
Abstract
Objective
To study the effect of a dietary supplement (TARGET 1®: a combination of casozepine, taurine, Eleutherococcus senticosus and extramel) on burnout symptomatology.
Methods
A 12-week, double-blind, randomized, placebo-controlled trial was conducted in workers engaged in professional contact with patients, students or clients. All were affected by burnout syndrome based on a score of ≥4 on the Burnout Measure Scale (BMS-10). The primary outcome measure was the change in the BMS-10 score; secondary outcome measures included the change in the Maslach’s Burnout Inventory scale-Human Service Survey (MBI-HSS) score and the Beck Depression Inventory. Five scores were evaluated.
Results
Eighty-seven participants were enrolled in the study: 44 received the active formulation (verum group); 43 received placebo. After 12 weeks’ supplementation, the placebo group showed significant improvements in scores for BMS-10, MBI-HSS fatigue and the Beck Depression Inventory, but MBI-HSS depersonalization and task management were not improved; the verum group showed significant improvements in all five scores. The verum group consistently showed significantly greater improvements in scores than the placebo group.
Conclusions
TARGET 1® significantly improved the symptoms of burnout after 12 weeks’ use.
Introduction
Burnout was first described in 1969, in professionals who had close contact with patients. The concept evolved to include professionals having no contact with patients, students or clients and is now described as a crisis related to work, rather than a crisis of relationships with persons under care during work.1–8 The first evaluation tool, Maslach’s Burnout Inventory scale-Human Service Survey (MBI-HSS), 9 comprises 22 items and is designed specifically for evaluating people in close professional contact with patients, students or clients; MBI-HSS aims to determine the relationship between the professional and the person being helped. Subsequent evaluation tools were adapted for general use, leading to the Malach-Pines Burnout Measure Scale, short version (BMS-10), 10 in which the number of items was reduced from 22 down to 10.
There is no standard treatment for burnout. Different forms of psychological intervention are usually attempted;11,12 with verbal exchange playing an important role. Medical treatment for burnout largely centres on the administration of anxiolytic and/or antidepressant agents, which are not necessarily effective. Trials involving herbal treatments have yielded few satisfactory results,13–15 apart from a randomized clinical trial of Rhodiola rosea in 60 patients, which provided evidence of an ‘antifatigue’ effect and an improvement in burnout symptoms.16,17
A dietary supplement combination product known as TARGET 1®, specifically produced for the present study by Laboratoria Wolfs (Zwijndrecht, Belgium; GMP certificate BE/2012/074), a was developed to act on different aspects of burnout syndrome. TARGET 1® includes four key ingredients: casozepine (milk casein), which is considered in the French pharmacopoeia as having a benzodiazepine-like profile and an action that targets depressive symptoms, which are always present in burnout;18–20 extramel, a melon extract rich in an antioxidant (superoxide dismutase) that reduces cellular oxidation (which is accelerated in burnout due to sleep and mood disorders, cramp, fatigue, and stress); 21 taurine, which is believed to have energizing properties and ‘antifatigue’ effects; 22–24 Eleutherococcus senticosus, which is classified as an ‘adaptogenic herb’,25–27 a term applied to plants such as ginseng that increase the body’s resistance to stress (another constant feature of burnout). The detailed composition of TARGET 1® is described in the ‘Randomization and supplementation’ section, below. The usual dose of TARGET 1® is two tablets per day, taken orally in the morning.
The hypothesis of the present study was that the efficacy of TARGET 1® would be confirmed if the BMS-10 score decreased by 1.5 points in the group receiving the active product (i.e. approximately a ≥30% reduction) between the start and end of the trial, after weighting the score by subtracting the score of the placebo group. The present study evaluated the efficacy and tolerability of TARGET 1® in a double-blind, randomized, placebo-controlled clinical trial in participants with burnout syndrome, and followed study subjects’ symptoms of burnout using different evaluation instruments.28–34
Methods
Study design
This 12-week, double-blind (active/placebo), randomized, two parallel-group clinical study was undertaken in the Department of Clinical Pharmacology, University of Bordeaux Ségalen, Bordeaux, France, between March 2012 and February 2013. Inclusions were suspended in June, July and August 2012 to avoid any interference from the summer vacation period. Participants were enrolled consecutively, as described below. All participants provided written informed consent. Written approval for the study was obtained from the South-West and Overseas III Committee for the protection of persons in biomedical research (approval granted on 28 March 2012; ID-RCN number: AFSSAPS: 2012-A00096–37 [Accreditation]). The clinical trial registration number of this study on clinicaltrials.gov is NCT01599169.
