
Abstract
Shifting cultural norms transform the uses and meanings of medical practices, and, in turn, medical practices have the capacity to alter social relations. In this article, I use hysterectomy as a case for understanding how reproductive health practices are constrained by and contribute to notions of gender, race, and stratified reproduction. Hysterectomy is regularly performed yet understudied and has been transformed by both technological advances and shifting norms in gender and reproduction. I draw on 100 in-depth interviews with individuals who had, want, or are considering hysterectomy to treat chronic reproductive health conditions or as gender-affirming care for trans and gender-nonbinary (TGNB) individuals. These comparative groups shed insight across three gender groups (cis women, trans men, nonbinary) as well as across race. Findings show divergent patient–provider interactions ranging from physician support to provider coercion to gatekeeping. Similarly, the data reveal that hysterectomy evokes a wide range of reactions—from delight to neutrality to grief. These distinct reactions and interactions map on to gender, race, and ethnicity, revealing persistent reproductive stratification by social positionality. Bringing together feminist science and technology studies with intersectional theories of the body and reproductive justice, I show how stratified reproduction operates when gender identities vary and introduce the concept of opting into infertility.
Gendered notions of reproduction and the family have been remade in recent decades by new and emerging technologies in tandem with changing sociocultural norms. From surrogate pregnancy (Markens 2007), egg and sperm donation (Almeling 2011), to in vitro fertilization and egg freezing (Bell 2009; Brown and Patrick 2018), biomedicalization (Clarke et al. 2003) has expanded the very meanings of reproduction and kinship. The family has also been remade by broader sociocultural and gendered forces, as a growing proportion of Americans identify as “childfree by choice” (Gillespie 2003) and forge queer and trans families (Mamo 2007). As the meanings of family, reproduction, and gender shift, so do the meanings associated with reproductive technologies—not only those who help one “overcome” infertility, but also those who are associated with “opting out of” fertility, such as abortion or sterilization procedures. In turn, these reproductive practices have the capacity to make and remake gender relations.
To continue to explore the ways medical practices are made by and in turn remake the social world, I focus on hysterectomy as a critical and understudied case. Hysterectomy is the most common gynecological surgery worldwide (Hammer et al. 2015) but has received very little sociological attention. In fact, one of three American women will have a hysterectomy by the age of 60, yet only one sociologist has explicitly studied hysterectomy (see Elson 2004). Although hysterectomy was once viewed as a final plea for terminally ill women—with a mortality rate of 70 percent as late as the 1880s (Sutton 1997), modern hysterectomies are nearly unrecognizable from its early forms, due particularly to its technological refinement in the late 1980s as a laparoscopic, often outpatient procedure. These technoscientific advancements have helped shift the use and meaning of a hysterectomy from a highly dangerous procedure for terminally ill women to a primarily “elective” procedure to allay chronic reproductive illness and pain—including endometriosis, adenomyosis, and fibroids—as well as into an essential element of transgender health care (Nolan, Kuhner, and Dy 2019). Despite the development of this practice, hysterectomy continues to be discursively framed in literature and dominant discourse as an “unnecessary” procedure forced upon women by “hyster-happy” practitioners (Angier 2000; Edozien 2005) both now and throughout history (Maines 2001; Porter 1998; Tasca et al. 2012).
At the same time, all reproductive practices must be contextualized within a broader set of gender and racial politics that aggregate to produce stratified reproduction (Colen 1986; Ginsburg and Rapp 1991; Ginsburg et al. 1995; Shreffler et al. 2015). Amid this system of reproductive politics, one’s social positionality shapes the degree of reproductive autonomy available, especially along racial lines. Hysterectomy in particular was used as a sterilization procedure wielded against Black, Indigenous, and women of color in the United States as part of state-sponsored eugenics initiatives that peaked in the 1960s and 1970s (Lawrence 2000; Novak et al. 2018). Therefore, I approach hysterectomy from a reproductive justice perspective, which expands beyond the right to not have a child, as in the case of birth control and abortion, to also emphasize the right to have a child and to parent children in safe and sustainable environments (Ross and Solinger 2017). In addition, I expand on this literature by examining how stratified reproduction operates when gender identity varies through an analysis that includes cis women, transgender men, and nonbinary and gender-expansive individuals.
Given hysterectomy’s complicated histories and the modern refinement of the technology itself, what are the contemporary meanings of and pathways to this procedure across social positionality? I draw on a diverse set of 100 interviews across two gendered case studies: hysterectomy as a treatment for chronic reproductive illness or as a part of transgender health care. This design allows for comparisons not only across gender identity but also within gender categories by race and by reason for a procedure. As I demonstrate, contemporary hysterectomy narratives reveal the continued salience of stratified reproduction—the mechanisms of which are complicated by gender identity. Whereas racialized ideologies in medicine construe some women’s bodies as “pre-pregnant,” (Waggoner 2017) and others as hyperfertile (Roberts 1999), trans men and nonbinary (TGNB) individuals are often viewed as detached from fertility and reproduction (Lampe, Carter, and Sumerau 2019), which leads to increased access to hysterectomy while simultaneously contributing to the devaluation of TGNB reproduction and families.
While reasons for a hysterectomy vary, all patients have subsequent infertility or sterility in common—whether because it was performed alongside a bilateral oophorectomy (removal of both ovaries) or due to the subsequent need for various reproductive technologies to produce a pregnancy. About a third of hysterectomies in the United States are performed alongside a bilateral oophorectomy (Doll, Dusetzina, and Robinson 2016), which leads to surgical menopause, and this type of hysterectomy is disproportionate among Black and Latinx women (Mahal et al. 2017). However, counter to the numerous studies demonstrating the sorrows of infertility and sterilization (e.g., Bell 2009; Greil et al. 2011) and of hysterectomy specifically (Elson 2004), my findings indicate a range of reactions to one’s hysterectomy: from delight to grief to neutrality, as well as a wide range in physician–patient interactions regarding hysterectomy—from physician support to provider coercion to gatekeeping. Yet the ability to feel delight or neutrality rather than grief is stratified, revealing important insight on how gender and race inequality shapes individual experiences with medicine, with reproduction, and even with one’s own body. This study, therefore, aims to answer the following question: Given that the composition of the uterus remains unchanged—a hollow, fist-sized, pear-shaped organ that lives in the pelvis—what explains these different experiences of hysterectomy?
