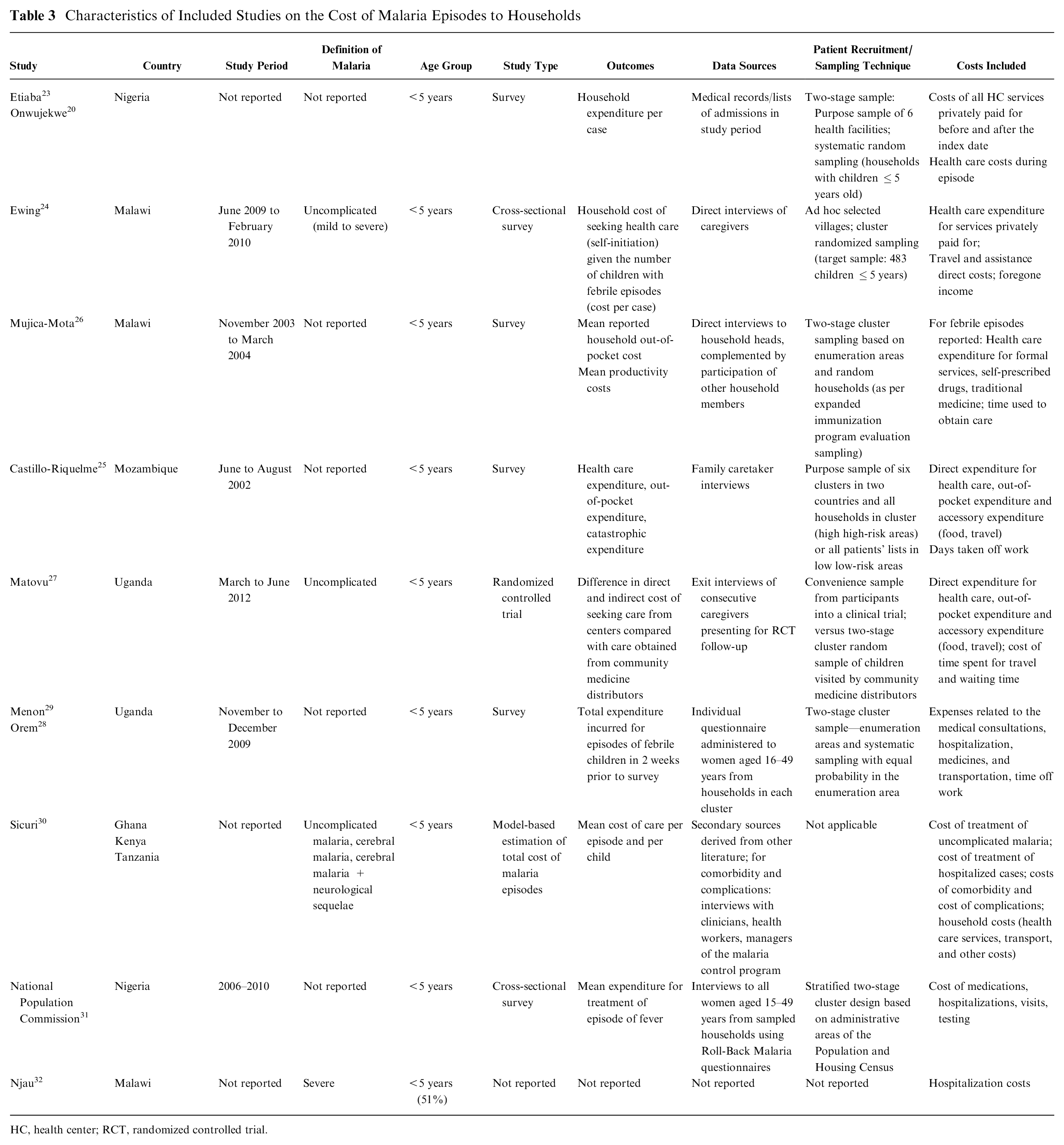
HC, health center; RCT, randomized controlled trial.
Out-of-Pocket Costs Borne by Households
Studies reporting data on health care out-of-pocket costs to households for an episode of malaria are summarized in Table 4. Out-of-pocket costs include direct costs attributed to drugs, consultation, diagnostics and hospitalization, and indirect costs attributed to caregiver transportation.
