
Abstract
Extensive sociological research concludes that education informs people’s desires for their lives and plays an instrumental role in facilitating the fulfillment of those desires. In this article, we ask if societal barriers can leave the most educated to desire outcomes that are unattainable and thus paradoxically place them at highest risk of unwanted outcomes. We answer this question by analyzing societal variation in the potential for education to facilitate women achieving their lower fertility desires: Are there fertility contexts wherein educated women’s lower fertility desires are distinctly unattainable? Multilevel models analyzing Demographic and Health Survey Program data on women from 50 low- and middle-income countries emphasize the collision of global scripts with local constraints: In low contraceptive contexts, education is associated with higher risk of unintended pregnancy. The results clarify that the potential for education to facilitate the achievement of desires is fraught with contingencies.
Keywords
Extensive sociological research suggests that education facilitates individuals’ achievement of desires over the life course. Across diverse global contexts, the most educated in a society tend to be the best resourced, healthiest, and happiest, and they enjoy the means to ensure the same for their children (Bonini 2008; Ross and Wu 1995; Tamborini, Kim, and Sakamoto 2015). By positioning individuals favorably in the social strata, education not only shapes people’s desires for their futures but also facilitates the achievement of these desires (Meier and Bell 1959).
In recent decades, sociologists of stratification have identified heterogeneity in the benefits of education, demonstrating that its effectiveness at guaranteeing desired outcomes varies across social groups (Brand and Xie 2010). Sociology’s foundational interest in how social structure shapes individual action (Coleman 1986; Collins 1981) and recognition that macro-structural elements can influence the intersection of education and stratification (Buchmann and Hannum 2001) suggest social structures that constrain individual behavior may mute or even reverse the influence of education on the achievement of desired outcomes. Against the backdrop of sociology’s long-standing recognition that some social structures facilitate individuals’ fulfilment of their desires as others impede their realization (Meier and Bell 1959), in this study, we ask if societal conditions alter the micro-level link between education and achievement of desires.
The swift expansion of education across the world in the past century makes answering this question of high sociological relevance. Although educational inequalities persist, youth across the globe are achieving increasingly high levels of education amid disparate social, cultural, and economic conditions. In many societies, even as youth are progressing to secondary and postsecondary school and are forming aspirational desires for their futures along the way (Frye 2012), they lack the social structures necessary to realize these desires (Kabiru et al. 2013; Smith-Greenaway and Yeatman 2020). As such, highly educated individuals may have a clear vision of what they want and the language to describe it but lack the societal conditions necessary to attain it. This raises questions of whether—contrary to the prevailing notion that education universally facilitates individual achievement by fusing a tight linkage between desired and actual outcomes—education may be a risk factor for experiencing undesired life course experiences in certain contexts. Despite the universality by which education encourages individuals to adopt specific life course desires, is the ability to fulfill these desires conditional on people’s social environment? Can societal conditions subvert the widely established micro-level link between education and achievement, leading the most educated to, at times, be at the highest risk of undesired outcomes?
In this study, we analyze a set of desires that are widely studied in the sociological and demographic literatures: fertility desires. A discrepancy between women’s fertility desire and outcome in the form of an unintended pregnancy is a common and consequential phenomenon (Bearak et al. 2018; Gipson, Koenig, and Hindin 2008), providing a propitious opportunity to study how societal conditions alter the relationship between education and achievement in a way that is meaningful to women’s lives. Using nationally representative data from 50 low- and middle-income countries and multilevel models, we examine whether contextual realities influence the relationship between education and unintended pregnancy.
Across diverse fertility contexts, more highly educated women have lower fertility desires: They want to delay their entry into motherhood and ultimately to have fewer children relative to women with less education (Bongaarts 2003). Research further shows that, as demonstrated in the contemporary U.S. (Hayford and Guzzo 2016; Musick et al. 2009), it is often true that being more highly educated best positions women to achieve these lower fertility desires (Bongaarts 1997, 2003; Lutz 2017), corresponding with their lower odds of unintended fertility. That is, more highly educated women are generally less likely to have a child from an unintended pregnancy relative to their less educated peers thanks mostly to their higher contraceptive use (Bongaarts 2003). 1 Yet across the globe, many highly educated women are navigating their reproductive years in societies where fertility decline is slow, or even “stalled,” due in part to infrastructural, social, and cultural barriers to contraceptive use (Alkema et al. 2013; Moreira et al. 2019). Thus, even if highly educated women ascribe to global scripts of the desirability of fewer children, the reflexivity between aggregate social structures and individual action is such that their lower fertility desires may be distinctly unattainable. This reality may result in situations wherein more highly educated women are more likely to experience an unintended pregnancy relative to their less educated peers because they have lower fertility desires yet lack the means to effectively achieve them.
Compared with sociological research on desires, expectations, and aspirations that has, among other things, emphasized how they can themselves be signals of social position (Johnson and Hitlin 2017), salient to individual well-being (Frye 2012; Hitlin and Kirkpatrick Johnson 2015) and group identity (Mische 2009; Tavory and Eliasoph 2013), other research attends to the mismatch between individuals’ desires and outcomes and the experience of having a set of desires go unfulfilled (Kabiru et al. 2013; Reynolds and Baird 2010; Smith-Greenaway and Yeatman 2020). An unintended pregnancy is an especially consequential example of an undesired life course outcome that has been studied intently by sociologists and demographers (Bachrach and Morgan 2013; Barber et al. 2013; Bearak et al. 2023; Bongaarts and Casterline 2018; Hayford and Guzzo 2016; Morgan and Bachrach 2011). Having an unintended birth can lead to declines in women’s health in low-income countries (Yeatman and Smith-Greenaway 2021)—regardless of women’s economic and social circumstances—emphasizing the need to understand the intersection of social forces that place women at risk of experiencing a pregnancy that they do not desire.
Education, Aspirations, and Achievement of Desires
Education is a major force of social stratification across the globe (Buchmann and Hannum 2001). Education shapes individuals’ ideas about what constitutes “the good life” (Lerner 1957), powerfully informing their narrative of the life they want to achieve. By encouraging people to adopt a vision of their life around key experiences, statuses, and achievements, education fundamentally informs the future that individuals imagine for themselves and their children—supplying them with a clear framework of what is desirable. This is especially true in contexts where the expansion of formal education is recent and what constitutes “the good life” is being redefined (Scott, Hinrichs, and Jensen 2018). In such contexts, school instills ideas about ways to structure one’s life and acts as a site in which the global export of ideas occurs; as Mojola (2015:221) states, schools act as “arbiter(s) of globalized cultural scripts and sub-scripts.” Supporting this supposition is a vast literature emphasizing the linkage between women’s education and the adoption of global cultural scripts (Hornik and McAnany 2001; Meyer, Ramirez, and Soysal 1992; Pierotti 2013; Thornton 2013).
