
Abstract
Teleworking has become a popular work arrangement in many developed countries. Although there are heated public debates over the benefits of teleworking, empirical evidence on the causal relationship between teleworking and health is still rare. Using panel data from the German BAuA Working Time Survey (2015, 2017, and 2019), the authors investigated the effects of teleworking on health and well-being. The authors applied an innovative research design to underscore different sources of selection. Overall, no concrete evidence was found for the positive effect of teleworking on workers’ self-reported health, quality of sleep, and psychosomatic conditions. The ostensible better health outcomes among teleworkers could be partially explained by the positive selection on both prior levels and prior trajectories of health into teleworking. Moreover, the health impacts of telework were contingent on workers’ gender and parenthood status and the intensity of teleworking. These findings indicate that the positive association between teleworking and health appears to reflect selection bias rather than a causal relationship in Germany before the COVID-19 pandemic.
Telework, either at home or in any other place outside a company, has become increasingly common within modern economies, even before the COVID-19 pandemic (ILO 2020). For employees, telework provides a degree of control over when and where they work (Eurofound 2017). For employers, providing telework may be used to increase the family friendliness of companies and give workers more influence over their work, thus enhancing workers’ performance (Davis and Kalleberg 2006; Ortega 2009).
Much of the discussion on telework has stressed the positive effects of workplace flexibility on job satisfaction (Bloom et al. 2015) and work-life balance (e.g., Allen et al. 2013; Lott 2015). Workplace flexibility can improve work-life balance by allowing workers to adapt their work demands to the demands of their families (Lott 2015). Thus, it is conceivable that such flexibility is associated with less mental health issues, such as exhaustion or depressive symptoms. However, recent literature has stressed that jobs with schedule or location flexibility are associated with work intensification and less family friendliness (Kelliher and Anderson 2010; Mas and Pallais 2020), as well as presenteeism and social isolation (Tavares 2017). Furthermore, inadequate equipment and less ergonomic conditions when working from home could also result in health problems, such as headaches or back pain (Tavares 2017).
Although there is already meta-analytic evidence regarding the effects of workplace flexibility on work-life balance (Allen et al. 2013; Gajendran and Harrison 2007), there is a paucity of research on the effects of telework on health-related outcomes (Allen, Golden, and Shockley 2015; Oakman et al. 2020; Tavares 2017; Wöhrmann and Ebner 2021). Previous studies investigating the health factors of telework yield inconclusive, miniscule, or even insignificant correlations (Allen et al. 2015). Moreover, it has been shown that women are less likely to experience improved health when working at home (Oakman et al. 2020; Yang et al. 2023).
It should be noted that many studies on the relationship between telework and health are based on a small number of respondents or even focus on single industries or companies (Wöhrmann and Ebner 2021). More important, to the best of our knowledge, all previous studies are based on cross-sectional data, which renders the causal relationship between the two empirically inconclusive. Furthermore, none of these studies takes into consideration that access to telework is highly selective with respect to education, branches, occupations, and other characteristics that may be correlated with one’s current health or health development over the course of their lives.
These considerations lead us to conclude that the actual relationship between telework and physical and mental health is unknown. Moreover, it is an open question whether the effects of telework on one’s health are causal or just spurious. Spurious relationships reflect statistical associations resulting from different types of selection issues. Specifically, three types of selection issues can lead to a positive association between telework and health: (1) selection into both doing telework and having better health because of common factors (i.e., confounding), (2) self-selection among individuals with a higher level of health into telework, and (3) self-selection among individuals with a slower decline in health into telework.
Thus, our analysis improves upon earlier research by disentangling the causal effect of telework on individual health from their associational relationship that is driven by selection issues. We use novel three-wave panel data from 2015 to 2019 from Germany—the Bundesanstalt für Arbeitsschutz und Arbeitsmedizin (BAuA; Federal Institute for Occupational Safety and Health) Working Time Survey—that include detailed information on work and health (Wöhrmann, Brauner, and Alexandra Michel 2021). We apply stepwise regression model comparison between pooled ordinary least squares (POLS), fixed-effects (FE), and FE individual-slope (FEIS) models to evaluate the extent to which the estimated effects of telework are biased because of different types of selection issues. Our results suggest that the observed relationships between telework and better health outcomes, including better general health, better quality of sleep, and less psychosomatic conditions, are explained largely by selection effects. Persons with access to telework are selective with respect to socioeconomic conditions, familial situations, and their employment situations. After accounting for these factors and individual fixed effects, we conclude that there is no significant health impact of switching to telework.
Theoretical Considerations and Empirical Evidence
Telework is an arrangement where an employee works outside the employer’s premises, regardless of whether the work is done from home or on the move (Messenger et al. 2017), though in Germany, most telework is generally done from home (Pfisterer, Streim, and Hampe 2013). In Germany, the term telework was legally defined for the first time in 2016; thus, a general approval capability was also assumed (Deutscher Bundestag 2017).
The association between teleworking and health has been made in two different branches of literature. First, the association is addressed in literature concerned with both the sociology and psychology of work, in which working conditions are discussed as a possible mechanism linking telework and health. Second, the association is also discussed in the literature on work-family balance or work-life balance, which focuses on the compatibility of work, family, and other areas of life. In addition to these two theoretical perspectives, we add a third, in which we discuss the selection into telework and the possible associations with health.
Telework, Working Conditions, and Health
Theoretically, the relationship between telework and health can be described with the job demands-resources model (Bakker and Demerouti 2007; Demerouti et al. 2001). According to this model, the demand of a job requires certain physiological and/or psychological efforts. High job demands can exhaust physical and mental resources of employees, which can result in more health problems. Job resources, on the other hand, refer to functional aspects of a job that support goal attainment, promote personal growth, and minimize the physiological and psychological costs associated with job demands (Bakker and Demerouti 2007). Therefore, job resources can have an impact on the health of employees in that they mitigate the effects of job demands on job strain and increase motivation because they satisfy basic human needs for independence, competence, and relatedness (Wöhrmann and Ebner 2021:351).
Telework has the potential to improve employees’ working conditions through increased job resources and reduced job demands (Demerouti et al. 2001). In reality, however, working conditions associated with telework can have both positive and negative implications on one’s health. Several mechanisms related to working time and interaction with coworkers seem to be relevant to the association between telework and health (Wöhrmann and Ebner 2021).
