
Abstract
Background:
There has been much research relating to stressors in the dental environment and concerns over dentists’ health and wellbeing. The determinants of dentists’ health and wellbeing within the UK include macro-factors, such as healthcare systems and regulation; meso-factors, such as job specification and workplace characteristics; and micro-factors, such as personal aspects, professional career level, and personal and professional relationships. Given the challenges in dentistry, research is needed to investigate the key determinants relating to the health and wellbeing of clinical dental care professionals (DCPs) nationally.
Aim:
To review the literature on the key determinants of health and wellbeing among dental hygienists, dental therapists, clinical dental technicians, and orthodontic therapists in the UK.
Materials and methods:
A systematic review of the literature was conducted across seven databases. The records were screened by title, abstract and full text based on the study inclusion criteria. Extraction of data and a qualitative synthesis of the included studies was performed. A mixed methods appraisal tool was used to quality assess for risk of bias.
Results:
Twelve studies were included in this review, eleven of which were medium to high quality (5*, 4*) and one low quality (2*). Ten studies focused on dental therapists, and/or hygienists, with only one each on orthodontic therapists and clinical dental technicians. Job satisfaction and professional careers were the primary factors explored in the included studies and clearly identified as determinants of health and wellbeing. However, there was evidence of these being associated and linked with a range of determinants at macro-, meso-, and micro-levels, with a general lack of evidence on the overall health and wellbeing.
Conclusion:
There is currently very limited evidence on the key determinants of health and wellbeing of clinical DCPs within the UK, but the available evidence maps to the same domains as dentists. Further well conducted research examining the overall health and wellbeing is required, with consideration of the full matrix of possible factors.
Learning Objectives
To report evidence of macro-, meso-, and micro factors impacting health and wellbeing of clinical dental care professionals
To highlight the need for further research
To signpost available health and wellbeing resources
Introduction
The dental team in the UK is diverse and professionalised. 1 Current evidence exploring the health and wellbeing of the dental workforce, largely focuses on dentists.2-4 Indicators of psychological distress, including depression, burnout and stress, are commonly noted by the dental workforce, which is concerning from a workforce perspective as the dental team practice in a field which is known to have high occupation-stress and suicide rates. 5 The health and wellbeing of clinical dental care professionals (DCPs) is also equally important from a patient care perspective as it directly impacts on quality and continuity of care, due to known influences on clinician−patient relationship, working patterns, and early retirement plans.6,7 As the health of individuals and communities is closely linked to their circumstances and the environment in which they live, 8 there are many combined factors that impact the health and wellbeing of individuals. The World Health Organization (WHO) states that the socio-economic and physical environment, as well as the characteristics and behaviours of individuals are all determinants of health. 8 In this regard, the body of evidence among dentists in the UK suggests that their health and wellbeing is associated with a wide range of determinants: from macro-level factors including professional regulation and system, to meso-level involving workplace and job specification, to micro-level involving personal factors, professional and social relationships, and professional careers.2-4 Furthermore, evidence suggests that having a significant NHS care commitment may impact on health and wellbeing.2-4
Given the evidence regarding dentists, there is a need for an equivalent review exploring the determinants of health and wellbeing of other clinical members of the dental team. Thus, this review exclusively focuses on dental hygienists, dental therapists, orthodontic therapists, and clinical dental technicians. It aims to examine the literature on the key determinants of the health and wellbeing of these clinical DCPs.
Methods
This systematic review followed a series of key steps starting with defining the review question and developing the inclusion criteria. This review followed the PEO framework defining the population/problem, the exposure, and the outcome. The key terms were combined to identify relevant studies. A detailed representation of the search terms and the search strategy used can be seen in Table 1.
