
Abstract
The common emphasis on the superior pregnancy protection of long-acting reversible contraception (LARC) may result in medical providers’ pressuring women, especially those belonging to groups experiencing reproductive disciplining, to use LARC. The authors consider reports of having felt pressured to get or keep LARC in the 2021 Delaware and Maryland Survey of Women (1,058 current users and 1,788 ever users of LARC) and examine variation in these outcomes by women’s sociodemographic characteristics. The results reveal a high prevalence of both pressure to get (26 percent of current users) and keep (11 percent of ever users) LARC overall and among young (<25 years) mothers in particular. In addition, pressure to keep LARC is more common among economically disadvantaged, unmarried, and Hispanic women. These findings reveal that in the context of “LARC first” and enduring stratified reproduction, LARC pressure is common, particularly among groups that have long been targets of reproductive disciplining.
Keywords
For the past decades, U.S. contraceptive policy and practice has reflected the dominant view that pregnancy prevention is “naturally” a woman’s responsibility (Littlejohn 2021). Responsible parenthood starts with planned reproduction; unplanned pregnancy is evidence of a woman’s failure to fulfill her obligation to prevent pregnancy (Ruhl 2002). Thus, women should be using effective contraception unless they are actively planning pregnancy (or are otherwise “not at risk for pregnancy”) and reproductive activism and policy should guarantee access to contraception and abortion as a way to safeguard women’s right to not have a child. These views are clearly illustrated in the reproductive rights movement’s focus on protecting the legal right to abortion as established in Roe v. Wade in 1973 (Luna and Luker 2013), as well as public health policy’s stated goal to “Increase the proportion of women at risk for unintended pregnancy who use effective birth control” (DHHS n.d.).
Yet elevating “planned reproduction” as the ideal and use of the most effective contraception as the way to achieving it ignores the reality that this ideal and approach might not be desirable or feasible to all women at all times (Aiken et al. 2016). Moreover, the common focus on women’s right to not have a child risks overlooking how some groups have long experienced the systematic devaluation of their reproduction (Ross 2006) and thus fails to address the many barriers faced by some individuals when trying to exercise the right to have children and the right to parent any children one has in a safe and healthy environment (Luna and Luker 2013; Roberts 1997; Ross and Solinger 2017). Grounded in social justice frameworks, feminists of color coined the term reproductive justice (RJ) in 1994 to spotlight how unequal power relationships lead some groups to experience reproductive disciplining while others experience privileging. The movement aims to eliminate reproductive oppression through intersectional analysis and organizing that tends to the interlocking consequences of racism, sexism, classism, and other forms of oppression. After all, failing to address reproductive disciplining and privileging risks perpetuating reproductive oppression through policy and practice.
Numerous studies have documented the long history of pressuring or coercing women, particularly those belonging to marginalized groups, to use (certain types of) contraception, from the “unfit” being targeted for coerced sterilization (Hansen and King 2013) to women being channeled into using hormonal pills (or other prescription methods; Littlejohn 2021). In this study, we consider the latest chapter of this long history by considering how recent policy and practice surrounding long-acting reversible contraception (LARC)—intrauterine devices (IUDs) and implants—has worked to center the methods without sufficiently safeguarding women’s reproductive autonomy. Since 2000, when the levonorgestrel-releasing IUD was approved for medical use in the United States, these highly effective, “forgettable” methods have attracted widespread attention and enthusiasm. Given the long-standing public health goal of reducing unintended pregnancy (see above), U.S. medical organizations soon started advocating for “increasing use of contraceptive implants and intrauterine devices to reduce unintended pregnancy” (ACOG 2009). Citing the many historical as well as contemporary examples of oppressive use of contraception, researchers and activists warned that policies and practices that focus on LARC, rather than women, risk discounting women’s preferences and undermining their reproductive autonomy (Foster 2020; Gomez, Fuentes, and Allina 2014; Sister Song Women of Color Reproductive Justice Collective and National Women’s Health Network 2017). That is, by “promoting LARC,” such policies and practices open the door to the methods becoming a source of reproductive oppression, rather than a beneficial contraceptive technology that benefits women’s reproductive autonomy. This risk is heightened for groups traditionally considered “at high risk for unintended pregnancy” or whose reproduction tends to be devalued, including women who are young, unmarried, poor, and/or belong to a minoritized racial/ethnic group.
In this study, we discuss and consider if and how reproductive oppression can result from reproductive health policy and practice, as the latter continue to be shaped by unequal power relations. More specifically, we examine the extent to which unchecked LARC enthusiasm has led to the discounting of women’s contraceptive preferences and the undermining of their reproductive autonomy (i.e., to reproductive oppression). We focus on women’s experiences of feeling pressured by a medical provider to use or to continue to use LARC, as reported in the 2021 Delaware and Maryland Survey of Women (SoW). Recent qualitative research has documented how some medical providers direct or pressure women to use LARC and/or resist patients’ requests for early LARC removal (Gomez and Wapman 2017; Higgins, Kramer, and Ryder 2016; Manzer and Bell 2022; Sznajder, Carvajal, and Sufrin 2020). Yet the scope of such experiences remains insufficiently understood as population-representative surveys have only recently included questions on this issue. In addition, although these qualitative studies clearly point to poor (and) minority women being particularly likely to experiencing LARC pressure, how their risk compares with that of other women is insufficiently understood.
Background
“LARC First”
LARC as a category includes two contraceptive methods: implants and IUDs (although the injectable was initially often included in this category, that inclusion is no longer common). The implant is a flexible rod that is inserted subcutaneously in the upper arm and is approved for up to 3 years of use. The IUD is a T-shaped device that is inserted into the uterus and is approved for up to 3 to 10 years of use, depending on device type (Dethier, Qasba, and Kaneshiro 2022). Among reversible methods, LARC methods provide the highest level of protection against pregnancy, in large part because they are long-acting, “forgettable” methods, meaning that their use is not susceptible to user error (Grimes 2009). Given that an estimated 43 percent of unintended pregnancies in 2000 and 2001 were attributable to inconsistent or incorrect use (Frost, Darroch, and Remez 2008), this feature of LARC could enable women to better control whether and when to have a child, thus enhancing their reproductive autonomy (Eeckhaut, Rendall, and Zvavitch 2021). During the past two decades, LARC use increased more than sixfold, from 1.5 percent of reproductive-aged women in 2002 to 10.4 percent in 2017–2019 (Branum and Jones 2015; Daniels and Abma 2020).
