
Abstract
Introduction
Perinatal outcomes refer to events affecting a newborn after fetal viability, typically from 28 weeks of gestation through the first seven days of life. Adverse perinatal outcomes include stillbirth, low birth weight, preterm birth, early neonatal death, perinatal mortality, admission to a neonatal intensive care unit, and birth asphyxia. Despite substantial reductions in under-five mortality over recent decades, neonatal mortality rates have shown minimal improvement in sub-Saharan Africa.
Objective
This study aimed to assess the effect of maternal near-miss on adverse perinatal outcomes among women admitted to hospitals of Gurage Zone, Ethiopia.
Method
A facility based prospective cohort study was conducted in Gurage zone public hospitals, from April 2022 to January 2023. The exposed groups were women admitted during pregnancy and childbirth in selected hospitals during the study period and fulfilled at least one of the near-miss conditions under the modified World Health Organization (WHO) near-miss criteria. Unexposed groups were women without any complications under the modified WHO near-miss criteria. The primary outcome of interest was the composite adverse perinatal outcome (stillbirth, low birth weight, preterm birth, early neonatal death, admission to the neonatal intensive care unit, and birth asphyxia). The perinatal period starts from 28 weeks of gestation to 7 days of life.
Results
A total of 1032 women (258 with near misses and 774 without near misses) completed the follow-up time (completion of the perinatal period, discharge from the hospital, or development of the outcome). The incidence of composite adverse perinatal outcomes was 19.48% (37.98% exposed vs. 13.31% unexposed). After adjusting for potential confounders, the risk of adverse perinatal outcomes was higher among women with near-miss events (adjusted relative risks [ARR]: 2.36; 95% confidence interval [CI]: 1.74, 3.18). In addition, there was a higher risk of adverse perinatal outcomes among rural residents (ARR: 1.52; 95% CI: 1.14, 2.03), women with chronic hypertension (ARR 1.66; 95% CI: 1.05, 2.62), and anemia (ARR 1.60; 95% CI: 1.10, 2.31).
Conclusions
The risk of adverse perinatal outcomes has remained higher among women with near-miss events, even after controlling for potential covariates. Adverse perinatal outcomes were also significantly higher among rural residents, women with chronic hypertension, and anemia. Therefore, interventions focusing on maternal risk factors are crucial for reducing adverse perinatal outcomes.
Introduction
Perinatal outcomes refer to events affecting a newborn after fetal viability, typically from 28 weeks of gestation through the first seven days of life. Adverse perinatal outcomes include stillbirth, low birth weight, preterm birth, early neonatal death, perinatal mortality, admission to a neonatal intensive care unit (ICU), and birth asphyxia (Jaleta et al., 2021; Liyew et al., 2018). Despite substantial reductions in under-five mortality over recent decades, neonatal mortality rates have shown minimal improvement in sub-Saharan Africa. The highest burden of neonatal deaths occurs in low- and middle-income countries (Jjuuko et al., 2024; World Health Organization, 2019). Approximately two-thirds of neonatal deaths occur within the first week of life, with the greatest risk occurring within the first 24 h after birth (Organization, 2007). Globally, an estimated four million perinatal and neonatal deaths occur each year (Blencowe et al., 2016). Ethiopia bears a significant burden of stillbirths and early neonatal deaths and is among the top 10 countries with the highest perinatal mortality rates worldwide (Akombi & Renzaho, 2019; Jena et al., 2020).
Maternal near-miss (MNM) refers to women who survive severe, life-threatening complications occurring during pregnancy, childbirth, or the postpartum period. Due to the overall reduction in maternal mortality in high-income countries and the need to improve the quality of care in low-income settings, studies focusing on MNM have become increasingly common (WHO, 2011). MNM events serve as proxy indicators of maternal and neonatal health and are used to evaluate the quality of obstetric care in health institutions (Pattinson et al., 2003). Despite efforts to scale up maternal and neonatal health services, neonatal mortality in Ethiopia remains high, with a slight increase from 29 to 30 deaths per 1,000 live births (Central Statistical Agency, 2016; Mini Ethiopian Demographic Health Survey, 2019). The contribution of maternal life-threatening complications to neonatal morbidity and mortality also remains substantial in Ethiopia (Liyew et al., 2018; Tura et al., 2020). Achieving the Sustainable Development Goal target for neonatal health—reducing neonatal mortality to 12 or fewer deaths per 1,000 live births by 2030 (Assembly General, 2015), require accelerated evidence-based interventions.