Out-of-Pocket Costs of Malaria Episodes to Households

CerM, cerebral malaria; CHAM, Christian Health Association of Malawi; IPD, inpatient department; MO, malaria hospitalization; NS, neurological sequelae; SA, severe anemia; UGX, Ugandan shilling; UM, uncomplicated malaria.
Cost data were standardized with US dollars, as calculated for the 2010 price year (Nigeria) and the 2009 price year (Uganda). Nigeria survey data originally reported average cost of treatment to be 871.7 Naira [US$1 = 150.298 Naira (2010)]. Study by Matuvo et al. (2009) 21 originally reported mean travel costs to be 1,417 UGX and 257.9 UGX for urban and rural settings, respectively [US$1 = 2030.488 UGX (2009)]. Exchange rates were obtained from the World Bank data.
The studies reported out-of-pocket payment as cost per episode or as cost per month. Values reported ranged from US$0.23 to US$36.56 per episode and US$0.29 to US$23.43 per month. Although the studies were heterogeneous in malaria severity and cost items reported, some trends were observed. The elements that made the largest contribution to total out-of-pocket costs per episode were transportation and complications in relation to malaria severity.
Transportation costs made the largest contribution to direct costs to households in Malawi, Mozambique, and Uganda. In Mozambique, 25 subjects spent US$7.6 per episode, of which 39% was attributable to medicines and more than half to transport for the sick person and the caregiver. In Malawi, even though consultation is free for children aged <5 years, households incurred costs for transportation to public health facilities. 26 It was also estimated that overall 27% of formal services users with children aged <5 years paid out-of-pocket costs for services received as a result of fever, related either to travel (16%) or medication (11%) costs. Malawian households living in villages far from hospital incurred greater out-of-pocket costs. 24 Travel costs made the largest contribution to direct cost and increased significantly for those living in hard-to-reach villages between the dry and wet seasons (Dry: US$0.36; Wet: US$1.04, P = 0.04). Direct costs for malaria episodes were greater for those living in hard-to-reach locations compared with villages near the hospital in both dry (US$0.44 v. US$0.23, P = 0.04) and wet (US$1.11 v. US$0.47, P = 0.08) seasons. 24 In Uganda, caregivers living in urban areas spent significantly more on transport to reach health centers than those in rural areas. 27 This is because people in urban areas tended to hire motor cycles or public transport vehicles to reach health centers, while those from rural areas walked or used their own (or borrowed) bicycles. On average, caregivers in the urban areas spent four times more than those in rural areas.
Although malaria severity type was not reported by some studies, it was possible to see a trend in out-of-pocket costs associated with hospitalization and treatment. The treatment costs for severe malaria cases were higher and potentially catastrophic to the majority of households particularly in Nigeria, Uganda, Ghana, Kenya, and Tanzania. In a study by Sicuri et al., 30 Ghanaian households needed to support higher direct costs (US$36.56/episode) compared with Tanzania (US$5.46/episode) and Kenya (US$11.83/episode), due to more expensive treatment and higher medical service costs, which include high health personnel salary. For cerebral malaria with neurological sequelae, households in Ghana had the highest direct medical costs (US$40.74) followed by Kenya (US$22.17) and Tanzania (US$8.71). In Nigeria, inpatient costs were greater than outpatient costs averaging to US$12.69 and US$23.43 per episode, respectively. 20 This was due to the cost of hospitalization, special services, comorbidities, and other systemic complications of severe malaria. These complications increase the time spent in hospital, thereby increasing costs. 20 Nigerian households also bear the costs of microscopy tests in inpatient departments. Although the national health insurance scheme was launched in Nigeria years ago to reduce the economic burden of illness borne by individuals, none of the respondents had any form of health insurance. In Uganda, 29 caregivers incurred US$7.58 total costs per episode, and costs were similar at either a private or public health facility. The authors also estimated that among those families with a febrile child who sought care, expenses were 4.3% of an average total monthly income per febrile episode. However, it is not clear whether these costs were largely attributed to medication, diagnostics, or other medical elements.
Non–Health Care Costs Associated With Productivity Loss Due to Malaria and Value of Time Lost to Households Due to Seeking Health Care
Table 5 summarizes information from studies reporting data on productivity loss in monetary value or days and time lost to households due to seeking health care for malaria. Three studies reported monetary value of productivity losses ranging from US$0.43 to US$235.34 per episode.18,33,34 The number of days lost were reported from three studies and ranged from 4.8 to 6 days per episode.15,17,34 Regarding the time spent to seek for health care, two studies reported ranges from 16 to 158 minutes.