search strategy and Inclusion and exclusion criteria
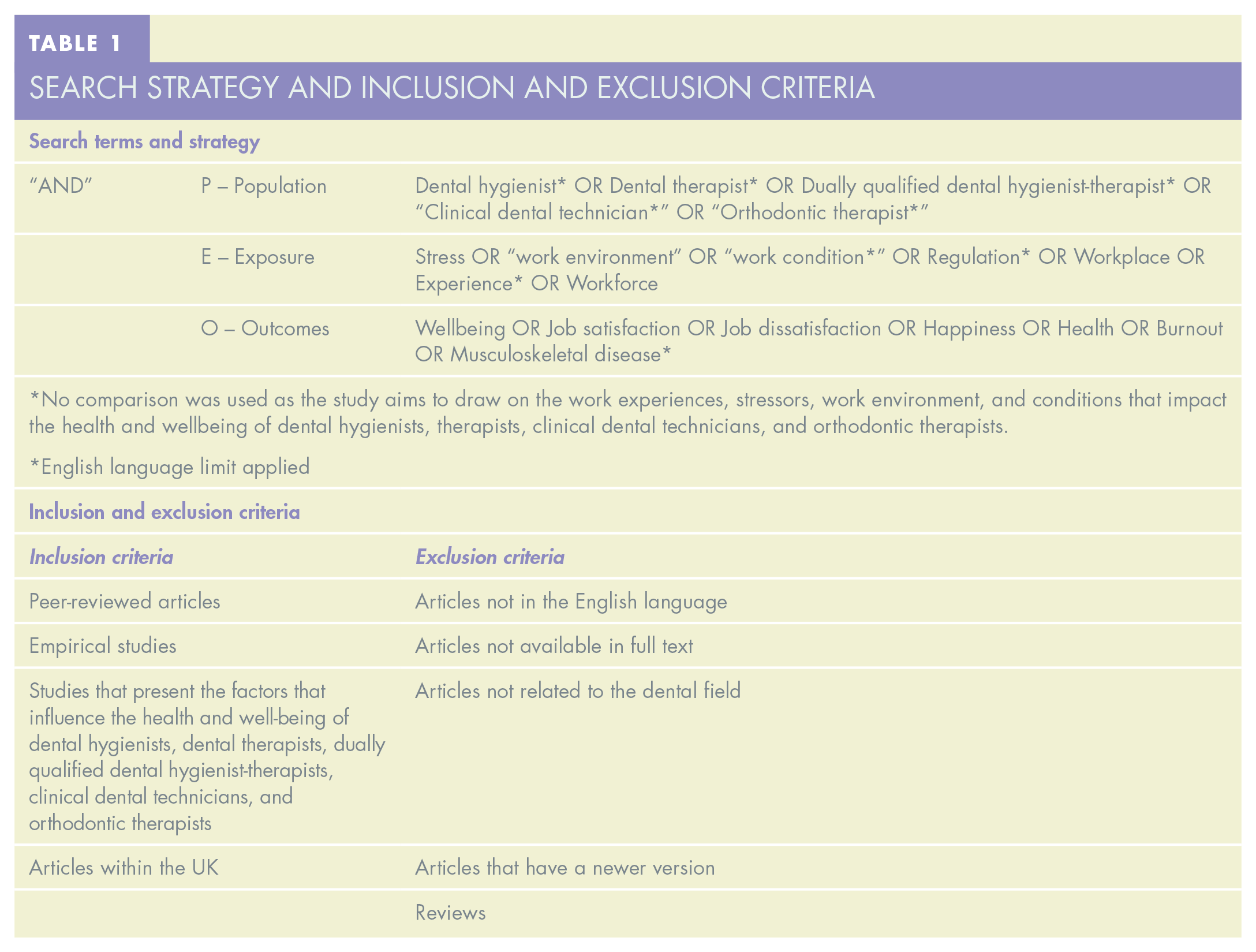
An electronic search was performed across seven health and social science databases: PubMed, Ovid (Embase, Medline® and Psycinfo), Cochrane, Web of Science, and Google Scholar. Records identified were downloaded to Rayyan® software (Rayyan Systems Inc., Cambridge, Massachusetts, USA) to be screened and duplicates were removed. Studies were then screened by two reviewers (LK, SK) separately based on title and abstract. Articles were potentially included based on the inclusion criteria described in Table 1. Full texts for all selected articles were obtained and reviewed by the first reviewer (LK), then checked by the second reviewer (SK). Differences were resolved by discussion in consultation with a third reviewer (JEG) where necessary.
The data from the studies that met the inclusion criteria were extracted by the first reviewer (LK) into a Microsoft Excel spreadsheet and were checked/revised by the second reviewer (SK). Any areas of disagreement were resolved by discussion with the third reviewer (JEG). The data were then analysed qualitatively and reported by themes. The framework by Colonio-Salazar et al. (2019) was used to identify the key themes. 2
Studies were assessed according to the Mixed Methods Appraisal Tool (MMAT). 9 The MMAT was utilised as it provides a methodological quality criterion for different study designs in one single tool, thereby allowing a direct comparison of quality of evidence in the different types of studies included. In addition, it has a limited number of core criteria, which allows for more efficient, yet detailed appraisal of articles.
