
Abstract
To assess and improve the quality of oral healthcare, we must first agree on what constitutes good care. Currently there is no internationally accepted definition for quality of oral healthcare. Therefore, the purpose of the study was to establish a working definition for quality of oral healthcare that would help to advance further improvements in the field of quality improvement in oral healthcare. The development of the working definition included a 3-step approach: 1) literature screening; 2) expert-based compilation of an initial list of topics, leaning on the National Academy of Medicine framework for quality of care; and 3) a World Café with voting, which took place during the annual general meeting of the International Association for Dental Research in 2018. Following this approach, the collective intelligence of involved participants yielded a comprehensive list of items, prioritized by relevance. The resulting working definition comprises 7 domains—patient safety, effectiveness, efficiency, patient-centeredness, equitability, timeliness, access to care—and 30 items, which together characterize quality of oral healthcare. This aspirational working definition provides the potential to facilitate further conversations and activities aiming at quality improvement in oral healthcare.
Knowledge Transfer Statement:
This special communication describes the development of a working definition for quality of oral healthcare. The findings of this study are intended to raise awareness of the relevance of quality improvement initiatives in oral healthcare. The working definition described here has the potential to facilitate further conversations and activities aiming at quality improvement in oral healthcare.
Keywords
Introduction
Patients, providers, payers, and policy makers across the globe are increasingly focused on assessing and improving the quality of healthcare. Healthcare quality has been defined as “the application of medical science and technology in a manner that maximises its benefit to health without correspondingly increasing the risk” (Donabedian 1988). Although healthcare accounts for a substantial part of a nation’s budget, many patients have no access to care, receive suboptimal care, or are even inadvertently harmed.
Measurement is a crucial element when seeking to improve the quality of care, and various sets of quality measures have been developed accordingly. Transparent information about healthcare quality, which reflects the structures, processes, and outcomes associated with healthcare, offers patients, policymakers, and healthcare providers the potential to learn from the feedback provided (Righolt et al. 2019).
A prerequisite for meaningful feedback information on quality of care is that such information embraces all relevant dimensions pertaining to quality of care. Several theoretical frameworks exist that broadly define quality of care; these all rely on an evidence base from general medicine (Campbell et al. 2000) and describe quality as a multidimensional concept. A frequently used framework is that developed by the National Academy of Medicine (NAM). It comprises 6 important components: patient safety, patient-centeredness, equitability, timeliness, effectiveness, and efficiency. To date, however, there is no internationally accepted definition for quality of oral healthcare.
Conceptualizing oral healthcare quality is complex since it is dependent on many factors. Large variations in dental policy systems exist, and standards and interpretations of quality of oral healthcare are dependent on local and national contexts, as well as the perceptions of various stakeholder groups (Campbell et al. 2000). A better understanding of quality can foster shared learning and contribute to a more comprehensive quality improvement knowledge base (FDI World Dental Federation 2017). A working definition can be refined over the years and may provide a sensible first step toward reaching a broad consensus on quality of oral healthcare.
Therefore, the purpose of the present study was to develop a working definition for quality of oral healthcare, which could facilitate conversations and activities aiming at improving this.
Methods
A 3-stage approach was used, which consisted of the following: 1) literature screening; 2) expert-based compilation of an initial list of topics; and 3) a World Café, which took place during the annual general meeting of the International Association for Dental Research (IADR) in 2018 (see Figure). Further details about the World Café, organized as an IADR Hands-on Workshop, are available via https://iadr2018.zerista.com/event/member/489683.
Stages.
According to the criteria of the Central Committee Involving Human Subjects (the Netherlands) and the Medical Research Involving Human Subjects Act, Medical Ethics Committee approval was not required.
Literature Screening and Initial List of Topics
To identify relevant aspects of the quality of oral healthcare, a literature screening was conducted in December 2017 with the electronic database MEDLINE (via PubMed). Based on the studies identified through literature screening, a “starting list” was developed, which consisted of an initial list of items that were categorized according to the 6 NAM domains. See Appendix up to and including Appendix Table A.3 for further details.