The Construction of Gendered, Raced Bodies in Medicine
Hegemonic gender ideologies influence our interpretation of medical practices and scientific technologies. Simultaneously, the way technologies are used and discursively framed can in turn (re)produce notions of gender and bodies (Fausto-Sterling 2000; Jones 2015). This is particularly the case for reproductive technoscience and gynecology, as elements of “women’s reproduction” often serve as symbolic repositories through which to express anxieties about gender and sexuality (Armstrong 2003; Markens 2007). From pelvic examinations (Kapsalis 1997), in vitro fertilization (Mamo 2007), and intrauterine devices (Mann et al. 2020) to surrogate pregnancy (Hovav 2019, 2020; Markens 2007), gender both shapes and is shaped by medical technology and practices. Medicine is also able to “give gender by giving sex” in the case of intersex and trans medicine by transforming bodies to align with culturally informed gendered meanings (Davis, Dewey, and Murphy 2016; Meadow 2018). In this way, bodies cannot be understood outside of gendered and medicalized social processes because the biology of bodies itself is as socially constructed as gender (Butler 2011).
Medical technologies are also made and remade by race. Scholars have consistently demonstrated the existence of stratified reproduction—a term that captures how reproduction is structured across demographic, social, and cultural boundaries (Colen 1986; Ginsburg and Rapp 1991; Luna and Luker 2013). Within this stratification, people are encouraged to “choose” different reproductive practices for divergent social outcomes based on cultural assumptions and obstetric racism (Davis 2019). For instance, in the United States, white, affluent women are encouraged toward new reproductive technologies—including egg freezing and in vitro fertilization—whereas women of color are disproportionately persuaded toward long-acting reversible contraceptives (LARC) and sterilization procedures (Gomez, Fuentes, and Allina 2014). In fact, sterilization is overrepresented in racial and ethnic minority groups (Shreffler et al. 2015), with race differences persisting when controlling for socioeconomic status, age, marital status, parity, and insurance status (Volscho 2010). These different uses of reproductive technologies are shaped by racialized notions of reproduction—for example, of white women as needing their fertility protected, while nonwhite and poor women are cast as hyperfertile and hypersexual. At the same time, these different uses also perpetuate notions of racialized gender and reproduction both within and outside of health care settings (Bridges 2011). It is, therefore, incomplete to examine the gendered nature of a technology without also examining the racialization embedded within, as various reproductive justice scholars have demonstrated (Combahee River Collective 1986; Luna and Luker 2013; Roberts 1999; Ross and Solinger 2017).
More recently, social scientists are beginning to examine the way technologies intersect with LGBTQIA (lesbian, gay, bisexual, transgender, queer, [questioning], intersex, asexual, and [agender]) identities (Mamo 2007). For instance, TGNB individuals have long “queered” the use of various technologies performed on cis women—particularly mastectomies and hysterectomies—to achieve their own distinct gendered and embodied goals (shuster 2021). Trans health scholars have written on the theoretical complexities of transgender medicalization: at once granting access to gender-affirming treatments while reinforcing “transnormative” notions of how to be trans (Johnson 2016; Vipond 2015). In this way, medical technologies are able to both construct and regulate trans identities and bodies. In their comparison of intersex and trans surgeries, Davis and colleagues (2016) similarly argue that providers draw upon essentialist notions of sex and gender when providing care to individuals whose bodies deviate from normative ideas. Incorporating TGNB experiences in a study of reproductive health care provides a more holistic view of the interplay among gender, embodiment, and medicine, as it remains unclear how stratified reproduction operates across variations in gender identities and across cis and trans experiences.
Social Construction of Medicine VIA Gender
The gendered symbolism attached to a medical procedure also shapes the meaning, experience, and provision of medicine. Symbolic meanings can be shaped by the reason for a procedure, which in turn impacts the perceived embodied experience. For instance, the process of in vitro fertilization elicits divergent experiences of “intensity” of the medical process if undertaken to become pregnant or as part of egg donation (Almeling and Willey 2017). In terms of positionality, Littlejohn (2013) showed how gender and class influence not only how and if an individual will use birth control, but also how they interpret the physical experience. Cultural gender expectations for U.S. women to be thin, in addition to cultural stigma of women’s “wild” emotions, led women to discontinue birth control due to weight gain and mood swings despite prevailing concerns about unintended pregnancy, in a way that departs from women in Cambodia and Egypt (Hassan et al. 1999; Sadana and Snow 1999). Similarly, the physical experience of menopause is perceived differently in the United States and Japan, with women reporting different symptoms, partly due to different national medical histories and cultural beliefs about gender and aging (Lock and Kaufert 2001). Cross-cultural findings such as these underscore the presence of what Lock and Kaufert (2001) call “local biologies” or bodily experiences produced by a “dialectic” between culture and biology.
Cultural gender, race, and class stereotypes also impact various facets of how reproductive health care is provided. From determining the “legitimacy” of an abortion (Kimport, Weitz and Freedman 2016) to the validity of early removal of one’s intrauterine device (IUD) (Manzer and Bell 2022), cultural ideologies influence the care patients receive, and thus individuals’ ability to make decisions about their health care and their own bodies. As another example, Hovav (2020) found that cesarean sections are excessively performed on Mexican surrogates based not on medical indication, but on cultural notions of gender, kinship, and fetal bonding—more specifically, to prevent excessive fetal bonding between a surrogate and the newborn. Last, researchers have examined what Waggoner (2017) terms the zero trimester, in which “women’s bodies” are treated as inevitably pre-pregnant starting in puberty, in a way that shapes the care and medical advice women receive.