Results
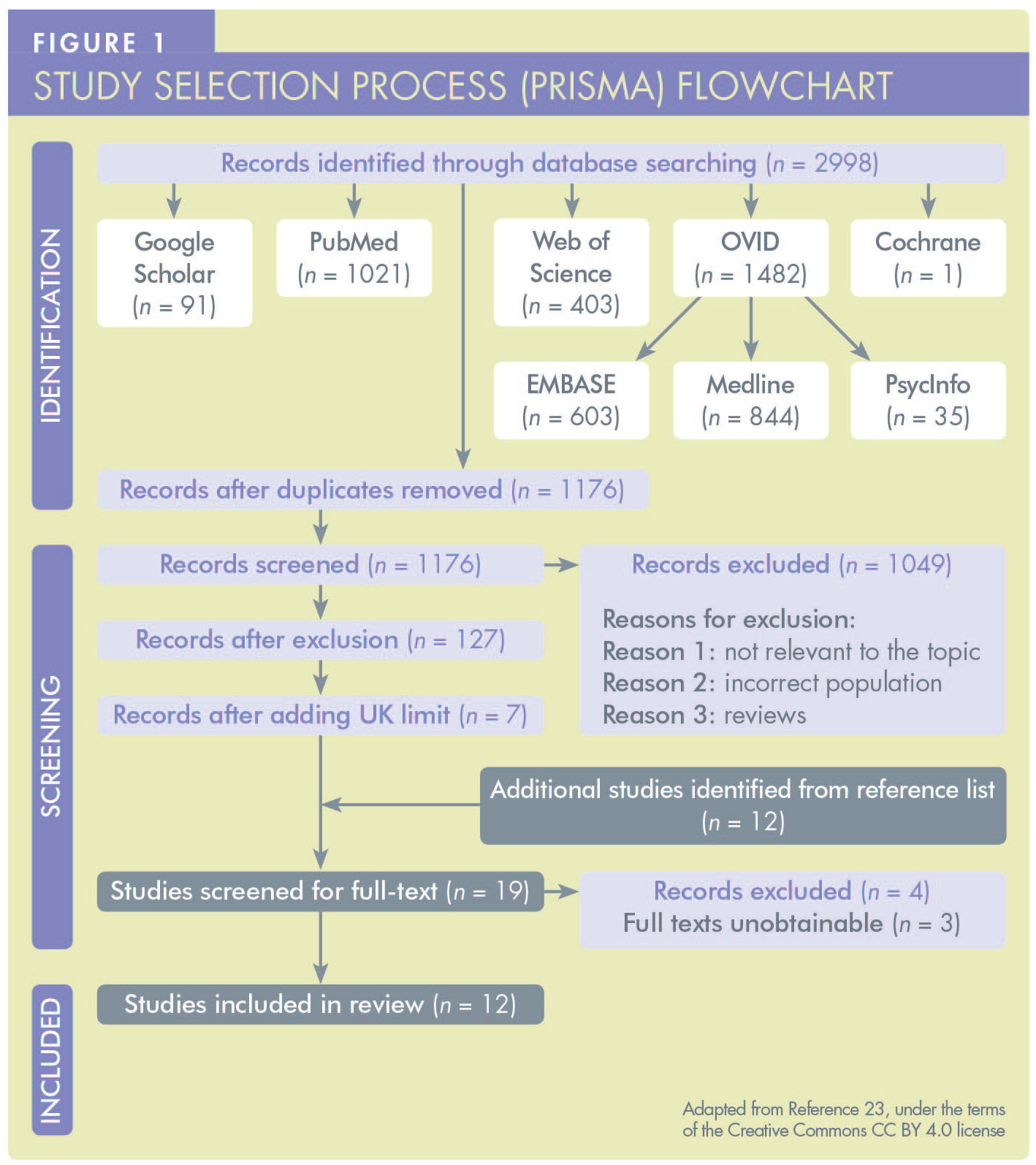
The electronic database search yielded 2,998 citations. After duplicates were removed, it resulted in 1,176 citations which were screened by title and abstract. One hundred and twenty-seven studies were included for full-text screening. A UK limit was applied afterwards to meet the aim of this study; broad search terms were initially used to assure that all relevant research was captured. Twelve studies met the inclusion criteria and were included in this review. A detailed presentation of the process of identifying the studies can be seen in the PRISMA flow chart presented in Figure 1.
While most studies were UK-wide,10-19 two were restricted to England only,20,21 and a final study provided comparative evidence of the dental workforce within the UK, New Zealand, and Trinidad and Tobago. 14 However, in the case of the latter paper, only evidence within the UK was considered for the review.
The included studies covered the following professional groups: dental hygienists, dental therapists, dually qualified dental hygienist-therapists, clinical dental technicians, and orthodontic therapists. Five studies focused on dental therapists (including dually qualified dental hygienist-therapists).10,11,13,14,19 Two studies were specific to dental hygienists.12,21 One study focused exclusively on dually qualified dental hygienist-therapists. 18 One study compared job satisfaction between dental hygienists, dental therapists, and dental practitioners, 15 and another focused on both dental hygienists and dental therapists (including dually qualified dental hygienist-therapists) providing ‘direct access’ care. 17 Finally, one study focused on orthodontic therapists only, 16 while another focused on clinical dental technicians. 20
The majority were quantitative studies involving questionnaires, while one was qualitative. The questionnaires used varied across the studies. The study conducted by Onabolu et al. (2018), used a questionnaire that was based on the Gallagher Motivation Instrument (GMI). 16 Two studies11,12 used a survey questionnaire based on the original tool used by McEwen and Seward. 22 The remaining quantitative descriptive studies did not report the instrument used.
Dental hygienists, dental therapists, dually qualified dental hygienist-therapists, and orthodontic therapists were mostly female, while clinical dental technicians were mostly male. The sampling frame used by most studies was the General Dental Council (GDC) register.