World Café and Voting
The World Café methodology facilitates group discussion through multiple rounds of short and focused conversations. The method enables the collection of a group’s collective intelligence. All delegates registering for the IADR General Session 2018 were informed about the opportunity to participate in the World Café, but the number of participants was limited to 50 (registration during conference registration on a “first come, first served” basis). All registered participants received an information package (see Appendix A.4) and the starting list. In the weeks preceding the workshop, participants could also share their thoughts via an interactive (anonymous) online platform. The information received was taken forward by the moderators as input for the face-to-face World Café.
The World Café took place on July 27, 2018. Each attending participant of the workshop was assigned to 1 group table, and the composition of these remained unchanged throughout the World Café. During 6 consecutive 10-min rounds, each of the 6 initially proposed domains and items of quality of care (Appendix Table A.2) were discussed and revised—domain by domain—by each group. Each group conversation was facilitated by 1 of the 6 moderators, who were each assigned 1 quality-of-care domain in advance of the workshop. The moderators rotated from 1 group table to the next until all domains were consecutively discussed by all groups and the moderators had collected the collective intelligence of all groups. After 6 iterations, each moderator presented a summary list of all collected topics.
Following the group discussions, each participant received 3 stickers to indicate his or her top priorities for each domain. Immediately after the World Café, the moderators discussed the main findings and results proceeding from the 6 iterations of group discussions. In addition, the moderators agreed on overarching topics that emerged from the discussion about the various domains. The results were processed by 1 researcher (A.J.R.) and then double-checked by all other moderators to ensure that all results were interpreted and processed correctly. In case of uncertainties during the processing of results, the moderator who had covered the relevant quality-of-care domain during the workshop was consulted for feedback according to her or his observations throughout the workshop.
Final Derivation of the Working Definition
On the basis of the World Café results, a working definition was established according to the following process:
1) For each NAM domain, items were ranked by the number of votes.
2) The 5 most frequently voted items per domain were always included in the definition.
3) Items with fewer votes than the 5 most frequently voted items were included only if the item was judged to be closely linked to at least 1 of the 5 most frequently voted items (see aforementioned criterion).
4) Included items that were discussed as being closely linked during the World Café were combined according to logical content.
5) If a specific topic area was named or discussed within >3 separate NAM domains and could not be categorized according to the NAM domains, an additional domain was established for the topic area.
Results
The literature screening yielded 146 articles for patient safety, 109 for effectiveness, 84 for patient-centeredness, 41 for timeliness, 302 for equitability, and 78 for efficiency (see Appendix Table A.5). The starting list of items for the World Café contained 5 items for the patient safety domain, 6 for equitability, 4 for patient-centeredness, 5 for timeliness, 4 for effectiveness, and 5 for efficiency (see Appendix Table A.3).