By eliminating user error, LARC allows more reliable fertility control. Yet exercising that control now depends on a provider to insert and remove the implant or IUD (though self-removal is a safe option for most IUD users, this is often not communicated to patients; Manzer and Bell 2022). This provider dependency, which is heightened in the case of LARC because it includes device insertion and removal, creates the potential for the methods to become a source of reproductive oppression. This potential for contraception to both benefit and undermine reproductive autonomy, termed the “contraceptive paradox” (Gomez, Mann, and Torres 2018), has been unmistakably clear in recent LARC policy and practice. In fact, the difficulty of balancing the public health goal of reducing unintended pregnancy with individuals’ fundamental right to reproductive autonomy has been acknowledged as arising in the context of contraceptive counseling (Biggs et al. 2020; Mann, Chen, and Johnson 2022) and was openly debated in discussions of recent LARC program (Dehlendorf and Perritt 2022; Horvath, Bumpus, and Luchowski 2020).
Recent LARC policy and practice arose in a context of very low LARC use: U.S. LARC use was much lower than in nearly any other low-fertility country at the start of the twenty-first century (Buhling et al. 2014; Finer, Jerman, and Kavanaugh 2012). A leading reason was that IUDs had acquired a poor reputation after serious safety concerns surrounding the Dalkon Shield IUD in the early 1970s led to a decade of legal battles and media scrutiny, as well as gaps in IUD availability (Sonfield 2007). Because of this very low LARC use, U.S. policy makers, clinicians, and researchers initially set out to identify and eliminate common barriers to the methods (Eeckhaut, Sweeney, and Gipson 2014; Eisenberg, McNicholas, and Peipert 2013). These barriers included lack of availability, high up-front cost due to lack of insurance coverage of the device and/or its insertion, lack of provider training, and lack of knowledge or presence of misconceptions (Strasser et al. 2016). Several efforts greatly increased LARC access and likely enhanced reproductive autonomy, by either removing barriers to a wide range of methods (e.g., the Affordable Care Act’s contraceptive mandate; Bearak et al. 2016) or eliminating LARC-specific barriers (e.g., Medicaid immediate postpartum LARC reforms; Moniz et al. 2015; though see also Brian, Grzanka, and Mann 2020).
Other LARC efforts prioritized LARC over other methods. Such efforts may have worked to decrease reproductive autonomy by creating pressure on individuals to use LARC, rather than another or no method (Dehlendorf and Perritt 2022; Sister Song Women of Color Reproductive Justice Collective and National Women’s Health Network 2017). A key example is the emergence of a “LARC-first” approach to contraceptive counseling, also referred to as “tiered effectiveness” counseling, which came to largely replace options-based counseling (Brandi and Fuentes 2020; Higgins 2014). Instead of presenting a wide range of methods, a “LARC-first” approach presents contraceptive options in order of declining effectiveness, starting with LARC and permanent sterilization. By presenting LARC as the top choice among reversible methods, this directive approach assumes that all women rank effectiveness as the most salient contraceptive feature. Accordingly, it downplays other features that women might consider important, such as those related to side effects, sexual pleasure, and disease prevention. This decentering of patient preferences and autonomy opens the door to individuals being pressured into making the seemingly “most rational” choice of using LARC. Key professional organizations adopted “LARC-first” counseling recommendations during the early 2010s, including the American College of Obstetricians and Gynecologists (ACOG 2011), the American Academy of Pediatrics (Ott and Sucato 2014), and the Centers for Disease Control and Prevention (Gavin et al. 2014).
The widespread diffusion of a “LARC-first” approach to contraceptive counseling came in the wake of its use as part of the CHOICE Project in St. Louis, Missouri (Brandi and Fuentes 2020). CHOICE started in 2007 as a prospective cohort study aimed at examining the impacts of providing no-cost reversible contraception and, more specifically, of increased LARC use (Birgisson et al. 2015). The study adopted a “LARC-first” approach to contraceptive counseling, which was deemed a success when 75 percent of study participants choose LARC. In the years since, several localities and states have seen the implementation of large-scale LARC programs, including the Colorado Family Planning Initiative, the HER Salt Lake Contraceptive Initiative, the Delaware Contraceptive Access Now (DelCAN) initiative, and the Greater Rochester LARC Initiative. These programs have been met with both enthusiasm (Peipert et al. 2012; Ricketts, Klingler, and Schwalberg 2014) and criticism (Dehlendorf and Perritt 2022): enthusiasm for their role in increasing LARC access through the removal of barriers related to cost, education, and policy and criticism for their adoption of a “LARC-first” approach to contraceptive counseling and for their implicit or explicit focus on (increasing) LARC, on specific groups of women (e.g., teens, disadvantaged women), and/or on the achievement of certain social objectives through women’s contraceptive use (e.g., Medicaid cost savings).
We address concerns that “LARC-first” contraceptive counseling and contraceptive access initiatives could work to undermine women’s reproductive autonomy by increasing the extent that medical providers exert pressure to (continue to) use LARC. Drawing on SoW data, we investigate women’s perceived LARC pressure in one state, Delaware, that recently implemented a statewide LARC program (Choi et al. 2020) and a comparable state that did not (Maryland). Given a stated DelCAN objective to “reduce Medicaid costs for unintended pregnancies” (Choi et al. 2020), which may have led to the targeting of women relying on Medicaid insurance for (continued) LARC use, we compare experiences of LARC pressure for women with Medicaid versus other or no health insurance specifically, in addition to considering such experiences among women overall.
Reproductive Oppression and LARC
By prioritizing LARC, recent promotion efforts may have cleared the way for the methods to become a source of reproductive oppression. Individuals typically considered at high risk for unintended pregnancy and individuals whose reproduction tends to be devalued—categories that tend to overlap—are likely to be especially vulnerable, as they have been in previous efforts to increase use of (other methods of) contraception (e.g., Littlejohn 2021): the former because providers and policy makers may be particularly likely to promote LARC if they perceive an individual to be “at high risk for unintended pregnancy,” regardless of user preferences and the latter because any LARC effort that centers on the methods’ high efficacy may target individuals whose reproduction tends to be devalued.
To avoid these pitfalls, policy and practice needs to center individuals, instead of LARC, and explicitly recognize and address the unequal power relationships that have long been at the basis of reproductive oppression, both as it relates to contraception and more broadly. The long history of reproductive injustices has been extensively detailed (Jacobs 2014; Roberts 1997) and includes the denial of reproductive autonomy to enslaved people, forced and coerced sterilization for eugenic reasons, and the removal of Native American children from their families. Recent decades have witnessed more subtle policies and practices, including the 1977 Hyde Amendment that prohibits the use of federal funds to pay for (poor women’s) abortions, the disproportionate punishing of Black women for drug use during pregnancy, and the use of welfare family caps to limit the fertility of poor women (Cappello 2021; Roberts 1997; Washington 2006).