The studies were generally 5*11,12,18,20,21 or 4*,10,13-16,19 rated using the MMAT. One study had a rating of 2* due to low participant response rate associated with a selective sampling strategy which involved a Google search to identify participants, inclusion of only one representative from practices where multiple DCPs were employed, and due to the use of a non-validated instrument. 17 Generally, studies had clear research questions and an appropriate data collection method. Recruitment of participants was mainly through identification from the GDC list, except for two studies.17,21
Health and wellbeing
There is very limited information regarding the overall health and wellbeing of clinical DCPs. However, the studies included macro-, meso-, and micro-level factors relating to job wellbeing and their professional careers. The key determinants of health and wellbeing, following Colonio-Salazar et al. (2019), 2 are demonstrated in Table 2 at three levels from macro-, to meso- and micro-level factors. The main challenges faced by these clinical DCPs and the key findings are presented below.
Determinants of the Health and Wellbeing of Clinical DCPs
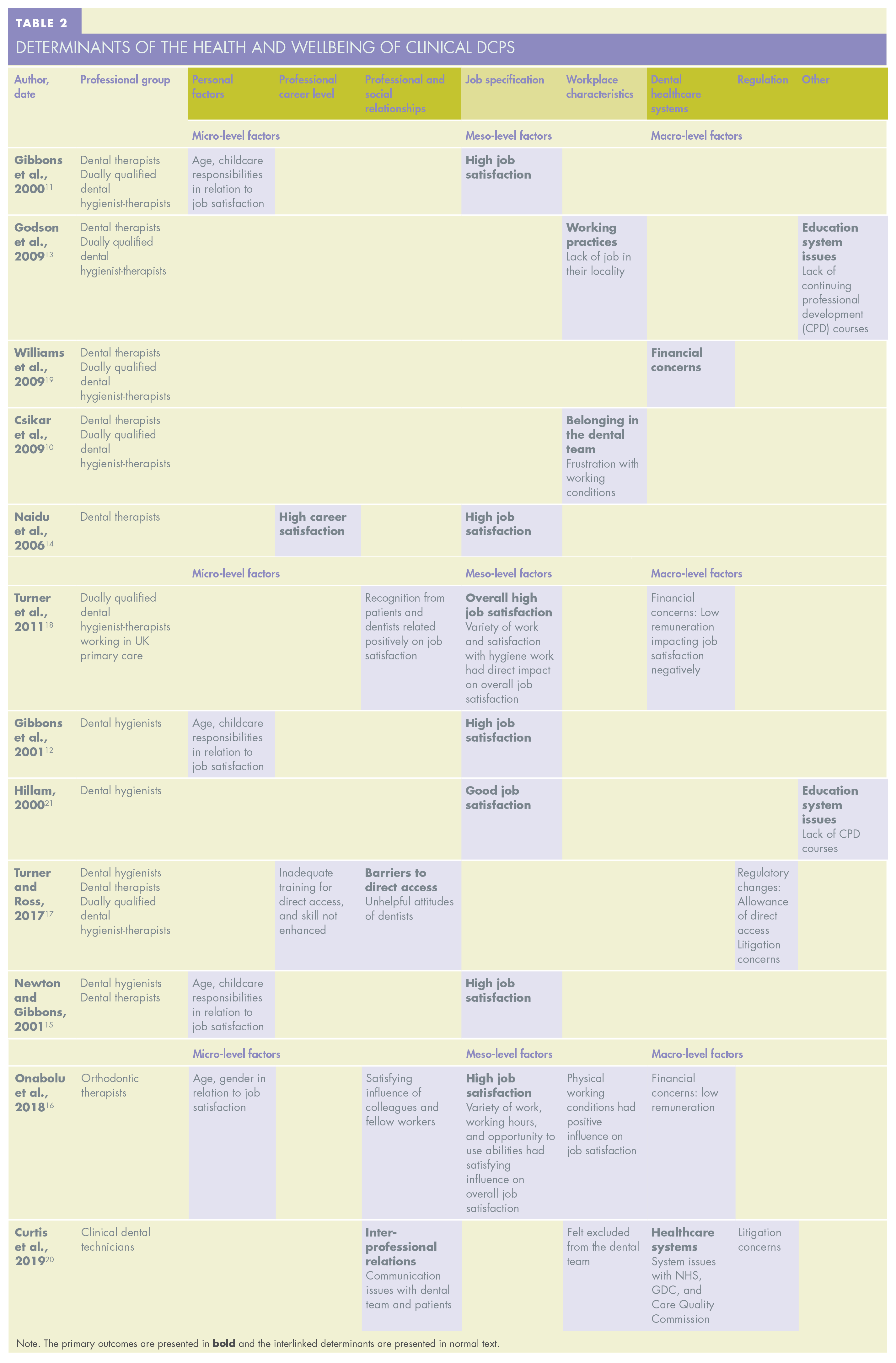
Note. The primary outcomes are presented in
Personal factors
Although we aimed to explore personal factors in relation to overall health and wellbeing, the included papers investigated personal factors in relation to job satisfaction only. Four out of the 12 studies reported several factors associated with job wellbeing, most notably age, gender, and childcare responsibilities.11,12,15,16
Age
Four studies discussed age in relation to job satisfaction.11,12,15,16 Overall, the evidence on job satisfaction relating to age for different clinical DCP groups showed that older hygienists (> 37 years old) reported higher job satisfaction than younger age groups.12,15 Similar results were also noted for the dental therapists, with older therapists (> 44 years old) reporting greater job satisfaction than younger age groups.11,15 However, there was no difference in age-related job satisfaction for orthodontic therapists. 16 Although Gibbons et al. (2000) included dually qualified dental hygienist-therapists, no separate data in age-related job satisfaction was reported for this group. 11 Therefore, across the papers which looked at job satisfaction in relation to age, dental hygienists and dental therapists who are generally older showed higher job satisfaction. No difference was noted for orthodontic therapists.