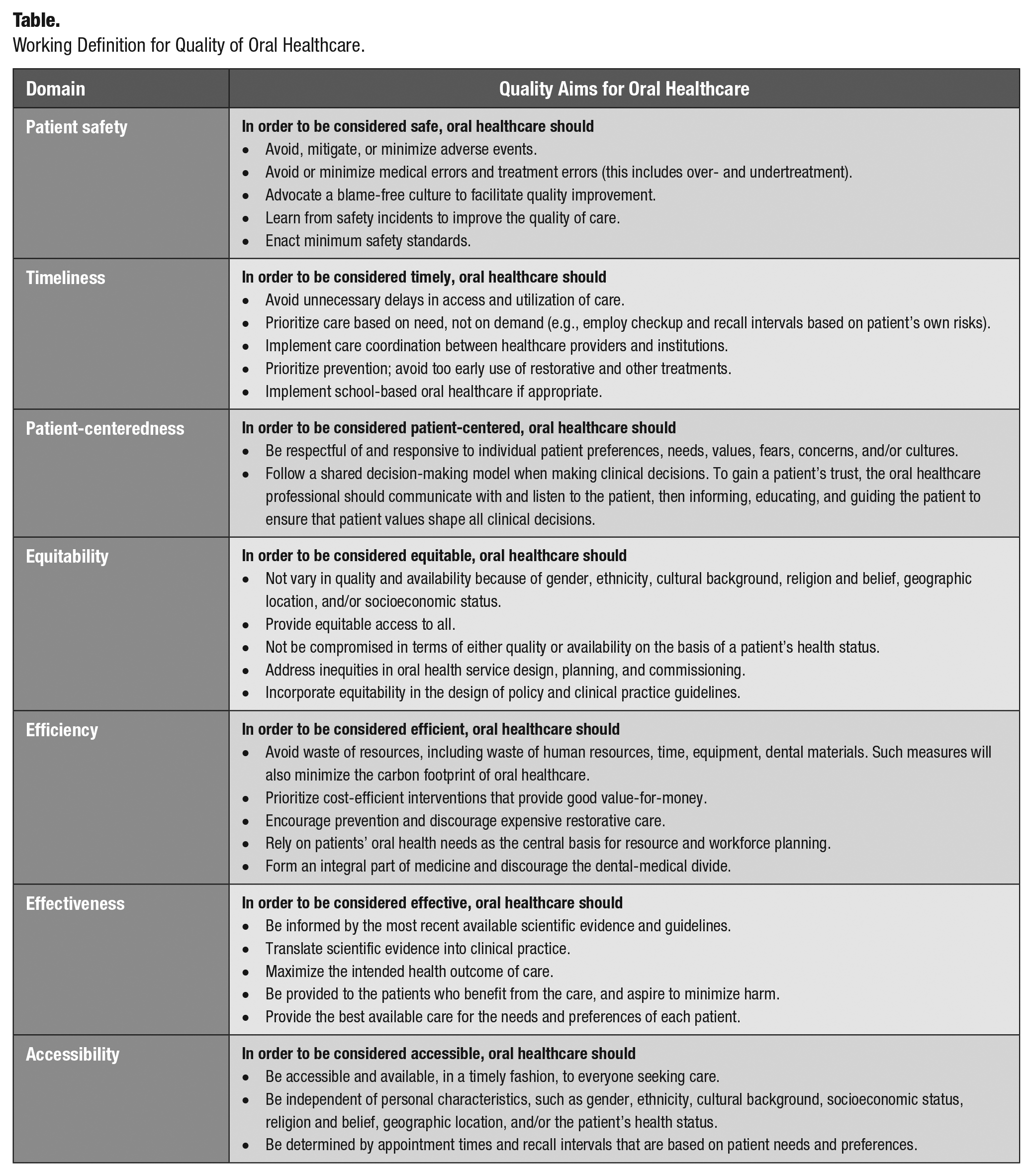
Out of the 50 workshop registrants, 25 participated in the World Café, of whom 20 subsequently participated in the voting procedure. The registrants’ countries ranged across all continents worldwide. The majority of participants were from high-income countries. Most registrants were native English speakers, and no language barriers were observed. The resulting list of the 5 most frequently voted items per domain are shown in Appendix Table A.6 (see Appendix Table A.7 for the complete list of items). Access to care was mentioned as a relevant aspect within all 6 initial domains. For 5 of the 6 initial domains, it was mentioned that the care provided should be tailored to the patient’s needs and preferences. Other topics that were discussed in >1 domain were acceptability of care, over- and underuse of services, and continuity of care. The working definition for quality of oral healthcare derived by this process is shown in the Table. It comprises 7 domains—patient safety, effectiveness, efficiency, patient-centeredness, equitability, timeliness, access to care—and 30 items.
Working Definition for Quality of Oral Healthcare.
Discussion
A novel 3-step approach was used to gather evidence from the literature and pool the collective intelligence of workshop participants at the 2018 IADR annual meeting. The proposed definition confirmed the relevance of the 6 domains to oral healthcare as identified by the NAM: equitability, patient safety, patient-centeredness, timeliness, effectiveness, and efficiency. In addition, a seventh domain of accessibility was incorporated into the working definition. These 7 domains of oral healthcare quality have the potential to encourage discussions about quality improvement.
