
Abstract
Drawing on content analysis of 517 New York Times news reports published between 1995 and 2016, the author examines the institutionalization of opioid responses in terms of changing media framing of opioid use. The findings indicate that news frames were situated between the lenses of medicalization and decriminalization. Modes of penal social control shifted as early as the 1990s because of budgetary concerns. Drug reform efforts pushed law enforcement agencies to criminalize doctors and big pharma. Consequently, medical professionals and social activists advocated for new cultural frameworks about opioid use. However, the expansion of medical concepts alone did not medicalize opioid use, as evidenced by persistent news frames opposing opioid maintenance treatments. Instead, medicalization materialized as part of the public health solution when law enforcement agencies adopted new modes of medical social control. This article illustrates the making of a new penal-medical nexus regulating drug use.
Media framing of opioid use has changed since the 1990s. When reporting opioid use incidents, news articles shifted from discussing crimes and risks, such as arrests made against heroin users and a “false sense of security” heroin might provide (Alvarez 1995), to focusing on public health responses and treatment options, such as “good Samaritan laws that provide immunity to people who call 911 to report an overdose” and “the dearth of available treatment [for] persons with an opioid use disorder” (Seelye 2016). The profiling of people who use opioids has also changed from potential criminals to people needing medical treatment. Although many have discussed elements contributing to these changes, such as paradigm shifts (Fischer and Rehm 2018; Shachar et al. 2020), social marginalities (Ezell et al. 2021; Kim, Morgan, and Nyhan 2020; Netherland and Hansen 2016), and political factors (Gollust and Haselswerdt 2021; Grogan et al. 2020; Weiss and Zoorob 2021), few have explored how this changing media framing “loops and spirals” (Ferrell, Hayward, and Young 2008) around changes in modes of penal and medical social control: how the social construction of opioid use and the institutionalization of new opioid responses feed into each other in producing a new regime on the drug problem. Through the conceptual framework of “institutional logics,” an inquiry into how historical and socially constructed patterns of ideas and practices are influenced and reproduced by individual and organizational actors (Thornton, Ocasio, and Lounsbury 2012), in this article I examine changing media framing of opioid use as a case of how the institutionalization process interacts with the social construction of a public health crisis.
Sociological studies on the drug problem often situate discussions in two theoretical frameworks: (bio)medicalization and (de)criminalization. The former explores how the medical institution medicalizes opioid use through the penetration of medical concepts into everyday life (Campbell 2012; Conrad and Mackie 2011), while the latter examines how the criminal justice institution incorporates medical solutions in creating a knowledge complex regulating social marginalities (Beckett and Brydolf-Horwitz 2020; Fassin 2011). Using these two frameworks, recent studies depict the social construction of the opioid crisis as mainly led by a narrative change of medical concepts penetrating the criminal justice institution and the wider society (Bowen and Irish 2019; Kim et al. 2020; Netherland and Hansen 2016; Smirnova and Owens 2017).
However, it remains unclear how distinct these two institutions, criminal justice and medicine, were in reframing the narrative. Historically, actors in both institutions readily brought together competing ideas and concepts into their practices and often blurred the boundaries of punishment and treatment (Campbell and Lovell 2012; Fuentes et al. 2020; Rafalovich 2020; Showalter 2019). In recent years, punitive treatments, such as prescription monitoring programs and treatment programs supervised by drug court–assigned case managers, have appeared more frequently (Chiarello 2015; Kaye 2019; Revier 2019; Tiger 2017). In these cases, the medical institution prioritizes punishing people with tendencies toward drug abuse over their well-being.
Moreover, the media plays a pivotal role in shaping narrative interpretations and thus reshaping practices on the basis of emerging narratives (Andrews and Caren 2010; Carter 2013). Recent studies have also shown that emerging media framing of the opioid crisis is beyond the one-way transition from punishment to treatment, questioning the traditional understanding of institutional influence (Bagley and Bright 2020; Orsini 2017; Webster, Rice, and Sud 2020). How, then, can we explain the changing media framing of opioid use beyond narrative changes originated from within static institutional boundaries? How did changes in modes of penal and medical social control interact with changes in media framing? What reality did emerging media framing construct? Moreover, how did medicalization and decriminalization, two major processes shaping opioid use narratives, happen in relation to each other in the social construction of the opioid (overdose) crisis?
To investigate these issues, I draw on quantitative content analysis of 517 New York Times articles published between 1995 and 2016 on the issue of opioid use, as well as qualitative analysis of articles from the same sample pool and opinion pieces and letters to the editor from the same source. Specifically, I compare different news frames (Carter 2013; D’Angelo 2018) that emerged in clear stages over the course of 22 years. I also examine how different framing ideas and practices (Aronowitz 2008; Brown 1995) 1 constructed these news frames. Quantitative assessments show that media framing of opioid use changed in multiple ways: responses changed from maintenance-based treatment options to abstinence-based control options, labels for opioid users changed from “addicts” to “patients,” targets to blame changed from drug dealers to doctors and pharmaceutical companies, and prosecutors and politicians became more active in the press. Qualitative analyses of these changes reveal that the decriminalization of opioid use happened much earlier than the medicalization process, mainly because of budget concerns. Modes of penal social control switched to emphasizing cost-efficient approaches and preferred treatment over incarceration. On the other hand, modes of medical social control extended to penal institutions as drug reforms left vacancies for regulating people who use drugs. Together, decriminalization and medicalization developed in parallel before reaching a junction to construct the opioid crisis as a crisis of overdose and treatment.
(Bio)medicalization, (De)criminalization, and the Penal-Medical Nexus
Contemporary (bio)medicalization frameworks adopt a social constructivist perspective in studying the penetration of medical knowledge into everyday life (Busfield 2017; Clarke et al. 2003; Conrad 2005; Williams, Martin, and Gabe 2011). Recent (bio)medicalization studies explain how an expanding reservoir of medical concepts turns social conditions into medical problems (Conrad and Bergey 2014; Epstein and Mamo 2017), particularly through the media (Arguedas 2020; Harwood et al. 2017). Contemporary studies on the drug problem follow this trend and explore how drug use is medicalized as medical concepts are spread from the medical community to the media and the wider society. For example, concepts such as opioid use disorder (OUD) and medication-assisted treatments (MATs) destigmatized drug use in the news and behind the bar, which in turn contributed to an encouraging environment for opioid use treatment and intervention (Netherland and Hansen 2016; Smirnova and Owens 2017).