Childcare responsibilities
Only three studies looked at childcare responsibilities in relation to job satisfaction.11,12,15 Across the clinical DCP groups, dental hygienists who had childcare responsibilities were found to have a significantly higher level of job satisfaction than those without childcare responsibilities. 12 However, in the study by Newton and Gibbons (2001), there was no significant difference in job satisfaction between dental hygienists with and without childcare responsibilities. 15 Similarly, no difference in job satisfaction in relation to childcare responsibilities was noted for dental therapists.11,15 Therefore, the evidence for job satisfaction in relation to childcare responsibilities for dental hygienists varied, while no difference in job satisfaction related to childcare responsibilities was noted for dental therapists.
Gender
Only one study looked at gender in relation to job satisfaction and reported no difference in job satisfaction between male and female orthodontic therapists. 16 No other study provided evidence of difference in job satisfaction in relation to gender, which could be related to the fact that a majority of dental hygienists and dental therapists participating in the studies were female.
In summary, only one study investigated job satisfaction in relation to gender and no differences were noted.
Professional career level
There was some evidence regarding influence of professional career level on the overall health and wellbeing of the clinical DCPs, although this was addressed in relation to job satisfaction, similarly to the personal factors discussed above.
One study looked at skill level and training, however this was limited to dental hygienists and dental therapists (including dually qualified dental hygienist-therapists) providing ‘direct access’ care. 17 Results showed that 21% of participants felt their training did not adequately support them to provide direct access, with 64% of participants expressing the need for additional support. Also, a majority of participants (52%) felt that providing direct access did not enhance their skills, although some (39%) reported that it slightly improved their satisfaction with work. 17
Therefore, job wellbeing for dental hygienists and dental therapists (including dually qualified dental hygienist-therapists) was explored in relation to their professional career, particularly for ‘direct access’ services, although the data for the two groups were not presented separately. Overall, the findings suggested the need for educational programmes to foster confidence and skills that dental hygienists and therapists need to work more independently, particularly for ‘direct access’ treatments.
Professional and social relationships
Only four studies looked at the professional and social relationships of clinical DCPs, one of which looked at dually qualified dental hygienist-therapists, 18 one looked at dental therapists and dental hygienists working in ‘direct access’ service, 17 one looked at orthodontic therapists, 16 and another considered clinical dental technicians. 20
Evidence suggests that clinical dental technicians reported frustration and disappointment due to misunderstandings by other dental professionals and patients about their service provision, skill set, and profession. 20
Dental hygienists and dental therapists working in ‘direct access’ identified attitudes of dentists as unhelpful, which was a barrier to providing the service.17,18 However, the evidence on professional and social relationships for dually qualified dental hygienist-therapists, showed that study participants highlighted recognition from dentists and patients as factors relating positively towards job satisfaction. 18 Moreover, they expressed higher satisfaction with the professional and social relationships that they shared with their colleagues and fellow workers. 18
The findings regarding the professional relationships of orthodontic therapists and their colleagues or fellow workers had a satisfying influence on their overall job satisfaction. 16
In summary, although clinical dental technicians reported frustration in their professional and social relationships, similar to dental hygienists and dental therapists working in ‘direct access’ service, dually qualified dental hygienist-therapists and orthodontic therapists reported a more favourable perspective of their professional and social relationships which improved their satisfaction.
Job specification
Three studies addressed certain aspects of job specification.14,16,18 Of these studies, one focused on the overall job satisfaction of dental therapists, showing that dental therapists within the UK expressed high job satisfaction. 14 Another study by Turner et al. (2011), looked at certain aspects of job specification that related to the overall job satisfaction of dually qualified dental hygienist-therapists working in primary care. 18 Satisfaction with the variety in their work, and considering the hygiene work rewarding, were direct predictors of their overall job satisfaction, whereas quality of clinical work and qualifications had an indirect effect on their overall job satisfaction. 18 Evidence suggests that the hours of work, the opportunity to use their abilities, and the variety of work of orthodontic therapists, were all considered satisfying influences on their job satisfaction. 16 In summary, dental therapists expressed high job satisfaction as did orthodontic therapists. The variety in the work of dually qualified dental hygienist-therapists and orthodontic therapists contributed to their overall job satisfaction.