Three study visits were scheduled at 6-week intervals: V1–day 0, V2–day 42 and V3–day 84, during which the following evaluation instruments were administered: BMS-10 (one score); 10 MBI-HSS 9 (three scores); Beck Depression Inventory (one score).29–31 All study visits and all evaluation tools were conducted by the same investigator (A.J.).
At each study visit, participants underwent interviews that discussed their family, social and professional relationships; the interview procedures are outlined below. Subjects also underwent evaluations to judge the safety and tolerability of the supplement that they received. At V1, participants also signed the consent form after verification of the inclusion and exclusion criteria, before they were randomly assigned a participant number and received a batch of 100 tablets (active or placebo supplement, outlined below). Unused tablets had to be returned at V2 and V3.
At V2 and V3, interviews focused on the evolution of each participant’s condition (identical, worse, improved) since the previous visit and any adverse effects were recorded. At V2, subjects received a second batch of 100 tablets. Compliance was calculated for each group at V2 and V3, using the following formula: real number of tablets swallowed/theoretical number of tablets to be swallowed.
Study participants
The study was advertised locally within the University Hospital Centre of Bordeaux and in local newspapers, as well as in family physicians’ waiting rooms. The study also aimed to identify and recruit a highly diversified range of individuals and professions. Participants were interviewed alone, to respect their anonymity and help them to speak in confidence.
The protocol stipulated that inclusion would be based on the date when participants entered the trial. The main inclusion criteria were: persons aged between 18 and 65 years; persons having given written consent to the study and its procedures; persons in professional contact with patients, students or clients (required for the use of the MBI-HSS); baseline BMS-10 score ≥4 (presence of burnout, high level or very high level of exposure to burnout); persons in continuous professional activity (no inclusion if the trial period encompassed a vacation period of >1 week); persons not undergoing treatment with antidepressant or anxiolytic medication. Subjects were not excluded on the basis of any underlying medical condition. Potential study participants were excluded if they met any of the following exclusion criteria: lactose intolerance (because of casozepine); sick leave >1 week; change in profession or position.
In each participant, burnout was formally diagnosed by the primary investigator (A.J.) using the evaluation tools (i.e. MBI-HSS, BMS-10 and Beck Depression Inventory), which were administered during the interview in V1. In order to comply with regulations for the conduct of studies involving dietary supplements, no other physical or clinical examinations were undertaken. Participants who were confirmed to have burnout by their scores on the evaluation tools were then included in the study. These scores were then used to quantify the extent of burnout in each individual.
Randomization and supplement
Randomization was performed using SAS® software, version 9.3 (SAS Institute, Cary, NC, USA), with a block size of 6 and a 1 : 1 allocation ratio for the active (verum) and placebo groups (undertaken by Unit CIC-P0005, National Institute of Statistics and Medical Research [INSERM], Bordeaux, France). The study product TARGET 1® will be marketed in specific countries from January 2015 [link to footnote marked 1]. The composition of TARGET 1® (640 mg tablet form) is: casozepine (α-S1 milk casein tryptic hydrolysate), 75 mg; extramel, 5 mg; taurine, 50 mg; Eleutherococcus senticosus, 50 mg dry extract (corresponding to 1.25 mg of eleutherosides). The placebo tablets contained only the inactive compounds used in TARGET 1®, namely: magnesium stearate; aerosil 20; microcrystalline cellulose; hydrogenated vegetable oil. The placebo tablets were formulated to be identical in appearance to the TARGET 1® tablets. All study participants took two of their allocated tablets daily, after breakfast with a glass of water, for 12 weeks.