However, medical concepts alone do not necessarily change the public perception of medical issues. Schnittker (2008) found that the growing popularity of medical explanations of mental illnesses did not lead to an increase in the tolerance of those conditions. Moreover, concepts developed by medical professionals do not always reflect medical purposes (Correia 2017; Davis 2006). For example, the label psychopath was created more in accordance with legal and penal criteria than medical ones (Showalter 2019). It was invented to serve criminal justice purposes: to assess the dangerousness of inmates. In other words, “psychopath” was a penal concept, not a medical one, despite being developed by medical professionals. Cases like this show that the expansion of medical concepts alone does not necessarily trigger the medicalization process.
On the other hand, the expansion of medical social control contributes to the social construction of medical issues. This medical social control differs from early medicalization theories emphasizing professional authority. Instead, it demonstrates that any power dynamic can institutionalize medical concepts and practices, not just medical authorities. As Rose (2001) put it, medicalization is simply one process of power dynamics in a network of power relations containing many modes of social control. In this context, Hancock (2018) showed how direct-to-consumer advertising redefines what is normal/abnormal through “the normalizing gaze” and thus medicalizes social conditions. Besides medical experts, lay experts, biomedicine, and the pharmaceutical industry can all be sources of power that either operationalize or internalize medical concepts and practices. Thus, medicalization happens when new power relations are filtered through any social arena that institutionalizes medical knowledge. Recent studies have demonstrated that, in cases involving multiple sources of expertise, medicalization intertwines with other processes, such as decriminalization (Greil et al. 2020; Lin 2017; Rafalovich 2020; Sundaram 2019). The result is hybrid institutional concepts and practices. In sum, a growing body of (bio)medicalization literature shows the necessity to explore the medicalization process through changes in medical social control, not just as an expanding reservoir of medical concepts.
(De)criminalization is another significant process shaping the social construction of opioid use. Sociologists focusing on the criminal justice institution note that penal social control has been transformed in the context of addressing mass incarceration and racial inequality (Beckett and Western 2001; Wacquant 2001; Western and Wideman 2009). The mass incarceration of drug offenders has turned into a problem unto itself, thus contributing to the decriminalization of drug use. However, recent studies show this transformation has not weakened penal social control. Instead, law enforcement agencies shifted from criminalizing drug possession to pursuing drug distributors (Beckett and Beach 2021; Beckett and Brydolf-Horwitz 2020).
Scholars studying the drug problem have discussed the implications of this transformation. Some focus on the criminal justice institution and present empirical evidence for displaced penal and medical narratives on policy and ground levels (Bowen and Irish 2019; Kim et al. 2020). Others note that penal social control has changed its ways of regulating social marginalities. For example, Revier (2019:6) theorized “a repackaging of carceral control,” arguing that the drug war approach incorporates noncriminal justice expertise to cope with criminal justice reforms while penal social control persists. In examining the drug court movement, Tiger (2012) painted a gloomy picture: the merger of the medical and penal frameworks creates a more coercive social control institution than ever. This hybrid institution now regulates not only poor urban minorities but also poor rural whites. Kaye (2019) noted that the establishment of the drug court marks a second wave of the neoliberal penology approach based on cost-benefit analysis. In this case, reforms in the criminal justice institution were more about economic concerns than social justice reasons. These studies show how penal social control in contemporary society has been extended beyond the criminal justice institution. Together with (bio)medicalization studies, they indicate the birth of a hybrid institution regulating opioid use.
Institutionalization, Institutional Logics, and the Making of the Penal-Medical Nexus
Although studies under both (bio)medicalization and (de)criminalization frameworks show that the medical institution and the criminal justice institution can produce hybrid forms of social control and thus update the penal-medical nexus regulating the drug problem, they often fall short in documenting the institutionalization process itself. Part of the reason lies in the current conceptual constructions of these two frameworks: both assume institutions and institutional actors as relatively static, such that the institutionalization processes remain underexamined. Although the two frameworks emphasize distinct areas of institutional knowledge and expertise, they share a core object of investigation: a process, a period, or a way of institutionalizing forms of social control into concepts and practices. In this article, I view institutions, such as criminal justice and medicine, not as fixed categories but as processes that reproduce and reconfigure ideas and practices.
I study the entanglements of different social control powers into hybrid institutional forms through the conceptual framework of “institutional logics” (Thornton et al. 2012). This perspective investigates how individual and organizational actors are influenced by and (re)produce historical and socially constructed patterns of ideas and practices. It is particularly relevant for understanding institutional changes over time (Scott et al. 2000; Thornton and Ocasio 1999) and explaining how competing or contradicting logics help establish new institutional norms (Dunn and Jones 2010; Furuta, Schofer, and Wick 2021)
Studies on the drug problem primarily use institutional logics to examine micro-level decision-making processes. For example, McPherson and Sauder (2013) showed how drug court participants manage institutional complexity by balancing multiple and conflicting institutional and organizational demands. Chiarello (2015) demonstrated how pharmacists faced pressure from competing institutional logics of medical and legal gatekeeping and became frontline workers reconciling two institutional demands.
Yet studies have not fully used the framework. Thornton et al. (2012) distinguished three levels of institutional logics: micro, field, and societal. The institutionalization of ideas and practices is more than micro-level decision-making processes. Few studies on the opioid crisis have analyzed how “field-level logics are both embedded in societal-level logics and subject to field-level processes that generate distinct forms of instantiation, variation, and combination of societal logics” (Thornton et al. 2012:148). As an exception, Showalter et al. (2021) explored how emerging organizational features moderate conflicting institutional logics. Their study illustrates how naloxone distribution as an opioid response was institutionalized.
