
Abstract
Introduction:
Like any health care practitioner, dental hygienists can experience mistreatment in the workplace. They can be subjected to harassment, bullying, abuse, and violence. These negative experiences can have adverse consequences on psychological and physical well-being and can lead to job dissatisfaction, depression, and burnout. The aim of this study was to describe dental hygienists’ experiences related to healthy and respectful workplaces.
Methods:
This was an online self-administered survey sent to all members of the Canadian Dental Hygienists Association. Respondents were asked to report the occurrence, frequency, and impact of different types of mistreatment as experienced over their career.
Results:
In total, 3,780 dental hygienists responded to the survey (response rate = 22%). More than 70% of respondents experienced some form of mistreatment over their career from dentists, office managers, coworkers, and/or patients. Of those who experienced mistreatment, 67% reported losing the respect they felt for the offending person, 55% reported experiencing symptoms of depression, and 30% quit their job.
Conclusions:
Mistreatment toward dental hygienists can be prevalent in Canadian dental care settings, resulting in negative consequences to dental hygienists’ well-being.
Knowledge Transfer Statement:
The findings of this article suggest that measures are needed to support healthy and respectful workplaces in Canadian dental care settings. This includes but is not limited to 1) training and education for all members of the dental care team concerning mistreatment, 2) enacting policies in dental care settings to discourage these types of behaviors, and 3) providing help and support to individuals who experience these incidents.
Introduction
Health care practitioners can be susceptible to negative workplace experiences. Working in dynamic settings where interactions with patients and coworkers are frequent may result in unique challenges. According to the World Health Organization (2010), violence in the health care industry can affect employees, colleagues, workplace ambiance, families, and society as a whole (Di Martino 2003). It can result in injury or death and/or psychological harm to the affected person, which itself can lead to exhaustion and/or burnout. Workplace violence, in particular, can lead to a reduction in productivity, increased health care costs, monetary losses to workplaces, and a loss of workdays among employees (Di Martino 2003). In 2016, Boyle and Wallis (2016) proposed a consensus definition of workplace violence that included 6 areas: bullying, verbal abuse, threat, physical abuse, sexual harassment, and sexual abuse. This is similar to categories previously defined in a systematic review of occupational mistreatment within oral health care settings (i.e., harassment, bullying, violence, and abuse), which can affect dentists, dental hygienists, dental assistants, and dental administrators, as well as patients, families, and communities (Binmadi and Alblowi 2019).
Dental hygienists represent the majority of all oral health care workers in Canada. According to the Canadian Institute for Health Information, in 2018, there were 29,251 dental hygienists eligible to practice (compared to 16,868 dental assistants and 24,731 dentists), with over 95% being female (Canadian Institute for Health Information 2016). Dental hygienists work in a variety of practice environments, such as private and public clinics, long-term care, and hospitals, where any number of potential factors can contribute to an unhealthy workplace (Canadian Dental Hygienists Association 2003). Most dental hygienists work directly with patients and dental care teams in fast-paced settings, which can produce stressful environments, in turn affecting psychological well-being and eventually leading to worker attrition (Gorter 2005; Jeon et al. 2017).
Research on dental care teams in the United States has shown that among dental hygienists who were predominantly female, sexual harassment and bullying were the most common types of workplace violence, and in many cases, the outcome of such incidents led to actions that negatively affected the dental hygienist’s career (Garvin and Sledge 1992; Pennington et al. 2000; McCombs et al. 2018). In some cases, no action was taken following the workplace incident, and no workplace policies appeared to be in place to manage such incidents (Garvin and Sledge 1992; Binmadi and Alblowi 2019). International research on workplace violence among health care practitioners in various fields shows similar results, with factors such as the age, sex, occupation, and work hours of the health care practitioner and the characteristics of the health care institution and system being independent determinants of experiencing workplace violence (Lahari et al. 2012; Abdellah and Salama 2017; Pinar et al. 2017; Norton et al. 2017). Workload pressures, occupational stress, and organizational culture are also known to be contributing factors to workplace violence (Sanders and Turcotte 2010; Carter et al. 2013; Berthelsen et al. 2017). Importantly, health care practitioners who experienced workplace violence report impaired job performance, fear, psychological issues, and lower levels of job satisfaction (Azodo et al. 2011). These health care practitioners are also more likely to report planning a decrease in work hours and engaging in direct patient care (Azodo et al. 2011; Askew et al. 2012). In addition, negative work environments are known to affect the quality of patient care and patient safety culture (Candell and Engström 2010; Choi et al. 2019).
