
Abstract
Smoking declines are uneven around the world, and we have few studies on the correlates of youth smoking in contexts like Saudi Arabia, where declines have been slowest. Using a broadly socio-ecological framework and network data, we report on one of the few studies to simultaneously examine peer, family, and school features associated with smoking in the Saudi context. We find strong and consistent peer and family associations with both occasional and regular smoking via direct modeling (level of peers/family that also smoke) and substantive interactions (lying to parents in the family domain, engaging in unsupervised youth-centric activities, or seeking popularity in the peer domain). Although our design precludes causal claims, our results are consistent with smoking initiation being driven by occasional use surrounding attempts to gain youth social status, whereas regular use depends on implicit family and peer acceptance.
Despite recent progress, smoking remains a significant health threat around the globe, with 2019 estimates of nearly 1.2 billion people smoking and 7.7 million tobacco-related deaths generating a cost of over a $1 trillion in health-related expenses worldwide (Dai, Gakidou, and Lopez 2022; GBD 2019 Tobacco Collaborators 2021). Smoking declines are most pronounced in high-income Western and European nations, and progress has been slower in developing countries in the Global South and Middle East, where the cost to health and economy are significant (Al-Zalabani 2020; Koronaiou et al. 2021). Unfortunately, improvements in smoking rates are somewhat offset by population growth and the long-acting reach of the disease, suggesting that the future burden on disease will remain significant for some time to come (World Health Organization [WHO] 2018). Saudi Arabia is one of the countries with little to no decline in smoking rates (GBD 2019 Tobacco Collaborators 2021), suggesting that understanding the social origins of smoking behavior in this context is necessary.
Smoking risks and health costs typically manifest late in life, but smoking initiation often starts when people are in their teens. Unfortunately, prevalence among young smokers remains stubbornly high around the globe (Reitsma et al. 2021). Although the trends have generally been good, recent estimates suggest that over 155 million people between age 15 and 24 are still smoking, with prevalence in this group remaining at around 20 percent, although variability across contexts is quite high. Given the difficulties associated with quitting tobacco once people regularly smoke, the best public health strategy continues to be prevention of habitual smoking in the first place.
Understanding the social contexts of smoking in young people is crucial in aiding efforts at smoking prevention (Al-Zalabani 2020; Monshi et al. 2023). Adolescence is a unique social period given that young people split their time between the family embeddedness typical of younger children and independent time spent with peers. During this time, adolescents are trying on behaviors that they perceive as conveying adult-like status and independence from parents while trying to gain status among their peers (Coleman 1961; Crosnoe 2011; Fuligni and Eccles 1993). Although we have many studies of the peer and social contexts for smoking behavior in Western European and American contexts (adams and Schaefer 2016; de la Haye et al. 2019; Mercken et al. 2010; Sohn, Moon and Kim 2024), there is less research on the contextual factors associated with youth smoking behavior in Middle Eastern countries.
Here, we provide evidence from a unique study of teen networks in Saudi Arabia on the contextual correlates of youth smoking. We examine family, peer, school, and healthy behavior contexts in an effort to better understand how different social features are related to smoking in this unique population. Because our study is one of the few to examine peer networks in this context, we take a broad exploratory approach to examining behaviors of close friends, family, and general health-relevant conditions and practices. We find that both family and peer environments have strong, independent associations with smoking (for both regular smoking and any smoking within the past year) even after accounting for various other activities. Within these environments, the strongest factors linked to any smoking in the past year include direct modeling behaviors, such as friends’ and parents’ smoking habits, and authority-oppositional activities, such as lying to parents and engaging in unsupervised behavior with peers. Regular smoking, however, is primarily associated with modeling behaviors from peers and family. Although our data collection design precludes a causal evaluation, these results are consistent with a process where initialization is driven by attempts to seek peer approval via generalized risk-taking, but smoking persistence requires the implicit acceptance of peers and family who also smoke. The fact that our results align closely with studies from Western contexts suggests that similar public health initiatives could be effective.
Background
Tobacco use is on the decline, with worldwide estimates dropping from 20.8 percent of people ages 15 to 24 years smoking in 2000 to 14.2 percent in 2020, although prevalence varies significantly by country and economic standing (WHO 2021). Research on the shifting trends in youth smoking over time reveals a complex interplay of factors driving the general decline across countries. Pampel and Aguilar (2008), using data on teens in the United States, identifies cigarette prices as a key factor in driving variation in smoking trends, whereas others underscore the role of negative social beliefs about smoking and intense public health efforts (East et al. 2021; Gilpin, Lee, and Pierce 2004). Work on the variation in trends suggests that smoking is a multifaceted outcome of different social contexts, so we adopt a broadly socio-ecological approach (Bronfenbrenner 1977; Kilanowski 2017) whereby actions are understood to be embedded in multiple social contexts that shape both opportunities and legitimacy for smoking behavior. Here, we examine four broad social contexts that likely affect smoking: family contexts, peer contexts, school contexts, and generalized health behavior (see also Al-Zalabani, 2015; Kim and Chun 2018).
Family Context and Smoking Behavior
Although we often focus on the adult-becoming aspects of teen identity, family influences are still among the strongest in predicting smoking. The direct association between parental activity and youth activity is clear: Parental and close adult family smoking is highly predictive of youth smoking (Al-Zalabani 2015; Jester et al. 2019; Mayhew, Flay, and Mott 2000; Turner, Mermelstein, and Flay 2004) both because parents model behavior that youth adopt and because parents’ smoking eases access to tobacco (DiFranza and Coleman 2001; Gendall et al. 2014).