The media is an ideal site for examining interactions between field-level processes and societal-level logics. It determines whether institutionalizing efforts can attract enough attention for stakeholders to proceed with desired institutional and social changes (Andrews and Caren 2010). It also constructs reality as news frames influence how the audience interprets events and turns narratives into practices (Carter 2013). For the opioid crisis, societal-level logics, such as treatment, abstinence, and punishment, are presented and represented in the news as field-level processes, such as (bio)medicalization and (de)criminalization, institutionalize emerging ideas and practices regarding opioid use. Although field-level processes often comply with societal-level logics (e.g., when medical professionals explain the necessity to expand MATs and law enforcement agents show how they destroyed a drug ring), they can also generate hybrid forms of ideas and practices, as when police officers present themselves as lifesavers in using naloxone kits and doctors talk about reporting patients to the authority in preventing drug abuse. Recent studies have confirmed that the changing media framing of opioid use is not simply a one-way transition from punishment to treatment. Instead, negative frames on treatment options (Bagley and Bright 2020), stigmatization of people who use drugs (Orsini 2017), and discussions of criminality (Webster et al. 2020) are still prevalent.
In this article I identify the historical and institutional contexts that enable multiple institutionalization processes to interact with emerging media framing and assemble new responses to opioid use. I aim to reveal how each mode of social control identifies problems, updates agendas toward solutions, and thus interacts with news frames to push for institutional and social changes. By distinguishing medical social control from penal social control and tracing each of their developments, I show how decriminalization, in terms of less prison-oriented modes of penal social control, shaped media framing of opioid use, which in turn pushed forward medicalization, in terms of more medication-oriented modes of medical social control. When the two processes came into a conjuncture, new hybrid forms of responses, such as promoting MATs with low abuse risks and equipping police officers with overdose-reversal medications, were institutionalized, and the drug problem was reconstructed as an opioid (overdose) crisis.
Data and Methods
The news sample is drawn from the New York Times between 1995 and 2016. The Times is a nationally distributed newspaper covering global and local issues. It is ideal for investigating media attention (Andrews and Caren 2010) to the drug problem across multiple levels. Its proximity to the Northeast and the eastern part of the rust belt made it sensitive to the first institutionalization efforts from key stakeholders. The starting point, 1995, was the year when OxyContin, the infamous drug often accused of causing the opioid crisis, was approved by the U.S. Food and Drug Administration (FDA) for pain management. Before that, there was no discussion of the prescription drug abuse issue. The end point, 2016, was the year when the first national opioid legislation, the Comprehensive Addiction and Recovery Act, was passed. After that, the drug problem had an official name—the opioid (overdose) crisis—along with validated responses that were made into law.
I used the following keywords to search headlines and leading paragraphs of news articles in the LexisNexis (now called Nexis Uni) newspaper database: “heroin/painkiller/prescription drug/opioid/opiate” and “addict 2 /misuse/abuse/overdose/death/crisis/epidemic.” These search terms were consistent with prior studies on media framing of opioid use (Bagley and Bright 2020; McGinty et al. 2016; Netherland and Hansen 2016; Russell, Spence, and Thames 2019). This yielded 1,339 articles. The articles were then coded into five news types: “corrections and quotations,” “to the editor,” “opinion,” “entertainment,” and “standard.” 3 Furthermore, articles were marked as either “irrelevant,” “relevant,” or “focused.” 4 The final data pool consisted of 517 “standard” and “focused” articles (see Figure 1). The amount of news media attention to all types of opioids in these 517 articles remained stable from 1995 to 2013. Starting in 2014, however, interest mounted thanks to speeches by politicians such as Governor Peter Shumlin (D-Vermont) and the deaths of celebrities such as Philip Seymour Hoffman. The media attention then retreated in 2015 because of the lack of follow-up events.

Numbers of news articles on heroin, painkiller/prescription drug, and opioid/opiate, New York Times, 1995 to 2016.
Following previous examples (Orsini 2017), I divided the period under examination into four chronological stages. I compared changes in the use of news frames across these stages. The four stages were determined by patterns of drug mentioning (see Figure 2): (1) from 1995 to 2000, heroin appeared in 95 percent of all the 517 articles, while painkiller/prescription drug (Rx) and opioid/opiate (opioid) appeared in only about 20 percent of them; (2) from 2001 to 2009, both heroin and Rx articles were about 60 percent, while opioid articles were less than 30 percent; (3) from 2010 to 2013, heroin articles continued to decline to about 50 percent, Rx articles continued to climb to about 80 percent, and opioid articles jumped to more than 60 percent; and (4) from 2014 to 2016, heroin articles recovered to about 80 percent, Rx articles retreated to about 60 percent, and opioid articles reached almost 80 percent. These four stages were the key independent variable in content analysis.

Opioids mentioned in “standard” “focused” news.
Coding
I aim to understand how shifting social control patterns interact with media framing of opioid use. I saw penal and medical social control in both discourses and practices of relevant stakeholders. On the basis of similar media framing studies (DiBennardo 2018; Van Gorp and Vercruysse 2012; Viladrich 2019; Webster et al. 2020), news frames of opioid use after 2016, and my reading of a subsample of news articles, I developed three sets of dependent variables for content analysis: (1) a spectrum of responses to the opioid problem, (2) social categorizations of the people involved, and (3) demographic categories. I coded these variables at the article level for all the articles in the final sample pool. The coding procedure was straightforward: if a keyword for a given variable appeared in an article, the article would be counted. Thus, the variables were all dichotomous, and the codes in each of them were independent of each other. All the expected values in the sample were larger than 5, making the χ2 test a decent measure of statistical significance.
In the Comprehensive Addiction and Recovery Act, certain responses to the opioid problem were included, whereas others were not. In this context, four categories of responses were created on the basis of each of their institutional logics and major sponsors: (1) social service options advocated by activist groups (needle exchange programs and safe drug injection sites), (2) maintenance-based treatment options practiced by medical professionals (methadone and Suboxone programs), (3) abstinence-based treatment options practiced by medical professionals (detoxification [detox] and naltrexone programs), and (4) abstinence-based control options performed by law enforcement agencies (naloxone kits for police officers and drug disposal sites in police departments). I also included a fifth category of crime to measure changes in the traditional role of law enforcement.