Strategies to support healthy and respectful workplaces include establishing formal policies on all aspects of workplace violence (Binmadi and Alblowi 2019; Sundburg 2019). A clear message of no tolerance can deter negative behaviors among health care teams and patients, as well as supports self-efficacy to act in response to any mistreatment (Binmadi and Alblowi 2019; Sundburg 2019). However, in Canada, details on the experiences of dental hygienists and their workplace environments are not well known. This knowledge is essential to developing strategies to promote healthy and respectful workplaces.
This article reports on an analysis of survey data collected with the aim of describing dental hygienists’ experiences related to healthy and respectful workplaces. Specifically, the objectives are to 1) understand the scope of issues related to healthy and respectful workplaces; 2) determine the prevalence and frequency of workplace issues related to harassment, bullying, and abusive and violent behaviors; and 3) explore the factors associated with these experiences.
Methods
Study Design
In the fall of 2018, the Canadian Dental Hygienists Association (CDHA)—the national professional organization for dental hygienists in Canada—undertook a cross-sectional survey to understand workplace issues experienced by dental hygienists. The CDHA contracted the researchers (AG, KKP, JF, CQ) to conduct an analysis of the CDHA survey data. An ethical review for the analysis was obtained from the Research Ethics Board (protocol number 39694).
Survey Development and Administration
A 72-item questionnaire was prepared by a private consulting firm (Harry Cummings and Associates Inc.) in consultation with a panel of dental hygienists and CDHA staff between September and October 2018. This ensured that questions and concepts used in the survey were relevant to the profession and comprehensive in examining a broad scope of workplace harassment, bullying, abuse and violence issues within the Canadian context. The survey was piloted with a random sample of eleven CDHA members to assess face validity, ease of completion, relevance of the material, and the appropriateness of the language used. Minor modifications were made as needed. The survey was then initiated on November 13, 2018, and 3 reminder notices were sent out before the survey was closed on December 17, 2018. This was an electronic survey administered through a web-based survey platform.
The terms used to describe and discuss mistreatment in the workplace can be confusing and used incorrectly and interchangeably. The full definitions of the terms used in this study are presented in Appendix 1 and were provided to the survey participants as a guide. This helped to preserve meaning and ensure the accuracy of statements. The definitions were adapted from various sources, such as the Canadian Centre for Occupational Health and Safety (Government of Canada 2020), WorkSafe British Columbia (2021), the Alberta Occupational Health and Safety Act (Government of Alberta 2012), and the Ontario Occupational Health and Safety Act (Government of Ontario 2020). In this article, the term mistreatment is used to denote any form of workplace harassment, bullying, abuse, or violence.
Sample Description and Recruitment
All CDHA members with an active email address were invited to participate in the survey. Members with student memberships were excluded, as the survey questions did not pertain to them. No further inclusion or exclusion criteria were employed. The invitation email was sent out to all dental hygienists regardless of their practice setting (clinical or alternative), working capacity (full-time, part-time, or temporary), or current registration status with a dental hygiene regulatory authority in Canada (practicing or retired). No written informed consent was obtained from participants, as responding to the survey was taken to imply consent.
Study Outcome Measures
The outcomes of interest were the prevalence and frequency of experiencing harassment, bullying, abuse, and/or violence. Participants were asked, “Over the course of your career as a dental hygienist, have you personally experienced any acts of harassment, bullying, abuse or violence from dentists/office managers/coworkers/patients in your workplace(s)?” This outcome was dichotomized as “yes” or “no” based on responses to 4 separate questions, each addressing one of the following: dentists, office managers, coworkers, and patients.
Those who answered “yes” to experiencing harassment, bullying, abuse, or violence were then asked a follow-up question: “How would you classify the frequency of harassment and/or bullying that you have experienced from dentists/office managers/coworkers/patients in your workplace(s)?” The responses were “never,” “rarely,” “occasionally,” “repeatedly,” or “constantly” in 3 time periods: “within the past 12 months,” “1 to 2 years ago,” and “3 years ago or longer.” A similar question was asked to classify the frequency of abuse and/or violence experienced by dentists/office managers/coworkers/patients in their workplace(s).