In addition to the direct modeling of parental smoking, there are multiple indirect pathways that likely link family context and smoking independent of parental smoking. First, tense family relationships, lack of open communication, and frequent conflict can create stress and anxiety, making teens more likely to seek coping mechanisms like smoking (Fletcher and Sindelar 2012; Scales et al. 2009; Wills, Sandy, and Yaeger 2002). Similarly, low parental monitoring makes it easier for youth to engage in unsanctioned behavior because parents are less likely to know of and thus intervene in teen activity. In general, having more unstructured time has been found to be associated with delinquent activity and substance use through either increases in opportunities or lower parental discipline (Hoeben and Weerman 2016; Osgood and Anderson 2004; Osgood et al. 1996). Within the Saudi context, prior research finds that parents were perceived to be the first source and most important source for youth smoking (Almutairi 2014; Al-Zalabani 2015; Al-Zalabani and Kasim 2015).
Peer Context and Smoking Behavior
Teen friends provide key social and emotional resources to peers, including trust, social support, and solidarity (Korkiamäki 2016; Traylor et al. 2016; Weller 2007), and generally guide behavior (Maxwell 2002). Peers contribute to social behavior and identity in at least two ways. First, networks capture the set of people one interacts with, and identity as intersection of contacts is well established in sociological theories of identity (Blau and Schwartz 2018; Simmel 1955). Second, one’s place in a network captures a social style—a way of interacting that reflects shared understandings of what is right, valuable, and status-conferring—that is reinforced by reciprocity, intimacy, and status recognition with peers. This combination of who one interacts with and what they value shapes one’s position in the adolescent society (Coleman 1961; McFarland et al. 2014). Over time, peers expose each other to activities and preferences, and simple social balance mechanisms provide pressure to align behavior (Heider 1946; McPherson, Smith-Lovin, and Cook 2001) because people change behavior or friends as best suited to build overall consistency in their network (adams and Schaefer 2016; Hallinan 1974). Adolescence is a particularly rich time for these dynamics because as teens navigate the process of becoming adults, they look to each other to decide what sorts of behaviors are acceptable and identify what type of person they want to be (Crosnoe 2011; Fuligni and Eccles 1993).
Research on adolescent peer groups has highlighted two constantly significant factors. First, friends are much more like each other than they are like the population as a whole across almost any dimension of interest. Work on homophily has focused on multiple aspects and behaviors, such as aspirations and school involvement (Bain and Anderson 1974; Coleman 1961), deviant behavior (Hagan 1991; Ragan 2020), sexual activity (Billy and Udry 1985; Trinh et al. 2019), race (Hallinan and Williams 1989; Moody 2001; Neray, Copeland, and Moody 2023), and gender (Eder and Hallinan 1978). The underlying explanation for group similarity is contentious: Do people select similar friends, or do they influence friends to become similar? For the most part, the empirical answer is “both” (adams and Schaefer 2016; de la Haye et al. 2019; Kandel 1978). Second, friendships tend to form bounded peer groups—sets of kids who interact more with each other than with anyone else. Moreover, these groups are often centered on a set of core members and thus ordered with some level of hierarchy internal to the group and are often ordered between groups, implicating a desirable status hierarchy that students orient their action toward (Coleman 1961; McFarland et al. 2014; Moody et al. 2011). These groups develop subcultures that are signaled by their understanding of themselves, their choice in activities and music/cultural consumption, and substance use (Bobakova et al. 2012; Dunphy 1963; Mulder et al. 2010).
This general process has been studied extensively with respect to smoking and substance use, at least in American and European contexts (Alexander et al. 2001; Haas and Schaefer 2014; Henneberger, Mushonga, and Preston 2021; Huang, Lu, et al. 2014; Huang, Soto, et al. 2014; Kandel 1978; Osgood, Feinberg et al. 2013; Osgood, Rage et al. 2013; Ragan 2016; Schaefer, adams, and Hass 2013; Simons-Morton and Farhat 2010; Steglich et al. 2012; Valente, Unger, and Johnson 2005), although the findings are generally replicated in the small number of other Saudi and Middle Eastern studies available (Al-Zalabani 2015; Mohammed et al. 2019). Current research agrees that there is generally high peer similarity in substance use generally and smoking specifically (Kawaguchi 2004; Lundborg 2006; McVicar and Polanski 2014).
Much of the literature recently has focused on attempts to disentangle peer influence from peer selection (Friedkin 1998; Snijders 2017). Determining the balance of these two forces toward similarity is difficult because the behaviors are generally endogenous (Shalizi and Thomas 2011), with each causing the other. The current state-of-the-art modeling efforts, which make use of simulation-based models for balancing selection and influence in dynamic network data (Burk, Steglich, and Snijders 2007; Snijders, Van de Bunt, and Steglich 2010), suggest that both selection and influence contribute to smoking homophily. These models require dynamic data in which one observes change in both the friends people report and their behavior, which our cross-sectional study does not allow. As such, we cannot distinguish the relative contributions of selection and influence in peer smoking homophily, noting only that any observed homophily is likely due to both features simultaneously.