An analysis of hysterectomy builds on this growing body of work on how culture, gender, and race impact the experience and provision of health care while extending it in key ways. I problematize the notion of “choice” in reproductive health care by showing how an elective hysterectomy lies on a continuum between choice and constraint and is shaped by both gendered and racialized processes in tandem. Moreover, I incorporate TGNB experiences to address the disproportionate focus within reproductive health scholarship on cis women (Lampe, Carter, and Sumerau 2019). With this study design, I capture how a reproductive technology can reproduce notions of gender and race while the experiences themselves are simultaneously shaped by these cultural ideologies.
Data and Method
To analyze contemporary hysterectomy experiences, I conducted in-depth interviews with 100 individuals who have had, want, or are considering a premenopausal “elective” hysterectomy. An additional inclusion criterion was having a chronic reproductive illness such as endometriosis or fibroids, to capture the leading reasons for an elective hysterectomy, or being transgender or nonbinary, to include a historically excluded population in reproductive health literature broadly, and hysterectomy specifically. I use trans or transgender as an umbrella term for those whose gender assigned at birth differs from their gender identity and nonbinary to refer to those who identify with a gender beyond the categories of man or woman (shuster 2021). Some people identify with only trans or nonbinary, and some identify as both (Miller and Grollman 2015). In addition, while some trans and nonbinary participants also had a chronic illness (n = 16), the majority (n = 30) did not.
I employed a multipronged recruitment strategy to identify participants from varying backgrounds. I targeted social media pages organized around chronic reproductive issues (looking for key terms: endometriosis, fibroids, and adenomyosis) and transgender interests and health, distributing calls for participants in these groups after building rapport with the group administrators. These groups include EndoBlack, Fibroids Project, EndoWarriors, and various private and public Facebook groups organized around transgender health care. I also relied on snowball sampling, and various participants pointed me to friends or relatives, or disseminated my digital recruitment flier in listservs and online groups. The flier said, “Hysterectomies: Let’s talk about it!” and invited individuals who either have a chronic reproductive illness or identify as trans or nonbinary to participate in a remote interview.
In interviews, I asked about their experiences being diagnosed with chronic illness or with seeking gender-affirming care; their journey toward having a hysterectomy; their experiences with medical providers; and their attitudes toward family formation, reproductive technologies, and the sterility/infertility associated with a hysterectomy. Interviews lasted an average of 55 minutes and were conducted in 2020 over Zoom or phone, recorded using an audio recorder, and transcribed into a transcript. Transcripts were coded and analyzed abductively (Timmermans and Tavory 2012) using Atlas.ti through multiple iterations—first garnering broad themes and then tracking a more nuanced set of themes and subthemes. An abductive grounded theory analysis allows for new theoretical concepts to develop in response to unexpected findings against a framework of theoretical knowledge (Timmermans and Tavory 2012). After developing broad open codes, I identified the three medical pathways to a hysterectomy as well as the three associated emotional reactions to the hysterectomy based on gendered infertility discourses. I then employed axial coding to examine more closely these themes via reproductive discourses (Charmaz 2006). During this more focused round of coding, data were analyzed for discourse related to a desire to be childfree, a desire to have a family, emotional reactions to having a hysterectomy, emotional reactions to becoming infertile, and comfort level with one’s gender identity after the hysterectomy. The protocol for this study was approved by the City University of New York’s Institutional Review Board.
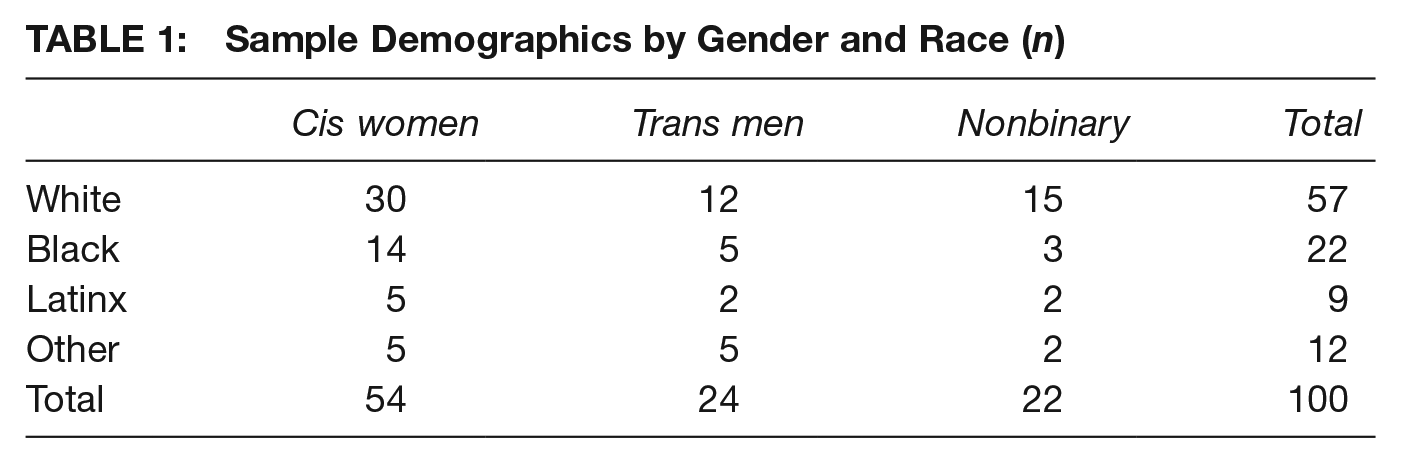
As shown in Table 1, the sample consists of 100 participants—46 TGNB individuals (24 trans men and 22 nonbinary, genderqueer, or agender) and 54 cis women. Of the 100 participants, 57 are white, 22 Black, 9 Latinx, and 12 Other which includes Asian American, American Indian, and Middle Eastern participants. Of the women, 36 are straight and 16 are lesbian or bisexual. Of the TGNB group, only one identifies as straight. The average age in the sample is 34 years and the range is 20–62 years. Of those with chronic reproductive illness (n = 70), 39 have endometriosis, 26 fibroids, 11 adenomyosis, 7 polycystic ovarian syndrome (PCOS), and 2 premenstrual dysphoric syndrome, with various having more than one of these diagnoses. In addition, the majority of participants (n = 71) had had a hysterectomy by the time of the interview, while 15 cis women and 14 trans or nonbinary participants had not yet had one; among those who had the procedure, 17 cis women and 15 trans men or nonbinary people also had a bilateral oophorectomy. Ninety-five participants were based in the United States across various states and regions, while four are based in Canada and one in England.