A particularly relevant example of contraception being used in oppressive ways is the targeted marketing of the Norplant implant to poor (young) Black women in the 1990s. Norplant was the first contraceptive implant approved in the United States, in 1990 (Strasser et al. 2016). Its high efficacy and convenience of use (not considering side effects) meant that the method was regarded as a major advance in contraceptive technology. Even though Norplant came at a relatively high cost—the device itself cost $365 and insertion and removal typically cost another $300 to $1,000 (Roberts 1997)—soon after it was brought to market, the group most likely to use Norplant were poor women (Malat 2000; Washington 2006). This outcome resulted from efforts to incentivize, pressure, and even mandate Norplant use for poor women, particularly for poor young Black women and mothers (Ross and Solinger 2017; Washington 2006). These efforts were motivated by the desire to save taxpayers’ money and often also by eugenic and racist ideology (Roberts 1997; Washington 2006). Once inserted—a “choice” typically paid for and even financially incentivized—poor women often found it difficult to have the implant removed, even in cases of adverse and persistent side effects. The cost of removal was typically not covered (even if insertion had been), and providers were often unwilling to remove the device early or may not have been trained or available to remove it at all or in a timely matter. As Roberts (1997) noted, “State funding structures and health professionals’ private biases have worked together to pressure poor women to keep the device in place” (p. 131). Thus, the device turned into a means of controlling poor women’s reproduction; an outcome that was aided by the method requiring provider intervention for both insertion and removal. The resulting backlash led Norplant to be withdrawn from market in 2002. A new implant was not approved until 2006 (Strasser et al. 2016).
The achievement of social objectives has long served as the impetus to regulate women’s, particularly poor (and) minority women’s, childbearing (Dehlendorf and Perritt 2022; Roberts 1997). Similar to Norplant in the 1990s, increasing LARC use has recently been proposed as a way to reducing not only early and unintended childbearing, but also welfare costs, poverty, inequality, and unmarried childbearing (Markell 2016; Sawhill 2014; Sheffield 2014). Although there is evidence that women’s ability to control their fertility positively affects their life chances (Lindo 2020), putting the responsibility of these social problems on the shoulders of women’s reproduction and their reproductive health behaviors draws attention away from the more fundamental sources of these problems (Foster 2020; Ross and Solinger 2017). It also puts women at risk for reproductive oppression, as it leads women’s bodies to be defined as risky: at risk for early and/or unintended childbearing and the associated negative outcomes (Foster 2020; Littlejohn 2021). Women can manage these risks by using highly effective contraception such as LARC. This framing of women’s bodies as in need of risk management and of LARC use as the most, or only rational tool to do so (Bertotti, Mann, and Miner 2021) has been argued to provide women “agency without choice” (Mann and Grzanka 2018).
Moreover, despite being seemingly neutral, the diagnosis of “at risk for unintended pregnancy” likely also has ideas of nonwhiteness and poverty attached to it, just as race and class tend to be embedded in medical diagnoses more generally (Metzl 2009). Social norms emphasize that motherhood requires financial readiness, a stable relationship, and being old enough, among other things (Briggs 2017; Geronimus 2003). Providers subscribing to such ideals about “normative readiness” may exclude poor, single, and young women from the universe of women who may reasonably be planning pregnancy (Stevens 2015), thereby defaulting them to being “at risk for unintended pregnancy” regardless of their actual fertility preferences. Thus the public health goal of reducing unintended pregnancy can act as a way for providers to impose socially normative expectations on their patients’ reproductive behavior, particularly their young, unmarried, poor, and minority patients’ reproductive behavior.
Prior Research on LARC Pressure
Prior research has extensively documented how contraception has been used in oppressive ways, and how it continues to be part of a system of “stratified reproduction,” that is, a system that privileges the reproduction of some groups while aiming to restrict the reproduction of others (Colen 1995). For example, class differences in contraceptive coverage versus infertility treatment have been argued to discourage childbearing among the poor but encourage it for the middle and upper classes (King and Meyer 1997). Providers have been shown more likely to advise poor (and) minority women to limit their childbearing (Downing, LaVeist, and Bullock 2007), more likely to steer them toward more long-acting and permanent forms of contraception (Dehlendorf et al. 2010; Downing et al. 2007), and more willing to perform female sterilization on them (Harrison and Cooke 1988).
There are clear indications that the long and ongoing history of contraception being used in oppressive ways, including an earlier type of LARC, Norplant, extends to current LARC practices. Although blatant coercive use of LARC is probably rare nowadays (though see ACLU Tennessee 2017 for a recent case of a judge offering a 30-day reduction in jail time to female inmates who get implants), a growing number of qualitative studies have detailed experiences of patients being pressured by providers to use, or to continue to use, LARC (Berndt and Bell 2021; Gomez and Wapman 2017; Higgins et al. 2016; Mann et al. 2019; Manzer and Bell 2022; Sznajder et al. 2020). Such LARC pressure can manifest in different forms and to varying degrees, and some individuals appear more vulnerable than others. Pressure to use LARC may manifest as providers emphasizing efficacy as a reason to choose LARC (e.g., “LARC first” counseling) or failing to discuss alternative contraceptive options as viable options, or at all. Studies on provider recommendations have shown that young, poor, minority women and mothers are particularly likely to be directed to LARC (Gomez and Wapman 2017; Manzer and Bell 2021), a disparity that providers explain by pointing to epidemiological data indicating that they are more likely to have an unintended pregnancy (Manzer and Bell 2021), a type of discrimination labeled “statistical discrimination” (Balsa, McGuire, and Meredith 2005). Providers have also been found to pressure patients to continue to use LARC. Studies on early LARC removal have shown that, in addition to sometimes refusing outright to remove LARC, providers use a variety of mechanisms to delay or prevent LARC removal (Manzer and Bell 2022), including minimizing side effects (Higgins et al. 2016) and imprinting on their patients that LARC is expensive and the decision for early removal should not be taken “lightly” (Hoggart, Newton, and Dickson 2013).