Saudi/Muslim Peer Context
Friendship holds a special place in traditional Muslim understandings, linked to the Islamic perception from the holy texts, both Quran and Hadith. In Islamic tradition, friendship was linked to spiritual harmony and religious influence, with affirmation of friends and peers on one’s goodness and purity. In Tafsir Al-Azhar (Quran interpretation by Al-Azhar), it is mentioned that sometimes good intentions and goals are constrained by the influence of friends because people have difficulty separating themselves from the relations around them and must thus choose friends who can lead them in a good direction (Hamka 1965).
Although there are fewer studies conducted on peer contexts in Muslim Middle Eastern contexts, the results we have are largely consistent with Western studies. Work in the Saudi context on peer reports of smoking confirms status homophily: Al-Zalabani and Kasim (2015) found that the factor with the highest association for smoking was that “most” or “all friends”’ also smoked. Although prevalence of cigarette smoking was comparatively low among adolescents in their sample, friends’ and parents’ smoking played an important role in increased smoking risk. Similarly, Almutairi (2014) argues that the main reason for smoking among adolescents was influence by friends, and Al-Zalabani (2015) found a positive association between smoking and both peer smoking and family smoking. Mohammed et al. (2019) find similar results in a longitudinal study of smoking initiation. Ismail (2016) studied friendship in secondary schools in Saudi Arabia and found that friendship provides a balance between cooperation and independence, helping adolescents navigate the transition to adulthood. Muslim culturally events, such as Ramadan and Eids, have been identified as significant contexts for attempts to quit smoking (Monshi et al. 2023).
School Context and Smoking
For most adolescents, schools are the key social context outside of their home. Schools aim to be health-protective: The school is generally actively supporting healthy behavior, enforcing nonsmoking policies, and generally promoting good health. As such, greater involvement in school activities tends to be associated with better health (Battistich and Hom 1997; Dornbusch et al. 2001; McBride et al. 1995; Nutbeam et al. 1993), which has also been shown in prior work on Saudi youth (Al-Zalabani 2015; Monshi et al. 2023). Prior work finds that school attachment and performance are generally negatively associated with tobacco use (Kim and Chun 2018). Others find that grades have clear negative effects on smoking, but feelings of attachment or bonding do not (Gaete, Montgomery, and Araya 2015). Sporting behavior associated with schools, such as being members of school teams and clubs, often comes with grade and behavior expectations that support good health and are likely negatively associated with smoking (Donato et al. 1997; Escobedo et al. 1993).
Mental Health and Healthy Behavior
Students suffering from depression and anxiety may turn to tobacco use. Prior work in teens shows that there is a strong positive correlation between tobacco use and depression/anxiety (Jorm et al. 1999; Patton et al. 1996). There is much debate on the causal direction of smoking and depression, and the two are likely endogenous (Mojtabai and Crum 2013; Steuber and Danner 2006) given that early smoking leads to depression and depressed smokers are less likely to quit (Berlin and Covey 2006; Glassman et al. 1990; Kinnunen et al. 1996; McKenzie et al. 2010; Niaura et al. 2001).
Finally, we anticipate that there will be a generalized correlation between smoking and other healthy behaviors because students who move in more health-conscious circles should be less likely to smoke (Hine et al. 1997). Generally, students who see health as valuable and worth perusing would be less likely to engage in any sort of unhealthy activity (Bojanowska and Kaczmarek 2022; Dieteren, Brouwer, and van Exel 2020; Lau, Hartman, and Ware 1986). Such effects are not necessarily causal; rather, these are endogenous features that are likely tied up with many similar characteristics, but controlling for them helps to ensure that we have as rigorous a test for family, school, and peer effects as possible within the constraints of a cross-sectional design.
The Current Study
Here, we examine correlates of smoking across multiple youth contexts in a unique sample of Saudi youth. Most work on smoking correlates has focused on Western and European contexts, with a small but growing body of work on Saudi contexts (Alasqah et al. 2019; Albangy, Mohamed, and Hammad 2019; Almutairi 2014; Al-Zalabani 2015; Al-Zalabani and Kasim 2015; Mohammed et al. 2019; Monshi et al. 2023), so this study provides a unique opportunity to see how well common correlates generalize to a new setting. Because adolescence is a time when initial health and behavior habits are formed, identifying the key contexts that correlate with smoking could help guide prevention strategies and future longitudinal work aimed at understanding causal associations between peers, family, school, and smoking behavior.
Data, Measures, and Modeling Approach
Data
Our data are collected from six high schools in urban and suburban Jeddah, KSA, as part of the Youth Health-Related Behaviors and Social Networks study (Copeland et al. 2021), which covered a wide set of activities and behaviors related to personal connections, way of life, and health. The Saudi education system has 12 grades, which are separated into elementary school (six years), middle school (three years), and high school (three years), when students are between generally between 15 and 18 years old (a;though irregular enrollment leads to somewhat wider age variation within grades than is typical in Western contexts). All Saudi adolescents have access to free public education from prekindergarten through high school, although private institutions normally charge an annual fee of $5,000 to $10,000. In comparison to public schools, private schools typically provide a broader variety of extracurricular activities and courses. Male and female pupils are rigidly separated into distinct campuses or schools within a school system (both represented in this sample). Although the school day is divided into several periods, students remain in the same classroom with the same classmates, and teachers move between classrooms.