The survey also asked about whether the respondents had witnessed mistreatment happen to a coworker, information about the impacts of experiencing mistreatment, and their response to these acts. Additional questions about the adequacy of workplace policies, reasons not to address/resolve incidents of workplace mistreatment, and dental hygienists’ opinions about aspects in the workplace that should be prioritized when addressing these issues were also explored.
Demographic and Practice-Related Variables
Sociodemographic (e.g., age, gender, Indigenous identity) and other practice-related variables (e.g., years of experience, practice setting and location) were collected. Due to the small sample sizes in some of the categories, we decided to recategorize some of the variables as outlined in Appendix 2.
Statistical Analysis
Descriptive statistics were performed to estimate the frequency and proportion of the variables explored in this study. Chi-square tests of independence were used to examine the relationship between the occurrence of mistreatment in the workplace (over the lifetime career of the dental hygienist) and various demographic and practice-related variables. All statistical analysis was performed using SPSS version 23.0 (SPSS, Inc.), and the level of statistical significance was set at P < 0.05.
Results
The survey was sent to 17,030 members of the CDHA and completed by 3,780 dental hygienists (22% response rate). The majority were female, had a dental hygiene diploma, and had practiced for more than 20 y (Table 1). Fourteen percent and 2% of respondents self-identified as a visible minority or Indigenous, respectively. The 3 most represented provinces included Ontario, followed by Alberta and British Columbia. Most respondents practiced in a clinical setting, in a large city with a full-time single-position job. All provinces and territories were represented among survey respondents, and the share of responses from each province/territory was similar to the distribution of the entire membership. The sociodemographic and clinical characteristics (age, gender, years of experience, highest level of education) of the respondents were also similar to the profile of respondents in the CDHA’s 2019 Job Market and Employment Survey (data not shown).
Dental Hygiene Participant Characteristics and Workplace Policies and Features.
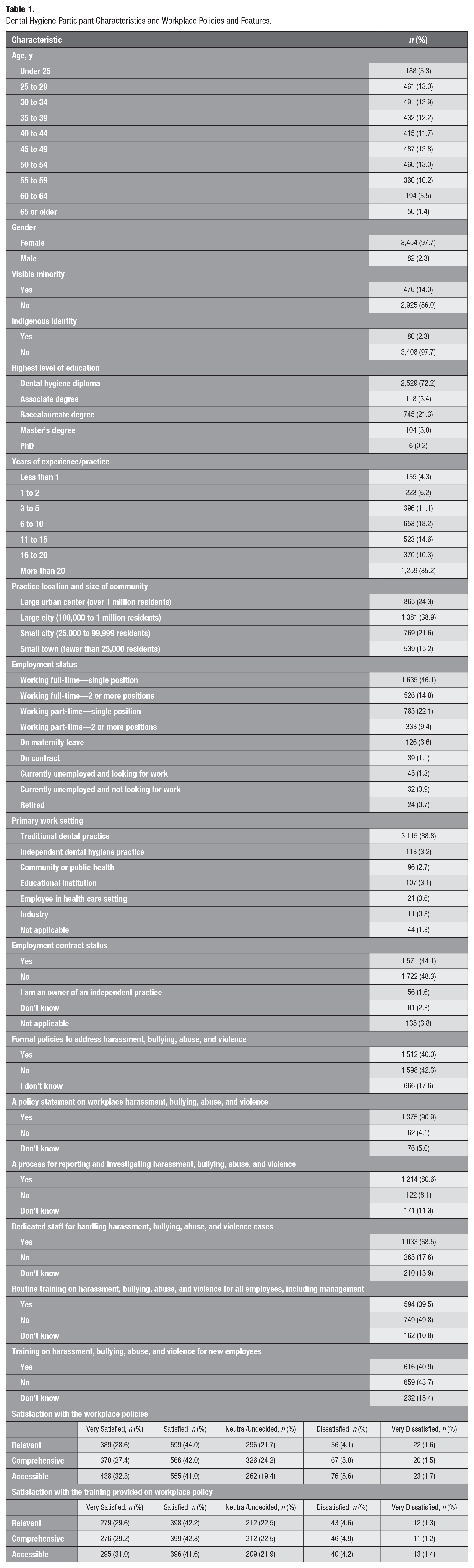
Approximately half of the respondents (48%) reported not having a written contract with their employer. Most respondents reported either not having (42%) or were unaware (18%) of the presence of formal measures/policies to address issues of harassment, bullying, abuse, or violence in their workplace. Similarly, almost half of respondents (44%) did not believe their workplace offered training for new employees regarding these issues. Of the respondents who confirmed having a formal workplace policy statement in place, approximately 70% reported that they were satisfied or very satisfied with these measures in terms of being relevant, comprehensive, and accessible. Similarly, most dental hygienists (72%) who received training on the workplace policy reported that they were satisfied or very satisfied with the training in terms of relevance, comprehensiveness, and accessibility.