Non–Health Care Costs Associated With Productivity Loss for Malaria Episodes and Value of Time Lost to Households Due to Seeking Health Care

This cost represents cost of time caring.
Formal health care facility (hospital inpatient, hospital outpatient, health center, dispensary, and private clinic), informal drug use (drug self-medication, pharmacy/chemist, shop).
Labor substitution is defined as another person doing the job of the sick person.
Two studies24,30 reported information on productivity loss covering Tanzania, Ghana, Kenya, and Malawi. In the study by Sicuri et al., households experiencing cerebral malaria with neurological sequelae in Kenya had the highest economic burden with large productivity losses. Average indirect costs were higher in Kenya, at close to US$8 per uncomplicated episode. This figure fell to US$1.4 in Ghana, where productivity losses were lower due to the lower minimum wage. Indirect costs increased sharply for hospitalized cases, and cases with neurological sequelae had the highest costs: US$77.82, US$99.46, and US$235.23 in Ghana, Tanzania, and Kenya respectively. In Malawi, 24 people living in hard-to-reach villages were less likely to attend a formal health facility compared with those living near the hospital. Hard-to-reach villages were as likely to attend in both dry and wet seasons. Indirect costs represented the main economic burden for households. Most indirect costs were due to time caring at home (Table 5). The cost of time spent caring was greater in hard-to-reach villages (US$4.69) compared with villages near the hospital (US$2.81) in the dry season (P = 0.02), but did not differ significantly in the wet season (P = 0.12). In addition, Malawian carers of feverish young children were as likely to lose earnings in a formal health care facility as in informal care (P = 0.60). It was not possible to make a comparison between Malawi and the other three countries, due to lack of information on malaria-confirmed diagnosis.
Four studies25–27,29 reported information on the time lost to households due to seeking health care, covering Mozambique, Malawi, and Uganda. The number of days lost was higher in Uganda (close to 5 days) than in Mozambique and Malawi (close to 3 days; Table 5). Information on episode duration from Uganda was not reported, so it is not possible to say whether the higher average number of days lost in Uganda could be associated with a longer duration of malaria episodes in Uganda compared with the duration of 6 days in Malawi (Table 5). Travel and waiting times at the facility were longer in Uganda (up to 90 minutes) than in Malawi (up to 30 minutes) regardless of malaria diagnosis and urban/rural setting (Table 5). Households in rural areas in Uganda 27 travelled for significantly longer (P < 0.001), but their waiting time was shorter than for urban households (P < 0.001). The combined effect of travel and waiting time was not significantly different between rural and urban households (P = 0.289). Caregivers travelled an average of 1.5 km to reach a health facility.
Risk of Bias Assessment
Table 6 reports the limitations associated to the studies included in the review.
Identification of Risks of Bias (i.e., Limitations) to the Identified Studies Reporting Resources Use and Cost Data

Potential inaccuracy of the data due to the retrospective design was the most common limitation raised across studies. Data collected might have been overestimated/underestimated as patients and/or caregivers had to recall the cost incurred to treat an episode of malaria. Additionally, most of the studies failed to describe the diagnosis procedure (often due to inadequate documentation) and thus reliability of diagnosis remained questionable.
Discussion
To our knowledge, this is the first systematic review of published cost data on the management of malaria episodes in children aged <5 years in sub-Saharan Africa. Seventeen studies covering nine countries allowed us to understand how malaria is managed in sub-Saharan countries and served to answer the research question of this systematic literature review.
Several studies estimated the cost of a malaria episode in the health system perspective, in inpatient or outpatient settings. These costs varied between the type of facility in which malaria was treated and the severity of malaria.19,27 The mean cost per severe malaria case treated as inpatient was US$60.44 (Min: 18.35; Max: 136.35), with the lowest costs reported from health centers in the Democratic Republic of Congo and highest cost in Ghana hospitals. 10 Regarding outpatient care, the costs reported showed broader disparity with an average cost of US$8.49 and median cost of US$3.46 (Min: 1.94; Max: 31.53).