Interview procedures
The extensive interviews (1.5 h per visit; all undertaken by A.J.) were structured in a manner that enabled all evaluation tools to be administered and their scores to be recorded. However, participants were also able to express themselves freely and in detail about their working conditions (including difficulties encountered with the people they ‘helped’, relationships with colleagues and workplace hierarchy), their family and social relationships. Together, the evaluation scores and interview data helped to refine the diagnosis of burnout, confirm the veracity of participants’ professional problems that were at the root of their condition and quantify the consequences of these problems (and burnout) on social and family life. Participants were also asked to give details of any constraints experienced and degradation of their various relationships.
During the interviews, participants were asked to speak precisely about the quality of their family life, their professional life and their sleep; they were also asked about their energy levels. Their scores for these four aspects were measured on a visual analogue scale (VAS, a horizontal 100-mm line on which the participant places a cursor; VAS scores ranged between 0 [worst possible] and 100 [best possible]). Improvements were indicated by an increase in score.
Primary outcome measure
Interpretation of the Short Version of the Malach-Pines Burnout Measure Scale (BMS-10) in terms of the level of burnout. 10

Secondary outcome measures
Secondary outcome measures included the change in the Maslach’s Burnout Inventory scale-Human Service Survey (MBI-HSS) score and the Beck Depression Inventory.
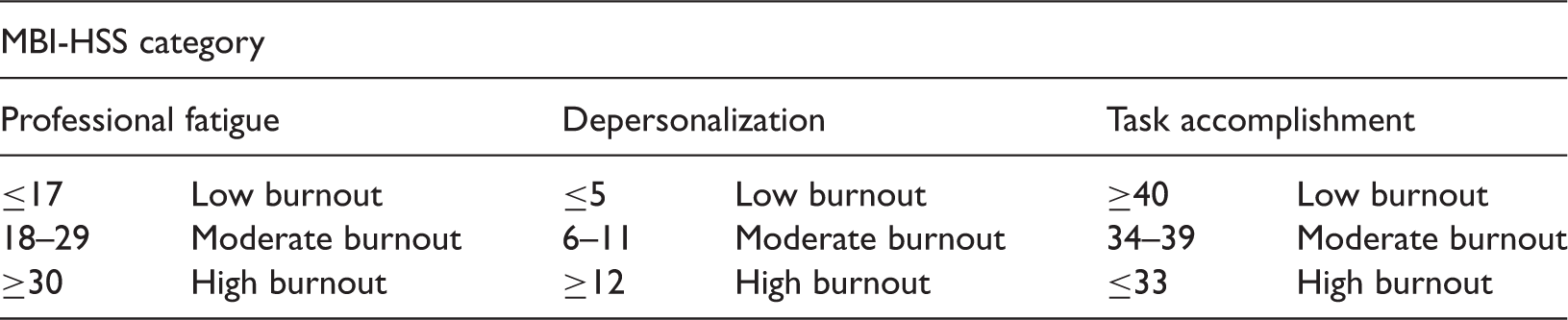
Interpretation of the Maslach’s Burnout Inventory scale-Human Service Survey (MBI-HSS) scores for the three categories in terms of level of burnout. 9
Interpretation of the Beck Depression Inventory scores.

Statistical analyses
Data were generally presented as mean ±SD. All statistical analyses were performed using the SAS® statistical package, version 9.2 (SAS Institute) and were undertaken by Unit CIC-P0005, INSERM, Bordeaux, France. Sensitivity analyses were conducted on the results of the primary outcome. For intragroup comparisons, the significance level was 5% in bilateral formulation, using Student’s t-test, a nonparametric paired Wilcoxon signed-rank test and regression models for repeated measures data (generalized linear model [GLM] type). For intergroup comparisons, the significance level was 5% in bilateral formulation, using Pearson’s χ2-test, Student’s t-test and regression models for repeated measures data (GLM type). A P-value ≤0.05 was considered statistically significant.