This study included one boys’ and one girls’ high school from each type of school: public, private, and international. The sample was collected from six schools, and all enrolled 11th-grade students were allowed to participate, with 702 students completing some portion of the study, although some surveys failed to record to our Qualtrics base. The data used for this article is a cross-sectional ego-network design (Perry, Pescosolido, and Borgatti 2018), with each student naming up to six peers and then describing activities of each, including smoking behavior and expectations. Nominated peers need not attend the same school, although most did. Our analytic sample, excluding incomplete cases and nonresponse, contains 534 unique individuals. Comparisons across analytic and population distributions for variables included in the models show no substantive differences, and results are robust to both alternative sample specifications and imputation techniques (Allison 2000; Rubin 1987). Surveys were administered using online forms created in Qualtrics in Arabic, which were then translated back to English for analysis.
Measures
Table 1 includes descriptive statistics and definitions for all variables used in the model, for the sample as a whole, and for each of our smoking-level subgroups.
Descriptive Statistics by Smoking Status, Mean (SD).

Dependent variable: smoking behavior
We measure smoking in two ways. The first is whether the student reports any recent tobacco use (“any smoking”), which we calculate based on two questions. The first asked about any cigarette smoking over the last year, and the second asked specifically about three different tobacco types (cigarette, hookah, and shisha) in the last 30 days. Students who reported tobacco use in either question were coded yes for “any smoking.” We then coded as “regular smokers” any student who reported smoking cigarettes, hookah, or shisha once a week or more over the last 30 days. All regular smokers are also any smokers. About 33 percent (178/534) of our sample reported any tobacco use, whereas only 15.7 percent of our sample reported regular smoking.
Background and demographics
The average age of our sample is 16.8 years and evenly split by gender. Consistent with prior work (Budin et al. 2021), smokers trend a little older than nonsmokers, although the difference is small. Surprisingly, girls in our sample are somewhat more likely to say they have experimented with smoking than boys (63 percent), although regular smoking is substantively even (56 percent). We include indicators for living with their biological family, household size, and ethnically Saudi background. The sample is 91 percent ethnically Saudi, and Saudi respondents are somewhat overrepresented in the smoking categories.
Family context
Family smoking was based on the distribution of smoking among student kin. Students were asked if any of four types of close relatives (father, mother, brother, sister) smoked, and we coded the proportion of these that do such that a score of 1 indicates that a student has relations in each category that smoke and a score of 0 would imply they had none. There is a clear difference between the level of smoking family members for nonsmokers (17 percent) compared to regular smokers (35 percent). We use two measures related to family discipline and trust. In the first, we use a single question about how often they lie to their parents. For the second, we created a “parental independence” scale based on six questions related to how often parents let the youth make their own decisions about curfew, people they spend time with, TV shows they watch, bedtime on school nights, type of food they eat, and major at school. The scale has a Cronbach’s alpha of 0.67. Smoking students (any or regular) report higher levels of lying to parents than never smokers (2.6 [any], 2.7 [regular] vs. 1.53). Although there is some evidence of difference by parental independence, the differences are minor and inconsistent.
Peer context
We include an extensive set of measures related to peer smoking, markers for cultural consumption, and youth-related activities. The most direct indicator is a question asking, for each named peer, whether the student smokes (yes/no). We weight this score by how close the student says they are to each student (1 = not very, 4 = very). The resulting score is the weighted average, with a 4 meaning that all of their close friends smoke and a value of 0 meaning none of their friends smoke. There is a clear trend in Table 1 between peers smoking and respondent smoking (0.24 for nonsmokers, 1.16. for regular smokers).
We include a set of indicators for the social character and status of the peer group because we anticipate that smoking is one aspect of a “cool” youth persona (Michell and Amos 1997; Moody et al. 2011; Plumridge, Fitzgerald, and Abel 2002; Scheffels annd Tokle 2017). We asked each student to rate the popularity of their friends (0 = not, 3 = very) and asked each student weather they would rather be remembered among their mates as popular or smart. A set of questions also asked students what characteristics set their peer group apart, and initial examinations suggested that students who claimed “being best-looking” as one of their attributes had greater smoking activity than those who did not. We also students about many types of musical preferences, and those that listened to traditional Arabic music seemed to have distinctive smoking patterns. Finally, students with easier online access—via having an iPad or smartphone—were likely higher status than those who did not. Most of these indicators exhibit some association with smoking in Table 1.
Finally, we added two measures related to how students interact with peers. Students who report difficulty getting along with other students are self-reporting exclusion from regular student interaction, and prior work suggests that isolation is related to substance use (Copeland et al. 2018). For a more general indicator, we created a scale of how often students engaged in youth-centric, unsupervised activities based on three items: acting on a dare, going to parties, and hanging out with peers alone. The Cronbach’s alpha on this scale is 0.41, but exploratory factor analysis reveals that all three load on a single factor. When entered separately in the models in the following, they do not perform substantively differently than the scale, so we use that for simplicity here.
School context
We have three school-specific (nonpeer) related indicators to capture investment in school-sanctioned activities. The first is their self-reported grade point average (GPA) across six subjects. The second is a scale for school attachment (Bollen and Hoyle 1990) that ascertains how students self-assess their closeness to the school (three items; α = 0.68). The third asks for the number of sporting activities each student is engaged in. Nonsmoking students report higher GPAs and more sporting activities than smoking students.