From a positive perspective, many studies have shown that telework is associated with higher working time autonomy (Gajendran and Harrison 2007; Messenger et al. 2017; Tremblay 2002; Wöhrmann et al. 2021), and higher general autonomy at work (Sardeshmukh, Sharma, and Golden 2012). Telework may also help reduce time pressure (Vesala and Tuomivaara 2015). For example, teleworkers commute less often compared with those who cannot work from home. In addition to saving time, there may also be no obligation to arrive at work at a certain time (Gajendran and Harrison 2007). Higher working time autonomy may provide better job resources, while lower time pressure relates to lower job demand, both of which contribute to reducing mental and physical stress in the workplace (Bakker and Demerouti 2007).
From a negative perspective, some studies show that although telework gives workers higher temporal flexibility, it may carry the risk of blurring the boundary between work and family time. Teleworking can foster the temporal decoupling of working hours for team members, including supervisors, which can result in contacts for work-related issues outside normal working hours. Empirical results support this perspective, showing that teleworking is related to overtime (Glass and Noonan 2016), working in the evenings and/or on the weekends (Messenger et al. 2017), and boundaryless working hours (Wöhrmann et al. 2021). Furthermore, teleworking may affect employees’ social interaction with coworkers, not only leading to a reduction in the frequency of contact with colleagues but also changing quality of relationships through reduced cooperation and social support between employees (Gajendran and Harrison 2007). Spontaneous discussions, the exchange of informal information, and networking are less frequent among teleworkers (Cooper and Kurland 2002). Information technologies, including e-mails and Zoom meetings, can only compensate for personal contacts to a certain extent because of the lack of spontaneity and the challenge of conveying subtle emotions (Golden 2006). In summary, increased job demands resulting from boundaryless working hours and decreased job resources due to fewer social interactions in the workplace could impose negative impacts on teleworkers’ health (Wöhrmann and Ebner 2021).
Telework, Work-Life Balance, and Health
Teleworking and especially home-office working entail a softening and shifting of the boundaries between work and private life, so that both areas are increasingly interpenetrating. Flexible working has the potential to improve the compatibility of work and family or private life (work-family balance or work-life balance). If employees have the option of organizing their places of work or working hours, they can more easily reconcile gainful employment with their nonwork activities and commitments, thus avoiding the stresses associated with a poor work-life balance (Lott 2015).
If work demands negatively affect the family sphere (work-to-family conflict) or, conversely, family demands negatively affect work (family-to-work conflict), this is associated with reduced health, in particular poorer mental health (Kelloway, Gottlieb, and Barham 1999; Vinokur, Pierce, and Buck 1999), quality of life (Carlson, Kacmar, and Williams 2000; Frone, Yardley, and Markel 1997), and life satisfaction (Ernst Kossek and Ozeki 1998).
Overall, the empirical evidence suggests that flexible work is associated with better work-life balance, although the effect is relatively small (Lott 2015; Shockley and Allen 2007). The benefits are due mostly to time flexibility rather than other forms of flexibility, such as location flexibility, and are also largely limited to working women with high family responsibilities rather than working women in general or other categories of employees (Shockley and Allen 2007).
Sex- and Family-Specific Effects
As women still predominantly bear the burden of unpaid work, including household work and care (Blossfeld and Drobnič 2001; Drobnič and León 2014), the demands and resources at work are likely to have a different impact on women’s and men’s work-life integration and, thus, on their overall health. Because of prevailing gender norms, women may also have different expectations about how work and private life should be integrated. These different expectations of women and men may in turn lead to different levels of satisfaction with the integration of the two spheres of life, even if they have the same job demands or resources.
Studies on gender differences in working conditions and their role in work-life integration do not show consistent results. Some studies showed no gender differences (e.g., Bianchi and Milkie 2010; Ford, Heinen, and Langkamer 2007), whereas other studies have shown gender differences in the relationship between working conditions and health (Nomaguchi, Milkie, and Bianchi 2005; Robone, Jones, and Rice 2011), demonstrating that experiencing the same level of job demands leads to a greater work-life conflict for women than for men (Grönlund and Öun 2010). Ernst Kossek and Ozeki (1998) showed that work-family conflict is more strongly related to life satisfaction for women than for men.
As job demands affect women and men differently, it is also likely that workplace resources have different impacts on women’s and men’s health. Because of their higher involvement in the household, especially if children are present, it can be assumed that, for women, telework may have a greater impact on their health than for men.
The German Legal Context and Selective Access to Telework
Unlike in some European Union countries, Germany does not (yet) have a legal right to work in a home office (teleworking). That means, German workers’ entitlement to telework depends on the negotiation between employees and employers in individual employment contracts, company agreements, or less often in collective agreements. In the German legal context, the supply of flexible work, including telework, should follow three principles of distributive justice: “need,” “equity,” and “equality” (Swanberg, Pitt-Catsouphes, and Drescher-Burke 2005). If employers are interested in accommodating employees’ family needs, those with corresponding needs will get access. The equity principle implies that access to flexible work is proportional to work performance; the higher the (expected) performance, the more likely flexible work will be made available. According to the equality principle, all workers should be granted equal access to flexible work, regardless of individual characteristics or status.
As women still bear the primary burden of domestic tasks, it is often assumed that women in particular demand teleworking and that it is also made possible according to the need principle. However, numerous studies have shown that men are more likely to work from home and telework than women. Parental status and family care responsibilities also play little role in access to flexible working hours (Chung and Van der Lippe 2020). What really matters is the level of education: highly qualified workers are more often found in flexible work (Wiß 2017). The few studies that take work characteristics (occupation and sector) into account suggest that these are more important than demographic or family factors in explaining the distribution of flexible work (Ortega 2009).
Access to telework based on the equity principle implies not only work output but also performance with respect to health determine one’s probability of teleworking. According to this principle, workers with better health are more likely to be granted the opportunity to telework because healthy workers are expected to have higher performance with this type of flexible work arrangement. Furthermore, people might be selected into telework not only because of their actual health but also because of unobservable traits promoting future health. According to the biopsychosocial model of health first proposed by Engel (1977), these include biological, psychological, and social risks and resources (Karunamuni, Imayama, and Goonetilleke 2021). Biological risks include factors such as lack of exercise and poor diet, while psychological risks include attitudes such as pessimism. Social resources include familial support and a good social network.