Previous studies have shown that MNM events are associated with a higher risk of adverse perinatal outcomes (Oliveira & Costa, 2013; Tura et al., 2020). Addressing factors that contribute to pregnancy-related complications may reduce adverse neonatal outcomes. Therefore, examining the association between MNM and adverse perinatal outcomes is essential. Even within a single country, certain populations are at higher risk of adverse perinatal outcomes, including women with short interpregnancy intervals, preexisting medical conditions, and obstetric complications (Farrar et al., 2016; Yao et al., 2019). A recent study conducted in public hospitals in eastern Ethiopia reported substantially higher perinatal mortality among women who experienced MNM compared with the general population (320 vs. 75 per 1,000 births) (Agarwal et al., 2022; Morka et al., 2024; Tura et al., 2020).
Although several studies have examined MNM in Ethiopia (Geleto et al., 2020; Tenaw et al., 2021), few have focused on subsequent adverse perinatal outcomes among affected women (Liyew et al., 2018; Tura et al., 2020). Moreover, existing literature has primarily emphasized stillbirth and neonatal mortality (Aliyi et al., 2021; Tura et al., 2020), which represent only a fraction of adverse perinatal outcomes. Therefore, assessing the effect of MNM on a broader range of perinatal outcomes is essential for designing evidence-based interventions to improve perinatal health. Accordingly, this study aimed to assess the effect of MNM on adverse perinatal outcomes among women admitted for pregnancy and childbirth in Gurage Zone hospitals.
Literature Review
Burden of Maternal Near Miss
The burden of MNM varies across world regions and is disproportionately concentrated in low- and middle-income countries, with the highest prevalence reported in African and Asian countries (Tunçalp et al., 2012). A study conducted in India reported an MNM ratio of 9.27 per 1,000 live births (Reena & Radha, 2018). While a similar study in China reported an MNM ratio of 4 per 1,000 live births. In Africa, reported MNM ratios range widely from 8 to 198 per 1,000 live births (Chikadaya et al., 2018; Mbachu et al., 2017). Studies conducted in Zimbabwe and Ghana have documented MNM ratios ranging from 8 to 28.6 per 1,000 live births, indicating substantial regional variation in the burden of severe maternal complications (Chikadaya et al., 2018; Tunçalp et al., 2013). In Ethiopia, a cross-sectional study conducted in public hospitals in Addis Ababa reported an MNM ratio of 8.01 per 1,000 live births (Liyew et al., 2017). Other studies conducted in public hospitals in Jimma and the Amhara Region reported MNM ratios of 50.4 per 1,000 live births, 24.2 per 1,000 live births, and 266 per 1,000 live births, respectively (Woldeyes et al., 2018; Worke et al., 2019).
Incidence of Adverse Perinatal Outcomes Among Women With and Without MNM
A cohort study among women admitted to public hospitals in Addis Ababa reported an overall incidence of adverse perinatal outcomes of 36.6%. The incidence was 72.9% among women with MNM and 24.5% among women with uncomplicated deliveries. The study further reported that, among women with MNM, 29.5% experienced stillbirth, 40.6% had preterm births, 39.6% had infants with low birth weight, 57.5% had infants with low 5 min Apgar scores, and 29.5% had infants admitted to the NICU (Liyew et al., 2018). Another study conducted in southeast Ethiopia reported that the incidence of adverse perinatal outcomes, specifically neonatal mortality, was 4.33% among women with MNM compared with 0.93% among women without MNM (Aliyi et al., 2021). Similarly, a study in eastern Ethiopia found that the incidence of perinatal mortality was 320 per 1,000 births among women with MNM, compared with 75 per 1,000 births among women without MNM (Tura et al., 2020).
Risk Factors Associated With Adverse Perinatal Outcomes
A study conducted in India reported that women in the MNM group had a significantly higher likelihood of delivering a stillborn infant (p < .001) (Agarwal et al., 2021). Similarly, a study in Brazil identified MNM as a significant risk factor for adverse perinatal outcomes (Oliveira & Costa, 2013). a finding that was also reported in Nigeria, where the risk of adverse perinatal outcomes was significantly higher among women with MNM (Adeoye et al., 2013). Another study conducted in Brazil further demonstrated an association between MNM and adverse perinatal outcomes (Zanardi et al., 2019). In Ethiopia, a prospective cohort study in Addis Ababa found that women with MNM had a fivefold higher risk of adverse perinatal outcomes compared with women who delivered without obstetric complications (Liyew et al., 2018). Likewise, a study in southwest Ethiopia reported that women who experienced MNM were eight times more likely to experience neonatal mortality than their counterparts (Aliyi et al., 2021).