Mental health and heathy behaviors
We use the 18 items from the Center for Epidemiologic Studies Depression Scale (CSDE; α = 0.83) as an indicator of mental health status and a pair of self-rated health questions to capture general health. Regular smokers report poorer mental and general health, although the differences are not particularly large. For healthy behavior, we include a series of questions about healthy diet in the prior week (five items; α = 0.42); nonsmoking students also report eating better than smokers.
Modeling Strategy
Given the wide range of potential variables to include, we take an exploratory modeling approach, starting by first assessing the bivariate associations with each measure, then entering the measures simultaneously within each of the different contextual domains, and finally, retaining those indicators that remain significant (at the p ≤ .10 level) in the domain-specific models for a final full model. Because our dependent variables are binary, we use logistic regression (Pampel 2020), although the results are substantively similar using linear probability models (Best and Wolf 2013). Although the nested nature of students in schools would often imply using a hierarchical model or similar school-based clustering, because school is perfectly correlated with gender in our sample, such models are difficult to fit. In gender-specific models, we have tested school-level random and fixed effects, and the data exhibit no systematic variation across schools, so we opt here for the simpler one-level model. Table 2 provides the any smoking models, and Table 3 provides the regular smoking models. Each table provides the base model coefficients in the original log-odds scale (change in log-odds of smoking for a 1 unit change in x) with standard errors and p values. Column 1 provides the bivariate association—each coefficient is from a model with simply the intercept and the row variable. Column 2 provides the coefficients for five different models—one for each of the domains, demarcated by the lines blocking out the table. Column 3 provides the model results for a single model retaining the significant variables from the prior model.
Logistic Regression Model Summaries for Any Smoking in Last 12 Months.

Note: Bivariate models include each variable in a separate model, block-level models include only variables within each context domain as discussed in text (five models total), and the final column is a single trimmed model. Standard errors are in parentheses.
p < 0.10. *p < .05. **p < .01. ***p < .001.
Logistic Regression Model summaries for Regular Smoking: Coefficient (SE) and p Values.

Note: Bivariate models include each variable in a separate model, block-level models include only variables within each context domain as discussed in text (five models total), and the final column is a single trimmed model.
p < 0.10. *p < .05. **p < .01. ***p < .001.
To aid in interpretation, Figures 1 and 2 provide coefficient plots using semi-standardized coefficients and their 95 percent confidence intervals, which provide the expected change in the log-odds of the dependent variable for a 1 SD change in the independent variable. Using semi-standardized effect sizes aids in comparing the substantive effect sizes across variables in the same model, allowing a rough guide on the comparative magnitude of each contextual feature. To retain the symmetry around null effects, we use the log-odds scale in the figures but have converted these to change in odds ratios (ORs) in the body of the text. All three modeling sets are layered on Figures 1 and 2, with the white points representing bivariate association, the light-gray points representing the domain-specific models, and the dark-gray points representing the full models. Variables that have been dropped in the final model are indicated by a dark circle with no confidence intervals, fixed at 0. Figures 3 and 4 provide predicted probability plots (with 95 percent confidence regions) for selected variables of interest for the final, full model. For space, we discuss the models jointly.

Model results for any smoking in the last 12 months: semi-standardized coefficients (log-odds) with confidence intervals.

Model results for regular smoking in the last month: semi-standardized coefficients (log-odds) with confidence intervals.

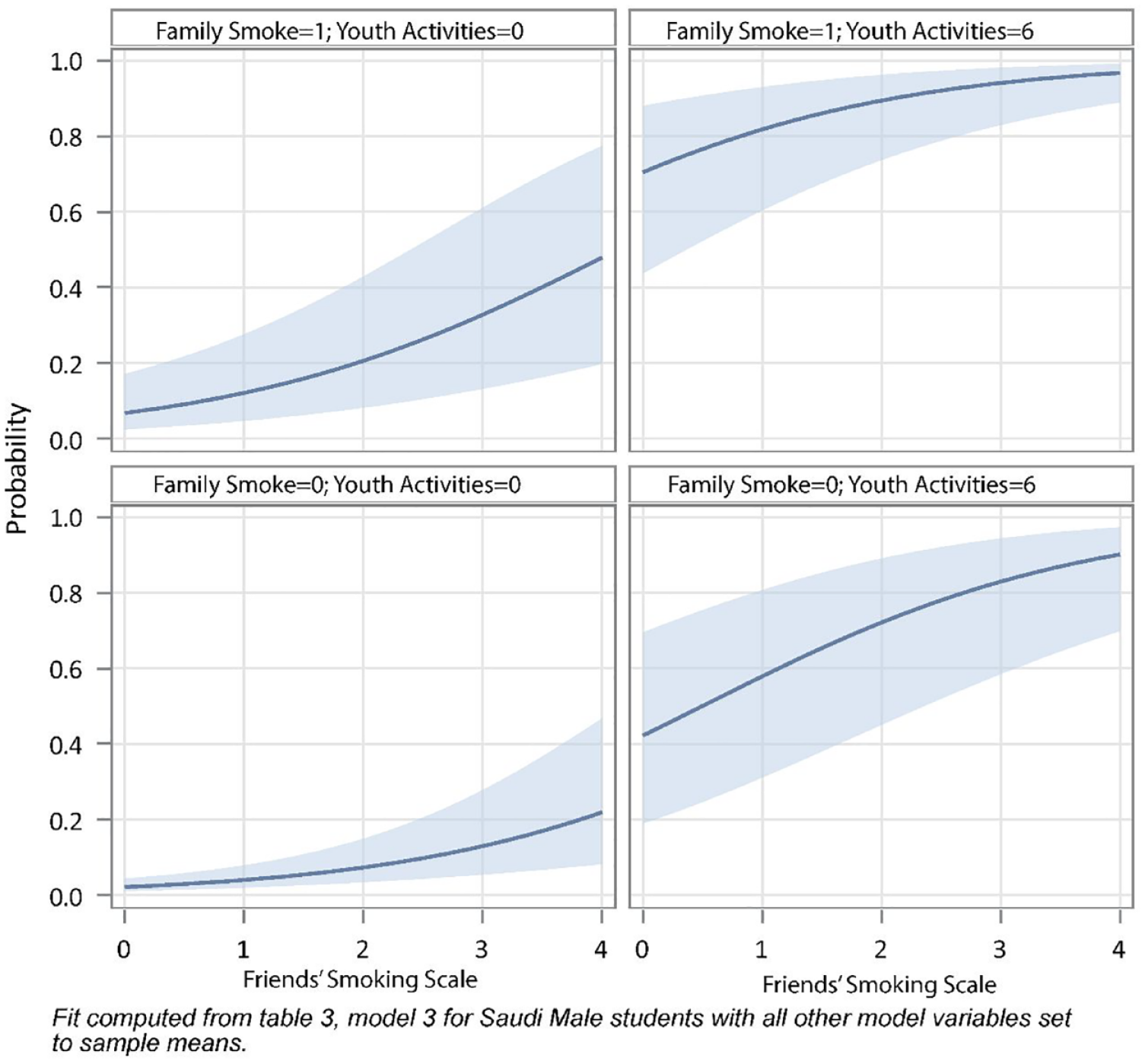
Predicted probability of reporting smoking in the last year by peer’s smoking, youth-centric activity, and family smoking.
Predicted probability of reporting regular smoking in the last year by peers’ smoking, youth-centric activity levels, and family smoking.