Education not only informs what people want in life, but it also influences their position in the social strata, enabling them to get what they want (Meier and Bell 1959). By helping individuals obtain social status and gain relative control over resources, education facilitates the development of valuable human capital, enhancing individuals’ ability to gather information and solve problems (Becker 2009). This human capital is rewarded in the labor market: People with higher education are more likely to be employed, have full-time positions, and enjoy higher and more stable incomes. By improving individuals’ socioeconomic conditions, education generally smooths their life paths, helping people by both reducing their exposure to adversity and increasing their access to resources that allow them to cope with adversity if it does surface (Mirowsky and Ross 2007; Pearlin 1989; Ross and Wu 1995; Turner and Noh 1983; Wheaton 1980). All in all, the extant literature emphasizes that education helps fuse a tight link between what people desire and what they achieve (Mirowsky and Ross 2007).
The faciliatory role of education for achievement at the individual level is complemented by societal-level advantages of the expansion of education (Hanushek and Woessmann 2010). The expansion of education has been linked to a host of major social changes, including economic growth, infrastructural improvement, demographic transition, democratization, and advanced gender equality (Baker et al. 2011; Caldwell, Reddy, and Caldwell 1988; Notestein 1945; Thornton and Lin 1994). The promise of educational expansion as an effective way to transform society has led to investment in it becoming an uncontested development strategy across low- and middle-income countries (Psacharopoulos and Woodhall 1993). Investment in educational access, particularly for girls, has become a de facto strategy for enabling individuals to improve their lives and their country’s economic and political standing.
Yet the expansion of education does not immediately or always produce widespread societal change. Instead, youth across low- and middle-income countries are increasingly achieving high levels of education in contexts where the societal-level conditions, from political-economic factors to social and cultural ones, necessary for achieving the desires that they formed in school are conspicuously absent (Kabiru et al. 2013). Grounded in recognition that macro-level realities can constrain individual-level opportunities and behaviors (Alexander 1988; Coleman 1986; Durkheim 2014), this raises questions of the universality by which education facilitates the achievement of desired outcomes.
Indeed, even as the individual- and societal-level benefits of education have been established across the globe, a handful of case studies show cracks in the universality of the relationship. These cases demonstrate the challenges of being highly educated in contexts where educational progress has eclipsed other political, economic, social, and cultural changes. For example, studies have highlighted how a society’s gender system (Berry 2015; Frye and Urbina 2020), political-economic conditions (Filmer and Fox 2014; Noland and Pack 2007), and health environment (Baker et al. 2017; Chang and Lauderdale 2009; Cheng et al. 2015; Fortson 2008) can suppress the benefits of education.
Thus, even as expanded education is anticipated to eventually have a transformative influence on society as a collective, individuals who achieve high levels of education in contexts that have not undergone such sweeping transformations may find themselves in hopeful anticipation, suspended in a state of “cruel optimism” (Berlant 2011). In other words, education may encourage individuals to maintain desires that exceed the constraints that define their social position, leaving the most educated paradoxically at higher risk of unfulfilled desires. This could pertain to a wide spectrum of desires. For instance, to the extent that education encourages individuals to maintain a set of ideas about economic success and consumption (Mojola 2014) to those pertaining to romantic relationships (Pierotti 2013), those residing in settings where such possibilities juxtapose local structural, cultural, or social constraints will be at the highest risk of unfulfilled desires.
This contradictory evidence is rarely reconciled or integrated into the much larger literature that emphasizes the salutary effects of education on achievement; our study seeks to remedy this disjuncture by assessing the potential for educational gradients to differ across contexts in relation to modifiable social structures. That is, a large literature on the socioeconomic and psychological benefits of education establishes that education informs individuals’ desires and provides them with the resources to achieve their desired life outcomes. Yet another literature shows select cases wherein societal conditions can disrupt the link between desires and desired outcomes, including for socially advantaged groups. We integrate these two areas of research to assess if the link between education and desires is impervious to social structure or if the potential for desires to be achieved is contingent on them. Specifically, we examine whether in certain contexts, education can leave women at risk of unintended pregnancy.
The Case of Education and Unintended Pregnancy
Education is a major determinant of women’s fertility behaviors, from the timing of their first child to the total number of children they eventually have (Axinn and Barber 2001; Blossfeld and Huinink 1991; Brewster and Rindfuss 2000). This is true in diverse societies across the globe that are at varying stages of fertility decline—emphasizing the persistence of the education-fertility link even as the strength of it varies (Bongaarts 2003; Jejeebhoy 1995; Rutstein and Calverton ORC Macro 2002).
Social science research is replete with explanations for why this is the case. A commonly invoked one is that the “opportunity cost” of childbearing is higher for more educated women (Becker and Becker 2009). Another explanation is the quality-quantity trade-off: Desired family size tends to be smaller for better educated women because they seek to maximize inputs, like nutrition and education, for each child (Becker 1991). Still another is that more highly educated women place less value on children than do women who have less education and fewer sources of purpose and meaning (Edin and Kefalas 2011; Smith-Greenaway and Yeatman 2020).
Additional explanations for the negative education-fertility association observed across low- and middle-income countries emphasize education as a global institution that acts as a homogenizing cultural force (Meyer et al. 1992), diffusing global models of behavior, including fertility desires and behaviors (Thornton 2013). Still other work emphasizes the maternal risk that childbearing represents in low- and middle-income contexts: in the absence of well-equipped health care services, childbearing poses serious risk to women’s health; highly educated women are aware of this and manage these risks by limiting the number of pregnancies (Lutz 2017). Bongaarts (2003:326) notes that “the higher the level of schooling, the later the age at marriage and the more preferences are implemented by means of contraceptive use” yet that “there is no agreement on the socioeconomic factors responsible for the inverse relationship between education and fertility.”
The unifying element of these otherwise diverse explanations for educational differentials in fertility is that they all stem from women’s desires and volition—reflecting intentional action. Although social scientists typically infer this intentionality rather than model it explicitly (Johnson-Hanks 2007), aligned with the general idea that education fosters a specific set of desires and places individuals in a better social position to organize their lives accordingly, more highly educated women’s lower fertility is attributable to both their intention to have fewer births and their greater success in achieving these intentions. For instance, Bongaarts (1997:272) aptly states: The higher their education level, the more likely women are to be knowledgeable about contraceptive methods, to be independent decision-makers regarding reproduction and other aspects of their lives, and to be innovators of new behaviors such as the adoption of birth control. Therefore, preference implementation would be expected to be positively correlated with level of education.