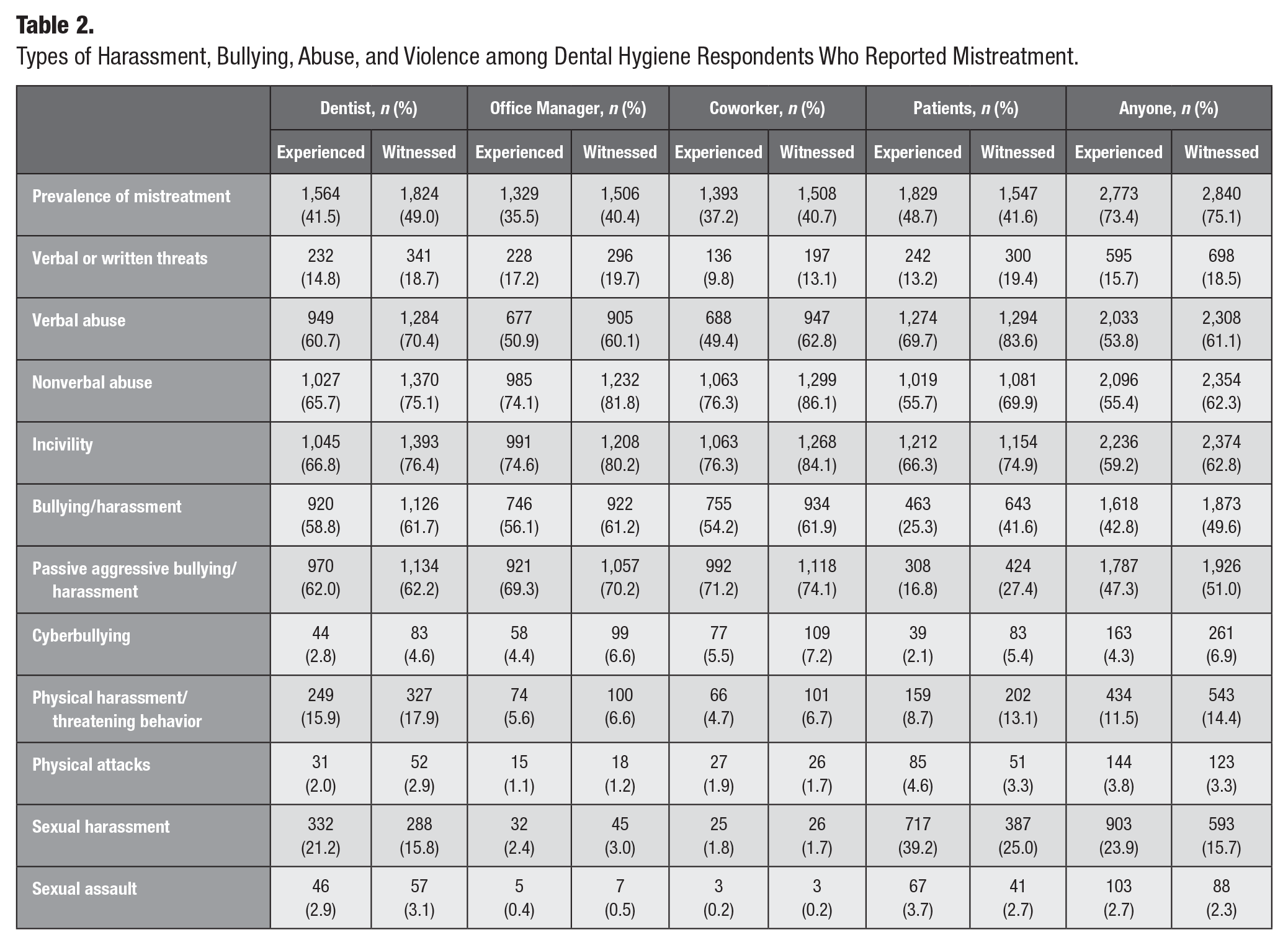
Instances of harassment and bullying among survey respondents were common in the dental care setting (Table 2). Approximately 42%, 36%, and 37% of participants reported experiencing a form of mistreatment in their workplace from dentists, office managers, and coworkers, respectively. Nearly half (49%) of respondents experienced a form of mistreatment from patients. Almost three-quarters (73%) of respondents reported being mistreated by a dentist, office manager, coworker, or patient at least once in their career. Incivility, verbal and nonverbal abuse, harassment, and bullying (including passive-aggressive behavior) were the most reported forms of mistreatment. It was interesting to note that while physical and sexual harassment were reported less often than other forms of mistreatment (<25% of respondents), this was predominately experienced from dentists and patients.