Workplace characteristics
Four studies looked at an aspect of work characteristics; the working environment of clinical DCPs, dental therapists, orthodontic therapists, and clinical dental technicians.10,13,16,20 Evidence suggests that the physical working conditions had a positive influence on the job satisfaction of orthodontic therapists. 16
There were both positive and negative comments regarding the workplace characteristics of dental therapists. Some dental therapists expressed frustration with their working conditions due to how they were treated by some dentists. This includes: being referred to as a hygienist rather than a therapist; being treated as an extra dentist, but with a lower remuneration; and, having their therapy skills underutilised when a new associate dentist is hired. 10 They also felt that dentists were generally unaware of their skills and scope of practice, were not confident in their abilities, and thus were not making use of them. 10 In contrast, other therapists expressed a positive outlook on their status in the practice, including feeling valued and supported. 10 They felt as an equal member of the dental team, that they were working to their full potential, and that they had an appropriate number of referrals and a wide range of patients. 10
Evidence also suggests that some dental therapists who left therapy were unwilling to return to work as therapists due to the lack of confidence, the need for a refresher course, or that they now work as hygienists. 13 Moreover, lack of jobs in their locality was of concern. 13 Based on the evidence, clinical dental technicians felt excluded from the dental team and felt concern due to patients and other dental professionals not comprehending their role. 20
In summary, orthodontic therapists reported favourable influence of physical working environment on job satisfaction. While dental therapists expressed positive comments regarding their status in the practice, frustration with their treatment by some dentists, lack of jobs, and lack of confidence in therapy skills were reported. Frustration was also expressed by clinical dental technicians for feeling excluded from the dental team.
Dental healthcare systems
With respect to dental healthcare systems, three studies16,18,19 highlighted financial concerns of dental therapists, dually qualified dental hygienist-therapists, and orthodontic therapists, while one 20 looked at the overall system issues regarding clinical dental technicians. Out of the three studies that looked at the financial concerns expressed by clinical DCPs, one focused on dental therapists, 19 one on dually qualified dental hygienist-therapists working in primary care, 18 and one on orthodontic therapists. 16
Dually qualified dental hygienist-therapists working in primary care reported inadequate remuneration as a factor that led to low job satisfaction. 18 Evidence also suggests that dental therapists expressed payment being low compared to dental hygienists. 19 They felt that the remuneration was considered poor given the amount of stress they experienced and the responsibilities in their job. 19 Concerns were also expressed by dental therapists towards the issue of dentists considering dental hygienists to be more cost-effective than dental therapists. 19 The study by Curtis et al. (2019), identified that clinical dental technicians expressed concerns and frustration with the NHS, and the Care Quality Commission. 20 They also expressed feeling excluded from the dental team due to their inability to provide NHS dental care.(20) The findings also suggests that orthodontic therapists who reported high job satisfaction were least satisfied with their remuneration. 16
In summary, dental therapists and dually qualified dental hygienist-therapists expressed dissatisfaction with remuneration within the health system, as did orthodontic therapists and clinical dental technicians. Dental therapists expressed concern with the perceived cost-effectiveness of dental hygienists. Orthodontic therapists considered their remuneration as having a dissatisfying influence on their job satisfaction. Furthermore, a lack of financial reward and status within the NHS impacted on dental hygienists’ and therapists’ job satisfaction. Status within the NHS was also a factor for clinical dental technicians.
Regulation
One study looked at regulatory changes in relation to job wellbeing. 17 It reported that the majority of participants were in favour of the change in regulation by the GDC allowing for ‘direct access’ by patients. 17 Evidence suggests that the majority (64%) of dental hygienists and dental therapists (including dually qualified dental hygienist-therapists) providing ‘direct access’ care felt that it enhanced their job satisfaction. 17 However, they also expressed concern with certain regulatory aspects that they felt needed improvement. 17 The reported barriers relating to ‘direct access’ care included restrictions on treatment planning, and prescribing radiographs. Moreover, some dental hygienists and dental therapists felt that their training and education did not prepare them sufficiently. 17 Thus, while the regulatory change that allowed for ‘direct access’ enhanced job satisfaction for dental hygienists and dental therapists, it highlighted the need for additional training and education.
Two studies addressed litigation concerns of clinical DCPs, exposing them to greater regulatory scrutiny. One looked at clinical dental technicians, 20 and the other looked at dental hygienists and dental therapists (including dually qualified dental hygienist-therapists) working in ‘direct access’ practices. 17 The evidence overall suggests that some dental hygienists and dental therapists (including dually qualified dental hygienist-therapists) expressed concern of possible litigation when working in ‘direct access’ practices. Litigation concerns were also expressed by some clinical dental technicians. 20
Continuing professional education
Two studies,13,21 addressed concerns with the continuing professional education. In the study by Hillam (2000), nearly half of the dental hygiene participants (46.5%) expressed availability of continuing professional education as being “good” or “very good”, while some (33.5%) expressed it as being “poor” or “very poor”. 21 A lack of opportunity to attend continuing professional development (CPD) courses was expressed by dental therapists in the study by Godson et al. (2009). 13 They expressed the need for more CPD courses for dental therapists to attend alongside dentists, as well as the need for hands-on courses. 13
In summary, while opinions about the availability of continuing professional education varied between dental hygienists and dental therapists, both groups expressed a lack of opportunity and availability of CPD courses.