Results
A total of 44 participants were included in the verum group (18 male and 26 female; mean age, 46.9 years; age range 29–61 years) and 43 in the placebo group (14 male and 29 female; mean age, 45.6 years; age range 27–63 years). Two participants aged <30 years were included in the analyses; we consider this a minor protocol deviation. Two subjects left the trial before V2 in the placebo group, for reasons related to the exclusion criteria (work leave and the prescription of anxiolytic treatment). Consequently, the analyses of data involving V2 and V3 are based on 85 validated observations.
Professions of subjects (n = 87) included in a 12-week, double-blind, randomized, placebo-controlled clinical trial, designed to evaluate the use of a dietary supplement (TARGET 1®) for alleviating the symptoms of burnout syndrome.

Primary and secondary outcome measure scores at three study timepoints (V1, V2, V3) for subjects with burnout, randomly assigned to receive active supplement (verum; n = 44; TARGET 1®) or placebo (n = 43 at V1; n = 41 at V2 and V3) for 12 weeks.

Data presented as: mean, for individual study timepoints; mean ± SD for V1–V3; percentage change (%) for V1–V3.
Score variations between V1 and V3 were calculated according to individual rather than mean scores. Values were obtained by subtracting the V3 score from the V1 score for each participant, then calculating the mean of all of these differences. Tables may show a slight difference between results listed in columns showing score evolution (difference between V1 and V3) and calculations the reader might make on the basis of data in the columns showing means of scores. The same applies to the percentages.
For intragroup comparisons, the significance level was 5% in bilateral formulation, using Student’s t-test, a nonparametric paired Wilcoxon signed-rank test and regression models for repeated measures data (generalized linear model [GLM] type). For intergroup comparisons, the significance level was 5% in bilateral formulation, using Pearson’s χ2-test, Student’s t-test and regression models for repeated measures data (GLM type)
Change in outcome measure between V1 and V3 in the verum group was significantly greater than that of the placebo group for each intergroup comparison.
BMS-10, Burnout Measure Scale; MBI-HSS, Maslach’s Burnout Inventory scale-Human Service Survey; NS, no statistically significant differences (P > 0.05).
In the placebo group, two of the four outcomes in the burnout scales significantly improved, as did the Beck Depression Inventory scores, over the 12-week study period: mean ± SD BMS-10 decreased by −0.6 ± 0.8 (−11.7%; P < 0.0001); and the mean ± SD MBI-HSS fatigue score decreased by −3.7 ± 7.0 (−9.1%; P = 0.0058); MBI-HSS depersonalization and MBI-HSS task accomplishment were not significantly improved. The mean ± SD Beck Depression Inventory score decreased by −6.8 ± 9.6 ( −20.4%; P < 0.0001).
In the verum group, all four outcomes for the burnout scales and the Beck Depression Inventory score improved significantly over the 12-week study period (P < 0.0001 for all comparisons). The mean ± SD BMS-10 decreased by −2.3 ± 0.9 ( −45.9%; P < 0.0001). The mean ± SD MBI-HSS fatigue score decreased by −22.9 ± 9.6 (−57.6%; P < 0.0001). The mean ± SD MBI-HSS depersonalization score decreased by −7.9 ± 4.8 (−50.3%; P < 0.0001). The mean ± SD MBI-HSS task accomplishment score increased by +7.4 ± 5.6 (+29.5%; P < 0.0001). The mean ± SD Beck Depression Inventory score decreased by −24.7 ± 11.0 (−75.5%; P < 0.0001). For the primary and secondary outcome measures, improvements observed in the verum group were significantly greater than those observed in the placebo group (P < 0.0001 for all comparisons). When weighting the raw score in the verum group relative to the placebo group, the verum group demonstrated a reduction of 1.7 (−34.2%). This decrease was greater than that specified (1.5) in the protocol to confirm the efficacy of TARGET 1® in improving the symptoms of professional fatigue or burnout syndrome.
Level of burnout exposure, based on Burnout Measure Scale (BMS-10) scores at two study timepoints (V1 and V3), in a placebo-controlled 12-week study evaluating the effects of the dietary supplement TARGET 1® (verum group) in subjects with burnout.