Taken together, these qualitative studies suggest that experiences of LARC pressure are common, particularly among groups typically considered at high risk for unintended pregnancy or whose reproduction tends to be devalued. Yet it is unclear exactly how prevalent they are, given that population-representative surveys have only recently included questions on this issue. Although we know of no representative survey that has asked questions on experiences of pressure to use LARC, the National Survey of Family Growth (NSFG) recently added a series of questions asking women who experienced difficulty discontinuing LARC whether provider discouragement was a primary reason. A recent analysis of these data (Poleon and Thompson 2022) indicated that among the 64 percent of female respondents who had intended to discontinue LARCs, 12 percent had had difficulty doing so. Of those, 6 percent indicated that provider discouragement was the primary reason for this difficulty, resulting in an estimated <1 percent of all LARC users who had intended to discontinue LARC reporting provider discouragement. However, this is likely an underestimate for (at least) two reasons. First, the use of filter questions means that people who experienced some pressure but got their LARC removed may not have reported “difficulty discontinuing LARC” (and thus were not asked about provider discouragement). Second, the filter questions also disregard the possibility of experiencing provider discouragement even when not actively seeking LARC removal. That is, qualitative studies have shown that some providers make it clear up-front that they will not consider requests for early LARC removal, or that they will consider such requests only if certain conditions have been fulfilled (Manzer and Bell 2022; Stevens 2018). For both these reasons, it is likely that this estimate is a lower bound of the extent to which women experience pressure to continue to use LARC.
In addition to uncertainty about the prevalence of LARC pressure, we know little about the extent to which such experiences have disparately affected groups typically considered at high risk for unintended pregnancy or whose reproduction tends to be devalued. These questions are vital because, as the RJ framework emphasizes, analyzing and understanding reproductive oppression is a necessary step toward its elimination. Additionally, from a reproductive health perspective, experiences of pressure to (continue to) use contraception have been linked to early discontinuation, reduced use of (prescription) contraception, and feelings of frustration and distrust toward providers (Amico et al. 2016; Berndt and Bell 2021; Gomez and Wapman 2017; Gomez et al. 2020; Higgins et al. 2016). Hence, understanding the extent to which experiences of LARC pressure are distributed unevenly is essential to help illuminate and address other reproductive health disparities.
Method
Data and Sample
We draw on data from the cross-sectional SoW, which is a population-representative household survey of reproductive behavior and attitudes of women 18 to 44 years old in Delaware and Maryland, conducted by NORC at the University of Chicago. SoW used a multimode approach, using Web- and mail-based questionnaires offered in English and Spanish. We draw on data from the most recent wave of the SoW, which was collected from February to October 2021 (Boudreaux, Eeckhaut, and Rendall 2022). This wave relied on similar methodology as the baseline SoW (NORC 2019) and had a response rate of 26.7 percent (27.8 percent in Delaware and 25.4 percent in Maryland), resulting in final sample sizes of 4,063 in Delaware and 3,078 in Maryland.
Given our focus on LARC, we exclude respondents who identified as transgender (n = 12) or who indicated having undergone tubal ligation or hysterectomy (n = 746). From this reduced sample of 6,882 women, we select two subsets. Our analysis of pressure to get LARC is restricted to women who stated that they are “currently using” an IUD or implant (n = 1,190). We omit those with missing information on the question regarding pressure to get LARC (n = 9) or on one of the other covariates (n = 123), resulting in a subsample of 1,058 women. Our analysis of pressure to keep LARC is restricted to women who indicated having ever used LARC (n = 2,112). We omit those with missing information on the questions regarding pressure to keep LARC (n = 33) or on one of the other covariates (n = 291), resulting in a subsample of 1,788 women.
Variables
Each of our two key dependent variables measures a type of LARC pressure exerted by a medical provider. Our first dependent variable measures pressure to get LARC and relies on a question, asked to women who indicated that they are “currently using” LARC: “If yes, how much pressure did you feel from a medical provider to have the IUD [implant] inserted?” Answer options were “none,” “a little,” “some,” “quite a bit,” and “a lot.” We categorized women who selected “none” as having felt no pressure, whereas all other response options were combined to indicate women who have felt pressure to get LARC. A more detailed categorization was not feasible, because of low numbers in the latter response categories. Our second dependent variable measures pressure to keep LARC and relies on a question asked to women who indicated having “ever used” LARC: “If yes, did you ever feel pressured by a medical provider to keep in the IUD [implant] that you were last using or are still using?” Women who selected “yes” were considered as having experienced pressure to keep LARC.
In follow-up analyses, we additionally consider women’s responses to a series of questions asking about the importance of certain contraceptive features (“How important are each of the following characteristics to you in deciding which birth control method to use?”). Specifically, given research showing that experiences of pressure to (continue to) use contraception can lead to feelings of distrust toward providers (see above), we consider as an additional dependent variable women’s reported level of importance of the contraceptive feature “I can get it without seeing a doctor or going to a clinic.” We distinguished between women who indicated that this contraceptive feature was “extremely” important rather than “somewhat” or “not at all” important.
In addition to these dependent variables, we focus on the following independent variables (see Table 1): women’s age, parity (number of “babies . . . born alive”), combined age AND parity, union status, race/ethnicity, educational attainment, current health insurance, and pretax household income. We additionally take account of nativity, LARC type, period of LARC initiation (analyses of pressure to get LARC only), and whether the woman is a current LARC user (analyses of pressure to keep LARC only). Finally, we consider differences by state of residence, as well as a potential effect of the statewide 2016–2020 DelCAN initiative by including an interaction term for state by period of LARC initiation for the analyses of pressure to get LARC only and an interaction term for state by current LARC user for the analyses of pressure to keep LARC only. Finally, to consider the possibility of the initiative having a disparate impact on women with public health insurance, we include an interaction term for state by current health insurance.
Percentage Distribution by Independent Variables, Percentages (95 Percent CIs) Reporting Experiences of Pressure to Get or Keep LARC in the Subsamples of Current and Ever Users of LARC, and Odds Ratios (95 Percent CIs) of Binary Logistic Models Regressing Each LARC Pressure Variable on These Independent Variables, Delaware and Maryland, 2021.