Discussion
This review adds to knowledge, as it is the first systematic review to investigate the health and wellbeing of clinical DCPs in the UK. It combined available evidence relating to dental hygienists, dental therapists, orthodontic therapists, and clinical dental technicians. There is paucity of research over two decades, that rarely considered all determinants and mostly focused on job satisfaction and job specification. However, evidence of a range of secondary and interlinked determinants suggests that there may be as wide a range of determinants for clinical DCPs, as suggested by Colonio-Salazar et al. (2019), 2 as for dentists. Furthermore, there were also system issues for clinical DCPs in relation to continuing professional education which could enhance or detract from their careers and job satisfaction.
There were some limitations to this review. Firstly, there was a lack of recent studies. Secondly, some of the professional groups are relatively new and there has not been much research conducted. Thirdly, we note an inability to locate full text of three studies due to age of publication. Lastly, not all studies used validated instruments.
While dental hygienists expressed high job satisfaction, especially those who were older and those who had childcare responsibilities, many of these studies were conducted two decades ago, in 2000 and 2001, and much has changed since that time. In more recently-conducted research, orthodontic therapists expressed high job satisfaction, but limited evidence made it hard to generalise results. There was some evidence that clinical dental technicians were mostly satisfied with and passionate about their work. However, they had concerns that stemmed from the miscommunication with dentists and patients, as well as concerns with policymakers and regulators. In contrast, evidence on dental therapists in relation to their job satisfaction was mixed. Again, however, most studies that suggested high job satisfaction11,15 were older, conducted during the period when dental therapist were singly-, rather than dually-, qualified. 24
This review investigated the macro-, meso-, and micro-level factors influencing health and wellbeing based on the framework provided by Colonio-Salazar et al. (2019). 2 Similarities were found between dentists and the investigated clinical DCP groups in terms of financial concerns which were expressed by dentists as a source of stress, demotivation, and burnout. 2 Dental therapists and orthodontic therapists also reported low remuneration as a negative influence on their job satisfaction. When exploring personal factors, Colonio-Salazar et al. (2019) reported that male dentists were more satisfied with their career. 2 However, this review found no differences in job satisfaction in relation to gender, which is possibly due to females comprising the majority of dental hygienists (95%), dental therapists (93%), and orthodontic therapists (97%). 1 Professional relationships expressed by dentists were mostly in relation to patients and management affecting their morale, whereas dental therapists and clinical dental technicians expressed most concerns in their relationship with dentists. This could be explained by the hierarchy within dentistry, and clinical DCPs’ reliance on dentists for prescription prior to treatment, which can also explain the enhancement in job satisfaction of dental hygienists and dental therapists under ‘direct access’ service. Social relationships in relation to health and wellbeing were not investigated for both dentists and clinical DCPs.
Further challenges have been imposed on dentistry since the COVID-19 pandemic. 25 A recent British Dental Association (BDA) survey of dentists in England revealed that many dentists are considering leaving their profession or seeking early retirement, if COVID-19 restrictions remain. 25 Additionally, dentists reported that the financial uncertainties and the mandated high-level personal protective equipment (PPE) are causing a devastating impact on their morale. 25 Findings from a recent Dental Defence Union (DDU) survey also suggest that stress and anxiety levels have increased among dentists due to the uncertainties of the pandemic, and that the wellbeing of providers is directly linked to patient quality of care. 26 Therefore, understanding determinants of health and wellbeing for the wider dental team is necessary to protect the workforce and patients.