Types of Harassment, Bullying, Abuse, and Violence among Dental Hygiene Respondents Who Reported Mistreatment.
Many reasons were attributed to not taking action in response to mistreatment. More than two-thirds of respondents (70%) who experienced mistreatment refrained from taking action due to fear of retaliation and/or losing their job (Table 3). Other less commonly reported reasons were concerns about the seriousness of the complaint process; doubt about whether the experience would be considered harassment, bullying, or abuse; and concerns about the adequacy of the complaint procedures in place. Over 50% of those who experienced mistreatment reported having symptoms of stress, 52% considered quitting their jobs, 67% reported losing respect for their employer, and 30% resigned or quit their job (Table 3).
Reasons Contributing to Not Taking Action to Address/Resolve an Incident of Harassment, Bullying, Abuse, and Violence among Dental Hygiene Respondents and the Prevalence of Impacts Due to Mistreatment in the Workplace.
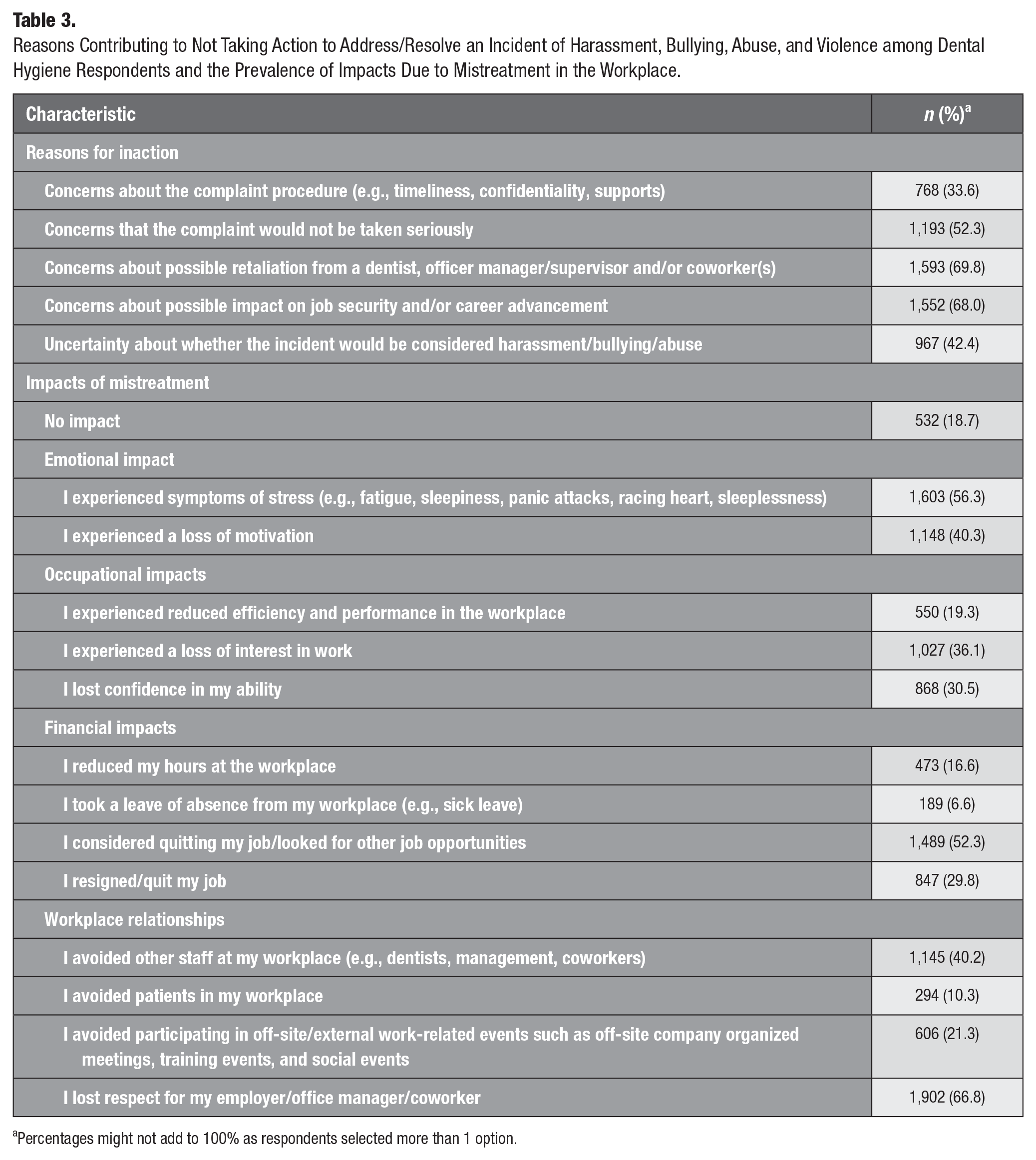
Percentages might not add to 100% as respondents selected more than 1 option.
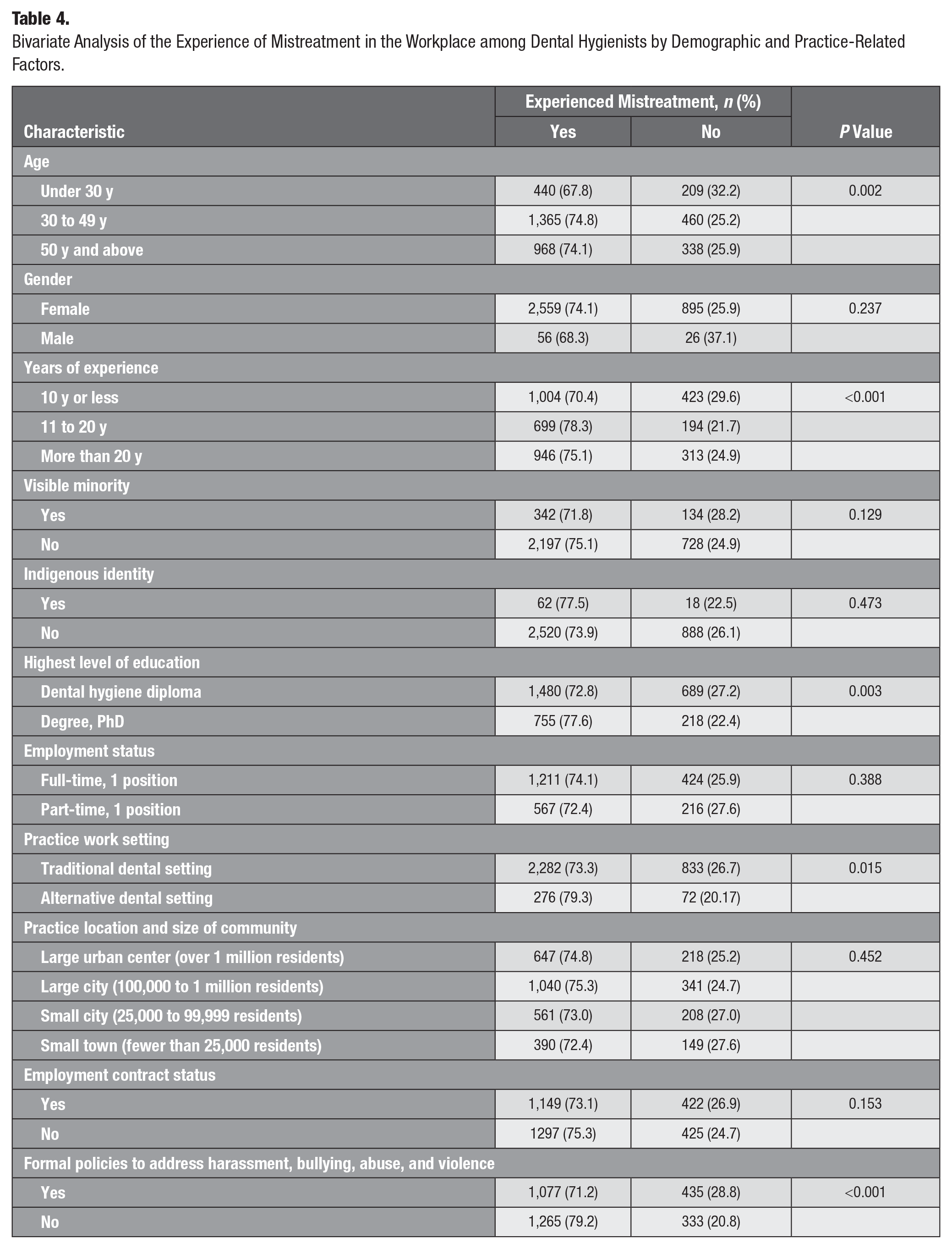
The bivariate analysis demonstrated statistically significant differences in the demographic and practice-related variables, including age (P = 0.002), years of experience (P < 0.001), level of education (P = 0.003), workplace setting (P = 0.015), presence of harassment policies in the workplace (P < 0.001), and experiencing mistreatment over one’s career (Table 4). Older dental hygienists and those with more years of experience and education appeared to more frequently experience workplace mistreatment than their younger, less experienced and educated