Results
Any Smoking
Demographic and background features
At the bivariate level, most of the demographic and background variables are associated with any smoking, a;though living with biological family is only significant at the .1 level (p = .08) and not retained in the final model (because 97 percent of our sample live with their biological family, the lack of significance is likely due to low power). As expected, older students are more likely to report smoking than younger students, and this association holds across models. Surprisingly, females are more likely to report any smoking activity in our sample than males, which may reflect inclusion of a wider set of culturally specific tabaco products (hookah and shisha), although the gender effect drops out of the final model.
Family context
Students from families with smokers are much more likely to report some smoking in the last year than students with families who do not, and this association remains significant and strong across the modeling frames. A 1 SD increase in the parental smoking scale increases the log-odds of reporting smoking by OR = 1.49 (95 percent confidence limit (CLM) = [1.18, 1.88]). Interestingly, the effect of students lying to parents is nearly as large in standardized effect size, with a 1 SD change in the lying scale resulting in OR = 1.62 (95 percent CLM = [1.27, 2.07]) change in the odds of reporting smoking. There is no effect of parental independence on reporting smoking.
Peer context
The proportion of peers who smoke is a strong and consistent predictor of smoking over the last year, and the effect size is larger than any other variable in the model based on the standardized coefficients. A 1 SD change in peer smoking increases the odds of the responded smoking by OR = 1.95 (95 percent CLM = [1.53, 2.49]) times. Items related to peer culture and popularity are generally related to the likelihood of smoking at the bivariate level but largely drop out once peer smoking and youth-centric activities are included in the models. For example, we see that students who prefer being known as popular rather than smart are significantly more likely to smoke at the bivariate level, and this is consistent controlling for other student activities (Model 2) but is not significant in the final model. Similarly, students who listen to traditional or shisha music are significantly more likely to smoke compared to those who do not, adjusting for nothing else in the model; but once we control for other features, the effect of a 1 SD increase drops to OR = 1.21 (95 percent CLM = [0.97, 1.51]). Similar patterns appear with claiming most attractive status for the peer group and having ready access to online resources.
In contrast, the scale capturing the amount of time students spend doing unsupervised youth-centric activities has a consistently strong positive effect on any smoking. For a 1 SD increase in the scale, the odds of smoking increase by OR = 1.68 (95 percent CLM = [1.31, 2.16]) times. The two consistent peer variables—peer smoking and the youth activities scale—likely outperform the specific cultural indicators because they are more general indicators for peer culture than any particular music or online activity. That is, although popularity-seeking students smoke more than academic students, some kids who smoke also prefer to get good grades. Similarly, although smokers disproportionately listen to traditional music, some smokers listen to contemporary music. This heterogeneity in specific markers for “being cool” adds noise to the signal that the more generic indicators for adult-like activities and direct smoking of close peers captures more succinctly.
School context
The variables associated with school context all show clear negative bivariate associations with smoking, but the effects are statistically weak, failing to reach traditional significance levels in the full model. In standardized form, the three variables (GPA, school attachment, and sports) have similar magnitude effect sizes in the bivariate and block-level models (all are about –0.15). But these effects are jointly significant in the domain-specific models only at the .1 level and do not reach statistical significance in the final models. This suggests that getting good grades, bonding with school, and/or engagement with sports in this setting are generally confounded with the peer and family contexts such that there is no independent effect in predicting smoking that is not already captured by youth activities and family context.