Three sets of variables were developed to help understand how the social categorizations of people involved in opioid framings changed. “People affected” contained two labels: addicts and patients and victims. “People accused” contained four major targets often accused of causing the opioid crisis: drug dealers facilitating drug sales, doctors overprescribing restricted opioids, painkillers and pharmaceutical(s) that are aggressively marketed, and the FDA loosening regulations on controlled substances. “Institutional voices” referred to people with institutional identities whose opinions were presented in the news. This set of variables includes doctors (Dr.), 5 police officers (police), prosecutor(s) and the Drug Enforcement Administration (DEA), and politicians. 6 In addition, certain demographic categories (race, class, gender, age, population size, and party affiliation) were established to help understand how opioid use was associated with different social groups.
Beyond the quantitative analysis, I also did discourse analysis to examine how changes in power relations interact with changes in news frames over these 22 years. In accordance with tradition (Wagner-Pacific 1994) as well as contemporary examples (Chuong, O’Doherty, and Secko 2015; Orsini 2017), I focused on power relations in the relationship between speech and institutions. There are two types of speech in my case: (1) directly cited speech from institutional voices and (2) news articles themselves as institutional speech. Accordingly, I examined two processes: first, how different stakeholders presented themselves or were represented in the news media and, second, how the news media framed opioid use under the influence of the power dynamics in the first process. Articles containing statistically significant variables were read and analyzed in detail. Themes were created on the basis of patterns of word choice, reporting sentiments, and the substantive matters involved. Quotations were attached to illustrate key themes as well as their negative cases. These themes were not solely about explaining variations found in the quantitative analysis but also about detailing those variations, revealing new variations, and showing general patterns in how news frames about opioid use interacted with the institutionalization of emerging opioid responses.
Findings
The news sample showed distinct differences among the four stages. From 1995 to 2000, articles blamed people who used drugs and suggested punitive measures within the criminal justice institution. For example, people were more likely to be labeled as addicts than as patients or victims, and the safety and ethics of providing medical treatments, such as methadone programs, came under strict scrutiny. From 2001 to 2009, articles focused on the prescription drug abuse issue, particularly by promoting the image of innocent, suffering OxyContin abusers, and blaming doctors and big pharma. Prosecutors and the DEA also receive more attention during this stage. From 2010 to 2013, medical professionals made a bigger presence, as they were both criticized for over-prescription and consulted for tentative solutions. From 2014 to 2016, hybrid responses became widely accepted, and articles turned to social inequality issues.
Changing News Frames: Different Targets, Same Stigma
As shown in Figure 3, medicalization did not happen in terms of promoting treatment-oriented responses, and decriminalization did not occur in terms of reducing control-oriented responses. The percentage of articles mentioning social service options declined from 13 percent in stage 1 to 1 percent in stage 3 and remained below 10 percent in stage 4. Articles mentioning maintenance-based treatment options shifted from more than 30 percent in stages 1 and 3 to less than 20 percent in stages 2 and 4. Articles mentioning abstinence-based treatment options declined steadily (changes not statistically significant). On the other hand, articles mentioning abstinence-based control options (i.e., naloxone and drug disposal sites) increased dramatically, from 2 percent in stage 1 to 29 percent in stage 4. Articles mentioning crime also increased, from 25 percent in stage 1 to an average of 39 percent in the later three stages.

Percentage of articles mentioning specific response options to opioid addiction.
Conceptual changes did happen, as evidenced by changing labels for opioid users. News articles in earlier years were more likely to mention addicts. In comparison, those in later years were more likely to mention patients and victims (see Figure 4). Seventy percent of the news articles in stage 1 mentioned addicts, compared with about 50 percent in stages 2 to 4. About 40 percent in stages 1 and 2 mentioned patients or victims, compared with about 55 percent in stages 3 and 4. Thus, the cultural image of people who use opioids shifted from undeserving junkies to innocent sufferers. In stage 2, however, both labels were used less. This dip is further examined in the following qualitative analysis sections.

Percentage of articles labeling opioids users.
The cultural image of drug dealers also confirmed conceptual changes. Yet this change was not about destigmatization but more about adding new names to the blame game. As shown in Figure 5, the percentage of articles mentioning drug dealers and drug traffickers remained stable across the four stages (changes not statistically significant). In contrast, the percentage of articles mentioning doctors, painkillers and pharmaceutical(s), or the FDA increased drastically in stages 2 and 3 before slightly retreating in stage 4. In other words, the media continued stigmatizing drug distributors, as doctors and big pharma became the new devils responsible for causing the opioid crisis.

Percentage of articles mentioning specific entities.
The cultural image of institutional voices showed an interesting pattern (see Figure 6). The percentage of articles mentioning doctors as speakers (Dr.) declined from 49 percent in stage 1 to 41 percent in stage 2, surged to 63 percent in stage 3, and settled at 50 percent in stage 4. Changes in mentioning police were not statistically significant. There was a contrast between articles mentioning prosecutors and the DEA and those mentioning politicians. In stage 2, prosecutors and the DEA made the most news (44 percent), while politicians made the least (15 percent), compared with themselves in other stages. Starting in stage 3, however, politicians became more engaged, while prosecutors and the DEA showed up less. In stage 4, politicians reversed the trend and made more news appearances (34 percent) than their counterparts (26 percent).

Percentage of articles mentioning specific participants.
Regarding demographic factors, only party affiliation, race, and population size showed significant results. Representatives and senators reacted to the opioid issue faster than governors and mayors, and Democrats reacted faster than Republicans. In both cases, the former group appeared more in stages 3 and 4, while the latter appeared more in stage 4. Media attention to whites raised significantly in stage 4 (p = .049). Any race (including whites and nonwhites) was not statistically significant. Articles mentioning rural significantly changed, increasing from 2 percent in stage 1 to 18 percent in stage 3 before retreating to 13 percent in stage 4. Changes in other population variables (i.e., urban and suburb), however, were not significant. Other demographic variables (i.e., class, gender, and age) were not significant predictors in the sample. These differences could be with the New York Times readership. The Times was often viewed as catering to “old white Democrats” (Kafka 2022). Although aging was more about newspaper readership overall, the other two were sound during the period under examination (1995–2016). In a 2012 Pew media consumption survey (Pew Research Center 2012), a typical Times reader was a relatively young man who was highly educated, well paid, and a Democrat. This readership might have given more media attention to Democrats and social justice issues while refraining from turning to discriminative categories.