The current data provide a good level of information on the cost of malaria in some sub-Saharan countries; however, several data gaps were noted. Studies reporting out-of-pocket costs of malaria episodes to households were heterogeneous, covering Nigeria, Mozambique, Malawi, Kenya, Tanzania, Ghana, and Uganda. No studies reported data from other sub-Saharan African countries (i.e., data were missing for more than 20 countries). Furthermore, cost components varied between studies. Only two studies 20 stated clearly how malaria cost was reported (“cost per case of malaria” and “cost per episode per child,” respectively). The lack of a clear case definition was a major limitation when analyzing the data, leading to heterogeneous cost results in different studies. Few studies specified the type of antimalarial treatment assigned to patients. Only Ezenduka et al. 18 and Ferrari et al. 16 clearly reported that participants were either on monotherapy (quinine) or ACTs, with ACTs being more expensive.
It was not possible to make meaningful comparisons between countries and studies. Only one publication, a model-based study, reported cost estimates from several countries obtained using consistent methods and thus allowed direct between-country comparisons. Total costs per episode in this study were lower in Tanzania than in Ghana or Kenya. Most other studies lacked information on malaria severity and the method of diagnosis for malaria treatment within health care facilities, indicating a potentially high incidence of overdiagnosis and overuse of antimalarial drugs.
Ten full publications20,23–31 and one abstract 32 estimated the costs of an episode of malaria to households, covering aspects such as out-of-pocket costs, time lost in travelling to and/or waiting at health care facilities, and productivity costs associated with caring for a child with malaria. Transportation costs made the largest contribution to direct costs to households. Findings illustrate the large economic burden to households for treating one episode of malaria.
It is important to note that household cost studies were mainly relying on the participants’ ability to recall costs accurately, while the provider cost studies relied on formal records. Another important difference relates to the case definition employed. Cost studies conducted at health facilities allow identifying patients who have been medically diagnosed with malaria, although this is not always well stated as mentioned above. In contrast, household surveys may use a less specific diagnosis for recruitment, such as families with a child who has experienced an episode of fever and may therefore include conditions other than malaria.
Despite a policy of free treatment for children aged <5 years at public health facilities in some sub-Saharan African countries such as Malawi, Uganda, Mozambique, and Nigeria, many households still pay for malaria treatment as a result of frequent scarcity of antimalarial drugs in government health facilities, and bear a proportion of diagnosis costs particularly at inpatient departments.20,25 Our review showed that out-of-pocket payments for malaria episodes ranged from US$5.46 in Tanzania to US$36.56/episode in Ghana. Out-of-pocket costs increased sharply in relation to malaria severity and complications. Studies from Nigeria and Kenya implied that most households were uninsured, paying for their health care directly from earnings and savings. In Kenya, all public health facilities charge user fees at the point of care which can be at similar levels to the user fees charged by mission hospitals, and these payments were a major challenge to households.
Our review indicated that the burden on households of transportation to health care facilities varied depending on location and seasonality. Transportation costs were identified for Nigeria, Mozambique, Malawi, and Uganda with the highest burden observed in Mozambique.
Considering the out-of-pocket payments, our findings highlight the potentially catastrophic payments incurred by care for a febrile child in sub-Saharan African countries, which could push households into extreme poverty because of health expenses.
Our review reported that indirect costs related to productivity loss also increased sharply for severe hospitalized cases and cases with neurological sequelae. The number of days lost by caregivers ranged from 3 to 5 days.
Our findings are comparable with other reviews conducted on the economic burden of malaria treatment to households, one of which concluded, For many people in sub-Saharan Africa the costs for the treatment of one case of malaria are such a high percentage of monthly income/expenditure that they lead to (household) catastrophe; on top of this, few countries in sub-Saharan Africa have healthcare insurance or subsidies for malaria treatment available, leading to extra catastrophe; and lastly, not every healthcare facility has appropriate treatment for malaria available, resulting in many ill people receiving incorrect or less effective treatment.
35
Several limitations were noted in the studies included in this systematic literature review. First, some papers did not state the cost base year, an important consideration since prices change over time. When costs were converted, the year of publication was used to inflate and convert cost. This approach might be subject to underestimation or overestimation of costs. Second, there was a lack of information regarding the number of episodes and the definition of an episode of malaria was not always well specified in the publications. Some provided specific information, for example, that an episode was equivalent to having fever 2 weeks prior to data collection,26,29 but the majority did not describe it. As a result, it was not possible to link costs to the treatment of particular symptoms. Some of the studies had a retrospective design, which is a limitation for household studies as people are unlikely to have detailed records of the costs incurred, and their recollections may be incomplete or inaccurate. Information on the duration of malaria episodes was also missing from some studies, so it was not possible to assess whether differences in the number of days lost between countries could be associated with differences in duration of malaria episodes. The systematic review process was also limited as not all languages were included. However, we included studies written in English and French, which decreases the potential for language bias.