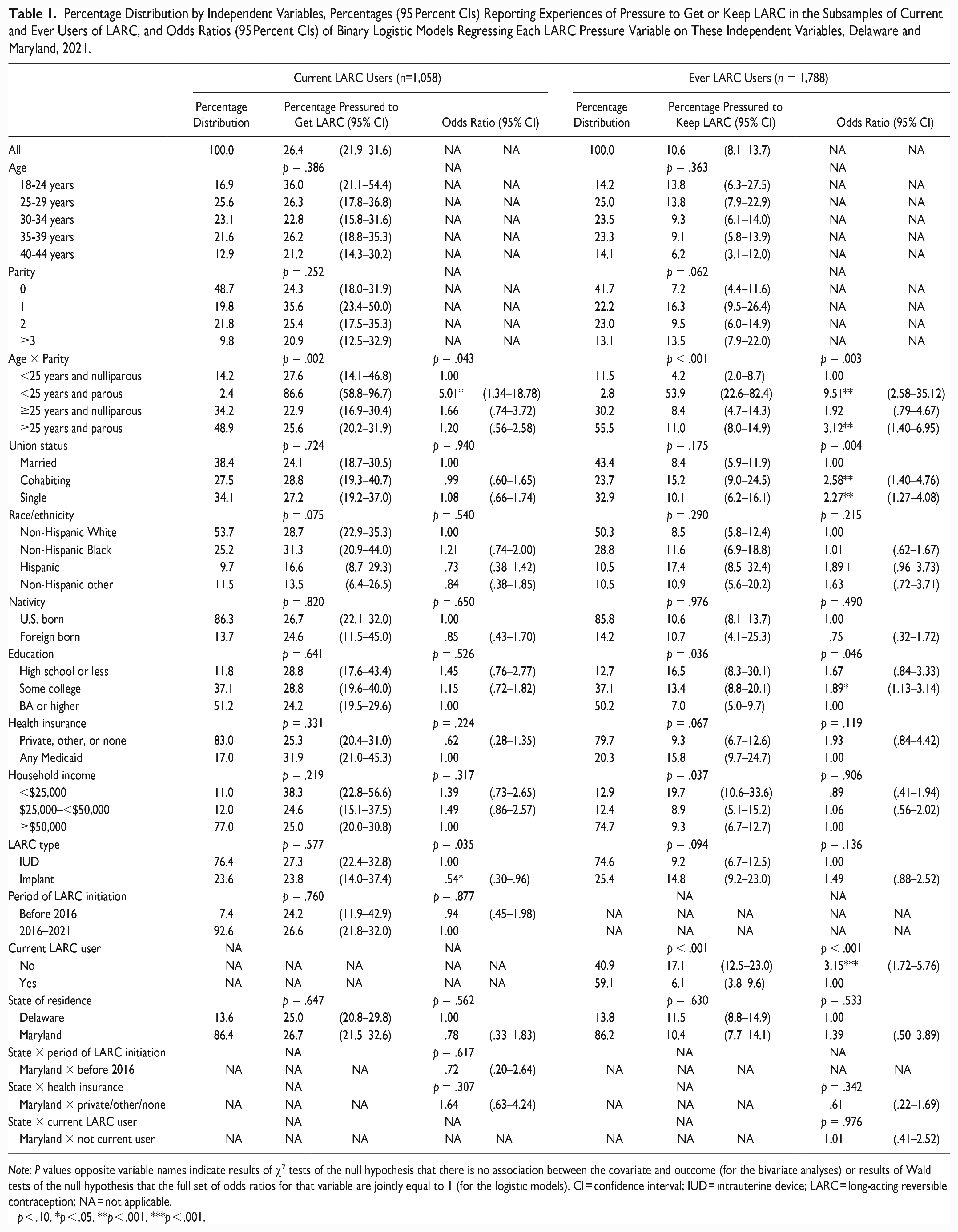
Note: P values opposite variable names indicate results of χ2 tests of the null hypothesis that there is no association between the covariate and outcome (for the bivariate analyses) or results of Wald tests of the null hypothesis that the full set of odds ratios for that variable are jointly equal to 1 (for the logistic models). CI = confidence interval; IUD = intrauterine device; LARC = long-acting reversible contraception; NA = not applicable.
p < .10. *p < .05. **p < .001. ***p < .001.
To better acknowledge that the interlocking consequences of racism, classism, and other forms of oppression may create an uneven burden of LARC pressure, we finally create a composite measure that captures whether, and how many, of the following four characteristics a woman has that may put her at heightened risk for experiencing LARC pressure: (1) is economically disadvantaged (has a pretax household income of <$25,000, high school or less level of education, or any current Medicaid health insurance), (2) belongs to a minoritized racial/ethnic group (is non-Hispanic Black, Hispanic, or non-Hispanic other), (3) is currently cohabiting, and (4) is a young mother (is younger than 25 and parous). This composite measure acknowledges that different forms of oppression may not shape experiences of LARC pressure in independent, additive ways that can be considered individually and while “controlling for” other forms of oppression.
Analytic Strategy
Parallel analyses were carried out for both key dependent variables, with each consisting of the same three steps. First, we relied on χ2 tests to examine the distribution of each dependent variable by our covariates. Next, binary logistic models regressed each dependent variable on the key independent variables, while adjusting for other covariates. A first model included women’s combined age and parity, union status, race/ethnicity, educational attainment, current health insurance, and pretax household income as key independent variables. A second model instead included the composite variable as the key independent variable. Both models additionally included nativity, LARC type, and the appropriate interaction terms for state by period of LARC initiation and state by current LARC user. The interaction term for state by current health insurance was included only in the first model. For the interaction terms, we used the margins and lincom commands to test for a difference in Delaware versus Maryland in the difference in predicted probabilities of LARC pressure by period of LARC initiation, by current LARC use, and by current health insurance. All analyses were adjusted for the SoW complex sampling design and weighted to adjust for the design of the SoW samples of the Delaware and Maryland populations (NORC 2019). For the logistic models, we normalized the weights for each state to have a mean of 1.
Results
Descriptive Analysis
Given the substantial overlap between current and ever LARC users (59 percent of ever users are current users), it is not surprising that their distributions are quite similar. In both groups, women who are married (about 38 percent and 43 percent, respectively) and nulliparous (about 49 percent and 42 percent, respectively) make up the largest group. The age distribution shows somewhat lower percentages in the youngest and oldest groups. About half of women are non-Hispanic White (54 percent and 50 percent, respectively), just over a quarter are non-Hispanic Black, and about 10 percent are in each of the Hispanic and non-Hispanic other groups. A majority are U.S. born (about 86 percent in both groups) and live in Maryland (about 86 percent in both groups). Most women had some college or a bachelor’s degree (≥87 percent in both groups), non-Medicaid health insurance (≥79 percent in both groups), and household incomes of ≥$50,000 (74+ percent in both groups). The majority (76 percent and 75 percent, respectively) were IUD versus implant users. Finally, most current users (93 percent) had initiated LARC use in 2016 or after.
More than one quarter (26 percent) of current users report having experienced pressure to get their LARC, and about 1 in 10 (11 percent) of ever LARC users report having experienced pressure to keep their last or current LARC. Thus pressure to get LARC appears more prevalent than pressure to keep LARC, though that difference is due partly to the latter being concentrated among ever users who discontinued LARC. That is, when limiting the sample to ever users who are no longer using LARC, the percentage having experienced pressure to keep LARC nearly doubles (17 percent).