Health and healthy behavior
Health and health-related behaviors were examined as ways to help distinguish smoking-specific effects from generalized health status. For mental and general health, the pattern discussed in prior contexts is repeated: The variables are significant in the bivariate models, but the association moderates when other variables are added to the model. We find, for example, that students who score high on the CSDE depression/anxiety scale are more likely to smoke, but this effect diminished once other activities are entered into the model.
Health-conferring behavior, however, appears to be informative: Students who eat healthy diets in the prior week report significantly lower smoking, even controlling for family and peer context features. This hints at the idea that students may have internalized a healthy lifestyle perspective because finding an effect net of parental independence, family/peer smoking and youth activities suggests that the association is not due merely to hanging out in healthy settings. We cannot tell from these data for sure, of course, but these models are consistent with students internalizing a healthy identity that carries over to avoiding smoking.
Because OR changes are difficult to interpret absent deep knowledge of the base rates, Figure 3 provides the predicted probability of any smoking based on the coefficients in Model 3 of Table 2, highlighting differences by family and peer context. The x-axis in each subplot is the scale of peer smoking (0 = none, 4 = all close friend), the columns contrast students who are actively engaged with other youth-centric activities (right column) compared to those who have not engaged in any such activities (left column), and the rows index family smoking context (top row is families who smoke; bottom row is families that do not). In each plot, the dark line is the point prediction, and the shaded area is the 95 percent confidence region.
Figure 3 nicely illustrates how there are multiple routes to high-probability smoking. So, for example, an otherwise average student who has no peers that smoke but who engages in multiple youth-centric activities (Figure 3, left end of upper-right panel) has about the same probability of smoking as a student who has many smoking peers but engages in no such activities (Figure 3, right side of upper-left panel).
Regular Smoking
The regular smoking models are substantively quite similar to the any smoking models, but given that many fewer students report regular smoking, we have lower power, and the estimates are much less precise, meaning that although the magnitude of estimates is generally similar, fewer variables are statistically significant. Give our model selection design, this means that the final full model will include fewer covariates.
For background and demographic effects, the main difference with the any smoking models is that there is no gender difference in regular smoking. Within the family context, we again find a strong and positive effect of family smoking, but the effect diminishes somewhat in the final models. In the bivariate case, a 1 SD increase in family smoking increases the odds of regular smoking by OR = 1.77 (95 percent CLM = [1.43, 2.20]), but the semi-standardized effect size drops by nearly half (0.57 to 0.31; OR = 1.37, 95 percent CLM = [1.06, 1.76]) once other features are added to the model. In contrast, lying to one’s parents is a consistently strong predictor of regular smoking, even net of other variables in the model, such that a 1 SD increase in the parental lying scale increases the odds of smoking by OR = 1.41 (95 percent CLM = [1.09, 1.82]).
Among the peer context variables, again, engaging in youth-centric activities and having peers that smoke are the best predictors of regular smoking, and these are the two largest effects in the final model. A 1 SD increase in peers smoking increases the odds or regular smoking by OR = 1.75 (95 percent CLM = [1.39, 2.22]), whereas a 1 SD increase in youth-centric activities increases the odds by OR = 1.88 (95 percent CLM = [1.41, 2.50]). Based on the standardized effect sizes, peer effects have the strongest association with regular smoking among those included in the final model.
The pattern of effects for school factors differs somewhat for the regular smoking models, although none of the variables admit to significant independent effects in the final models. However, although GPA was fully unrelated to any smoking, suggesting that both strong and weak students experimented with smoking, the coefficient is strongly negative for GPA, such that a 1 SD increase in GPA would lead to an expected 13 percent decline (OR = 0.87) in regular smoking, although this effect is not statistically significant (95 percent CI = [0.66, 1.13]). Neither number of sporting activities nor attachment to school show any significant association with regular smoking.
Health and healthy behavior factors are in the expected direction, with students who eat healthily also being less likely to smoke regularly, and students who score high on depressive symptoms are similarly more likely to report smoking, although this effect is not statistically significant in the final model.
Figure 4 provides the predicted probability of regular smoking by peer and family context for otherwise average students, following the same layout pattern as Figure 3.
Compared to the any smoking models, the shift across columns is somewhat higher, reflecting the stronger effect of youth-centric activities in these models. For example, for students with no unsupervised peer activities, the probability of engaging in regular smoking is always low; even if all of their peers and family smoke (Figure 4, right side of upper-left panel), the probability of the student smoking is under 50 percent.
Conclusions, Limitations, and Future Work
Despite concerted, worldwide efforts over decades, youth smoking has remained stubbornly high. Although progress has been steady in many developed western nations, progress is generally slower if not completely stalled in other parts of the world, with Saudi Arabia making generally slow progress. Given that general information about the dangers of smoking and official prohibitions consistently admonish youth to not smoke, continued uptake of smoking is likely driven by unique family and peer contexts. In this study, using social network measures, we have reported on the association of smoking with peer, family, school, and health contexts in a unique sample of Saudi youth. We find that both occasional/experimental tobacco use over the last year and regular smoking are strongly correlated with peer and family activities: Students whose close family or close peers smoke are much more likely to report smoking themselves. Family and peer similarity in smoking is consistent with multiple direct influence mechanisms, including increased access to tobacco products, greater normative acceptance, and likely selection into homophilous groups for peers (selection is less likely for family effects, which plausibly predate teen activity).