peers. Those who worked in alternative practice settings (e.g., educational institution) or who reported not having policies to address incidents of mistreatment reported experiencing these negative acts more frequently compared to their colleagues who practiced in clinical settings or who had mistreatment policies in place.
Bivariate Analysis of the Experience of Mistreatment in the Workplace among Dental Hygienists by Demographic and Practice-Related Factors.
Discussion
This was a descriptive cross-sectional study aimed at gauging the prevalence, frequency, and types of mistreatment experienced by dental hygienists in Canada. Harassment, bullying, abuse, and violence appear to be prevalent issues affecting more than 70% of dental hygienists in Canada. When comparing our estimates to that of nursing, a profession that arguably resembles dental hygiene (Taylor 2016), we find similar results. According to a study published by the Canadian Federation Health Union, 61% of nurses said they had experienced abuse, harassment, or assault in their workplace in the past 12 mo (Reichert 2017). Other professionals are also not immune to such mistreatment in their workplace. For example, in an international survey of lawyers from 135 countries, bullying in the workplace was reported by 1 out of every 2 female respondents and by 1 in 3 male respondents (Pender 2019). Sexual harassment was also prevalent, with one-third of female respondents and 7% of male respondents reporting being sexually harassed at work. These issues exist in the general working population as well. According to the General Social Survey on Canadians at Work and Home (GSS), 19% and 13% of female and male workers, respectively, reported experiencing workplace harassment in the