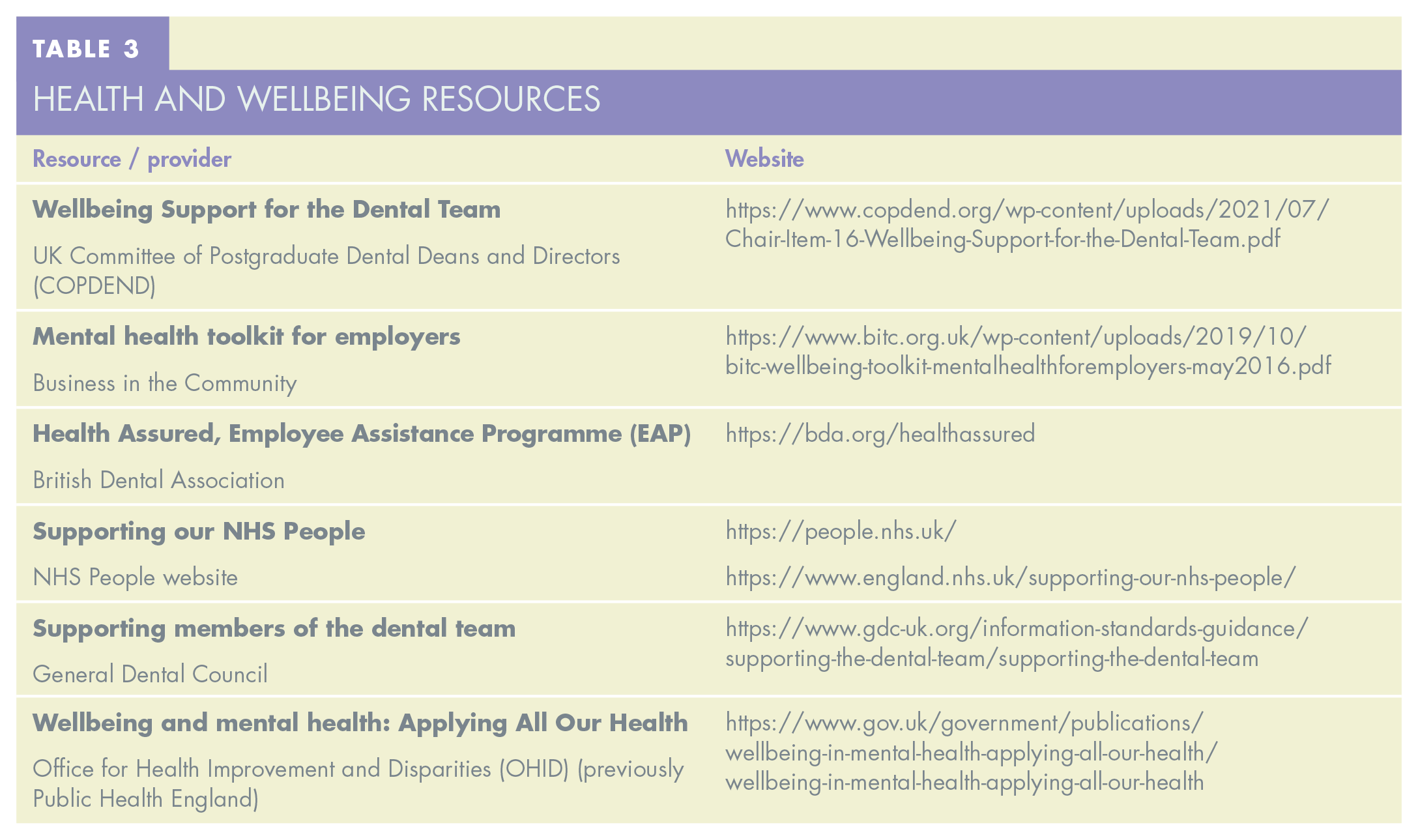
In addition, based on the former research on the key determinants of health and wellbeing of dentists, 2 it has been shown that the level of stress, anxiety, burnout, and early retirement due to ill-health is high among dentists, while there is a distinct lack of evidence on clinical DCPs’ mental health and wellbeing in the UK. This lack of evidence is confirmed by a recent GDC report which recommends further empirical research to determine the impact of poor wellbeing and mental health on the performance of the dental team and the safety of patients. 27 Particularly, with the expansion in DCP numbers and their role in health care systems, it is necessary to further investigate the key determinants of their health and wellbeing to protect the workforce as well as patients, and to avoid future problems. Therefore, up-to-date research using validated instruments is recommended to understand the range of factors contributing to the health and wellbeing of the various clinical DCP groups. Research is also needed to investigate the health and wellbeing of dental nurses, who comprise the biggest group of DCPs. Furthermore, it should take account of regulatory differences between sectors (NHS and private) and countries. Thus, contemporary research across the four nations of the UK is necessary to understand the health and wellbeing of DCPs. Finally, given available evidence of pressure on the dental team generally, it is important to highlight the range of resources available to support health and wellbeing, as shown in Table 3.
Health and Wellbeing Resources
Conclusion
There is limited evidence on the health and wellbeing of clinical DCPs and its determinants. Most studies focused on job satisfaction and job specification. Based on the evidence, overall job satisfaction was expressed by dental hygienists and orthodontic therapists. While some studies suggested overall satisfaction of dental therapists, others showed concerns relating to low remuneration, underutilisation of skills, lack of job opportunities and dentists not understanding dental therapists’ scope of practice. Clinical dental technicians felt pride and passion for their work and expressed satisfaction. Nevertheless, they also expressed having communication issues with other dental professionals and patients, and problems with regulations and policies. However, the results must be considered carefully due to the limited number of studies. Further well conducted research is needed on the key determinants of overall health and wellbeing of the DCP workforce and to better their future. Furthermore, relevant issues concerning DCPs’ job satisfaction in particular must be addressed to support the overall health and wellbeing of the wider clinical dental team.
Footnotes
Acknowledgements
The authors would like to thank the library services at King’s College London for their help and efforts during the literature search and screening.