Bivariate analyses confirm that experiences of pressure to get LARC are much more common (87 percent) among young women who have already given birth (i.e., those aged <25 years and parous) compared with young women who are nulliparous (28 percent) or older women who are either nulliparous (23 percent) or parous (26 percent). Contrary to expectations, no significant differences in pressure to get LARC are observed by union status, race/ethnicity, education, current health insurance, or household income. The latter likely explains why results for our composite measure (see Table 2), which considers how risk for LARC pressure compounds, indicate that experiences of pressure to get LARC are spread relatively evenly across women. That is, despite the extremely high risk among the small group of young parous women (2 percent of the sample), pressure to get LARC is relatively common among both women with zero characteristics (the minimum number) and those with three or more characteristics (the maximum number) that may put them at heightened risk (23 percent and 32 percent, respectively), and these differences are not statistically significant (p = .70). Finally, no significant differences in pressure to get LARC are observed by state of residence, period of LARC initiation, or any of the other covariates (see Table 1).
Results of Bivariate and Binary Logistic Analysis a Examining How Our Composite Measure, Which Measures the Number of Characteristics a Woman Has That May Put Her at Heightened Risk for LARC Pressure, Is Associated with Experiences of Pressure to Get or Keep LARC in the Subsamples of Current Users and Ever Users of LARC, Delaware and Maryland, 2021.

Note: P values indicate results of χ2 tests of the null hypothesis that there is no association between the composite measure and the outcome (for the bivariate analyses) or results of Wald tests of the null hypothesis that the full set of odds ratios for the composite measure are jointly equal to one (for the logistic models). CI = confidence interval; LARC = long-acting reversible contraception.
The binary logistic models include the following additional covariates for the analyses for pressure to get LARC: LARC type (intrauterine device or implant), state of residence, period of insertion (before 2016 or 2016–2021), and the interaction term for state of residence × period of insertion. For the analyses for pressure to keep LARC, the following additional covariates are included: LARC type (intrauterine device or implant), current LARC user (yes or no), state of residence (Delaware or Maryland), and the interaction term for state of residence × current LARC user.
The composite measure indicates how many of the following four characteristics a woman has: (1) is economically disadvantaged (has a pretax household income of <$25,000, high school or less, or any current Medicaid health insurance), (2) belongs to a minoritized racial/ethnic group (is non-Hispanic Black, Hispanic, or non-Hispanic other), (3) is currently cohabiting, and (4) is a young mother (is younger than 25 and parous).
p < .100. *p < .050. **p < .010. ***p < .001.
Although having experienced pressure to keep LARC is less common overall (see above), it too is much more common among young parous women (54 percent) compared with young nulliparous women (4 percent) or older women who are either nulliparous (8 percent) or parous (11 percent). Pressure to keep LARC additionally shows a positive association with all three measures of economic disadvantage; it is more common among ever users with high school or less or some college (17 percent and 13 percent, respectively, vs. 7 percent among those with bachelor’s degrees), among those in the lowest income category (20 percent vs. 9 percent among both those with incomes of $25,000 to <$50,000 and those with incomes ≥$50,000), and among those with any Medicaid (16 percent vs. 9 percent among those with private, other, or no insurance), though the latter association is only marginally significant (p = .07). Pressure to keep LARC also appears more common among Hispanic (17 percent vs. 9 percent among non-Hispanic White women) and cohabiting (15 percent vs. 8 percent among married women) women, though these differences by union status and race/ethnicity are not statistically significant (p > .10). Nevertheless, in line with these bivariate patterns by age/parity and economic disadvantage (and, to a lesser extent, race/ethnicity and union status), bivariate results for the composite measure (see Table 2) indicate that the risk for pressure to keep LARC is distributed much more unevenly than the risk for pressure to get LARC; it varies from a low of 5 percent for women with zero characteristics that may put them at heightened risk, doubling to 10 to 11 percent for women with one or two such characteristics, and then increasing to 28 percent, a near sixfold increase, for women with three or more such characteristics (the maximum number).
Table 1 also confirms that pressure to keep LARC is more common among ever LARC users who are not currently using LARC (17 percent vs. 6 percent among current users). And though the difference is only marginally significant (p = .09), it is more common among those who use(d) the implant versus an IUD (15 percent vs. 9 percent). In supplemental analyses that include only ever users who are not current users (n = 721, results not shown), no differences remain in pressure to keep LARC by method type, suggesting that the observed differences among all ever users are driven by ever users of the implant being more likely than ever users of the IUD to have discontinued their LARC by the time of the survey. Finally, we observe no significant differences in pressure to keep LARC by state of residence or nativity.
Multivariate Models
In the first set of logistic models, we examine associations between LARC pressure and each of our key independent variables, focusing on their independent effects. These models again confirm that young parous women are much more likely than young nulliparous women to experience both pressure to get and keep LARC (odds ratios [ORs] of 5.0 and 9.5, respectively). Older parous women are also somewhat more likely to experience pressure to keep LARC (OR = 3.1) than are young nulliparous women. Results for the other key covariates indicate that pressure to keep, though not pressure to get, LARC is more common among cohabiting (OR = 2.6) and single (OR = 2.3) compared with married women, more common among women with some college (OR = 1.9) compared with those with a bachelor’s degree or more, and more common among Hispanic (OR = 1.9) compared with non-Hispanic White women, though this latter difference is only marginally significant (p = .07). These patterns for pressure to keep and, to a lesser extent, pressure to get LARC are in line with our expectation that the risk for LARC pressure disparately affects women typically considered at high risk for unintended pregnancy or whose reproduction tends to be devalued, including young, unmarried, poor, and minority women.
Results of the second set of binary logistic models (Table 2) additionally confirm that the risk for LARC pressure, particularly of pressure to keep LARC, compounds. Whereas the risk for pressure to get LARC shows only a marginally significant association (p = .08) with the number of characteristics a woman has that may put her at heightened risk, the risk for pressure to keep LARC is heavily concentrated among women who are at the intersection of multiple forms of oppression. Compared with a woman who has zero characteristics that may put her at heightened risk, women who have two such characteristics face more than double the risk for experiencing pressure to keep LARC (OR = 2.2), and women who have three or four such characteristics (the maximum number) face a near fivefold increase in risk (OR = 4.9).
Finally, the logistic models again confirm that ever users who are not currently using LARC (OR = 3.2) are more likely to report experiences of pressure to keep LARC. For pressure to get LARC, the only additional association is with method type, with implant versus IUD users being less likely to experience pressure to get LARC (OR = 0.5). No statistically significant association with either pressure to get or keep LARC is found for either state of residence, or any of the interaction terms that consider a potential effect of the statewide 2016–2020 DelCAN initiative.
Does LARC Pressure Lead to Provider Distrust?
To explore linkage of experiences of LARC pressure with distrust toward providers (see above), we next analyze whether those who report having experienced LARC pressure are more likely to state at survey interview that “I can get it without seeing a doctor or going to a clinic” is an “extremely” important characteristic in deciding which birth control method to use.