A definition of quality of care can be of practical value for facilitating quality improvement activities. When core sets of quality measures are being developed, a comprehensive definition can help to ensure that all relevant aspects are being covered. With the growing number of measures currently being developed, decisions about which aspects of oral healthcare need to be measured should be driven by the most relevant aspects (Kalenderian et al. 2018). A recent systematic review suggests that various dimensions of quality of oral healthcare have been considered to various extents by different developers of quality of oral healthcare measures (Righolt et al. 2019). While societal preferences and expectations toward oral healthcare will continue to evolve, comprehensive, harmonized, and timely monitoring of oral health and care is highly relevant.
In this study, accessibility played an overarching role in each domain and was thus considered to be an important aspect of quality of oral healthcare. This could also reflect concerns in terms of room for improvement with respect to achieving more universal coverage for oral health. Although accessibility was not included as a separate domain of quality in the NAM framework, other frameworks have suggested access as a separate domain (see Appendix A.3). The needs and preferences of patients were also recurring themes in most domains. Thus far, patients have often been excluded from the development of quality measures, but all relevant stakeholders should be included to ensure collective responsibility for quality improvement. In this study, the items of quality of oral healthcare were presented in the domains as suggested by the participants. However, various items might also be categorized within other domains. For example, the items “implement school-based oral healthcare if appropriate” and “implement care coordination between healthcare providers and institutions” are both listed within the timeliness domain but could also be considered relevant within the accessibility and efficiency domains, respectively.
Limitations
Some limitations should be considered when interpreting the findings of this study. First, the group of participants consisted of researchers and oral healthcare professionals present at the conference. Most participants were native English speakers and came from high-income countries. More detailed information about the study participants’ backgrounds was not collected, and this limits the interpretability of the study findings in terms of applicability across various settings worldwide. To reach a broader consensus of what comprises quality of oral healthcare, the findings of this study should be tested with other stakeholder groups (especially with patients) and in different settings worldwide. Nevertheless, the findings provide a starting point to advance improvements related to quality of oral healthcare. Second, several video calls were organized among the moderators to decide whether participants should receive an initial list of topics that could be used as a starting point for the World Café (considering advantages, such as providing tangible input information to swiftly initiate thinking/discussions among workshop participants, vs. potential disadvantages, such as anchoring toward previously established concepts/measures of quality of care). After careful consideration, the moderators chose to use a topic list to make sure that participants were familiar with the most recently available scientific evidence. Another limitation is that the specifics listed within each domain of the working definition are not fully operational or readily measurable so far. Future work is warranted to make the definition operational.
Conclusion
In conclusion, this is the first study providing an aspirational working definition of quality of oral healthcare. It is hoped that this provides a step toward a broader consensus of what constitutes quality of oral healthcare and to facilitate additional conversations aiming at quality improvement. To advance quality improvements in oral healthcare, future research should evaluate the extent to which the working definition encompasses the perceptions of other stakeholder groups, such as patients and policy makers.
Author Contributions
A.J. Righolt, contributed to design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; M.F. Walji, J.S. Feine, D.M. Williams, contributed to design, data acquisition, analysis, and interpretation, critically revised the manuscript; E. Kalenderian, contributed to conception, design, data acquisition, analysis, and interpretation, critically revised the manuscript; S. Listl, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
DS_10.1177_2380084419875442 – Supplemental material for An International Working Definition for Quality of Oral Healthcare
Supplemental material, DS_10.1177_2380084419875442 for An International Working Definition for Quality of Oral Healthcare by A.J. Righolt, M.F. Walji, J.S. Feine, D.M. Williams, E. Kalenderian and S. Listl in JDR Clinical & Translational Research
Footnotes
Acknowledgements
We thank everyone who participated in the World Café for their valuable input.
A supplemental appendix to this article is available online.
The authors received no financial support and declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.