Consistent with this idea, research in the contemporary United States and Europe has demonstrated that almost all of the educational gradient in fertility is explained by more highly educated women having fewer unintended pregnancies relative to their less educated peers (Ciganda, Lorenti, and Dommermuth 2021; Finer and Henshaw 2006; Musick et al. 2009; Sobotka et al. 2015).
In countries that have recently undergone or are still undergoing fertility decline during demographic transition, like many across the global south, education is hypothesized similarly to empower women to achieve lower fertility aligned with their lower fertility desires (Lutz 2017). Bongaarts (2003) demonstrates that across several societies undergoing fertility transition, women with secondary education have lower unwanted fertility than women with less education. However, his research showcases select exceptions to this rule where unwanted fertility among women with primary education, specifically, is higher than among women with no formal education. Most clearly demonstrated in the case of Vietnam before the turn of the twenty-first century, Bongaarts (2003:332) concludes that “the reason for this is not clear”—raising questions of whether this is a one-off finding or more broadly observable.
Of particular interest is the role that the contraceptive context may have in patterning these linkages given the significance of contraception as a means by which education is hypothesized to enable women to achieve their lower fertility desires (Bongaarts 1997, 2003). Thus, even though education generally corresponds with lower unintended fertility risk, especially where there is widespread adoption of fertility-limiting behaviors, like modern contraceptive use, these gradients could be inverted for cohorts of women navigating their childbearing years in less supportive contraceptive contexts. Specifically, living in a context wherein fertility-limiting strategies are uncommon could interfere with educated women’s desire to avoid pregnancy due to their lacking the material and social means to bring their vision to fruition. This could put them at the highest risk of unintended pregnancy.
In addition to issues of material and social barriers to using contraceptives in their community, more highly educated women living in high fertility, low contracepting contexts may also face a web of more intimate obstacles in the context of their romantic relationship—they may lack the social and partner support to avoid pregnancy. In higher fertility contexts where few women are actively avoiding pregnancy with effective contraceptives, more educated women may face “backlash” from their romantic partners for having achieved higher levels of education (Behrman 2019; Urbina 2022) and could be penalized for maintaining desires that are not compatible with pronatalist norms. This could manifest in coercive behaviors and gendered power inequalities that ultimately lead more educated women to be at higher risk of unintended pregnancy. That is, to the extent that a woman having achieved more education challenges men’s status, either in the context of their romantic relationship or broader community, these women may gain minimal autonomy (Koenig et al. 2003) and may even experience more intimate partner violence (Behrman 2019), the latter of which is known to be a major determinant of pregnancy (Barber et al. 2018).
Alternatively, other literatures suggest that autonomous processes could also lead more highly educated women to experience a higher risk of unintended pregnancy in high fertility contexts. Highly educated women residing in such societies are likely confronted with pronatal cultural schemas circulating freely in their community and perhaps even in their own household and romantic relationship—schemas that are likely incompatible with their personal fertility desires. Competing cultural models are known to weaken the link between what people say they want and how they behave (Harding 2007); as such, in higher fertility societies where relatively few women use contraceptives, more highly educated women may face a dilemma over the competing ideals surrounding what it means to be a successful, educated woman. This tension between the cultural models to which women are exposed in their “educated” network and those they are exposed to in their local community could result in women behaving in ways that directly conflict with their personal desire to postpone pregnancy, ultimately corresponding with their having higher risk of unintended pregnancy. Indeed, in line with the rich sociological literature on ‘doing gender’ (Legerski and Cornwall 2010), women may engage in some sort of performative, intentional pronatal behaviors that ultimately put them at higher risk of pregnancy as they work to compensate for their ‘deviant’ standing as an educated woman. Such behaviors could ultimately put a woman at risk of pregnancy despite her having no immediate desire for one.
Regardless of whether residing in a higher fertility society poses barriers to highly educated women achieving their fertility desires or increases their risk of unintended pregnancy by exposing them to competing schemas—a theoretical distinction we cannot untangle here—these possibilities together suggest that in societal contexts where fertility-limiting behaviors are not widespread, education will correspond with women’s higher odds of unintended pregnancy. Alternatively, in lower fertility settings, where fertility-limiting behaviors are widespread, we anticipate that, aligned with evidence based on contemporary data from the United States and Europe, educated women will have lower risk of unintended pregnancy. That is, in in these settings, more highly educated women will be best positioned to make use of available material and social resources to ensure their fertility outcomes align with their lower fertility desires and may be most likely to enjoy the support of their romantic partners in avoiding pregnancy as desired. Similarly, more highly educated women in societies where more women contracept are less likely to be confronted with competing models of the life course and thus less likely to face the corresponding conflict between their desires and behaviors.
To test these possibilities, we take a cross-contextual approach that makes use of variation in contraceptive contexts across 50 low- and middle-income countries by pooling synchronized Demographic and Health Survey (DHS) Program data collected since 2010. This affords us the opportunity to examine if there is systematic, cross-contextual variation in the association between women’s education and unintended pregnancy. Research from the United States suggests that unintended births, not necessarily pregnancies, carry health risks (Foster 2021); however, in contexts of high maternal morbidity and mortality and restricted abortion access, like many of the ones we study here, unintended pregnancy is itself a health risk, mandating a clear understanding of its social patterning.
Analytic Approach
Data and Sample
The DHS Program is a standard data source for studying women’s fertility outcomes worldwide. Since the mid-1980s, the DHS Program has collected standardized surveys across low- and middle-income countries, allowing researchers to analyze the public use data in a comparative framework. The DHS uses a stratified random sampling approach with clusters providing the primary sampling unit. The sampling frame consists of enumeration areas, often derived from census data. The DHS Program then designates enumeration areas as urban or rural, defining the sampling strata. The first stage of sampling from each country’s enumeration area is selected with a probability of selection according to the size of the population. At the second stage, the DHS Program selects households systematically from urban and rural areas. The DHS Program then invites all women of reproductive age (between 15 and 49 years) to complete an interview. Comprehensive information about the implementation of each country survey is in the final country reports (available at https://dhsprogram.com/).
Our cross-contextual analysis uses the most recent round of DHS Program survey data from each country collected since 2010. See Appendix Table A1 for a list of the 50 countries included across Africa, Asia, and Latin America. Because of the tremendous variation in fertility within and between countries, our contextual unit of focus is the subnational region level. 2 Subnational regions can represent political districts or administrative units; however, in all contexts, they reflect socially meaningful geographic boundaries. In total, there are 596 subnational contexts across 50 low- and middle-income countries. Our analysis directly measures variation in the contraceptive contexts in the subnational regions to examine if this statistically moderates the size and direction of the association between education and unintended pregnancy. Note that although some women may continue to be enrolled in school at the time of the survey, given that we are modeling unintended (and intended) pregnancy at the time of the survey, this allows us to understand how women’s educational attainment to date corresponds with their pregnancy outcomes. 3 We exclude the ≈1 percent of women who are missing data on key variables, resulting in a total sample of 1,486,365 women in 596 subnational regions in 50 countries. 4
Measures
Unintended pregnancy
Even as unintended pregnancies are singular events, they represent ‘vital conjunctures’ (Johnson-Hanks 2002a)—pivotal life events that upend one’s anticipated future—and are known to set off a cascade of disadvantages for women, from declining health (Yeatman and Smith-Greenaway 2021) to additional unintended pregnancies (Guzzo and Hayford 2011).