Hence, even if there is no causal effect of telework on health, the selection process might nevertheless produce a spurious correlation. Moreover, there are implications of the selection arguments for the time path of health that have not been discussed in the literature before. It may be that people with good health trajectories, wherein health conditions are improving or are at least not deteriorating, are more likely to be (self-)selected into telework. In this case, the preteleworking health trajectory of teleworkers has a milder declining trend over ages compared with nonteleworkers. In summary, even if teleworking per se affects neither the level nor the growth of health, the selection procedures mentioned above might still produce better health outcomes of teleworkers over nonteleworkers. We term this selection-induced group difference the “healthy teleworkers hypothesis.” The methodological implication is that ignoring these selections of telework will produce spurious causal effect estimates.
Method
Data and Sample
The empirical analyses were based on the BAuA Working Time Survey on behalf of the BAuA, conducted in 2015 (BAuA-AZB2015_1, https://doi.org/10.21934/baua.azb15.suf.1), 2017 (BAuA-AZB2017_1, https://doi.org/10.21934/baua.azb17.suf.1), and 2019 (https://doi.org/10.48697/baua.azb19.suf.1) in Germany. The data were accessed via scientific-use files provided by BAuA. For data documentation, see Brauner et al. (2019a, 2019b) and Pattloch et al. (2021).
The interviews were conducted via computer-assisted telephone interviews based on randomly generated landline and mobile numbers by the Infas Institute for Applied Social Sciences. The interviews lasted an average of 35 minutes and covered a wide range of topics related to work and well-being, with a particular focus on issues related to working time. The survey focused on the organization of working time and related health aspects, as well as physical and mental stress. It is a representative panel survey of people aged 15 years and older who work at least 10 hours per week in paid employment. In addition to persons subject to social security contributions, the population includes, among others, self-employed persons, and assisting family members. In 2015, a total of 20,030 interviews were conducted, which corresponds to a response rate of approximately 33 percent (Brauner et al. 2019b). In the second and third waves, a total of 10,459 and 10,540 interviews were carried out, including a panel refreshment of 22.4 percent in 2017 and 21.4 percent in 2019 (Wöhrmann et al. 2021). A nonresponse analysis based on 1,353 persons who refused participation in the survey but agreed to answer few questions found only minor differences between the original sample and the nonresponse sample in terms of sex, age, education, average hours worked, occupational status, or whether the respondent worked in an intellectual or manual job (Häring et al. 2016).
The initial sample for our empirical analyses consisted of 38,964 individuals. We dropped persons younger than 18 years and older than 65 years from the sample (n = 38,061 remained), as well as persons without valid information on telework (n = 34,677 remained).
Measures
Telework
Our central measure of treatment is represented by a dummy variable for an agreement of teleworking or home-office work with the employer.
To account for the strength of the treatment, we accounted for the number of days per week where the respondents teleworked on average (up to one day, up to three days, more than three days).
Health
The different dimensions of self-reported health, including general health, quality of sleep, and psychosomatic health, were captured with three measures:
“How would you describe your general state of health?” The five-point answer scale was recoded such that higher values indicated better health (1 = “very bad,”, 5 = “very good”). Self-rated health is the most widely used, validated, single-item indicator of health status across social science research that independently predicts morbidity and mortality (Idler and Benyamini 1997; Jylhä 2009).
“How would you rate your sleep in the last week?” The five-point answer scale was again recoded with higher values indicating better health (1 = “very bad,”, 5 = “very good”). The item is similar to the Pittsburgh Sleep Quality Index, which uses a four-point scale and asks about the last month (Buysse et al. 1989). The association between sleep problems and physical and mental health–related quality of life has been well documented (Carpi, Cianfarani, and Vestri 2022).
The third measure is a summary index of psychosomatic disorders based on a list of health complaints following Franke (2015) and Wöhrmann and Ebner (2021). Participants were asked to indicate whether the following eight health issues occurred frequently in the past 12 months while working or on workdays: headache; fatigue, weariness, or lassitude; stomach and digestion problems; tension and irritability; sleep disorders; dejection; physical exhaustion; and emotional exhaustion. Thus, the index ranges from 0 (none of the psychosomatic health issues) to 8 (all of the psychosomatic health issues). Cronbach’s α coefficient for this index of psychosomatic disorders is .768.
Controls
All analyses control for a set of variables that could confound the relationship between telework and health. As the share of teleworking persons increased over time, we controlled for period effects using dummy variables. To control for age effects and other demographic characteristics, we included in the models individuals’ age (continuous), the presence of a partner (binary: yes or no), the presence of children younger than 18 years in the household (binary: yes or no), educational degree (categorical: low, medium, or high), and vocational training qualifications (categorical: none, low, medium, or high). 1
To allow international comparison, we converted the German educational degrees to the International Standard Classification of Education (ISCED) 2011 scale and recoded it into three categories: low, ISCED 0 to 2; medium, ISCED 3 and 4; and high, ISCED 5 to 8. Guidelines for this procedure be found on the Web site of the Federal Ministry of Education and Research (https://www.datenportal.bmbf.de/portal/de/G293.html).
We also controlled for workplace-related confounders, including work hours per week (continuous), occupation, and firm size. The occupation variable was recoded into nine major categories following the International Standard Classification of Occupations (ISCO) 2008: (1) managers; (2) professionals; (3) technicians and associate professionals; (4) clerical support workers; (5) service and sales workers; (6) skilled agricultural, forestry, and fishery workers; (7) craft and related trades workers; (8) plant and machine operators and assemblers; and (9) elementary occupations. Full lists of occupations in each subcategory can be found at https://isco-ilo.netlify.app/en/isco-08/. Firm size was recoded into three categories: (1) 1 to 49 employees, (2) 50 to 499 employees, and (3) 500 or more employees.
Descriptive information on the development of the prevalence of telework for women and men is presented in Figure 1. Figure 2 shows means and confidence intervals of the gender-specific health outcomes of the three panels. The means of the variables in our panel analyses for men and women both in and not in telework are depicted in Table A1 in the Appendix.