A sizable share of current and ever users of LARC (15 percent and 21 percent, respectively) report that “I can get it without seeing a doctor or going to a clinic” is an “extremely” important characteristic in deciding which birth control method to use (Table 3). Current LARC users who experienced pressure to get LARC are somewhat more likely than those who did not experience such pressure to indicate that this characteristic is “extremely” important (20 percent vs. 14 percent, respectively), though this difference is not statistically significant (p = .29). Ever LARC users who experienced pressure to keep LARC, however, are more than twice as likely than those who did not experience such pressure to report this feature as “extremely” important (42 percent vs. 18 percent). This supports the hypothesis that experiences of LARC pressure, particularly pressure to keep LARC, may result in a preference to avoid methods that require provider interaction, including LARC which requires a prescription and is provider controlled.
Percentage (95 Percent Confidence Interval) Reporting “I Can Get It without Seeing a Doctor or Going to a Clinic” as an “Extremely” Important Characteristic in Deciding Which Birth Control Method to Use, by Whether or Not They Reported Experiences of Pressure to Get (Current LARC Users) or Keep (Ever LARC Users) LARC.
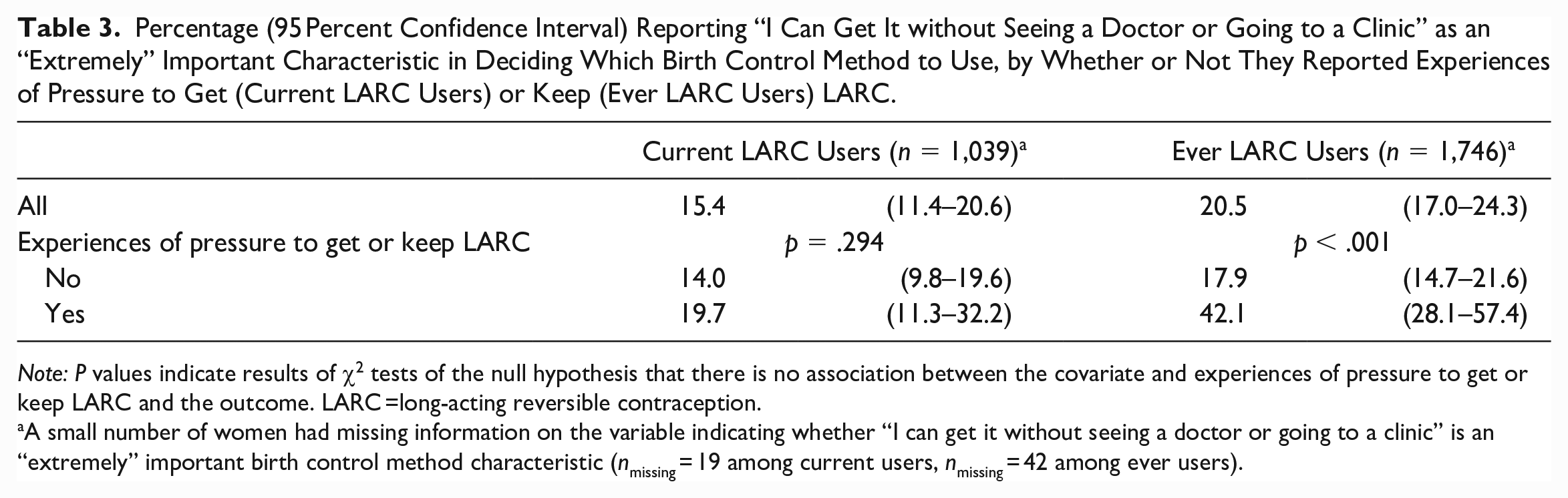
Note: P values indicate results of χ2 tests of the null hypothesis that there is no association between the covariate and experiences of pressure to get or keep LARC and the outcome. LARC =long-acting reversible contraception.
A small number of women had missing information on the variable indicating whether “I can get it without seeing a doctor or going to a clinic” is an “extremely” important birth control method characteristic (nmissing = 19 among current users, nmissing = 42 among ever users).
Conclusion and Discussion
Two main findings emerged from this study. First, experiences of pressure to get and keep LARC are common among current and ever LARC users, respectively. Prior research has documented experiences of LARC pressure, but these studies have been overwhelmingly qualitative and provide limited clarity on the prevalence of such experiences. The current study showed that 26 percent of current LARC users have felt pressured to get their current LARC; consistent with a context of recent LARC policy and practice in which medical organizations have advocated for “increasing use of contraceptive implants and intrauterine devices to reduce unintended pregnancy” (ACOG 2009) and have recommended a “LARC-first” approach to contraceptive counseling (ACOG 2011; Gavin et al. 2014; Ott and Sucato 2014). Against the backdrop of decades of public health messaging on the need to reduce unintended pregnancy (Klerman 2000), these guidelines and recommendations likely resulted in some providers being eager to recommend LARC, and this was perceived by their patients.
Pressure to keep LARC was reported by 11 percent of ever LARC users and 17 percent of ever users who were not current users (i.e., who discontinued LARC). This is a much higher percentage than that based on NSFG analyses by Poleon and Thompson (2022), which suggested that <1 percent of users who had intended to discontinue LARC experienced provider discouragement (see “Prior Research on LARC Pressure”). However, the use of filter questions in their data source (the NSFG) means that only women who had intended to discontinue LARC and had reported “difficulty discontinuing LARC” were asked about experiences of provider discouragement. Moreover, the pertinent question asked about the primary reason for women’s difficulty discontinuing LARC, rather than about experiences of LARC pressure more broadly. These two features likely explain why the SoW data, in contrast to the NSFG data, show pressure to keep LARC to be a common experience, reported by 11 percent of ever users. This finding, together with the high share of current users reporting experiences of pressure to get LARC, is cause for concern as it bears out warnings about the risk of policies and practices that focus on LARC, rather than women, leading to the discounting of women’s preferences and the undermining of their reproductive autonomy (Foster 2020; Gomez et al. 2014; Sister Song Women of Color Reproductive Justice Collective and National Women’s Health Network 2017). Although the pendulum appears to be swinging back in favor of a more cautious approach to LARC policy and practice in recent years (see, e.g., Horvath et al. 2020), the more fundamental question might be whether it is possible for reproductive health policy to pursue social or public health objectives without compromising reproductive autonomy, given the inherent tension between the two (see, e.g., Bertotti et al. 2021). That is, although enhancing reproductive autonomy is likely to lead to positive social and public health outcomes (Lindo 2020), making such outcomes the target of contraceptive policy carries an inherent risk for compromising individuals’ reproductive autonomy.