Sample Demographics by Gender and Race (n)
Findings
The results are presented in two parts. First, I examine patients’ interactions with their providers, which range from physician support to provider coercion to gatekeeping. Next, I discuss findings on patients’ experiences with their hysterectomy, which range from delight to grief to neutrality.
Same Procedure, Different Physician Interactions
Across interviews, I identified racial and gendered patterns in interactions with physicians, pointing to diverse meanings associated with hysterectomy. The patient–provider interaction regarding hysterectomy varies from total refusal, stoic coercion, to bureaucratic gatekeeping largely depending on the patient’s race and gender identity. These divergent interactions likewise indicate continued stratified reproduction (Luna and Luker 2013) whereby people have varying degrees of ability to achieve their reproductive goals based on their social positionality. However, in addition to stripping from Black and Indigenous women the ability to reproduce, physicians prevent white women (and nonbinary people gendered as women) from choosing to be sterilized. In addition, the fertility of trans individuals is often not foregrounded in the way it is for cis women, which allows increased access to hysterectomy while devaluing trans reproduction.
White women and many white nonbinary individuals throughout the life course in this study were told they were too young to have a hysterectomy, encouraged to try pregnancy instead as a solution to their chronic illness, or told they must have children first before they can have a hysterectomy. In other words, this group was often barred from the ability to opt into infertility. For instance, Stacey, a 24-year-old white woman, was told at the age of 21 by multiple doctors that she was too young for a hysterectomy and that she should consider having a baby to cure her endometriosis. When she explained that she was not interested in having a baby at this time, the doctor explained she did not need to keep the baby, but that the pregnancy would be therapeutic in and of itself, thus pushing her to reproduce at any cost, as she relayed, I was, like, “I’m not ready to have a kid. What are my other options?” and the first doctor was like hysterectomy, but since you’re so young, like, your insurance may not approve it, And the second doctor just didn’t give it as an option at all. He mentioned children. And he was like, “Well, you could always like, give it up for adoption, like you need your body to go through the process to help you.” And they just . . . the pregnancy was prioritized for some reason. I felt a lot of pressure from the doctors that a hysterectomy was such an extreme choice for me to have at my age, yet the option of having a kid at 21 didn’t seem as extreme to them.
Even white participants in their 30s reported being regarded as “too young” to be granted a hysterectomy they wanted. Instead, they were encouraged to try other routes of treatment for their condition, including various surgeries to remove endometriosis growths and fibroids, as well as Lupron, a hormone therapy that produces a temporary menopause. For instance, Arlo, a nonbinary person who has had debilitating endometriosis since age 17, sought a hysterectomy at age 30 with a doctor at a women’s clinic. As I will elaborate on later, Arlo did not follow the accepted medical steps of masculinization (hormone replacement and double mastectomy), and therefore was not viewed as a trans person receiving a trans surgery, but rather as a white woman, per Arlo’s perspective. Arlo recounted that the doctor “immediately shut it down and was like, we don’t even consider doing that until they’ve tried every other possible method.” Similarly, Ocean, a 26-year-old white nonbinary person, faced obstacles to hysterectomy due to “being gendered as a woman” by their doctors.
Even white patients whose ability to create or sustain a pregnancy was deemed implausible were still blocked from a hysterectomy. Take Clara, for instance, a married 27-year-old woman who has actively sought a hysterectomy for her PCOS and endometriosis for several years. After multiple refusals, she and her husband agreed on him obtaining a vasectomy as a way to “prove” their desire to be childless. She recounts it taking 20 minutes for her husband’s doctor to approve the vasectomy, although it did not work as a means of convincing doctors to grant her a hysterectomy.
In the case of Angelica, a 25-year-old white lesbian, doctors wanted to save her uterus in case a future, hypothetical male partner wanted a child with her. Multiple doctors told her a viable pregnancy would be nearly impossible for her due to the severity of her endometriosis and said hysterectomy was her only available treatment option. The following recounts what she was told at 24 years after asking for a hysterectomy: It was this circular conversation where they said “you don’t have to get rid of your uterus, but you also can never have a baby with it.” . . . He kept saying like. . .“what if you change your mind wanted to be with a man?” And I was like “I’m never gonna be with a man . . . and having a male partner would not make this medical decision different because you’re telling me I will only be safe and healthy if I take it out.” They were ready to prioritize fertility over my health and they were ready to prioritize the possibility of ever having a male partner who would value me for my fertility over my health.
In this way, white patients were often deemed too young well into their 30s, and their fertility—real and imaginary—was deemed more important than a desire for a hysterectomy or relief from chronic symptoms.
As a contrast, providers often recommended a hysterectomy to Black and Afro-Latina women before they ever desired one, and this recommendation often verged on coercion. For instance, Luna, a Black woman, with endometriosis symptoms similar to Stacey’s, was told at age 20 that she needed to have a hysterectomy to cure her endometriosis. Both women were college students in large metropolitan areas in their early 20s with severe and debilitating pelvic and menstrual pain later diagnosed as endometriosis. However, Stacey is white while Luna is a Black woman, leading to drastically different physician interpretations of their age, their fertility, and the implications of a hysterectomy. Luna recalls the following story at an OB-GYN (obstetrician-gynecologist) appointment for her pain between classes: They told me that I should get a hysterectomy. And I was like, “I’m 20. . .,” and they were quite callous about it, very nonchalant. They’re like, “You need to get a hysterectomy, you’re not gonna be able to have children.” And I was like how you going to tell 20-year-old woman that she needs to get a hysterectomy. She can’t even drink yet. She hasn’t started her life.