Two study participants left the study prematurely and were excluded from analyses.
Very few adverse events were reported by study participants. In the placebo group, some digestive events occurred (soft stools, episodes of mild constipation, slight gastric disturbance, and gastro-oesophageal reflux). All such events disappeared within 5 days of starting the study, with the exception of a moderate increase in stool frequency. Other events were not considered to be attributed to the research (cystitis, sinusitis, bronchitis, and heavy legs). In the verum group, some digestive adverse events occurred (diarrhoea for 48 h, mild constipation and mild flatulence). All such events disappeared within 5 days of starting the study, except in the case of two study participants who experienced mild constipation until the end of the trial. No subject required treatment for these events. Other events were not considered to be linked to the research (fall, bronchitis, ear ache, and oral herpes simplex virus infection).
Tolerability to the study product TARGET 1® was judged to be ‘excellent’ at the end of the study. Compliance levels in the active group were 98.4% (±5.3) on V2 and 98.3% (±4.7) on V3, and in the placebo group were 97.2% (±6.0) on V2 and 97.0% (±5.8) on V3.
Visual analogue scale scores in subjects with burnout, receiving TARGET 1® (verum; n = 44) or placebo (n = 43 at V1; n = 41 at V2 and V3) for 12 weeks. Scores range between 0 (worst possible) and 100 (best possible), and were obtained at three visits (V1, day 0, V2, day 42, V3, day 84).

Data presented as mean ± SD.
For intragroup comparisons, the significance level was 5% in bilateral formulation, using Student’s t-test, a nonparametric paired Wilcoxon signed-rank test and regression models for repeated measures data (generalized linear model [GLM] type). For intergroup comparisons, the significance level was 5% in bilateral formulation, using Pearson’s χ2-test, Student’s t-test and regression models for repeated measures data (GLM type).
The interview sessions at each study visit highlighted the main professional difficulties that the participants encountered. These included moral and/or physical exhaustion resulting from too heavy a workload, a lack of means or a ‘bad atmosphere’ in the workplace: the hierarchy, seen as uncompromising and often dehumanized (where the employee becomes an ‘object of production’), was often held responsible for these disorders. Participants described a typical profile of constraints that were generally thought to be at the root of burnout, which (in addition to the demanding hierarchy) included: an unattainable work goal (e.g. an increased workload, to be undertaken in a shorter timeframe, leading to extreme fatigue and depersonalization); ‘means’ (i.e. tools or time in which to undertake the work) being increasingly reduced, with the same amount of work being required; an inhumane attitude in the working environment (e.g. a macho environment with bullying, racism, moral or sexual harassment; an air of superiority on the part of managers).
Participants reported that malaise at work rapidly led to several consequences, firstly in regard to professional life (lower motivation, reduced performance, development of a depressive syndrome even in those with no noteworthy depressive history, aggression toward superiors and colleagues), quickly followed by effects on social and family life (loss of sleep, fatigue, irritability, gradual loss of dialogue with aggression toward their spouse and children, lack of interest in social life). A strong feeling of ‘loneliness’ prevailed, they explained.
In addition, it is worth commenting that potential participants were attracted to the current study because it took place in a University Hospital setting under medical control; the opportunity that it gave individuals to ‘finally talk about work problems in complete anonymity’ was seen as a relief. The fact that employers or occupational physicians were not present raised confidence (due to respect for anonymity). However, participants commented that they rarely spoke about their problems associated with fatigue and burnout, even with their own doctors.
Discussion
Findings of this 12-week clinical study, conducted in professionals affected by burnout, demonstrated important and significant improvements in all three internationally recognized evaluation instruments for burnout used (i.e. a total of five scores) in the active (verum) group, whereas a moderate but significant improvement was found for three out of five scores in the placebo group.
For the primary outcome measure, the BMS-10 score, both study groups demonstrated significant reductions over the 12-week study period. However, when weighting the raw score in the verum group relative to that seen in the placebo group, the verum group demonstrated a reduction of 1.7 (−34.2%). This decrease was greater than that specified in the protocol to confirm the efficacy of TARGET 1® in improving the symptoms of professional fatigue or burnout syndrome. In addition, the tolerability of this novel dietary supplement was judged to be excellent.