Our second key finding is that experiences of LARC pressure, particularly pressure to keep LARC, are concentrated among groups typically considered at high risk for unintended pregnancy or whose reproduction tends to be devalued, including young mothers, economically disadvantaged women, unmarried women, and Hispanic women. Results showed particularly high levels of LARC pressure for young (<25 years old) mothers, with 87 percent reporting experiences of pressure to get their current LARC and 54 percent reporting experiences of pressure to keep their current or last LARC. These results are consistent with qualitative results showing that some doctors feel a need “to ‘responsibilize’ younger patients via LARC” (Mann et al. 2022:69; see also Manzer and Bell 2021) and with studies finding young women, particularly young mothers, to be more likely to receive provider-driven contraceptive counseling and directive recommendations (Dehlendorf et al. 2014; Gomez and Wapman 2017), to which some agree, only to discontinue the recommended method shortly after (Gomez and Wapman 2017).
Results also showed the expected associations between pressure to keep, though not get, LARC and economic disadvantage, union status, and Hispanic ethnicity. These results are in line with prior qualitative findings on early LARC removal suggesting that marginalized women are especially likely to encounter resistance to LARC removal (Higgins et al. 2016; Manzer and Bell 2022). They also confirm that some women are especially vulnerable to experiencing reproductive disciplining because of racism, classism, and other forms of oppression. Moreover, our composite measure supported the RJ tenet that these forms of oppression interlock to produce a particularly high risk for LARC pressure for women at the intersection of multiple groups typically considered at high risk for unintended pregnancy or whose reproduction tends to be devalued. This again illustrates the dangers of policies that propose LARC as a way to reduce welfare costs, poverty, and/or inequality (see above), as such proposals implicitly or explicitly identify young, poor, unmarried, and minority women’s fertility as an important source of these social problems. This leads to the logical conclusion that reducing their fertility is conducive or even necessary to making progress on these issues, a conclusion that puts these women at risk for reproductive oppression (Foster 2020; Littlejohn 2021). Although pressure to get LARC appeared to be more evenly spread across women, future research should consider if this finding might be due to differential selection into LARC use across different subgroups of women.
Two additional findings are worth discussing. First, we found no evidence of a heightened risk for LARC pressure in Delaware, which recently implemented a statewide LARC program, versus Maryland. This conclusion holds both when considering all women and when looking specifically at women with Medicaid insurance, with the latter potentially being targeted because of DelCAN’s stated goal of reducing Medicaid costs, among other things. Large-scale LARC programs have been criticized for potentially undermining, rather than enhancing, women’s reproductive autonomy. That we found no meaningful differences could be due to “LARC-first” contraceptive counseling having become the standard across the country (Brandi and Fuentes 2020; Higgins 2014), and not just in Delaware, after several key professional organizations adopted “LARC-first” counseling recommendations during the early 2010s (e.g., ACOG 2011). Moreover, decades of public health messaging on the need to reduce unintended pregnancy rates in the United States (Klerman 2000) could explain why experiences and patterns of LARC pressure were no different in Delaware but instead appeared to be a symptom of the more widespread mindset governing LARC policy and practice in the (late) 2010s.
A second additional finding is that results were in line with the hypothesis that experiences of LARC pressure, particularly pressure to keep LARC, may result in a preference to avoid methods that require provider interaction, as evidenced by a higher likelihood of stating that “I can get it without seeing a doctor or going to a clinic” is an “extremely” important characteristic in deciding which birth control method to use. This finding adds to a growing literature (e.g., Berndt and Bell 2021; Gomez and Wapman 2017; Gomez et al. 2020; Higgins et al. 2016) showing how experiences of pressure to (continue to) use contraception can negatively affect subsequent reproductive health outcomes.
A few strengths and limitations should be noted regarding the interpretation of results. First, we rely on data on reproductive-aged women in Delaware and Maryland to provide the first population-based estimates of the prevalence and patterning of both pressure to get and keep LARC. One limitation is the difference in question wording and answer options of the two pressure questions, with the question on pressure to get LARC asking how much pressure was experienced—“none,” “a little,” “some,” “quite a bit,” and “a lot”—versus the question on pressure to keep LARC asking whether the woman ever felt pressured—“yes” or “no.” It is possible that these differences account for some of the difference in the prevalence of reported pressure to get versus keep LARC, as an experience of “a little” pressure to get LARC might have gone unreported if the question had instead asked whether the woman had felt pressured. This possibility is also supported by research showing that providers still retain significant authority (Stivers and McCabe 2021), which might lead to reluctance to report less blatant experiences of pressure (unless asked specifically). Second, we limited our analyses of pressure to get LARC to current users, as their LARC use ascertains that they were both LARC eligible and visited a provider who offered LARC. Future research should additionally consider this outcome among all LARC-eligible women receiving contraceptive counseling, including LARC nonusers, as this would further advance understanding of its prevalence. Third, the SoW had an overall response rate of 27 percent, which is lower than government-funded reproductive health surveys such as the NSFG (63 percent in 2017–2019; DHHS 2020) but similar to other non-government-funded representative reproductive health surveys such as the Fog Zone (20 percent; Kaye, Suellentrop, and Sloup 2009) and the National Survey of Fertility Barriers (wave 1: 37 percent; Johnson et al. 2009). Moreover, all analyses were weighted to adjust for differences in the distributions of important demographic variables between the SoW sample and the Delaware and Maryland populations.
Our analyses advance understanding of how recent LARC “enthusiasm” has led women to experience LARC pressure, thus undermining their reproductive autonomy. Some groups were found to be particularly vulnerable, most importantly young mothers but also economically disadvantaged, unmarried, and Hispanic women. By adding to the extensive body of work detailing the long history of reproductive injustice in the United States, these findings spotlight the continued need to prevent, reveal, and reduce the reproductive disciplining experienced by many, but particularly by those facing racism, classism, and other forms of oppression. It also adds to a growing body of research showing the dangers of prioritizing LARC (or any other contraceptive method), and of using reproductive health policy to achieve social objectives, as doing so is inherently at odds with safeguarding reproductive autonomy. To avoid these pitfalls, policy and practice need to center individuals, and explicitly recognize and address unequal power relationships that have long been at the basis of reproductive oppression and continue to shape reproductive health policy and practice. This will likely be of particular importance in light of the recent overturning of Roe v. Wade and the continuing attacks on abortion and contraception access, as this context may reinforce the centering of the right to not have a child at the expense of the right to have children and the right to parent any children one has in a safe and healthy environment, as well as of the impacts of reproductive disciplining and privileging more broadly.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (population research infrastructure grant P2C-HD041041) and by a research grant from an anonymous private philanthropic foundation.