Similarly, Kat, a Black woman in her 40s, recalls doctors beginning to recommend a hysterectomy to her in her 20s, a suggestion that became relentless over time and across various doctors. As she told me, Every time I had a physical exam, every time I had a vaginal exam, every time I had a pelvic exam every time, it was like “hysterectomy, hysterectomy, hysterectomy,” it was it was definitely pushed.
Kat was resolved on having children and repeatedly told doctors that a hysterectomy was her last resort. Despite this, she recalled being informed by a nurse of a verbal altercation that occurred between her two surgeons while she was under general anesthesia for an excision surgery. In this retelling, one of the surgeons “was like, ‘just go ahead and do it. She’s in pain, she’s suffering. Just go ahead and give her hysterectomy.’” Kat told me she remembers asking herself “Why is she pushing a hysterectomy so hard?”
As another example, Carina, a 33-year-old Afro-Latina woman, recounted being surprised when her doctor recommended a hysterectomy to treat her endometriosis. However, she later found out that various women in her family had also had this procedure. She told me, I went back and he said, “Well, yeah. I see that the endometriosis is back so we need to do a hysterectomy.” He said, “Depending on how your ovaries are, I will keep them, so you can get the necessary hormones.” For me, it was like a shock, I was like, “Whoa, a hysterectomy?” and when I told my mom, she said “Oh, a hysterectomy? Yeah. Your aunt so and so had it and this other aunt had it” and I'm like, “Wait a minute. What do you mean she had it?” Nobody had told me anything. Why did she have it? She's like, “Oh, yeah. We have bad periods.”
As this excerpt indicates, experience with hysterectomy is often widespread among communities of color, such that for some, it comes to be viewed as a routine or inevitable surgery. This echoes López (2008) who found that sterilization procedures, including hysterectomy, are so widespread among Puerto Rican women that it is now referred to simply as “la operación” (“the surgery”). However, given stigma surrounding hysterectomy as well as gynecological care more broadly, the pervasiveness of this surgery might be unknown to some, as it was for Carina. As a contrast, Hazel, a 39-year-old Black woman, began feeling this inevitability as early as in her 20s because her aunt also had had endometriosis and thus a hysterectomy. As she told me, I was walking around in grad school, in my early 20s and I said, somebody's going to have to take this out eventually. And I remember that my aunt had a hysterectomy. Certainly no one my age had had it but I just had this thought. . .I just remember that consciously in my early 20s being like, this is going to go eventually.
This inevitability is rooted in the pervasiveness of hysterectomy as well as the lack of long-term alternatives for many chronic reproductive illnesses.
However, some women are hesitant to have a hysterectomy because it was a procedure that was pushed on their mothers or aunts. For instance, Michelle, a 36-year-old Black woman with fibroids, said a hysterectomy was pushed on her mother and led to medical complications. She recalled when a hysterectomy was offered to her in her 30s: I was offended that it was offered . . . and with me knowing the history of Black women’s bodies in medicine my immediate response was “I’m not going to do it.” The first time it was brought up in 2016, I ignored it. The second time in 2017 after having a well woman’s exam, I took a little more offensively that that would be the only option offered to me as someone that was in their mid-30s. So much so that I decided to change my OBGYN.
This hesitation was echoed by a handful of Black and Afro-Latina women who had been or currently are hoping to avoid hysterectomy.
In terms of cis versus trans experiences, perceived masculinity was the most salient factor in shaping the physician–patient navigation. In other words, for trans men and nonbinary people following the medicalized model of trans care—whom doctors often perceived as men, as reported by the participants in this study—there was an emphasis on following the bureaucratic steps associated with a medical gender transition in a way that superseded concerns over fertility. These steps typically begin with a gender dysphoria diagnosis and/or letter of approval by a mental health professional, followed by taking testosterone, top surgery, and then hysterectomy. Although the scientific evidence is unclear, many doctors consider hysterectomy an important health procedure for trans people on testosterone to avoid reproductive cancers, vaginal atrophy, and cramping associated with long-term testosterone use. Of note, unlike with cis women, race did not seem to shape these medical trajectories, as physicians appeared highly focused on gender and following the “standard trans health steps.” However, reaching the point at which a provider understands trans health and is willing to provide a hysterectomy requires first identifying a trans-affirming physician and overcoming bureaucratic and financial obstacles, including trans-exclusionary or incompetent insurance plans.
Across race and age, the physician approach to a hysterectomy for trans and nonbinary patients was along the lines of “you’ve followed these steps, you’re confirmed trans, hysterectomy comes next.” For instance, this is how Sam, a 22-year-old white trans man, described his journey to a hysterectomy with a bilateral oophorectomy when he was 19 years old: It was a suggestion from my doctor, actually. I was sort of asking him in the appointment about birth control, and he said, “Why not just get a hysterectomy? It seems like you don’t really need it for much.” And I thought, yeah, that’s probably true, I probably am not going to use my uterus at all . . . And it was fairly easy to get access to. So, I just figured it was the easiest and best decision for me at that point in my transition.