Proportion men and women in telework in 2015, 2017, and 2019 with 95 percent confidence intervals.

Mean health of men and women by telework with 95 percent confidence intervals.
Models
To assess the causal effect of telework and home-office work (treatment) on health (outcome), and to account for selection into treatment on the basis of the level of outcome, as well as on the trend (slope) of the outcome, three different models were estimated. First, we used POLS models to investigate the effect of telework on health netting of observable confounding variables. Second, we used FE panel models to control for unmeasured time-constant characteristics of workers that could affect both the likelihood of telework and health. Using a within-estimation methodology, FE models can better account for the baseline differences between teleworkers and others, thus ruling out the selection into telework on the basis of the level of health. Third, we used FEIS models to further account for (self-)selection into telework on the basis of the growth of health (Ludwig and Brüderl 2018; Rüttenauer and Ludwig 2023).
The data generation process (DGP) of POLS and FE models to estimate the effect of teleworking (x) on health outcomes (y) of person (i) at time (t) is given in equation 1:

where α
i
is a person-specific time-constant unobserved characteristic that influences the outcome variable yi, and ε
it
is a time-varying idiosyncratic error term. In the POLS model, the estimated coefficient
The exogeneity assumption (1) needed for POLS is relaxed in the case of the FE estimator. Through a within-transformation procedure, where each variable in the DGP is demeaned by individual mean values,
Although the conventional FE estimator is already a large improvement compared with POLS in estimating causal effects, it still yields biased estimates when the strict exogeneity assumption does not hold, either by omitting time-varying unobserved confounders or in the presence of heterogeneous outcome trends in the treatment and control groups (i.e., violation of the parallel trend assumption). To further address the latter issue, several authors (Brüderl and Ludwig 2015; Rüttenauer and Ludwig 2023; Wooldridge 2010) have proposed the FEIS model. The DGP of FEIS is given by

where individual slopes αi2 account for the average growth trajectories of yit regarding changes in the baseline variable w. In the context in which age is specified as w, the FEIS models account for selection into telework on the basis of different age trajectories of health. The conventional FE model is a special case of the FEIS model in which the unobservables related to telework can be subsumed in the individual intercepts. If selection operates only on health levels, FE and FEIS produce identical point estimates. However, if selection additionally operates on health trajectories over time, the FE estimator produces biased estimates.
Note that FEIS is a “data hungry” method (Rüttenauer and Ludwig 2023) that requires relatively long panels, precisely T > J, where J is the number of specified slope parameters. To fulfill the data requirements in the estimation process, we modeled αi2 using age as a linear variable. In the present data context featuring a relatively short panel (i.e., only covering four year), a linear specification of age slopes should suffice.
Finally, we split the analytical sample by gender and ran separate models for female and male respondents because the relationships between our dependent and independent variables (including the control variables) may, in theory, differ by gender. Instead of running regressions with multiple interaction terms for all predictors, our strategy provides gender-specific coefficients for all independent variables in a parsimonious way. All models were estimated using Stata 17.0. For the FEIS models, we applied the module XTFEIS of Ludwig (2015).
Descriptive Statistics
(Self-)Selection in telework
Although access to telework and home-office work increased significantly over time for both men and women, men were significantly more likely to have access to telework and home-office work in each single year (Figure 1). In 2019, 25 percent of male employees were teleworking compared with 18 percent of female employees. Additional analysis reveals that the transition to telework and home-office work was 7 percent for women and 9.3 percent for men. Overall, men seem to be more likely to telework than women.
For an initial assessment of the question of (self-)selection into specific forms of work, we examined at the distribution of men and women with different individual, familial, and occupational characteristics. Younger (actually middle-aged) workers had a higher proportion doing telework (Figure A1). Men and women with low education and medium education were less likely to be found in teleworking. In contrast, persons with high education were more likely to have the agreements for home or telework. Gender inequality in terms of home-office work is found in all educational groups. Regarding the possible need of home-office and telework, women and men with children younger than 18 years in the household reported a significantly greater access than persons without children in the household (Figure A2). Moreover, both women and men with a partner in the household engaged more often in home-office work compared with persons without partners.
There is also a clear gradient in telework across vocational training lines (Figure A2). Interestingly, persons of both sexes with the highest levels of vocational training (university degree, doctorate) were significantly less likely to engage in home-office work compared with persons with intermediate levels of vocational training. In terms of working hours, a relatively large proportion of telework arrangements were observed among women and men who worked more than 50 hours per week. Moreover, those who worked in large firms (i.e., ≥500 employees) were more likely to telework. Finally, in terms of occupational distribution of teleworking, male and female managers and professionals were the most likely to work from home.
Association between Telework and Health
Figure 2 shows the distribution of health for women and men in employment situations with and without the possibility of teleworking. In terms of general health, there are clear differences for women and men with and without the option of teleworking. On average, people with the option of teleworking reported significantly better general health compared with those without this option. The sleep quality of those in telework was also better than those not in telework, although statistically significant health differences were only found for men.
Concerning the number of psychosomatic health problems, there were different patterns for men and women doing or not doing telework. Women in telework did not differ from those not in telework regarding psychosomatic problems. However, for teleworking men, the number of psychosomatic complaints was significantly lower than those not teleworking.
In summary, the descriptive results indicate that men and women in telework show better general health and sleep quality than those who do not telework. Regarding the number of psychosomatic complaints, only men in telework seemed to be better off; for women no significant differences were found.
Multivariate Regression Analyses
Causal and (Self-)Selection Effects of Telework on Health
The estimated coefficients of telework on different indicators of health based on the three statistical models are depicted in Figure 3 (see Appendix Tables A2–A4 for full regression results). The point estimates and the 95 percent confidence intervals of the POLS model, the FE models, and the FEIS models are presented. We also report in the Appendix tables the effect sizes in terms of standardized mean difference (i.e., Cohen’s d) to enhance the evaluation of our results’ practical significance (Sullivan and Feinn 2012). All models were separately estimated for women and men and controlled for a set of confounders discussed in the previous section.

Pooled ordinary least squares (POLS), fixed-effects (FE), and FE individual-slope (FEIS) models of telework on general health, sleep quality, and psychosomatic symptoms for women and men with 95 percent confidence intervals.