Research on unintended pregnancy often relies on women’s retrospective reports of their most recent pregnancy after they have already given birth and parented a child. Researchers have long expressed skepticism about the quality of retrospective reports (Ryder 1973; Trussell, Vaughan, and Stanford 1999; Westoff and Bankole 1996), with indications of bias due to social desirability, recall error, and ex post rationalization (Joyce, Kaestner, and Korenman 2000; Sennott et al. 2016). Thus, rather than rely on women’s postnatal reports, we instead use data on the subsample of women who are pregnant at the time of the DHS survey and reported on the desirability of their current pregnancy. Although this measurement strategy is not prospective to the conception, it nonetheless represents an improvement to the typical retrospective report, given it is prospective to the birth.
If a woman is currently pregnant at the time of her interview, the interviewer asks her if at the time she became pregnant, she wanted the pregnancy then, later, or not at all. 5 In a first set of analyses, we created a binary measure of whether a woman’s current pregnancy is unintended (wanted later or not at all = 1) versus intended (wanted then = 0). 6 Like past research, we also study another comparison group: women who remain unpregnant (Guzzo and Hayford 2011; Yeatman and Smith-Greenaway 2021). This allows us to assess educational differences not only between women who have an unintended versus intended pregnancy but also relative to women who remain not pregnant. 7
Education
The key explanatory variable is women’s years of education. Women reported the highest level of school they attended. We code women’s education in single years, ranging from 0 to 20+ years of school. Note that we code women’s years of education continuously given our multicountry study design and the ease with which years of education can be directly compared. That is, given that a specific level of education, like primary school, can differ in terms of years of school, standards, and expectations across the country contexts that we study, we instead make use of a more directly comparable, simple measure of years of schooling. 8 In supplementary analyses, we also examine whether our findings are robust to the use of a relative education measure. That is, whereas our results pertain to women’s absolute level of education in terms of total years, in supplementary results, we consider whether women are more/less educated relative to their subnational region and assess the stability of the findings to this coding of women’s education (see the “Robustness Checks” section).
Subnational region-level contraceptive use
The key subnational-level variable of interest in our cross-contextual analysis is the prevalence of women currently using modern contraceptives. We calculate the prevalence of reproductive-age women who are currently using medical contraceptives and barrier methods (i.e., pill, IUD, injectable contraceptive, condoms, implant, foam or jelly, patch, permanent contraception), conventionally labeled “modern contraceptives.” This indicator affords a summative, singular measure that approximates the extent to which women in a subnational region have physical, social, and cultural access to—and are actively making use of—external, effective means to limit their fertility (Feyisetan and Casterline 2000). This is not to suggest other, “traditional” contraception methods, like periodic abstinence, are ineffective (Johnson-Hanks 2002b) or that we know why, specifically, women are using modern contraceptives. Nonetheless, the measure offers a valuable summary indicator of the overall material, social, and cultural availability of and use of effective, external means to limit one’s fertility. We aggregate this variable to identify the subnational-level percentage of women ages 15 to 49 currently using modern contraceptives for the 596 subnational regions in our data.
Statistical Models
We estimate multilevel logistic regression models of the association between women’s education and unintended pregnancy and examine if it varies systematically across subnational regions with distinct fertility profiles, specifically, levels of modern contraceptive use. 9
These random-effects logit models address the binary dependent variable and the hierarchical nature of the data:

where p is the probability that woman i in subnational region j in country k has an unintended pregnancy; a is the intercept; X ijk is a vector of individual-level covariates; Y jk is a vector of subnational region-level covariates; C k are country dummy variables that allow us to control for unobserved confounders at the country level; u j is the subnational region-level random effect; and the βs represent the corresponding coefficients. Note that a country-level fixed-effects approach allows us to account for constant, unobserved factors that vary across countries. Because a fixed-effects approach is less efficient, our analyses will yield more conservative estimates.
Specifically, we estimate the following model:
The model includes the two key explanatory variables, the subnational region-level prevalence of contraceptive use and women’s years of education, and a cross-level interaction term between them to determine whether the association between education and unintended pregnancy is conditional on the contraceptive context for woman i in subnational region j in country k, net of country dummy variables. The model further includes individual- and subnational region-level controls to ensure any associations are not spurious. Specifically, at the individual level, the model includes women’s current number of children, current age (in years), marital status, and whether their house is in an urban (vs. rural) community. We also include controls for women’s socioeconomic status, including a preconstructed measure of their household’s wealth. A principal component factor analysis of a household’s ownership of various assets (e.g., radio, television, refrigerator, bicycle, car) and housing characteristics (e.g., availability of electricity, source of drinking water, type of toilet facility, number of rooms) is the basis for categorizing households into five wealth quintiles: poorest, poorer, middle, richer, and richest (Filmer and Pritchett 2001).
At the subnational region level, the model includes other characteristics of the local context that correlate with its fertility and contraceptive profile. To account for socioeconomic inequalities, we include an indicator of the percentage of households with electricity, the percentage of households that have either a landline or a mobile phone, the percentage of households classified as urban, and the percentage of households in the two highest wealth quintiles. We further control for women’s average years of education and the completed fertility rate (among women ages 45–49 years old). Appendix Table A2 demonstrates the distinct profiles of subnational contexts wherein contraceptive use remains rare versus those where it is widespread. Subnational settings wherein contraceptive use is widespread are also those that are more urbanized, feature better infrastructure and lower fertility, and are settings where the average woman has attended more education—emphasizing the need to account for these additional contextual differences in our models.
Again, we estimate all models with two distinct reference groups, women who are intentionally pregnant and women who remain not pregnant, and we graph the predicted probabilities using marginal effects.