Conclusion
The cost to the health system varied from US$1.94 to US$31.53 for outpatient cases to a range of US$18.35 to US$136.35 for inpatient cases. The highest cost was related to severe cases, particularly cerebral malaria cases with neurological sequelae. Families bear a large share of the burden through out-of-pocket payments of medical care and loss in income due to time off work. Overall, the publications identified in this systematic review provided information focused on a small number of sub-Saharan countries with some methodological gaps.
Supplemental Material
3.2_Supplemental_-_PRISMA_checklist_BOI_online_supp – Supplemental material for Economic and Resource Use Associated With Management of Malaria in Children Aged <5 Years in Sub-Saharan Africa: A Systematic Literature Review
Supplemental material, 3.2_Supplemental_-_PRISMA_checklist_BOI_online_supp for Economic and Resource Use Associated With Management of Malaria in Children Aged <5 Years in Sub-Saharan Africa: A Systematic Literature Review by Amira El-Houderi, Joëlle Constantin, Emanuela Castelnuovo and Christophe Sauboin in MDM Policy & Practice
Supplemental Material
Focus_On_Patient_REVISED.rjf_online_supp – Supplemental material for Economic and Resource Use Associated With Management of Malaria in Children Aged <5 Years in Sub-Saharan Africa: A Systematic Literature Review
Supplemental material, Focus_On_Patient_REVISED.rjf_online_supp for Economic and Resource Use Associated With Management of Malaria in Children Aged <5 Years in Sub-Saharan Africa: A Systematic Literature Review by Amira El-Houderi, Joëlle Constantin, Emanuela Castelnuovo and Christophe Sauboin in MDM Policy & Practice
Supplemental Material
Manuscript_REVISED_supplement_PICOS_online_supp – Supplemental material for Economic and Resource Use Associated With Management of Malaria in Children Aged <5 Years in Sub-Saharan Africa: A Systematic Literature Review
Supplemental material, Manuscript_REVISED_supplement_PICOS_online_supp for Economic and Resource Use Associated With Management of Malaria in Children Aged <5 Years in Sub-Saharan Africa: A Systematic Literature Review by Amira El-Houderi, Joëlle Constantin, Emanuela Castelnuovo and Christophe Sauboin in MDM Policy & Practice
Supplemental Material
Manuscript_REVISED_supplement_search_terms_online_supp – Supplemental material for Economic and Resource Use Associated With Management of Malaria in Children Aged <5 Years in Sub-Saharan Africa: A Systematic Literature Review
Supplemental material, Manuscript_REVISED_supplement_search_terms_online_supp for Economic and Resource Use Associated With Management of Malaria in Children Aged <5 Years in Sub-Saharan Africa: A Systematic Literature Review by Amira El-Houderi, Joëlle Constantin, Emanuela Castelnuovo and Christophe Sauboin in MDM Policy & Practice
Footnotes
Acknowledgements
The authors would like to thank Carole Nadin (Fleetwith Ltd, on behalf of GSK) for medical writing assistance and Business & Decision Life Sciences platform for editorial assistance and manuscript coordination, on behalf of GSK. Fabien Debailleul coordinated publication development and editorial support.
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Amira El-Houderi, Joëlle Constantin, and Emanuela Castelnuovo report no conflict of interest. Christophe Sauboin is an employee of the GSK group of companies and holds shares in the GSK group of companies.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: GlaxoSmithKline Biologicals SA (Rixensart, Belgium) funded this study and all costs related to the development of the related publications.
Author Contributions
All authors comply with the ICMJE criteria for authorship. AE-H, EC, and CS were involved in the conception or the design of the study/project. AE-H, JC, and EC participated in the collection or generation of the data. AE-H, JC, EC, and CS performed the study/project. AE-H and CS contributed to the material/analysis tools. AE-H, JC, EC, and CS were involved in the analyses or interpretation of the data. All authors read and approved the final manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.