The General Pattern: Decriminalization and Medicalization Developed in Parallel
Qualitative analysis of significant variations in quantitative assessment showed that decriminalization and medicalization significantly contributed to institutionalizing new concepts and practices regarding opioid use. They occurred, however, in parallel before reaching a junction: prioritizing the reduction of opioid overdose deaths over the prevention of opioid abuse or the treatment for addiction suffering. In other words, two field-level institutional logics, penal and medical, independently developed diverse responses to the opioid issue, even though they periodically crossed fixed-institutional boundaries to expand their social control powers.
Modes of penal social control moved from incarceration to other alternatives. Among these alternatives, those easing punitive measurements on drug users, including medical treatments, won out for cost-efficiency reasons. As drug reforms continued, the discretion of whether to divert drug offenders to treatment was handed over from prosecutors to judges, freeing medical assessments from law enforcement interpretations. Prosecutors and the DEA thus switched their focus from people who use drugs to those who provide drugs. These changes opened the door to the possibility of treating people with medications. They happened mostly in stages 1 and 2 before efforts advocating for MATs and harm reduction became significant (see Figure 7).

The decriminalization process.
As the public became more aware of the prescription drug abuse crisis in the early 2000s, medical concepts were more frequently discussed. However, this alone did not medicalize the drug problem, as evidenced by the persistence of negative news frames associated with maintenance-based treatment options. Instead, the expansion of medical social control to nonmedical professionals medicalized opioid use. As law enforcement agencies started to provide medical interventions, the power of defining and responding to the drug problem as a medical one was steered away from medical professionals, creating room for new medical products, procedures, and practices associated with nonmedical professionals (see Figure 8).
The medicalization process.
Starting Drug Reform: Seeking Alternatives Because of Budget Concerns
In the summer of 1998, New York City mayor Rudolph W. Giuliani revealed “his desire to abolish all methadone treatment programs for heroin addicts” in the city (Swarns 1998). Immediately, he was flooded with criticism. General Barry R. McCaffrey, the White House drug policy chief, quickly got into an argument with Giuliani, saying that the call conflicted with knowledge of science and medicine. Giuliani wrote back, claiming that methadone treatment was nothing but substituting one drug for another. Their quarrel intensified into the fall. In the end, Giuliani abandoned his ambitious plan after a short experiment in city hospitals, while McCaffrey managed to persuade the Clinton administration to apply his proposal nationwide (Wren 1999).
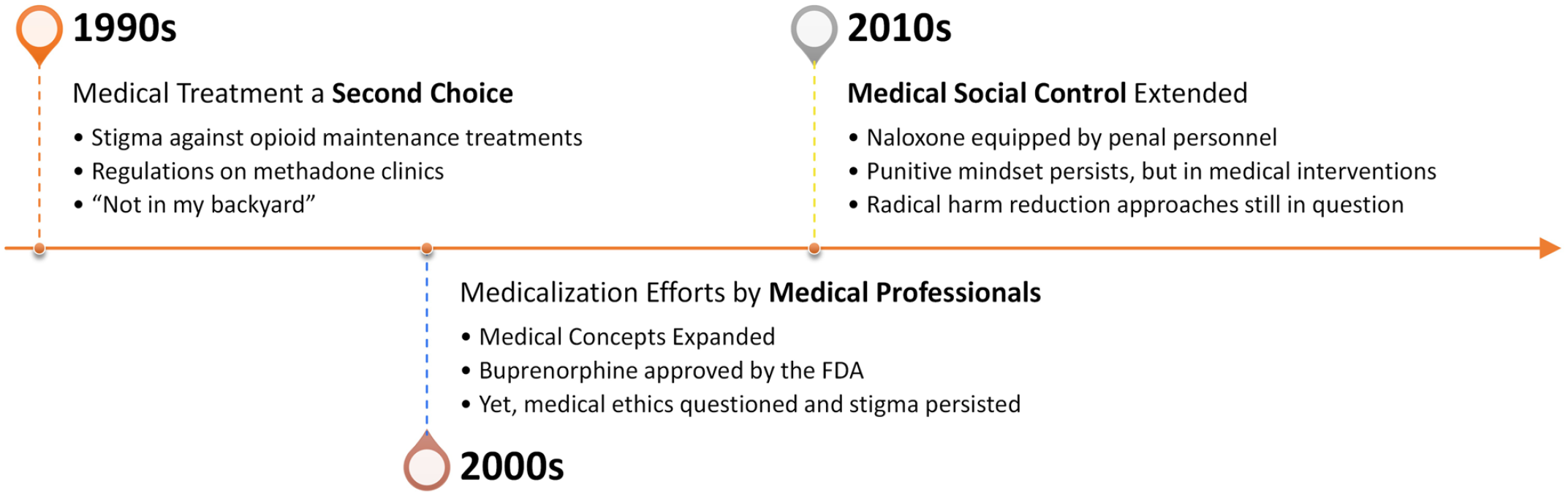
What was behind this unusual exchange between a drug czar and a mayor was a dilemma that bothered lawmakers in the late 1990s: how to reduce drug-related spending without sacrificing a tough-on-crime attitude. Heavy criminalization efforts led to a fast-growing prison population while shrinking government budgets. When presented with studies showing the cost efficiency of expanding treatment, the federal government adopted the policy. On the local level, however, prohibitionists like Giuliani were calling for total abstinence, and local communities were having a “not in my backyard” moment against opioid treatment facilities (Cotsalas 2001).