past year (Hang and Moyser 2018). The report also revealed that health care sector practitioners experienced significantly higher levels of violence and abuse compared to others in the workforce (Hang and Moyser 2018). Ultimately, workplace mistreatment represents an occupational stressor, which, in our case, places significant strain on dental hygienists’ physical and psychological health, leading to adverse outcomes.
Interestingly, previous surveys of US dental hygienists suggest significantly lower rates of workplace bullying than the ones reported in our study. For instance, McCombs et al. (2018) reported that 1 in every 4 Virginia dental hygienists reported experiencing workplace bullying. Likewise, in a national survey, Sundburg (2019) reported that 1 in every 4 dental hygienists in the United States met the criteria for being bullied in the workplace. These authors also reported that dental hygienists with less experience (5 to 10 y of experience) were more likely to report these negative acts. Our findings also do not corroborate results from McCombs et al. (2018) suggesting that experienced hygienists are less likely to experience mistreatment than their less experienced peers.
One potential explanation for our findings is that, as employees spend more time in practice, they might expect more respectful treatment from employers and coworkers, resulting in less tolerance for behaviors thought to be acceptable in the past (Einarsen and Skogstad 1996). Also, our findings support the need for written policies in the workplace as described by McCombs et al. (2018). Having these measures conveys a sense of accountability to all members of the dental team and increases the odds of feeling supported when such events take place.