According to the POLS models, which control for common observable factors of telework and health, there were positive and statistically significant effects of telework on general health for both women (β = 0.08, p = .004, d = 0.086) and men (β = 0.05, p = .020, d = 0.058). Similar patterns were also found regarding men’s sleep quality, where teleworking had statistically significant effect for men (β = 0.07, p = .016, d = 0.060). Finally, according to the POLS models, teleworking was associated with lower psychosomatic symptoms for women (β = −0.08, p = .294, d = −0.033) and for men (β = −0.11, p = .056, d = −0.050), although both effects were not statistically significant. In summary, results from the POLS models were generally in line with the conventional expectation that teleworking might lead to better health outcomes, although the effect sizes are mostly very small.
However, the POLS estimates could be biased at the presence of omitted unobserved variables and self-selections. An FE estimator, in contrast, can largely address the biases resulting from omitted variables because it rules out the individual FE α i in equation 1, which includes unobserved time-constant confounders such as personality or family background. Indeed, the F tests on α i = 0 in our FE models (available on request) provide evidence of the existence of individual FEs, which favors the use of FE over POLS models.
According to our FE models, teleworking had positively small yet statistically non-significant effects on general health for women (β = 0.01, p = .799, d = 0.013) and men (β = 0.05, p = .222, d = 0.054). More interestingly, the estimated effects of teleworking on sleep quality and psychosomatic symptoms differed between the POLS and the FE models, especially for men. For men, the positive effect of teleworking on sleep quality found in the POLS model vanished in the FE model (β = 0.01, p = .839, d = 0.009), and the negative effect of teleworking on men’s psychosomatic symptoms became positive (β = 0.07, p = .399, d = 0.033). In summary, differences between the FE and POLS modeling results might indicate a positive selection of pretreatment health levels into teleworking: women who had better health and men who had better sleep quality or fewer psychosomatic symptoms were more likely to telework. Without accounting for this selection, the POLS model likely overestimated the positive effect of teleworking on improving worker’s health and well-being.
Moving beyond the FE models, the FEIS models provided further information about the presence of heterogeneous growth curves in outcomes that were related to the parameter of interest (Rüttenauer and Ludwig 2023). We first performed the Hausman-like artificial regression test to check for heterogeneous age slopes of outcomes (Rüttenauer and Ludwig 2023). The test results indicated the presence of heterogeneous growth curves in health and well-being, especially in the models of sleep quality and psychosomatic symptoms. Specifically, the between-individual differences in the age growth curves were statistically significant in women’s sleep quality (χ2 = 77.04, p < .001), men’s sleep quality (χ2 = 29.89, p = .094), and women’s psychosomatic symptoms (χ2 = 54.54, p < .001). The presence of heterogeneous growth curves, if not accounted for, would correlate with the treatment variables in the FE models and thus bias the parameter estimates. Therefore, in the following we focused on the comparison between the FE and the FEIS estimation results in these two aspects (i.e., sleep quality and psychosomatic symptoms).
Regarding sleep quality, we found that implementing FEIS yield mixed results across genders. For women, FEIS estimated a more positive effect of telework on sleep quality (β = 0.04, p = .757, d = 0.039) than the FE models. Although the effect was statistically insignificant, such a difference indicated a negative selection on female pretreatment sleep trajectories into telework. That is, women who experienced more negative sleep trajectories were more likely to engage in teleworking. For men, we found an opposite story. The FEIS model estimated a more negative yet insignificant effect of telework on sleep quality (β = −0.07, p = .409, d = −0.069) than the FE model, indicating a positive selection on male pretreatment health trajectories into telework.
A more striking result was found in the psychosomatic symptoms models. The FEIS models estimated much more positive effects of telework on the number of psychosomatic symptoms than the FE models for both women (β = 0.50, p = .029, d = 0.213) and men (β = 0.28, p = .125, d = 0.126). The differences between the FE and FEIS estimates indicated a negative selection on pretreatment symptom growths into teleworking. That is, women and men who were in a better aging track of a smoother growth of psychosomatic symptoms were more likely to be teleworking. This pattern supports the “healthy teleworker hypothesis” that people with good health trajectories were more likely to (self-)select into teleworking. Without concerning the pretreatment slope differences, the FE models could underestimate the effect of telework on increasing psychosomatic symptoms.
Although the FEIS is, in theory, a preferable estimator compared with FE and POLS, one should notice that implementing the FEIS estimator comes with the cost of losing sample cases that had less than three panel observations. This empirical limitation is especially problematic for statistical analyses using short-running panel data such as BAuA because it may lead to considerably larger confidence intervals in the FEIS estimation. This was the major reason why our FEIS estimates had high statistical uncertainty and could not reach the threshold of statistical significance (except for the model of women’s psychosomatic symptoms). Therefore, we suggested using the more conservative results from the FE models as the benchmark when concluding the health and well-being effects of teleworking, while using the FEIS results to detect potential selection on the pretreatment trend. Accordingly, in the following sections, we presented the FE modeling results for the additional analyses on effect heterogeneity by treatment intensity and parenthood status.
Effect Heterogeneity by the Intensity of Teleworking
To explore whether the effects of teleworking on health and well-being differ by treatment intensity, we regressed the outcome variables on a trichotomous treatment variable that differentiates between those who telework for only one day, for up to three days, and for more than three days per week. Using the FE estimator and the same set of control variables, the results are presented in Figure 4 (see Appendix Table A5 for full regression results).

Fixed effects of days in telework on general health, sleep quality, and psychosomatic symptoms for women and men (95 percent confidence intervals).
For women, the effects of teleworking on general health and sleep quality became more negative with an increased number of days teleworking, especially for women’s general health by teleworking more than three days a week (β = −0.24, p = .043, d = 0.249). For men, however, teleworking three or more days per week had a more positive effect on general health and sleep quality compared with the effect of teleworking for only one day per week. Regarding the impacts on psychosomatic symptoms, we found that teleworking for three or more days per week could significantly increase women’s psychosomatic symptoms (β = .50, p = .050, d = 0.214). For men, the effects of teleworking on psychosomatic symptoms were all similar regardless of the intensity. In summary, more days of teleworking seemed to benefit men’s health and well-being but harm those of women.