Nevertheless, incentives for switching to treatment programs were high. An opinion piece commenting on drug policy noted: “But this punitive approach has failed. . . . Our penchant for punishment has blinded us to the most effective strategy for combating drug use: offering comprehensive treatment to every addict who requests it” (Wren 1998a:48). The piece dismissed both radical abstinence approaches like Giuliani’s and radical harm reduction efforts such as drug legalization. It advocated instead for “drug treatment”: “treatment was 7 times more cost-effective than domestic law enforcement, 10 times more effective than interdiction and 23 times more effective than attacking drugs at their source” (Wren 1998a:48). Echoing the drug czar, this article represented a common understanding of the drug problem in the late 1990s. From a cost-efficiency standpoint, treating people who use drugs was way better than overcrowding them in prisons.
At the state level, legislators were also experimenting with treatment-oriented policies. Connecticut, “an unlikely laboratory for experimentation with drug policy,” passed the nation’s first medical marijuana law in 1981, led many other states to offer alternatives to jail, and was considering “a major overhaul of its drug laws that would shift the emphasis from punishment toward treatment of drug abuse as a public problem, in part as an attempt to reduce the costs of imprisonment” (Wren 1997). Connecticut state legislators became interested in these changes simply because they did the math: $25,000 a year to lock up a drug offender versus $8,000 to $10,000 yearly to provide treatment. Moneywise, treatment was appealing.
Overall, budget concerns were the initial force pushing policymakers to introduce substantial changes to nontolerant drug policies. Most significantly, drug offenses were decriminalized, and alternative approaches, particularly drug treatment options, were experimented with in the late 1990s. However, concern about appearing too soft on crime limited the scope of reform and prevented the adoption of radical harm reduction options.
Proceeding with Drug Reform: Adding New Names to the Blame Game
Widely held to be the most severe tough-on-crime laws in New York, the Rockefeller laws set a minimum sentence of 15 years for minor drug possession or drug dealing. In 2001, New York governor George E. Pataki, “a Republican with a tough-on-crime record,” found himself discussing details of reforming the Rockefeller laws with Democrats, with no mention of OxyContin abuse or other prescription drug abuse issues at all (McKinley 2001). The reasons cited for reform were the state’s declining crime rate, an increasing prison population, and minorities being disproportionally affected. Three years later, Governor Pataki signed the Drug Law Reform Act of 2004, reducing the minimum penalty to 8 years and giving more discretion to judges. However, prosecutors, instead of judges, still had the power to decide whether to divert a drug offender to treatment. Another five years later, in 2009, Governor David A. Paterson, a Democrat, with Democrats controlling the state legislature, took further steps to disassemble the Rockefeller laws (Peters 2009). The reforms he later signed into law removed the mandatory minimum sentence and allowed judges to divert drug offenders to treatment.
Other states were also trying to offer alternative pathways for drug offenders. In 2005, Illinois established a new state prison dedicated to drug treatment (Zernike 2005). It gave job training and addiction counseling to drug offenders, aiming to reduce the occurrence of repeated offenses. Again, the cited reasons had nothing to do with expanded medical knowledge or OxyContin abuse but were all about reducing the number of inmates in state prisons.
As drug reform efforts spread, prosecutors switched their focus to pursuing drug-related crimes. The newspaper appearance of New York City’s special narcotics prosecutor illustrates a typical trajectory. Before 2009, Robert H. Silbering (1992–1997) appeared two times and Bridget G. Brennan (1998 to present) appeared four times in the initial sample pool (a total of 748 articles from 1995 to 2008), talking mainly about seizing drugs from smugglers and sharing concerns about heroin attracting younger users. Ms. Brennan appeared 11 times in and after 2009 (591 articles from 2009 to 2016), including in two letters to the editor. As New York’s drug reforms were finalized in 2009, Brennan expressed dissent about downplaying the role of prosecutors in making treatment discretions (Peters 2009). She quickly moved on to collaborate with medical professionals, community organizers, and state legislators in educating people about the danger of heroin (Buckley 2009). Yet less than one year later, she appeared in a news article questioning a message sent out by New York City health officials promoting the safe use of heroin (Hartocollis 2010). This ambivalence indicates that prosecutors such as Brennan had a tough time defending the core value of prosecutors when experimenting with alternative approaches other than simply putting people into prisons.
Ms. Brennan soon found a solution: accusing doctors of murdering patients. In 2011, she charged Dr. Stan XuHui Li with 15 counts of selling drugs and 5 counts of reckless endangerment (Bilefsky 2011). Three years later, Dr. Li was found guilty of 200 of the 211 charges against him, including two counts of second-degree manslaughter (Madan 2014). Targeting doctors and big pharma was hardly a surprise, as federal prosecutors years before had already managed to hold Purdue Pharma accountable for its aggressive marketing (Meier 2007). Dr. Li’s case, however, marked the first time New York charged a doctor with manslaughter on top of the criminal sale, indicating that prosecutors had found ways of applying harsh punishment to newly identified “drug dealers.” News reports on cases such as this did not promote an encouraging environment for expanding maintenance-based treatment options for opioid use. On the contrary, they reinforced a tough-on-crime image for prosecutors such as Brennan, questioning the medicalization of pain management and justifying the criminalization of doctors. However, as law enforcement agencies switched focus from “drug addicts” to new “drug dealers,” they opened the possibility to destigmatize people who use drugs, clearing the way for solving the opioid problem with medical tools.
From Methadone to Suboxone: Negative News Frames All Along
Turning to the medicalization of opioid use, the news sample showed that concepts like “harm reduction” and MATs circulated in public as early as the 1990s. Their future at that moment, however, did not look very promising. Methadone, a synthetic opioid agonist approved by the FDA for treating opioid dependence in 1972, did not get any improvements over the almost 30 years since its approval, nor did regulation efforts against it become any looser (Wren 1999). In fact, the FDA was more concerned with preventing people from reselling methadone on the street. Medical professionals constantly complained about shortage of supplies, tight control over distribution, and the lack of research efforts on alternatives. News frames about methadone treatment were often negative (Wren 1998b). Besides Giuliani’s radical proposal to eliminate all methadone clinics and other “not in my backyard” concerns, methadone was also associated with illicit drug resales, limited effectiveness, and overdose incidents.