Importantly, these direct modeling associations are complemented with other behaviors that hint at other social mechanisms. For family, we find a clear and strong association between a student’s propensity to lie to their parents and their likelihood of smoking. This may reflect students’ attempts to hide unsanctioned smoking activities from parents but likely reflects a broader propensity toward delinquency and rebellion that could drive seeking out adult-like behavior to signal independence (Gottfredson and Hirschi 1990). Interestingly, however, there was no effect of explicit independence from parents, at least as reflected in the extent to which parents allow students to make their own decisions about daily activities. This null finding is likely due to heterogeneity in the underlying causes of youth freedom: Some students make their own choices because parents (rightfully) trust them to make good choice, whereas other make their own choices despite parents’ wishes. Lying to parents, in contrast, is a clear indicator of opposition and subterfuge.
Similarly with peers, students who report doing youth-centric activities (e.g., acting on dares, hanging out unsupervised, or attending parties) are much more likely to report smoking. Our work replicates the evidence from Western studies that unsupervised time leads youth to engage in minor delinquency and unhealthy activities (Osgood and Anderson 2004). Again, the mechanisms may be multiple: Having time hanging out with friends allows students greater opportunity to find tobacco, but unsupervised time also opens the door for activities where students are primarily trying to impress (or at least not disappoint) each other, and these sorts of activities often confer status. This is corroborated by the suggestive effects of wanting to be thought of as “popular” within their school—tobacco use seems to track interest in gaining status in school (Moody et al. 2011).
Although the design limits of our study preclude making any causal claims, the combined effect of these results are consistent with prior work in Western contexts and suggest a general process whereby students, perhaps predisposed by extensive family exposure, engage in initial experimental smoking activity to gain popularity and peer acceptance and generally to fit in with peers. Students from smoking families likely have greater access (and hiding the smell may be easier), and lying to parents generally likely reinforces any oppositional tendencies that then increase smoking. Dabbling in smoking activity maps onto visible cultural identities—through music, for example—but these effects are epiphenomenal in comparison to the combined effects of peer and family modeling, popularity seeking, and family opposition.
Our study provides a rare opportunity to examine smoking correlates across multiple school and family contexts within Saudi Arabia. Still, like all studies, ours has significant limitations. Because the design is cross-sectional and relies on respondent reports of alter activity, we cannot disentangle selection and influence. Students with a propensity to smoke likely seek out smoking peers, and prior work has shown that both selection and influence are generally active in smoking initiation and that selection is particularly strong for continued smoking. We expect, as others have shown, that smoking and peer homophily are generally endogenous and mutually reinforcing, so disentangling the two is always going to be complicated. Similarly, although our sample includes a diverse set of schools, all cases are drawn from one region (Jeddah) of Saudi Arabia, and underlying smoking propensities likely vary across the country, particularly by an urban/rural gradient. Moreover, our sample of schools is small, making it impossible to estimate the effects of systematic school-level features, such as curricula type or public/private distinctions. As with any voluntary survey-based study, there are always concerns around reporting bias (students may not want to admit to deviant behavior, particularly in strict settings) and self-selection (students who engage in more smoking behavior may have opted out). Interviews were conducted by members of our team who were not formally associated with the schools sampled, so we hope that limited such features. Although our models included more covariates than most similar studies, there is always a risk of omitted confounders.
The broad outlines of our findings align with those of other studies conducted across diverse cultural contexts, including both Western and Middle Eastern regions. Peer and family smoking consistently emerge as strong predictors of youth smoking behavior. On one hand, the similarity in results across different contexts suggests that variations in peer and family dynamics are unlikely to explain the differences in smoking cessation levels between countries. On the other hand, this consistency implies that strategies leveraging peer and family influences could be effective in this context. For instance, research in the United States demonstrates that interventions designed to help students resist negative peer influence can significantly reduce smoking initiation (Osgood, Ragan et al. 2013). Additionally, peer-based interventions in various settings have been shown to be effective in promoting positive behaviors and reducing smoking rates, reinforcing the potential of these approaches in smoking prevention efforts worldwide (Sussman, Dent, and Stacy et al. 2004). Similarly, any effective large-scale public health interventions effects found effective for adults—such as increasing taxes on cigarettes—would likely have spillover effects on youth initialization via a decrease in family modeling behavior.
Future work can build on this study in multiple ways. First, larger nationally representative network studies would be a boon to adolescent research generally given that almost all work in this field has been conducted using Western and European samples. Longitudinal studies would allow one to examine the full trajectory of smoking behavior, helping to identify the set of activities that likely drive initiation within this context from those that foster continuation. Our models sought to do a little more than merely show homophily on smoking by including some indicators of how students interact with family and peers and how they generally approach health and healthy behavior. Although these hint at consistent mechanisms, the best way to extend this work would be with detailed qualitative research on the reasons why students start smoking, how they think about different tobacco delivery mechanisms, and what they perceive as the trade-offs between health, peer status, and family.
Footnotes
Acknowledgements
The authors thank the Deanship of Scientific Research, King Abdulaziz University for technical and financial support. We also thank the administration and students of the participating high schools in Jeddah (Alyusr, Anduls, Dar-Alfeker, The 42nd, Ibn-Khadun). We thank Gabriel Varela and Madelynn Wellons for comments on earlier drafts and Brent Curdy and Molly Copeland for insights on data and analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Deanship of Scientific Research, King Abdulaziz University, under Grant No. 2-125-36-HiCi.