Effect Heterogeneity by Individual Parenthood Status
The moderating effect of one’s family background was investigated with separate estimates of the FE models of general health, sleep quality, and psychosomatic symptoms for men and women with and without children in the household. Estimation results are displayed in Figure 5. The full models were printed in Table A6 in the Appendix.
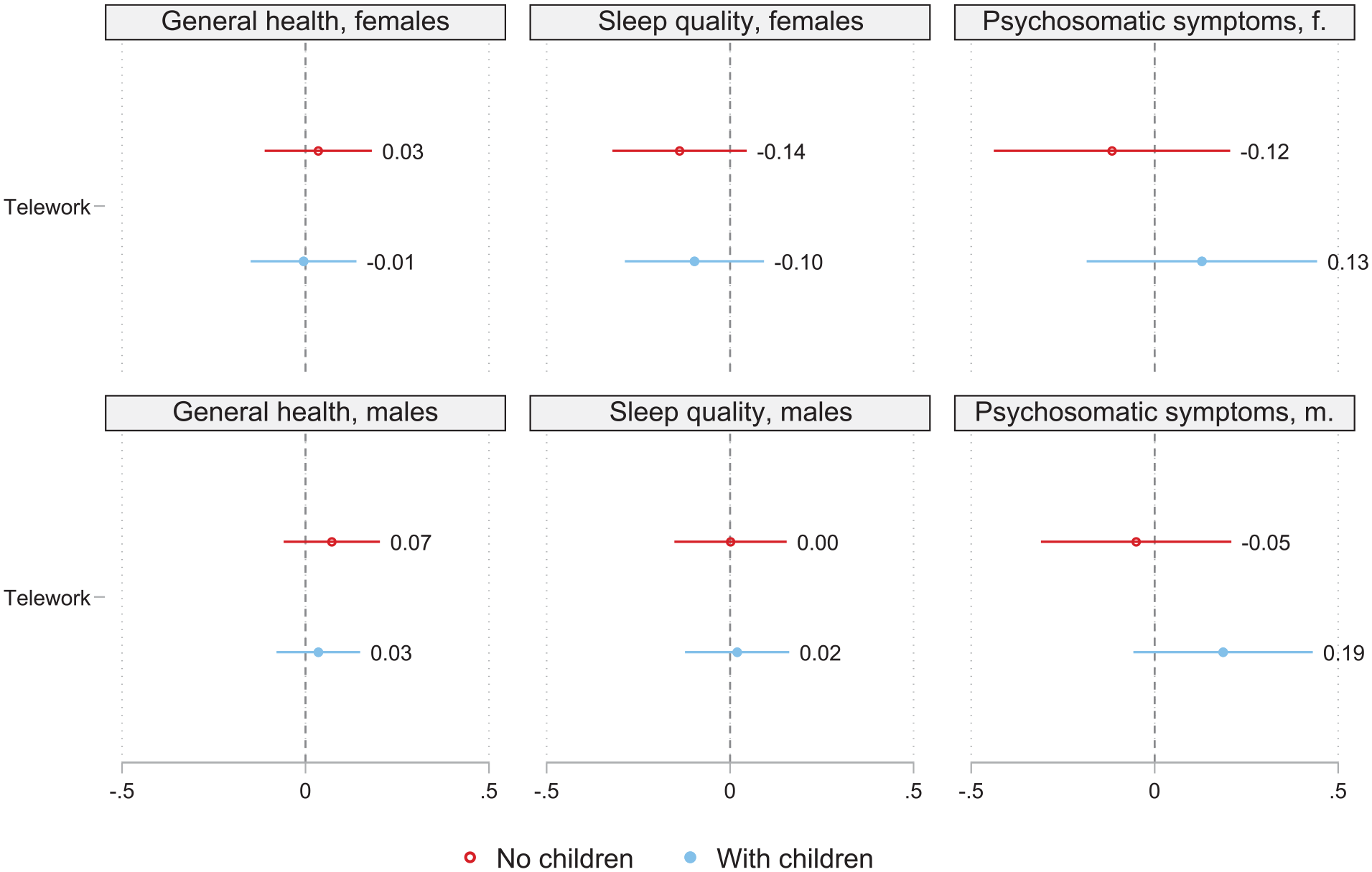
Fixed effects of telework on general health, sleep quality, and psychosomatic symptoms for women and men with and without children in the household with 95 percent confidence intervals.
For both sexes, we found no substantial differences in the estimated effects of teleworking on general health and sleep quality. Nevertheless, our models did show that teleworking could decrease the number of psychosomatic symptoms among nonparents while increasing such symptoms among parents for both women and men. This pattern supported the expectation that teleworking at home could become a stress factor for workers who take care of children and work at the same time. However, as all effect estimates in Figure 5 were substantively small and statistically insignificant, our findings did not indicate any significant group heterogeneity by individual parenthood status.
Discussion
In this study, we investigated the effects of access to telework and home-office work on an individual’s general health, sleep quality, and number of psychosomatic symptoms. Using data from the German panel of the BAuA Working Time Survey from 2015, 2017, and 2019, we estimated POLS, FE, and FEIS models to disentangle different selection effects: selection into both telework and different health outcomes, selection into telework on the basis of the level of pretreatment health, and selection into telework on the basis of the pretreatment individual trajectory of health.
According to the descriptive results, male and female teleworkers reported significantly better general health, better sleep quality, and fewer psychosomatic symptoms compared with their nonteleworking counterparts. However, there were also remarkable differences in people’s access to telework across individual, familial, and occupational characteristics, indicating that the associations between teleworking and health outcomes could be driven by selection.
To tackle the different sources of selection, we first performed the POLS model in which observed common factors of teleworking and health and well-being were controlled for (i.e., age and period, educational level, vocational training, the presence of a partner and children in the household, working hours, firm size, and occupations). According to this analysis, teleworking seemed to have positive influences on workers’ health and well-being, causing better health evaluation and sleep quality, while reducing psychosomatic symptoms.
Going beyond the POLS models, we performed FE models to further control for unobserved time-constant heterogeneities and to account for selection into telework on the pretreatment level of health. In general, we found small and statistically insignificant effects of telework on health and well-being across all scenarios. However, one nuance is worth discussing. In contrast to the POLS models’ findings that men’s sleep quality and psychosomatic wellness benefited from teleworking, the results of the FE models showed no effect. Such contrast indicated a positive selection of pretreatment health levels into telework: men who had better sleep quality and fewer psychosomatic symptoms were more likely to access telework. This finding supported the “healthy teleworker hypothesis.”