Things started to look different at the start of the 2000s as people became more aware of the OxyContin abuse issue. In 2001, a lengthy article tackled this matter, setting the tone for future reports. The reporter, touring the tiny West Virginia town of Man with a local guide, jotted down what he saw: “The neighborhood doesn’t feel dangerous—no graffiti, no pit bulls, no broken bottles lying around. Still, Paula points out criminal activity in every second home, peering through the front windshield and gesturing left and right.” As his informant casually pointed out drug dealers’ houses, the reporter learned that when people wanted to buy pills, “there aren’t lookouts involved, or secret passwords or elaborate drop sites.” Buyers would go to a dealer’s house and “[knock] on the front door in broad daylight” (Tough 2001). These frames show that the categorization of people involved in this new drug problem was evolving. Together with the transformation of penal social control around the same time, these frames provide a way to explain the interesting gap in stage 2, in which both addicts and patients and victims were less mentioned (see Figure 4): although decriminalization efforts diverted attention from “drug addicts” to unscrupulous doctors and big pharma, medicalization efforts still needed some time to mainstream medical understandings of people who use drugs in the media.
Medical professionals took the opportunity to advocate for more medications. They persuaded the FDA to approve Suboxone (a combination of buprenorphine and naloxone) and Subutex (pure buprenorphine) for treating OUD in October 2002 (Markel 2002). Given the success of Subutex in France in the past decade, doctors and public health officials cheered the approvals and hoped that these medications would bring about positive changes. Yet as the drugs revolutionized treatment and gradually replaced the long-stigmatized methadone, scrutiny followed. After almost a decade of quiet development, Suboxone resurfaced in the news for its popularity among people who use drugs, not only because of its effectiveness against opioid addiction but also because of its potential to be abused: More than a decade after Suboxone went on the market, and with the Affordable Care Act poised to bring many more addicts into treatment, the high hopes have been tempered by a messy reality. Buprenorphine has become both medication and dope: a treatment with considerable successes and failures and a street and prison drug bedeviling local authorities. (Sontag 2013)
Scrutiny persisted as medical professionals advocated for the effectiveness of Suboxone in reducing opioid overdose deaths, particularly in stage 3. News stories portrayed correction officers ripping open incoming mail looking for smuggled Suboxone (Goodnough and Zezima 2011), doctors who prescribed Suboxone being rigorously policed for potential misconduct (Sontag 2013), and doctors running abstinence-based rehabs questioning the effectiveness of Suboxone in addressing the core causes of addiction (Glaser 2016). In short, the media framing of opioid use was still mainly about curbing drug abuse instead of addressing addiction suffering, despite efforts from medical professionals. These negative news frames showed that promoting medications and introducing medical concepts in the media only partially contributed to the medicalization of opioid use.
Naloxone: Medical Social Control Performed by Penal Personnel
Naloxone as a medication had two uses: as a supplement in the detox treatment of addiction, it could smooth the transition from opioids to naltrexone, an opioid antagonist; as a stand-alone medication, it was used in emergency rooms to reverse opioid overdoses for decades. On both occasions, the use was exclusive to medical professionals. Before 2010, naloxone rarely appeared in the news. When mentioned, stakeholders expressed little interest in promoting its wider distribution. In 2007, for example, when Massachusetts officials decided to give heroin users naloxone kits to reverse overdoses, they failed to gain “the support of the White House Office of National Drug Control Policy and some advocates in the field, including former heroin users” (Associated Press 2007). Starting in 2014, the situation changed rapidly. As the number of overdose deaths mounted, medical professionals advocated for the FDA approval of naloxone for over-the-counter use (Hoffman 2014). At the same time, law enforcement agencies proposed to equip police officers on duty with naloxone kits (Goodman 2014). The former was a move for medicalizing opioid use via the pharmaceutical industry. It achieved limited success while facing constant scrutiny. The latter, however, revealed a new pathway for expanding medical social control and thus fundamentally altered the trajectory of medicalization.
As mentioned earlier, drug reform efforts diverted the focus of penal social control away from “drug addicts.” This resulted in a practical dilemma for police officers: “drug addicts” were no longer a point of interest in pursuing drug crimes. However, overdose scenes were encountered repeatedly when responding to emergencies. After successful tries, police officers became more willing to step into overdose situations. This became the moment when medical social control managed to fill the vacancy left by penal social control. The police department in Quincy, Massachusetts, was one of the earliest departments to equip its officers with naloxone. The police chief, Paul Keenan, explained the process: Once in a while, you’ll get pushback from officers or the public—why are we saving junkies? . . . But our officers were going to too many houses to explain to families that their loved ones had passed away. We embraced it and we ran with it. (Goodman and Hartocollis 2014)
In this case, police officers decided to administer naloxone on the basis of a medical rationale—whether the person was overdosed or not—instead of a penal one—whether the person possessed drugs or not. Although some might voice dissents on a moral basis—whether “junkies” deserved to receive medical assistance—they were not challenging the medical rationale. Thus, police officers carrying naloxone kits became more like medical practitioners with strong abstinent beliefs than their assigned roles of law enforcers.
Starting in 2014, legislators began resolving this role conflict for police officers. In 2016, for example, Maine passed a law allowing police officers to carry naloxone kits (Seelye 2016). The legislation process, however, was not smooth. Governor Paul LePage initially vetoed the bill, only to see his veto overturned by the Maine legislature. “Naloxone does not truly save lives; it merely extends them until the next overdose,” Governor LePage claimed (Seelye 2016). Interestingly, the governor did not use a penal rationale to argue against the bill: police officers should not behave like medical practitioners. Instead, he used the same medical rationale as naloxone advocators: opioid overdoses should be addressed with proper medical tools. He was merely contending with whether naloxone would be a suitable tool. From then on, (de)criminalization and medicalization efforts reached a juncture: curbing opioid overdose deaths should be prioritized through medications. Although penal social control continued to focus on holding doctors and big pharma accountable, medical social control managed to persuade penal personnel into delivering medical practices. The drug problem was thus constructed as an opioid (overdose) crisis, and the focus was on reducing the number of overdose deaths.