While white women were considered too young well into their 30s and doctors were very concerned about their future fertility, for Sam and other young trans men, a uterus was viewed as expendable and unnecessary—as evident in “seems like you don’t really need it”—and removing it was an easy process as long as the prior steps in their trans journeys had been taken. This shows the continued salience of gender and a physician’s desire to align the patient’s body with binary notions of gender, sex, and bodies (Kessler 1990); having a uterus is not in line with biological essentialist, binary notions of being a man. Many participants understood this transnormativity and biases against nonbinary individuals in health care, including Emmett, a 27-year-old white nonbinary person who had a hysterectomy and bilateral oophorectomy. They wanted a hysterectomy for chronic issues related to premenstrual dysphoric disorder but allowed doctors to assume that they were a trans man—because of taking testosterone—and that they wanted the surgery for gender affirmation. They told me, “I think my trans identity helped convince her that I would be a good candidate for surgery, even though I wasn’t pursuing the surgery because I am trans” and mentioned not correcting clinicians when they used he/him pronouns due to “bias or confusion around how nonbinary fits into a very binary medicalized system.”
Kai, a nonbinary person who had been taking testosterone, remembers being surprised their doctor recommended the surgery when they went in for birth control: She said, I want to explain to you all the options you have. And she included the option of hysterectomy and I was probably like, 26 or 25. And I was just like, “What? That’s an option at this age?” And she said, “Yeah, it’s your body, you get to decide what happens.” The next day, I was like, I’m ready for this hysterectomy. Let’s get this ball rolling.
This notion of bodily autonomy for trans folks was present across race groups. For instance, Jake, a biracial (Black and white) 30-year-old man, went in for cramping and was similarly surprised by the ease of getting the surgery (with bilateral oophorectomy) approved and by the amount of autonomy granted to him: I went in and he was like, “Yes, you are in pain. Do you want hysterectomy? Like, I’ll do it in two weeks.” . . . He was like “You know what you’re doing” and I was like, “I do know what I’m doing, thank you so much.” And he was like, “Okay, I can book you in like in two or three weeks. I was like, “Okay.”
Across age, race, and geographic location, the transnormative steps and masculinity took precedence, and if these factors were evident, fertility ceased to be a concern. Binary notions of the body also influence these encounters, as men’s bodies are discursively constructed as not “supposed” to get pregnant; trans men are, therefore, exempt from discourses of women’s bodies as pre-pregnant (Waggoner 2017) despite having pregnancy potential. Jax, a white 32-year-old trans man, said fertility was mentioned in the same way as other side effects of testosterone and hysterectomy such as balding. He said, I didn’t ever really have conversations about fertility preservation with anyone. I think it was mentioned in the same way we’ve mentioned that it was mentioned I would lose my hair and I wish that I would have understood that a little more now. But I don’t regret not having done that process.
As this section has demonstrated, the gendered notion of women’s bodies as “pre-pregnant” in health care is complicated by racialized reproductive politics. At the same time, transmasculine bodies are often construed as detached from these reproductive discourses.
Same Uterus, Different Reactions
The different patient–provider interactions in turn led to distinct individual reactions to one’s hysterectomy—whether they had already had kids or not. For those who had to fight for a hysterectomy—typically white women—there is delight associated with the hysterectomy. This joy surrounding the hysterectomy tended to be particularly tied to the end of menstruation and the alleviation of chronic pain and bleeding. The feelings around infertility were secondary to the relief and happiness of lessened symptoms. Many respondents said the surgery was the best choice they have made or the best way they have ever taken care of themselves; thus, the process of becoming infertile, in these cases, was full of joy and relief. Some even say they wish they had it sooner, such as Samantha, a 36-year-old white lesbian who had to “fight” to have surgery—seeing dozens of doctors and being forced to have a psychological evaluation before a surgeon agreed to the hysterectomy. She finally had the surgery at age 32 (and kept one ovary) after 7 years of debilitating symptoms, and this is how she explained her feelings about the surgery: It was the best thing I ever did. Oh my god. Yeah. Great. My quality of life has improved like 1,000%. I’m very happy that I did it . . . My only grudge is that like, I didn’t, I wasn’t able to access it even earlier . . . My only regret is not being able to get it earlier.
This feeling was echoed across interviews—predominantly by white women—whether the woman had kids already or not. For instance, Janet, a 43-year-old white woman (who kept both ovaries), said the following: It was the best thing I ever did for myself was having that surgery. I was a little concerned that it would make me feel less like a woman in some way. But it really hasn’t. It hasn’t made me feel less feminine or anything and if anything I feel more confident because I’m not so preoccupied with it. I mean, it served a purpose. And I didn’t end up using it for its intended purpose. You know, I was done with it. So, no it didn’t make me feel less feminine or less of a woman.
This was the case for white women across ages. For instance, Samantha, a white woman who had a hysterectomy (and kept both ovaries) at 24 for fibroids and PCOS, said her advice for other women is “Don’t dread it, look forward to it.”
While these feelings mapped on to race, the key variable is feeling agentic and actively choosing hysterectomy, which tended to be felt by white women. However, Faizah, a 31-year-old Black woman, had to fight for her hysterectomy in a way that resembled the common struggle among white women. After 6 years of not being believed by various doctors, she was finally diagnosed with endometriosis, and a reluctant surgeon agreed to the hysterectomy and bilateral oophorectomy after an altercation in his office. After this struggle, Faizah echoed sentiments of being thrilled about the surgery and feeling more feminine postsurgery rather than less: I can’t recommend it enough. I had six years of just pain for what reason? If somebody had just been like “a hysterectomy might be possible for you” earlier, the course of my life would have changed. I’m so excited and happy now. So just in all aspects it got better because of that one like three-hour surgery . . . They say that one of the side effects after the surgery is just sadness because there’s a loss there. In fact, like, I have felt more feminine after this because I’m not constantly bleeding and feeling disgusting you know? So yeah, I didn’t feel that loss not for one moment.
This feeling of delight over the surgery was the prevailing feeling among white women, with many saying they did not feel emotionally connected to their uterus nor had a grief about losing fertility or femininity, even if they did not already have kids or if they had one or two ovaries removed. For instance, Elizabeth, a 43-year-old white woman who never had children, said the following about her hysterectomy with bilateral oophorectomy: I don’t know if it’s about being a woman, but I felt like once I had it done, I had my autonomy back. Because all these organs were like conspiring against me for so long that it was just good to be rid of them.