Our findings identified a range of negative impacts experienced by dental hygienists due to mistreatment in the workplace. A large proportion who experienced mistreatment reported emotional and financial impacts as well as changes in workplace relationships. Prior research has identified job change and negative job satisfaction as a consequence of negative workplace experiences (Yee et al. 2005; McCombs et al. 2018). These findings thus reinforce the need and role of employers and coworkers in promoting wellness in the workplace (Grawitch et al. 2006).
All members of the dental care team should be treated with dignity and respect. Environments that are free of harassment, bullying, abuse, and violence foster a respectful and safe working environment. They contribute to one’s self-worth and to positive interpersonal relationships that ultimately improve the quality of patient care. The findings from this study highlight the need to adopt measures to address these problems. First and foremost, it is crucial for every workplace to establish and/or strengthen policies that address these negative behaviors. Second, employers should ensure that each office/workplace has personnel who dental hygienists can approach when seeking help regarding these issues. Third, all employees must receive adequate training on how to prevent these behaviors in the workplace. Not only may this increase awareness about mistreatment in the workplace, but it may also propagate a sense of security that will encourage those who have encountered mistreatment to bring their concerns forward. Finally, in the case of an incident, dental hygienists should be provided with support services that allows them to overcome this experience and reintegrate into the dental office and/or workforce. In fact, many subnational, national, and international organizations have published resources to help health care employers with developing a healthy workplace environment (Health and Safety Ontario 2011).
Strengths and Limitations
This study has several strengths. To our knowledge, it is the first to describe the extent of harassment, abuse, bullying, and/or violence among dental hygienists in Canada. Thus, it is a foundation for future research to explore similar or related issues. Our survey also yielded a relatively acceptable response rate (22%) considering the historically low and declining response rates among health care professionals, which averages at roughly 11% to 42% (Hardigan et al. 2012; Funkhouser et al. 2017). In terms of limitations, our survey did not incorporate questions about job satisfaction, coping mechanisms such as the use of alcohol or illicit drugs, or other non-work-related factors (e.g., relationships with friends and family) that could alter a person’s experience with these behaviors (Bidwal et al. 2015; Koinis et al. 2015). These are significant factors that ought to be considered when exploring these issues in future research. Also, the survey questions used in this study were different from other studies done in this field, limiting our ability to compare the findings across different jurisdictions and time periods. Furthermore, our analysis is based on self-reported data that rely on the participant’s ability to recall incidents that happened over their career. Recalling episodes that could have happened months or years ago could be challenging and can introduce an unknown estimate of recall bias. This could result in an over- or underestimate of our outcomes. Finally, we were not able to compare the sociodemographic characteristics (age, gender, years of experience, educational attainment, etc.) of our sample population to the overall population of dental hygienists in Canada, as these data were unavailable. Thus, we were unable to assess if survey respondents differed from nonrespondents in a way that is important to the study (i.e., nonresponse bias) (Dillman et al. 2014). However, the general characteristics of our survey sample are consistent with previously conducted surveys by the CDHA, which may suggest that nonresponse bias in our study is minimal. Nonetheless, caution should be taken when generalizing the findings from this survey to the entire population of dental hygienists in Canada.
Conclusion
Harassment, bullying, abuse, and violence are prevalent issues that affect a significant proportion of dental hygienists in Canada. These problems have serious implications that threaten the psychological and physical well-being of dental hygienists, as well as the productivity of oral health care settings. Recognizing the significance of these alarming behaviors is the first step in establishing a healthy and respectful workplace that fosters optimal patient care.
Supplemental Material
sj-pdf-1-jct-10.1177_23800844211001827 – Supplemental material for Healthy and Respectful Workplaces: The Experiences of Dental Hygienists in Canada
Supplemental material, sj-pdf-1-jct-10.1177_23800844211001827 for Healthy and Respectful Workplaces: The Experiences of Dental Hygienists in Canada by A. Ghoneim, K.K. Parbhakar, J. Farmer and C. Quiñonez in JDR Clinical & Translational Research
Footnotes
Author Contributions
A. Ghoneim, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; K.K. Parbhakar, contributed to conception, design, data acquisition, and analysis, drafted and critically revised the manuscript; J. Farmer, contributed to conception, design, data acquisition, and analysis, critically revised the manuscript; C. Quiñonez, contributed to conception, design, data acquisition, analysis, and interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was provided by the Canadian Dental Hygienists Association (CDHA).
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.