Discussion and Conclusion
Decriminalization of opioid use started before medicalization because of the convergence of fiscal constraints with the availability of opioid treatment options. On the budget end, policymakers actively sought alternatives as the punitive model was becoming increasingly unsustainable. They turned to OUD treatments after cost-benefit analyses. On the treatment end, medications for OUD treatments have been available since the 1970s. Yet the medicalization of opioid use did not happen until the 2000s, indicating the dominant role of (de)criminalization in constructing opioid use. Moreover, modes of penal social control continued to change independent of medicalization efforts entering the new century. Prosecutors adapted to their new roles after the drug reform by actively holding doctors and big pharma accountable. Ironically, in 2019, the Justice Department fined Reckitt Benckiser Group $1.4 billion for selling Suboxone, the most effective medication for treating OUD.
Medical professionals pushed for medicalization as the OxyContin abuse issue caught public attention. Early news frames on innocent rural opioid users played a role in this process. However, the part was far from decisive, as scrutiny of maintenance-based treatment options never faded. Opioid use was constantly associated with negative news frames such as danger, crime, and violence, especially in local newspapers and before 2014 (McGinty et al. 2016; Russell et al. 2019; Tunnell [2004] 2016; Whelan, Asbridge, and Haydt 2011). In other words, opioid use was not medicalized as medical professionals mainstreaming medical concepts. Instead, it was medicalized when medical social control extended to nonmedical professionals, especially law enforcement agencies. After 2014, when new modes of medical social control were established, media attention turned to nonpenal issues such as the availability of MATs and racial disparities. Other studies have also confirmed that in cases in which penal social control transformed while medical social control did not expand (e.g., methamphetamine use), negative frames of drug use were still prevailing while media attention never turned to treatment (Linnemann and Wall 2013; Peterson, Gubrium, and Fiddian-Green 2019). In the case of opioid use, however, a common moral ground was found: preventing opioid overdose deaths should be prioritized over preventing opioid abuse—a penal focus or addressing addiction suffering—a medical one. In this sense, studies focusing on how racial inequality might have contributed to the transformation of the opioid problem (Gollust and Miller 2020; Kim et al. 2020; Netherland and Hansen 2016; Om 2018) captured only one aspect of the process. They ignored the shifting power dynamics before 2014, which led to discussions of social inequality issues.
The changing media framing of opioid use from 1995 to 2016 depicted a story of how penal social control transformed while medical social control expanded, resulting in people who use opioids being managed under a new set of moral judgments. First, the public would tolerate occasional opioid uses, but opioid overdoses had to be reversed; secondly, nonmedical professionals could address opioid abuse medically, but only through restricted pathways; thirdly, people who use opioids were no longer dangerous devils, but they were still deviant individuals requiring regulatory efforts while doctors and big pharma became new targets to be blamed. Thus, this transformation of the penal-medical nexus was not just about a narrative change of medical concepts replacing punitive ones. It was more about a shift of networks of expertise (Eyal 2013). Historically bonded emerging ideas and practices regulating opioid use became institutionalized as new arrangements set new roles for doctors, police officers, prosecutors, activists, and the public. Consequently, the opioid crisis became a crisis of overdose and treatment.
This new knowledge regime extends medical social control through the hands of penal personnel. Police officers, an unexpected agent for medical practices, became de facto medical practitioners. On the other side, persistently negative news frames against maintenance-based treatment options prohibited medical professionals from proceeding with medicalization via the traditional way. For example, harm reduction activists, an expected ally of medical professionals, had a hard time promoting drug injection sites (the fight is still on as of 2023). Yet the new regime aims at accomplishing the same thing as the old one: managing people who use opioids and preventing them from causing other problems. With this goal untouched, it is hard to imagine how the drug problem might be handled differently, despite new media framing calling attention to treatment first.
These findings clarify myths reflective of (bio)medicalization and (de)criminalization perspectives. Specifically, this article contributes to the conceptual framework of medicalization by recentering medical social control. In addition, via institutional logics, this research has demonstrated that medicalization and decriminalization developed in parallel in constructing the opioid (overdose) crisis. However, these two institutional processes could have developed differently. Campbell and Lovell (2012) showed that medicalization occurred solely within criminalization in the early days of opioid treatment research, as nonaddictive analgesics were the primary research subjects in addiction therapeutics in the 1920s. Showalter (2019) revealed that medicalization has never happened in treating “psychopaths.” Instead, penal social control has always been the dominant control modality determining the meaning of the term. Future studies should examine whether this parallel development also happens in other cases involving changing media framing, e.g., the legalization of marijuana or the illegalization of abortion.
I examined the institutionalization of new penal-medical knowledge through the discursive frames of news articles. One limitation is that it only relied on one newspaper. As mentioned earlier, the New York Times readership might have affected the results, especially those regarding demographic variables. News frames generated by the New York Times, a national and city-focused newspaper, might have also differed from those of local and rural-based newspapers (Bagley and Bright 2020; Russell et al. 2019). A more systematic examination of newspapers, or other media sources, can better reflect how media portrayals interact with institutional logics, especially at the local level. To better understand how the two modes of social control shifted beyond the media, future research would also benefit by using other methods. Although this research revealed that decriminalization and medicalization happened independently during the period under investigation, other approaches could better explore how institutional logics might have intersected, especially after common ground was found. In other words, it would be fruitful to explore how after 2016, when certain response options were written into laws, key stakeholders in the opioid issue extended, defended, and reconstructed institutional boundaries in collaborative coalitions.
Research Data
sj-xlsx-1-srd-10.1177_23780231231186731 – Parallel Development: Medicalization and Decriminalization in the Changing Media Framing of the Opioid Overdose Crisis
sj-xlsx-1-srd-10.1177_23780231231186731 for Parallel Development: Medicalization and Decriminalization in the Changing Media Framing of the Opioid Overdose Crisis by Xinyan Wu in Socius
Research Data
sj-xlsx-2-srd-10.1177_23780231231186731 – Parallel Development: Medicalization and Decriminalization in the Changing Media Framing of the Opioid Overdose Crisis
sj-xlsx-2-srd-10.1177_23780231231186731 for Parallel Development: Medicalization and Decriminalization in the Changing Media Framing of the Opioid Overdose Crisis by Xinyan Wu in Socius
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.