In the placebo group, 14 participants still presented with a high level of burnout at the end of the trial compared with 26 on inclusion, whereas in the verum group only two participants presented with a high level of burnout at the end of the trial compared with 33 on inclusion (Table 6).
The substantial improvements in depressive symptoms (as measured by BMS-10) observed in the present study may be related to at least two factors. First, one of the ingredients of the study product, casozepine, is referred to as ‘benzodiazepine-like’ in the French pharmacopoeia. 18–20 Secondly, the extensive and detailed interviews, conducted by the doctor at each of the three study visits, allowed participants to calmly and clearly express their problems and malaise at work, and the repercussions of these issues on their social and family life, and their general wellbeing.
In the context of burnout, it is our opinion that verbal expression is an absolute priority during the course of supplementation. The extensive (1.5 h) interviews forming each study enabled participants to express themselves at length about their difficult professional experiences. These sessions likely played a substantial role in improving participants’ wellbeing in the present study, but the timeframe was identical for all subjects, regardless of their allocated group. However, improvements were far more noticeable in the verum group than in the placebo group. Verbal expression on the subject of burnout is often difficult or even impossible, yet all the participants agreed that the interview structure provided a real benefit to their wellbeing. ‘Words’ in this context seemed to be of prime importance, and health professionals, doctors and psychologists in particular should give special attention to the verbal aspects of burnout management.
The 1.5-h interviews also provided a detailed profile of the constraints that the participants experienced, which are always at the root of burnout. Typically these manifested as mental and/or physical exhaustion resulting from too heavy a workload, a lack of means or a bad atmosphere in the workplace. The hierarchy, seen as uncompromising and often ‘dehumanized’, was often held responsible. Consequently, in addition to providing the scores for the specific scales, the interviews also helped to refine the diagnosis and causes of burnout.
It was of interest to note that the participants in this trial most often had no significant history of depression, their depression being related to the incessant and/or inhumane working conditions and humiliations to which they were subjected
Relative inhomogeneity was observed in the professions in each group. Homogenous distribution would not have been possible in this study design, because it would have meant knowing who was in the verum and placebo groups, and the double-blind nature of the study would not have been respected. Indeed, as reported in the Results, two people with the same job title in different settings were affected by burnout for very different reasons.
It was unsurprising to see that there was a high proportion of female participants in the study. In our anecdotal experience, women appear to find it easier than men to discuss their problems.
It was a strength of this study in that it include different evaluation tools. The MBI-HSS cannot be used alone as a diagnostic element: it is specifically for subjects who have an immediate work relationship with patients, students or clients. While the MBI-HSS provides a ‘measurement’ of various items (professional fatigue, depersonalization and task accomplishment), 9 it gives no relevant indication of the depressive effect of burnout, whereas the Beck Depression Inventory29–31 fulfilled this requirement. Another strength of this study was that potential participants were attracted by the anonymous nature of its design. The 1.5 h interview structure, conducted in private, provided them with novel opportunities to discuss burnout.
The present study also had a number of limitations. First, it was a single-centre trial. Secondly, the number of study participants was small. However, it should be borne in mind that drug legislation does not apply to dietary supplements, which can be placed on the market without a clinical trial. This present study complied with the standard requirements for products of this class.
In conclusion, the value of this 12-week, randomized, placebo-controlled trial lies in the fact that, to our knowledge, no other dietary product has been evaluated in this manner for the overall management of people affected by burnout, despite this being a common problem in many countries. For this reason, the dietary supplement TARGET 1®, when used in association with verbal expression, might represent a primary tool in the care of people affected by burnout in the future.
Footnotes
Acknowledgements
This clinical trial was entrusted to us by Laboratoires Nanox International, Hasselt, Belgium.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
a
TARGET 1® is to be marketed and distributed in individual countries by specific licensed companies. The names and addresses of these companies are available from the Corresponding Author on request.