Results
Table 1 contains key descriptive statistics for the two analytic samples. Beginning with the subsample of all currently pregnant women, 21.5 percent report that their pregnancy is unintended (mistimed or unwanted), whereas 78.5 percent of women are intentionally pregnant. The data show that women have, on average, between five and six years of school across the two analytic samples, and the average woman lives in a subnational region where just 24.2 percent of women are using modern contraceptives. The average respondent is approximately 26 years old. As shown in the second column of Table 1, although most women interviewed by the DHS Program are not pregnant at the time of the survey, a small percentage of women are—and are specifically unintentionally pregnant (i.e., reported that the pregnancy was either mistimed or unwanted). As shown across the two columns, the currently pregnant subsample is more likely to be in a union and to live in a rural household, as anticipated; however, the characteristics of women’s subnational regions across the two analytic samples are comparable. Among the sample including never pregnant women, women are slightly more educated, significantly less likely to be in a union, and live in wealthier households relative to the currently pregnant sample.
Descriptive Characteristics of Women in 596 Subnational Regional Contexts in 50 Low- and Middle-Income Countries.

Source: Demographic and Health Survey Program.
Figure 1 shows the tremendous variation in the prevalence of women using modern contraceptives across the 596 subnational regional contexts. Overall, contraceptive prevalence ranges from effectively 0 percent of women in a region in Chad to nearly 70 percent of women in a region in the Dominican Republic. In 35 of the 50 countries, there are subnational regions where fewer than one in five women are using modern contraceptives, and in nearly 20 countries, upward of nearly one-half of women are using them in at least some regions. For comparison, recent data show that in the contemporary United States, approximately 45 percent of reproductive-age women use modern contraceptives (Daniels and Abma 2020). Figure 1 also depicts considerable within-country variation, confirming the appropriateness of focusing on the subnational level: in many countries, the subnational regional prevalence of current contraceptive use varies from 30 to 50 percentage points.
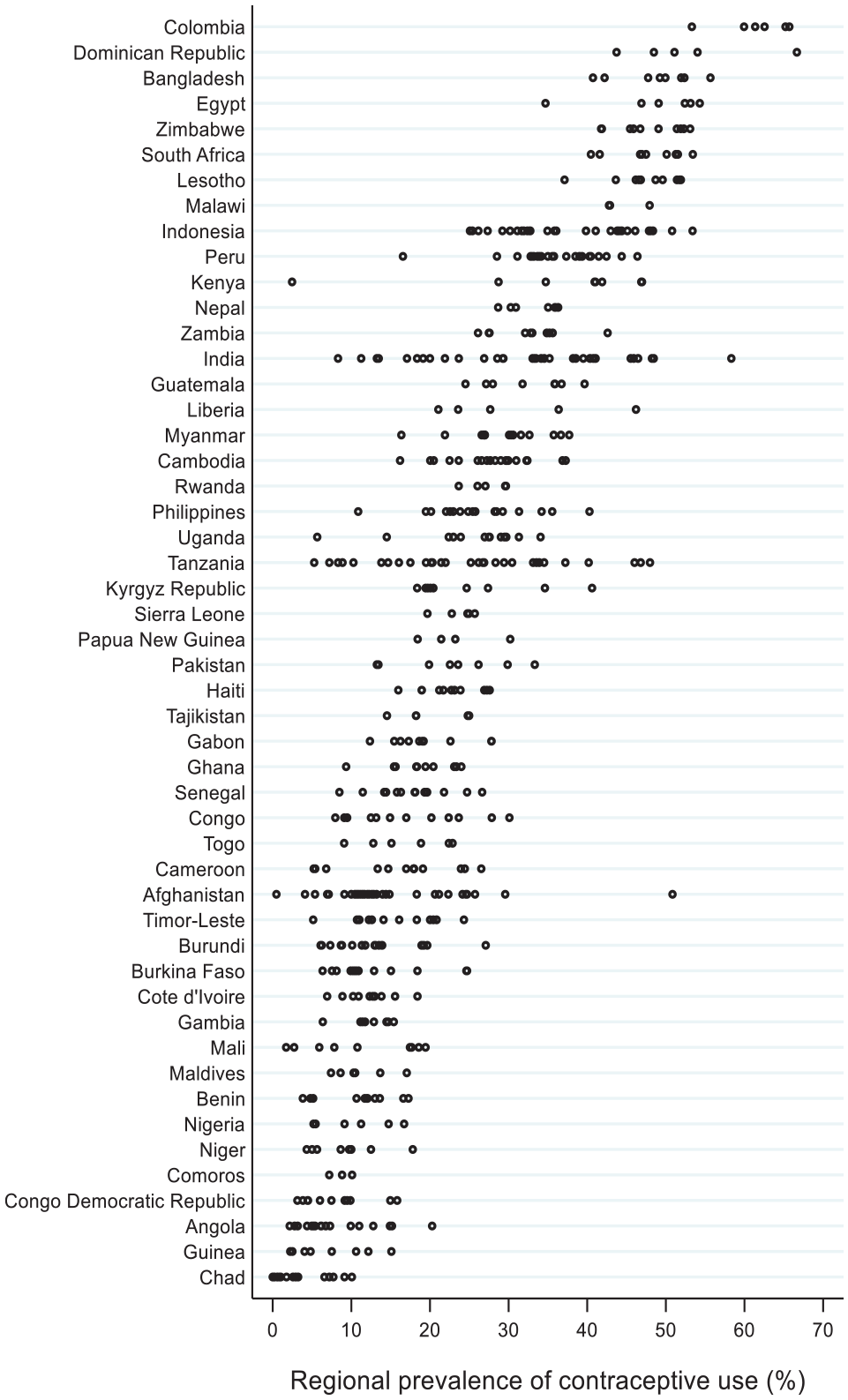
Subnational regional variation in contraceptive-use prevalence (percentage) by country.
Table 2 presents the multilevel logistic regression models. Beginning with the first two columns, we estimate the odds of unintended pregnancy versus intended pregnancy. As shown, there is a significant, negative, cross-level interaction between women’s education and the subnational regional prevalence of modern contraceptive use (OR = 0.83; p < .001). This negative interaction term suggests that the direct, positive association between education and unintended pregnancy—a finding that is itself surprising—becomes significantly smaller as the subnational prevalence of modern contraceptive use is higher. Note that this moderation is present net of individual- and subnational region-level indicators, indicating significant, systematic cross-contextual variation in the association between education and the odds of viewing one’s current pregnancy as unintended (vs. intended).
Multilevel Logistic Regression Models of Unintended Pregnancy among Women in 596 Subnational Regional Contexts in 50 Low- and Middle-Income Countries.

Source: Demographic and Health Survey Program.
p < .05. **p < .01. ***p < .001.
The second model presented in Table 2, which alters the reference group to be those that remain not pregnant at the time of the survey, shows comparable moderation. Notably, however, in this model, living where contraceptive use is higher is associated with women’s lower odds of unintended pregnancy, but the association is not statistically significant.