This account is in the same cadence as women who did already have children, such as Anabelle, a white woman who had a hysterectomy at 30 (and kept one ovary) and had one child. She said her feelings before surgery was, “It did what it needed to do. Now I’m not using it and it’s only causing problems.” Encapsulating this positive spin on hysterectomy and gender, Arizona—a white woman who had a hysterectomy and a bilateral oophorectomy at 28 and never had children—told me, “I am the best I’ve been in ages . . . I am a new woman without ovaries or uterus.” In these cases, the process of opting into infertility is a source of joy and relief, and even becoming more confident as a woman.
On the other end of the spectrum of emotions, women who felt pressured by their physician to have a hysterectomy reported the most grief from having had the procedure and from becoming infertile as a result. These accounts were by far the most gendered, even more so than the accounts of TGNB participants, because the gender identities of these interviewees were highly tied to reproduction and having a uterus. Moreover, the grief was the most prominent among Black women in the sample, who said across many interviews that they fight feelings of being “less of a woman.” For instance, Tamara, a Black woman who had a hysterectomy (and kept both ovaries) at 26, said, When the one thing that separates you versus a man is taken away, it makes you question your identity . . . I struggled with feeling like I wasn’t, like, worth being a mom. Or like, worth being a wife? And when the role that’s in question is as deep as being a woman, and whether or not you’re good enough to be seen as a woman or good enough to fulfill the role women are supposed to fill and when you ask yourself that, the answer is no, because you don’t have a uterus.
Tamara’s grief is so strong, she has sticky notes on her mirror to remind herself daily “you are worthy of being a woman” and “you’re worthy of being a mom.” Similarly, Daisy, a Black woman who had a hysterectomy with a bilateral oophorectomy at 28 for endometriosis, echoed these sentiments when I asked how no longer menstruating made her feel about being a woman: Oh, I feel like I failed at it. I feel like I failed the one job I supposed to do. So not being able to reproduce. So I barely feel womanly . . . now I just feel like I’m full male, you know? I know I’m meant for more, of course, but God created woman and man to reproduce. So my job is to reproduce or at least to bring life to the world. And so, I’m not fulfilling my full purpose. Not getting a cycle, the whole surgery took that from me. That took the one key role in life for me.
This connection between reproducing and womanhood was evident among other women of color in the sample, such as Marisol, a 31-year-old Afro-Latina with fibroids and endometriosis. She is putting off a hysterectomy because she wants to have a biological child but has not been able to carry a pregnancy to full term. She said her pain was so bad, she “would want to grab a knife and just literally pull my uterus, out of me if I could,” but is waiting until she turns 35 to have the surgery. Her connection between reproducing, her uterus, and her gender identity comes through in her account below: Not being able to have a baby full term almost makes me feel like less of a woman. And I hate that. I hate feeling like I am less of a woman, because I can’t carry a child for full term. So, I can only imagine if I didn’t have a uterus. I think that would definitely affect my femininity and how I feel as a woman. It’s kinda like a man getting rid of his testicles, or taking out their testosterone. How is a man gonna feel? It’s the same.
In Marisol’s case, her gender identity is rooted in having a full-term pregnancy and in having a uterus, and she equates the removal of a uterus with a man losing his testicles or testosterone. Valeria, a 42-year-old Asian American woman, said she regarded her reproduction as a duty to her husband and her family. She had one child, but her endometriosis scarring led to repeated miscarriages. She did not desire a hysterectomy until her mom mentioned it to her: My mom told me, “Why don’t you just get a hysterectomy?” And I think that was a permission I needed. You know, because with a lot of immigrant families like, the bigger the family the better, you know, it was expected that I was going to have like six kids. So, I felt I wanted to hold on to that because I felt like I was letting my husband down and I was letting my family down because I was. . .I was unable to reproduce more. And I think that’s why I held on to trying for such a long time.
Despite her mom’s “permission,” Valeria did experience gendered grief after surgery (in which she kept her ovaries), saying, “You always associate your uterus with births and reproducing, right? So yeah, I think for a moment there, I definitely questioned my worth as a woman.”
Surprisingly, the accounts of trans men and nonbinary participants were much less gendered, compared with those of women of color. While delight and gender euphoria were present for some—particularly those who are nonbinary and do not take testosterone—the majority reported feeling neutral about the surgery and its associated process of becoming infertile, a feeling that was not reported by any other gender. This neutrality was even present among those who were also experiencing chronic symptoms. In this case, a hysterectomy is viewed as a to-do list item on a long list of needed procedures and therapies in their medical transition—mirroring the way physicians treated the surgery. For instance, Cole, a 21-year-old Black trans man who had a hysterectomy (and kept one ovary) at 19, describes it as part of a long process that logically came next: It was sort of a step in a pretty long process. I had started socially transitioning at the onset of middle school. And then I had gotten top surgery at 15. And then I knew there’s like, this kind of ongoing thing in the trans community of like, does testosterone cause like atrophy of reproductive organs? There’s not like a clear consensus on if it does. And, for me, it was just kinda like the natural next step. I know, that probably doesn’t sound very, like substantial but it’s sort of almost like, logistic wise, it just sort of worked with timing.
Like Cole, many trans and nonbinary interviewees described the risk of cancer and atrophy as a primary motivator to having a hysterectomy, particularly because menstruation typically ceases while taking testosterone. For instance, Jules, a 30-year-old white trans man, describes his feelings toward a hysterectomy, which he has not had yet because it feels like “a hassle,” but he plans to: I don’t want it enough to overcome obstacles, because it’s sort of like getting your flu shot. You know you should get your flu shot, but I’m also not like, excited to get my flu shot, you know, and so if someone makes it really difficult for me to get one, I’m gonna be like, well, screw you . . . . If someone came to me and they’re like, I can give you a pill that will guarantee that you will never get reproductive cancer. I’d be like, okay, I’ll do that. And I don’t need to deal with this.