On the basis of these findings, we further examined whether there was also a selection on pretreatment health trajectories into teleworking by comparing the results of FEIS models with those of the benchmark FE models. We found some evidence of a positive selection into telework on the basis of better pretreatment health. Particularly for the models of psychosomatic symptoms, after accounting for this source of selection, we found that access to telework could significantly increase psychosomatic symptoms for women.
Concerning the effect heterogeneity by intensity of telework, we found that more days of telework seemed to benefit men’s health but harm women’s. In particular, women who teleworked more than three days per week could experience worse health and more psychosomatic symptoms. This finding has crucial implications for tackling gender inequality in the labor market, especially when telework has become widely spread in recent years (Aksoy et al. 2023). Researchers and policy makers alike should keep monitoring the potential downside of telework and provide policy measures to protect certain demographic groups, such as women, from being jeopardized by the rise of the new working arrangement.
Finally, we did not find robust evidence regarding the heterogeneous effects of telework on health across parenthood status groups. However, our analysis on psychosomatic symptoms did show that nonparents were more likely to experience fewer symptoms, whereas parents’ psychosomatic symptoms tended to increase by teleworking.
In summary, our additional findings on the effect heterogeneities showed that the influences of telework on health and well-being could differ according to gender and family structures. In particular, the health situations of women and families with children could be at risk by having a high-intensity telework arrangement. Such a finding echoes a recent review article on this issue (Furuya et al. 2022), which reported worsening mental health outcomes of teleworkers among women and mothers in several studies.
To briefly conclude, our study casts doubt on the proposed health-promoting effects of teleworking. No concrete evidence for the positive, causal effects of telework on health and well-being was found in pre-pendemic Germany. Instead, we found that an intense teleworking schedule (i.e., more than three days per week) might hamper women’s health. To explain why the observed positive associations between teleworking and health were potentially spurious, we highlighted the crucial role of selection mechanisms through different channels. We found that teleworking women and men were a highly selective group in terms of individual, family, occupational, and company-specific characteristics. Moreover, positive selection on both prior levels and prior trajectories of health were found to partially shape the ostensibly better health outcomes among teleworkers. However, to what extent this selection was based on self-selection or external selection by the employer could not be assessed in the present study and remained an open question.
Moreover, our results indicated that the effect of telework on health was affected by the choice of health measures. We observed the strongest effects of telework on psychosomatic symptoms. On one hand, this generic health measure may be less subjective compared with the self-evaluated categories of general health and sleep quality. On the other hand, our index of psychosomatic symptoms summarizes various symptoms of body and mind that are often caused by medium to high levels of stress, anxiety, or depression (Wöhrmann et al. 2021). Thus, the index of psychosomatic symptoms focuses on other aspects of health compared with subjective health and sleep quality. Although subjective general health measures may also include both physiological and psychological symptoms, the individual weighting of health complaints may differ. Thus, as telework affects various dimensions of health differently, it is important for further studies to take different health measures into consideration.
Another limitation of the present study concerns the central dependent variable in which telework and home-office work are mixed according to the German legal definition of telework. As telework can be performed from home as well as any other location, two spatially flexible forms of work are mixed here. Whether the respondents were aware of the legal definition cannot be assessed at this point. However, a more specific query of telework and home-office work as two different flexible forms of work would be desirable.
Moreover, we should cautiously validate the “healthy teleworker hypothesis” in other legal contexts. The hypothesis was derived in Germany, where the right to telework was negotiated in company agreements rather than being regulated by law. However, the underlying selection mechanisms might differ in countries where telework is legally regulated at the national level, such as in Belgium and France, or where workers who have health issues or care-related demands are granted more opportunities for telework, such as in Portugal (Eurofound 2022).
Finally, our analyses were restricted to the time before the coronavirus disease 2019 pandemic. Shortly after the outbreak of the pandemic, in Germany as in many other countries around the world, the workforce was sent to the home office wherever possible. Since then, the restrictions have been lifted and many people have returned to in-office work, at least partially. Estimating the causal effect of telecommuting on health during the lockdowns and thereafter would require a more sophisticated methodological approach in which this external shock is explicitly modeled. With the future publication of further waves of the BAuA Working Time Survey, it will be possible to address these questions.
Related to the last two points, we want to discuss an unresolved puzzle in telework research: why does the demand for telework remain strong in the postpandemic era (Aksoy et al. 2023; Barrero, Bloom, and Davis 2023), despite its rather ambiguous and sometimes negative impacts on workers’ health according to our findings and previous research conducted before the pandemic (Furuya et al. 2022)? Although we have no direct answer to this question, we suspect that the composition of teleworkers has fundamentally changed since the pandemic. Before the pandemic, at least in Germany, the right to telework was more likely to be granted for those who had better work performance. Among this selective group, the urgent need for telework to address work-family conflicts or serious commuting issues might be proportionally smaller. During the pandemic, however, those who demanded for telework but were otherwise not allowed to suddenly had the chance to telework. This compositional change of the target population could markedly shift the average evaluation to telework in the short run. Nevertheless, we should not overlook the long-term influences of telework on people’s life outcomes. Instead, with telework becoming more and more popular and corresponding changes in labor market practices, we call for more sophisticated data collection (especially via panel surveys) and better attention to the health and well-being consequences of telework throughout the life course.
Footnotes
Appendix
Results from Fixed-Effects Models: Effect of Telework on General Health, Sleep Quality, and Psychosomatic Symptoms by Presence of Children in the Household.