Because it is difficult to interpret interaction terms in the context of a logistic regression model (Ai and Norton 2003; Long and Mustillo 2021), to meaningfully interpret these results, both in terms of size and statistical significance, we plot the marginal effects for women residing in subnational regions with highly dissimilar contraceptive-use profiles. Figure 2 depicts the predicted probability of currently having an unintended pregnancy by women’s education for individuals residing where 1 in 10 or fewer women are currently using contraceptives. As shown, in these low-contraceptive regions, each year of education corresponds with a significantly higher probability of unintended pregnancy. Of note, beginning at five years of school and higher, women’s probability of currently having an unintended pregnancy at the time of the survey is significantly larger than those of their peers with no years of education. Overall, the probability of currently having an unintended pregnancy at the time of the survey nearly doubles for women in this region, from 0.16 for the least and 0.29 for the most educated women in the sample.
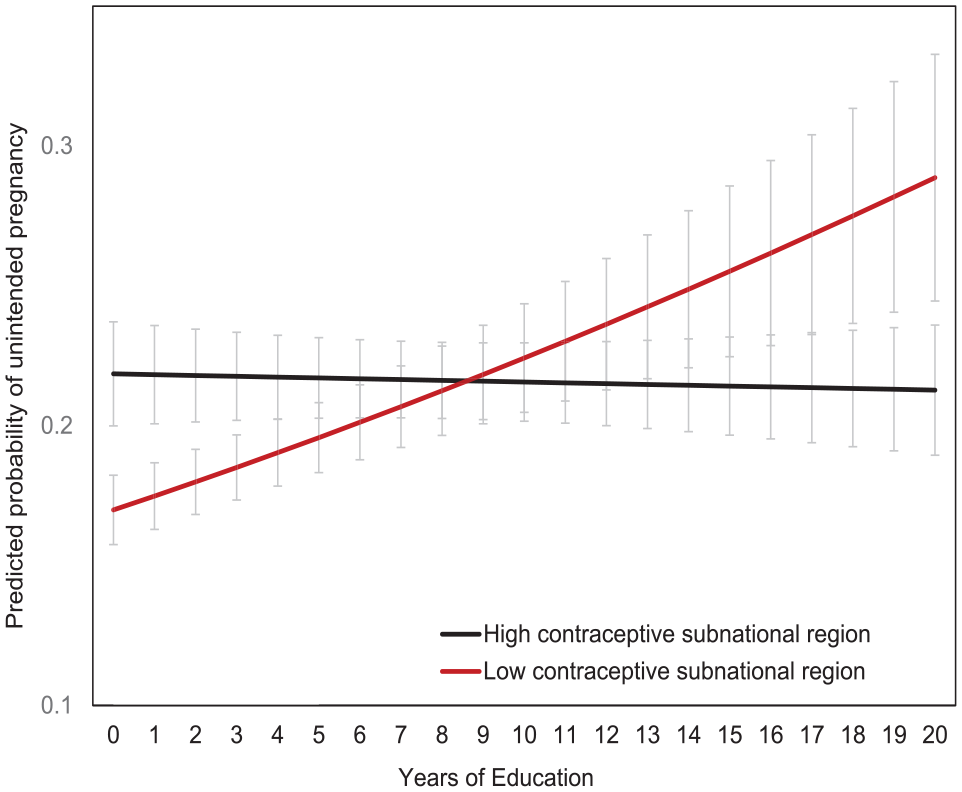
Predicted probability of unintended pregnancy versus intended pregnancy by years of education and subnational regional-level contraceptive use prevalence.
Conversely, Figure 2 further shows that for women living in settings where nearly one-half (40 percent+) of women are using contraceptives, education is not a risk factor for unintended pregnancy. Interestingly, however, it does not provide the protective influence that would be expected. That is, unlike in contemporary Western contexts, the results show that—net of other demographic, social, and economic characteristics—education has no significant protective association with women’s likelihood of unintended pregnancy—even where a higher proportion of women are contracepting. Indeed, the least educated women residing in high contraceptive contexts have slightly higher probabilities of unintended pregnancy relative to their similarly educated counterparts living in lower contraceptive settings.
Whereas Figure 2 focuses on the subsample of women who are currently pregnant, comparing the probability that the pregnancy is unintended versus intended, in Figure 3, we examine increases in the probability of unintended pregnancy versus remaining not pregnant at the time of the survey by women’s years of education. The probabilities are, as expected, significantly smaller given we are capturing women who are, by chance, pregnant at the time of the survey and not their lifetime probability of unintended pregnancy. Yet even so, as shown in Figure 3, for women living in subnational regions where fewer than 10 percent of women use modern contraceptives, each year of education corresponds with a significantly higher probability of currently having an unintended pregnancy (rather than remaining not pregnant). The significant differences emerge at a dozen years of school or more. Conversely, education comes with no elevated probability of having an unintended pregnancy in subnational regions where contraceptive coverage approaches one-half of women.

Predicted probability of unintended pregnancy versus not currently pregnant by years of education and subnational regional-level contraceptive use prevalence.
Robustness Checks
We performed several robustness checks to test the stability of the findings. First, to ensure that the aforementioned results were not influenced by the inclusion of any specific country, we reestimated all models, excluding each country in turn. As shown in Appendix Table A3, these model results demonstrate the notable robustness of the key results with the in-turn omission of each country.
Given our measurement of education in terms of women’s absolute years of education, despite our studying dramatically disparate educational contexts, we were also interested in understanding the stability of the results to the theorizing of women’s educational attainment in a more localized way. This asks a related but somewhat distinct question to our main one. That is, does having higher education relative to one’s particular context put women at higher risk of unintended pregnancy? To answer this, we created a relative education measure—attending to whether women are more educated, comparably educated, or less educated than the average woman in their subnational region. As shown in Appendix Table A4, the results are even more dramatic than those shown in Table 2, further attesting to the robustness of the results to not only the sample but also our measurement of a key construct.
We were also interested in the robustness of the findings to altering our reference group and to further sample restrictions. In terms of the former, we first assessed if the educational gradient in unintended pregnancy risk as a function of women’s contraceptive context is observed when comparing women to both their peers who remain not pregnant and those who were pregnant intentionally. As shown in Appendix Table A5 and Figure A1, the results are consistent when we combine the two reference groups to assess women’s risk of unintended pregnancy: where contraceptive use is high, we see no major influence of education on women’s likelihood of unintended pregnancy net of controls—even as these women generally experience lower probabilities of unintended pregnancy. However, in settings where contraceptive use is low, we observe a strong increase in the probability of unintended pregnancy as women attain higher levels of education. More highly educated women experience significantly higher probabilities of unintended pregnancy relative to their less educated peers in low contraceptive use settings.