In Jules’s case, he would much rather avoid a hysterectomy and its associated challenges. Across interviews, this was largely due to a neutrality regarding the uterus, and not anticipating or feeling gender euphoria from having the uterus removed. This is particularly the case when comparing their gender euphoria associated with having top surgery (a double mastectomy), which across the board elicited joy. Jake, a 30-year-old biracial trans man, compared his feelings after a hysterectomy and top surgery: It feels with the top surgery there was like a visual. It was like “Okay, now I can wear like shirts I want” and this one is like internal so it almost feels like nothing happened to a certain extent. Definitely like the pain I was having stopped which was great. But like, it doesn’t necessarily like feel like a huge shift occurred.
As Jake’s quotation shows, a hysterectomy was often described in these neutral medical terms—as a means of stopping cramps or preventing illness associated with testosterone usage. Similarly, Daniel, a 28-year-old mixed-race man, described his hysterectomy (with bilateral oophorectomy) in impartial, medical terms: I guess I feel quite neutral. It’s like, just a necessary medical procedure. . . Like, if you have like a broken arm, you feel like, “Oh, I’m glad that my arm is no longer broken, I had surgery to fix that,” it’s kind of like just a neutral feeling.
This neutral feeling was repeated across interviews—spanning age and race. This neutrality is exemplified by Jax, a 32-year-old white man who wants a hysterectomy one day, who says for him the surgery is “not very emotional. It seems more practical.”
Discussion
In this study, I examined hysterectomy narratives across two gendered case studies. Hysterectomy is a contested medical practice that affects reproduction—specifically, one that removes one or more “women’s reproductive organs.” Thus, an analysis of hysterectomy narratives reveals broader social norms and politics surrounding gender, reproduction, race, and bodies. As prior scholars of reproductive politics and stratified reproduction have demonstrated, social positionality largely influences the degree of bodily autonomy and reproductive choice afforded. Gendered pronatalist discourses of women’s bodies as pre-pregnant combine with racialized discourses of women of color as hyperfertile and white women’s fertility as in need of protection. By including stories of trans and nonbinary individuals, I provide a more holistic understanding of how these gendered discourses of bodies shape reproductive politics and produce reproductive stratification. Examining stratified reproduction across gender identity reveals how all reproductive choices are constrained—simultaneously pushing some individuals toward loss of fertility while paternalistically barring others from the ability to opt into infertility or sterility.
As I demonstrated, stratified reproduction influences not only the patient–provider interaction but also the way one understands the biological experience of a hysterectomy. This pattern is unrelated to the additional removal of ovaries, despite Elson’s (2003) finding of oophorectomy leading to increased regret, since perceived agency was key in shaping one’s reaction rather than the type of surgery. Rather than based solely on medical and biological fact, then, modern hysterectomy experiences are influenced by gender and race. Counter to dominant assumptions in discourse and sociological literature of hysterectomy—and sterilization and infertility writ large—causing grief and pain, the hysterectomy narratives I draw from reveal a wide range of responses—from delight to neutrality to grief. Similarly, these stories reveal patient–provider interactions ranging from physician support to provider coercion to gatekeeping. These patterns map on to gender, race, and ethnicity, revealing persistent reproductive stratification by social positionality and the importance of a reproductive justice framework.
As I delineated above, the experience of a hysterectomy was not the most gendered among the trans population, as expected, but rather by women of color who did not feel agentic in their hysterectomy experiences. Whereas trans men and transmasculine nonbinary people described their hysterectomy in neutral medical language or as one step on a long to-do list, descriptions of feeling like “less of a woman” were frequent in interviews with women of color. White women, on the other hand, across the board described not feeling their gender is tied to reproduction or reproductive body parts. These findings show the complexity in meanings of gender, bodies, and reproduction, in a way that necessitates an intersectional analysis of reproductive experiences. Moreover, these findings add to literature on reproductive justice by examining how social positionality influences the degree of choice one has in making reproductive decisions, not only in terms of opting into infertility but also in terms of maintaining one’s capacity to safely gestate a pregnancy.
Conclusion
Reproduction often serves as a symbolic repository through which to express anxieties and clarify values surrounding gender, race, and the family. Examining the various meanings embedded in a complex sterilization procedure such as hysterectomy—entwined as it is in notions of medical sexism, racist abuse, and trans health care—is, therefore, an important step in understanding and dismantling the power structures across various social institutions.
Moreover, these findings have important implications for theory and policy. First, these findings underscore the importance of a trans-inclusive, intersectional approach in studies of reproductive health because race and gender identity are key in shaping these health care experiences. Analyses that account for the role of race and gender in reproductive health are critical for challenging hegemonic notions of reproduction and the body, particularly given the longstanding centering of cisgender, white women in sociological studies of reproduction. Furthermore, this study highlights the importance of increased biomedical research on chronic reproductive illness and trans health, as well as the value of a patient-centered approach to health care to reduce the extant barriers patients currently have in the ability to make reproductive choices. In the current sociopolitical landscape in which abortion, contraception, and gender-affirming health care are simultaneously under legislative attack, increased attention to all elements of reproductive and gendered health care is of heightened importance.
Footnotes
Author’s note:
I gratefully thank Susan Markens for her mentorship and support throughout the entire process of this study. I am also grateful to Virginia Kuulei Berndt, Lynn Chancer, stef shuster, Mary Clare Lennon, and the anonymous reviewers for their helpful comments as well as to every participant who trusted me with their story. This work was supported by the Society of Family Planning Emerging Scholars Grant.
Andréa Becker is a postdoctoral researcher at the University of California, San Francisco, in the research program Advancing New Standards in Reproductive Health (ANSIRH). Dr. Becker’s research examines “contested medical practices,” or elements of medicine culturally deemed controversial, with particular interest in reproductive health. Dr. Becker’s forthcoming book Unchoosable (NYU Press 2024) examines elective hysterectomy experiences from a feminist science and technology studies framework.