| General Health, b (SE) | Sleep Quality, b (SE) | Psychosomatic Symptoms, b (SE) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No Children | Children | No Children | Children | |||||||||
| Women | Men | Women | Men | Women | Men | Women | Men | Women | Men | Women | Men | |
| Telework | .036 (.074) | .071 (.067) | −.005 (.073) | .035 (.058) | −.135 (.093) | .000 (.078) | −.096 (.097) | .019 (.072) | −.117 (.164) | −.051 (.132) | .131 (.160) | .186 (.125) |
| Year (reference = 2015) | ||||||||||||
| 2017 | .115*** (.028) | .034 (.028) | .120*** (.035) | .096** (.030) | .108** (.036) | .001 (.033) | .093* (.046) | .099** (.037) | −.110 (.062) | −.042 (.056) | −.148 (.076) | −.121 (.064) |
| 2019 | .084** (.032) | .014 (.032) | .109** (.040) | .112** (.035) | .102* (.040) | −.064 (.038) | .083 (.053) | .136** (.043) | .004 (.071) | .006 (.064) | −.050 (.088) | −.212** (.074) |
| Education (reference = high) | ||||||||||||
| Low | .223 (.376) | .047 (.254) | .198 (.378) | .034 (.320) | −.287 (.471) | .248 (.296) | −.148 (.498) | .373 (.398) | .409 (.825) | .800 (.508) | 1.432 (.825) | −.634 (.687) |
| Medium | .022 (.306) | .148 (.252) | .068 (.370) | .102 (.262) | .162 (.384) | .399 (.294) | .246 (.487) | −.328 (.327) | .198 (.673) | .269 (.501) | −.969 (.807) | −.210 (.570) |
| Vocational training (reference = high) | ||||||||||||
| None | −.334 (.221) | .266 (.243) | .116 (.253) | .050 (.204) | −.441 (.277) | −.338 (.284) | .053 (.333) | .298 (.254) | −.455 (.485) | −.462 (.481) | .539 (.552) | −.041 (.438) |
| Low | .362 (.283) | .245 (.264) | .210 (.282) | −.313 (.202) | −.537 (.354) | −.125 (.308) | .305 (.371) | −.011 (.251) | −1.014 (.621) | −.572 (.523) | −.060 (.614) | .002 (.432) |
| Medium | .326 (.314) | .450 (.272) | −.038 (.340) | −.063 (.266) | −.109 (.393) | .101 (.317) | .236 (.447) | .041 (.332) | 1.056 (.689) | .029 (.538) | .777 (.741) | .445 (.570) |
| Partner in household | .044 (.135) | .085 (.130) | −.180 (.114) | .186 (.194) | −.023 (.169) | .380* (.152) | .105 (.151) | .436 (.242) | −.046 (.296) | −.272 (.257) | −.095 (.249) | .050 (.416) |
| Actual working hours | −.007* (.003) | −.002 (.003) | −.003 (.004) | −.004 (.004) | .001 (.004) | −.007* (.003) | −.005 (.005) | .004 (.005) | .025*** (.007) | .025*** (.006) | .016* (.008) | .013 (.008) |
| Firm size (reference = 1–49) | ||||||||||||
| 50–499 | .016 (.062) | −.045 (.066) | −.102 (.075) | −.058 (.070) | −.154* (.078) | −.063 (.077) | −.184 (.098) | .226** (.087) | .010 (.137) | .071 (.130) | −.173 (.164) | −.123 (.149) |
| ≥500 | −.005 (.078) | −.040 (.075) | −.052 (.089) | −.116 (.079) | −.273** (.098) | .021 (.087) | −.047 (.118) | .103 (.098) | −.039 (.173) | −.074 (.148) | −.217 (.195) | −.030 (.169) |
| Occupation (reference = manager) | ||||||||||||
| Professionals | .420 (.244) | −.239 (.179) | −.064 (.226) | −.055 (.165) | −.065 (.306) | −.463* (.209) | −.261 (.298) | .020 (.205) | −.187 (.537) | .112 (.361) | .027 (.493) | −.342 (.354) |
| Technicians | .456 (.238) | −.107 (.193) | .127 (.264) | .160 (.188) | .036 (.298) | .028 (.225) | −.266 (.347) | −.186 (.234) | .449 (.523) | −.509 (.383) | −.013 (.575) | −.320 (.403) |
| Clerical support | .283 (.253) | .101 (.264) | −.006 (.281) | .270 (.243) | .165 (.318) | .101 (.308) | .227 (.370) | .138 (.303) | .400 (.557) | −.239 (.523) | −.224 (.612) | −.919 (.521) |
| Service and sales | .394 (.299) | .013 (.269) | −.047 (.345) | −.244 (.283) | .044 (.375) | −.038 (.314) | −.519 (.462) | −.580 (.353) | −.398 (.656) | −.025 (.534) | 1.023 (.753) | −.217 (.606) |
| Agricultural | −.729 (1.051) | .071 (.427) | −.632 (.766) | .162 (.973) | −.895 (1.317) | .305 (.499) | −1.959 (1.011) | −.495 (1.212) | 4.113 (2.309) | −.835 (.847) | 1.451 (1.670) | −.386 (2.081) |
| Craft and trades | .317 (.431) | .121 (.254) | −.411 (.615) | .039 (.252) | −.043 (.540) | .256 (.297) | −.483 (.810) | −.622* (.314) | 1.010 (.946) | −.805 (.504) | .205 (1.342) | −.141 (.540) |
| Operators, assemblers | .230 (.405) | −.392 (.311) | −.162 (.575) | .249 (.315) | .204 (.507) | .304 (.362) | −.153 (.757) | .011 (.392) | .627 (.889) | .391 (.615) | .618 (1.254) | −.513 (.679) |
| Elementary occupations | .178 (.394) | .433 (.355) | −.193 (.419) | −.278 (.588) | .121 (.494) | .222 (.414) | −.106 (.551) | −.199 (.733) | −.095 (.867) | .028 (.702) | .527 (.913) | .639 (1.258) |
| Constant | 3.500*** (.362) | 3.527*** (.320) | 3.930*** (.361) | 3.925*** (.359) | 3.813*** (.453) | 3.645*** (.373) | 3.588*** (.475) | 2.901*** (.447) | 1.933* (.795) | 1.718** (.634) | 2.306** (.787) | 2.121** (.768) |
| Observations | 7,653 | 7,580 | 5,013 | 5,869 | 7,652 | 7,577 | 5,010 | 5,866 | 7,609 | 7,557 | 4,990 | 5,850 |
| Cohen’s d of telework | .037 | .075 | −.005 | .039 | −.117 | .000 | −.083 | .017 | −.050 | −.023 | .055 | .085 |
p < .05. **p < 0.01. ***p < .001.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded by the State Institute for Family Research at the University of Bamberg.