Note that we were also interested in examining the results among a more homogeneous sample of women in the 50 countries that we study: women who have not had their first child and/or are currently pregnant. That is, given fertility is high in these settings, many of the women in the full sample may have very recently had a child and thus may not be “at risk” of an unintended pregnancy due to amenorrhea and/or postpartum abstinence. Furthermore, in many settings, extended breastfeeding is widely practiced, and thus many women may be experiencing lactation-induced amenorrhea. Additionally, factors such as the health and sex composition of women’s existing children may affect their fertility desires. As such, in additional models, we focus on childless women, a subsample for whom we know child compositional and/or reproductive factors are not influencing their likelihood of unintended pregnancy.
As shown in Appendix Table A6 and Figure A2, the restriction to childless women—which rids the data of the ‘noise’ introduced by both women’s prior fertility and their existing children’s characteristics—produces even more dramatic results than those shown in the main Table 2 and depicted in Figures 2 and 3. 10 Among childless women, although there is a slight positive gradient in the probability of unintended pregnancy by education in high contraceptive use contexts, the probabilities are not statistically significant at any level of education. Conversely, in the lowest contraceptive use settings, there is an increase in women’s probability of unintended pregnancy: the probability of currently having an unintended pregnancy more than doubles, with as few as five years of school. These results are notable given evidence that it is especially consequential to transition into motherhood as the result of an unintended pregnancy.
Together, the robustness of the study results to the comparison group and sample criteria attests to the stability of the key finding that education can be a risk factor for unintended pregnancy among women in low contraceptive contexts. Nonetheless, the study design leverages cross-contextual variation, comparing contexts that may differ in ways more numerous than the contraceptive environment alone. To assess the sensitivity of our findings to the cross-contextual variation, in a final, extensive set of robustness checks, we adopt a historical research design. Specifically, we study a single country context over a period of dramatic fertility and contraceptive change and analyze if there is a temporal shift in the association between women’s education and their risk of unintended pregnancy.
Specifically, we focus these analyses on Malawi, a small southeast African country where the prevalence of modern contraceptive use doubled over a brief 15-year period (2000–15; see Figure A3 11 ). With repeated, cross-sectional DHS Program data, we examine if the relationship between education and women’s risk of unintended pregnancy changed with this societal shift, evolving from an initial risk factor for unintended pregnancy to a protective one after societal conditions supportive of lower fertility desires emerged. Specifically, we use Malawi DHS data from 2000, 2004–2005, 2010, and 2015–2016 12 . See Appendix Table A7 for information on the analytic samples.
We again estimated multilevel logistic regression models of the association between women’s education and unintended pregnancy. Figure A4 plots the predicted probability of unintended pregnancy (vs. no pregnancy in the top panel; vs. intended pregnancy in the bottom panel) by women’s education in Malawi between 2000 and 2015. The figures show that when contraceptive use was low, education was a significant risk factor of unintended pregnancy, yet education converted to a (nonsignificant) protective factor as the contraceptive context shifted in subsequent years.
Study Limitations
Before turning to discuss the study results, it is important to acknowledge limitations that remain despite our exhaustive empirical approach. One limitation is that the study can only measure those constructs available in observational data. As such, we lack empirical markers of many of the concepts discussed throughout the study. Rather than demonstrate empirically that education corresponds with women’s adoption of ‘global scripts’—like the desirability of lower fertility—we instead rely on the literature that has established these linkages. Furthermore, although we are interested in the contraceptive context as a marker of the overall ease by which women want to and can control their fertility, we lack hard measures of each of these difficult-to-observe dimensions of the reproductive contexts in which women reside and instead approximate them with the tangible measures that we do have.
One notable dimension of the reproductive contexts in which women reside that is measurable yet we lack measures of is women’s access to abortion. Although a country-level fixed-effects approach allows us to control for constant, unobserved factors that vary across countries, including the legality of abortion, we lack information on variation in access to abortion, which may correlate with the contraceptive context. However, although a high proportion of unintended pregnancies are aborted (Bearak et al. 2022), it is important to note that our data likely disproportionately feature pregnancies that women are planning to carry to term. That is, because the DHS data feature women’s self-reports of pregnancy and women can selectively disclose their pregnancy, we suspect we are largely capturing unintended pregnancies that women do not intend to terminate.
Moreover, we lack other measures of women’s affect, including in response to the unintended pregnancies that we capture here. Despite growing recognition that women often find their unintended pregnancies acceptable (Aiken et al. 2016; Gomez et al. 2018; Yeatman and Smith-Greenaway 2021), we are unable to distinguish between what may be qualitatively distinct pregnancy experiences even as they were each labeled as unintended at the time. For example, some of the unintended pregnancies in our data could have resulted from women forfeiting a less important goal to have the more important one fulfilled (Johnson-Hanks 2004)—they may be settling with becoming pregnant sooner than desired to be able to fulfill the goal of marriage.
Additionally, our results pertain only to women, and it is possible that these findings do not extend to men. Moreover, if we were able to account for the characteristics of the men in the lives of the women whom we study, this may offer key insights into the processes documented here. Women do not make reproductive decisions alone; their partners’ intentions are highly relevant to the actions taken (Miller and Pasta 1995; Thomson 1997). As outlined in the background, it is entirely possible that the findings reflect educated women’s partners’ desires trumping their own and the low contraceptive context—and broader fertility and gender context it entails—leaving them with few options to achieve their desires that may differ from those of their partner. Indeed, to the extent that these pregnancies reflect men’s desires and not women’s, it is possible that highly educated men may be experiencing precisely what they desire across distinct reproductive contexts despite the same not being true for women (Dodoo 1998). Furthermore, given that our results are population-based and thus speak to the average experience of women in our data, it is possible that there are subsamples of women for whom the results are more or less salient—a question that we hope will motivate future research.
Furthermore, the broad categorization of pregnancies as “unintended” will leave some readers rightly unsatisfied. We are unable to account for any degree of ambivalence or variation in the strength of a woman’s desires. As such, some differential selection of more highly educated women’s commitment to their pregnancy desires could be implicated. As Johnson-Hanks (2006:20) specifies, “selectivity effects are not threats to the data quality but are instead the processes most central to understanding a phenomenon”; thus, to the extent that highly educated women in differing fertility contexts are themselves different is an interesting and plausible possibility. Nonetheless, robust evidence that unintended pregnancies still lead to women’s health decline—even in highly pronatal contexts (Yeatman and Smith-Greenaway 2021)—emphasizes the need to understand how and why women end up in situations where their personal desires go unrealized.
Discussion and Conclusion
Education encourages individuals to form aspirational desires for their futures, but people are constrained by the limits that attend their social context. In this study, we center this dualism and show how societal conditions can invert the education–achievement link, leaving the most highly educated paradoxically at risk of maintaining unattainable desires and thus experiencing undesired outcomes. Countering the extant literature on the salutary effects of education, we find that in low- and middle-income settings, where societal support for limiting fertility is generally lower, education does not lower women’s odds of unintended pregnancy. Indeed, in pockets where contraceptive use remains particularly limited, education corresponds with women’s significantly higher odds of unintended pregnancy.
Sewell (1992:20–21) noted that the “kinds of desires people can have, what intentions they can form, and what sorts of creative transpositions they can carry out vary dramatically from one social world to another depending on the nature of the particular structures that inform those social worlds.” Our study results emphasize that an equally striking reality is the degree to which the social world itself conditions one’s ability to achieve those desires. In many contexts, education can paradoxically undermine achievement by encouraging individuals to form desires that are simply unattainable under existing contextual constraints. Thus, although the most highly educated women share lower fertility desires across diverse fertility contexts, those in settings where these ideas are not widely supported experience significant friction between what they desire and what they experience. Thus, although the notion that education is a major determinant of women achieving their lower fertility goals has motivated a slew of progressive policies aimed at getting low- and middle-income countries to expand educational access (Grant 2015), this study shows things can go awry: local constraints can impede the potential for education to facilitate a goal. Education can profoundly shape individuals’ ideas about what they want, but their ability to realize these goals is deeply dependent on their access to the broader resources needed to bring those desires to fruition.
Even as past work emphasizes the relativity of educational benefits, the prevailing notion is that education is universally advantageous, with only the size of the advantage varying (Brand 2010; Brand and Davis 2011). Our results are thus distinct from the growing literature on the “heterogeneous effects” of education in the United States (Brand and Xie 2010) because they show that the benefits of education are not universal—varying only in size—but instead can invert. Indeed, in our data, we do not find strong evidence of education having a protective impact on women’s likelihood of unintended pregnancy—even in contexts where contraceptive use is more common. Although this may be surprising on its face, our results align with little acknowledged findings that defy the overarching narrative of education as protective against unintended pregnancy. For instance, consider historical findings from U.S. data from the 1970s, when modern contraceptives had only recently become available: at that time, the unintended pregnancy rate was higher for more highly educated women (Hayford and Guzzo 2016). Moreover, the results align with Bongaarts (2003) reporting select inversions of the prevailing pattern of lower unwanted fertility among more highly educated women. By demonstrating the systematic variability in the link between education and unintended pregnancy across distinct contraceptive contexts in a comparative framework—leveraging data on hundreds of societies across the globe—our study affirms the contextual dependency of educational benefits.
Our study adds to the chorus of concern related to the potentially meager returns of education for women in many communities across the globe. Although investing in girls’ education has become a de facto development strategy, a growing number of studies emphasize that educational attainment does not always produce the expected gains, from mastering cognitive skills (Smith-Greenaway 2013) to generating economic opportunity (Chatterjee, Desai, and Vanneman 2018). This work complements the growing literature that has carefully attended to changes in the meaning of education as the institution expands (Frye and Lopus 2018; Grant 2015; Lopus and Frye 2020; Urbina 2022) by demonstrating that contextual differences are another axis of variation.
The study also speaks to other literatures emphasizing cases wherein women lack the means to achieve the desires they form. Although we focus on the case of unintended pregnancy, this work is relevant for understanding the toll that other unachievable desires can have on women. For instance, Mojola’s (2014, 2015) research on how globalization and consumer expectations and desires are misaligned with the economic constraints that young Kenyan women face offers a nice parallel. In line with the Western codes of modernity, in contemporary Kenya, consumption is a central element of being a “modern woman,” with scripts that “bind modern femininity and consumption” together (Mojola 2015); yet against the backdrop of gender inequality in access to income, women are dependent on men to engage in conspicuous consumption. Because women’s consumer desires are constrained by their economic realities, they often engage in behaviors that put their health at risk to remedy the disjuncture between what they want and what they can achieve.
Maintaining a set of unattainable desires may not only put women’s health in jeopardy, as Mojola’s (2014, 2015) work documents, but could also have broader societal consequences. Grounded in anomie and strain theory (Agnew 1992; Merton 1938), some work has pointed to the implications of unattained desires for youth delinquency. When youth realize that there are no paths by which they can achieve their expectations, they create new ones through antisocial means (Chavez Villegas 2018; Kabiru et al. 2013). As such, unrealized desires can undergird social unrest and political turmoil (Oberschall 1969), as evidenced in the “Arab Spring” (Campante and Chor 2012). Across low- and middle-income countries, a growing share of youth are achieving higher levels of education, yet the broader provisions needed to facilitate their goals—from economic aspirations to marital and fertility plans—are missing. As education encourages them to develop templates for their lives that contrast with their circumstances, this could be consequential for their well-being and sense of life satisfaction and the stability and health of the collective society. Although past recognition of this conundrum has centered mostly on youth angst due to limited economic opportunities (Bloom 2012), our results emphasize the need to think more broadly—not just about the consequences of unfulfilled economic desires but also of other equally important life domains.
The settings where educational expansion is recent and youth desires are often misaligned with their immediate context are also those where youth make up a sizeable share of the overall population, emphasizing the urgent need to understand the consequences of the collision of global scripts with local constraints. Even as the education–achievement link has a long and venerable showing across diverse contexts, the results from this study remind us that the potential for education to benefit individuals is fraught with contingencies. This contextual dependency requires that we anchor women’s educational experiences to the specific conditions in which they are charting their life’s course.
Footnotes
Appendices
Demographic and Health Survey Included in the Historical Analyses of Malawi.

| Year | Total Women Sampled | Childless Women | Final Analytic Sample | % Excluded due to Missing Data | |
|---|---|---|---|---|---|
| Malawi (historical analysis) | 2000 | 13,220 | 1,798 | 1,731 | 3.7 |
| 2004–2005 | 11,698 | 1,517 | 1,472 | 3.0 | |
| 2010 | 23,020 | 2,678 | 2,570 | 4.0 | |
| 2015–2016 | 24,562 | 3,447 | 3,376 | 2.1 |
Acknowledgements
This research was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R03-HD097360) and the NICHD-funded University of Colorado Population Center (P2C HD066613). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. An earlier version of this paper was presented at the 2022 Population Association of America meeting–we thank session 213 participants for their helpful feedback. The authors also thank the Socius Editors and two anonymous reviewers for helpful feedback.
Data Availability
The data underlying this article were secured with permission. All data used in this study are publicly available. Demographic and Health Survey Program data are available for public use at https://dhsprogram.com/ and ![]() . Files to fully replicate all results on the public-use data are available upon request.
. Files to fully replicate all results on the public-use data are available upon request.