Other factors associated with adverse perinatal outcomes include rural residence, a history of stillbirth, twin pregnancy, and maternal educational status (Liyew et al., 2018; Santana et al., 2018). The risk of adverse perinatal outcomes was 1.5 times higher among twin pregnancies compared with singleton pregnancies (Santana et al., 2018). A study conducted in Addis Ababa reported that women residing in rural areas were twice as likely to experience adverse perinatal outcomes, independent of the presence of MNM. The same study also found that women with a history of stillbirth were at increased risk of adverse perinatal outcomes (Liyew et al., 2018). Additionally, a study in eastern Ethiopia reported that the risk of perinatal mortality was three times higher among grand multiparous women (Tura et al., 2020).
Research Questions
What is the incidence of adverse perinatal outcomes among women without MNM in Gurage zone public hospitals, central Ethiopia?
What is the incidence of adverse perinatal outcomes among women with MNM in Gurage zone public hospitals, central Ethiopia?
What is the determinant of the effect of MNM on adverse perinatal outcomes in Gurage zone public hospitals, central Ethiopia?
Methods
Study Settings, Design, and Time Frame
This study was a facility-based prospective cohort conducted among women admitted to hospitals in the Gurage Zone, including Wolkite Specialized Teaching Hospital, Atat Primary Hospital, Butajira General Hospital, and Bue Primary Hospital. These hospitals were selected because of their high annual delivery volumes, the presence of qualified consultants capable of managing life-threatening maternal complications including emergency cesarean sections and established ICUs. The study was conducted from April 1, 2022, to January 30, 2023.
Participants
The source population included all women admitted during pregnancy and childbirth to hospitals in the Gurage Zone. The study population consisted of women admitted during pregnancy and childbirth to the selected hospitals in the Gurage Zone from April 1, 2022, to January 30, 2023.
Exposed Group
Women admitted during pregnancy and childbirth to the selected hospitals during the study period who met at least one of the MNM conditions, as defined by the modified World Health Organization (WHO) MNM criteria (Tura et al., 2017).
Unexposed Group
Women admitted to the same hospitals who delivered without any complications, according to the modified WHO MNM criteria, constituted the nonexposed group. Nonexposed participants were selected on the same day as each near-miss case.
Inclusion Criteria
Women who experienced MNM comprised the exposed group. Accordingly, all women admitted for delivery to the selected hospitals during the study period who met at least one of the WHO MNM criteria were included in the exposed group (Tura et al., 2017). Women who delivered without any complications were included as nonexposed group.
Exclusion Criteria
Women with MNM events related to abortion or ectopic pregnancy were excluded from the study. Additionally, women with MNM who delivered at another facility were excluded, as it was not possible to determine perinatal outcomes. Women whose fetal vital status was unknown at the end of follow up were also excluded. Although women with multiple pregnancies are recognized risk factors for preterm birth, low birth weight, and low Apgar scores key indicators of adverse perinatal outcomes no women with multiple pregnancies were identified during the study period.
Sample Size and Sampling Procedure
The sample size was determined using Epi-Info 7 Statcalc for cohort studies by using the following assumptions: two-sided confidence level of 95%, power of 80%, exposed to the unexposed ratio of 1:3, and proportion of adverse perinatal outcomes among women with MNM (4.33%), and without MNM (0.93%) from previous studies in Ethiopia (Aliyi et al., 2021). By adding 10% losses to follow-up rates, the final sample size required for this study was 1,044 women (261 exposed and 783 unexposed).
All women who met the MNM criteria and were admitted to the hospitals during the study period were included in the exposed group. The entry point for women in the exposed group was the time of exposure identification, which occurred upon their arrival at the hospital. For the unexposed group, the entry point was the time of random selection of study participants. The exit point for both groups was the end of the perinatal period (seven days after delivery), discharge from the hospital, or the occurrence of the outcome, whichever came first. For each woman in the exposed group, three women admitted on the same day were selected for the unexposed group. A lottery method was used to randomly select unexposed participants from among eligible women.
Data Collection Tool and Procedure
Data were collected using an interviewer-administered questionnaire and a thorough review of maternal and neonatal medical records. The questionnaire was translated from English to Amharic and then back to English to ensure consistency. Data collection was conducted through face-to-face interviews using the Amharic version of the questionnaire. Four trained BSc midwives and one MSc midwife supervisor collected data from participants at the selected hospitals. To ensure data quality, the data collectors and supervisor received two days of training on the study objectives, relevance, pretesting, interview techniques, and ethical handling of participant information.
A pretest was conducted on 5% of the total sample at a public hospital in the Gurage Zone that was not part of the study sites to validate the survey tool and standardize the questionnaire. The questionnaire included sections on sociodemographic characteristics, reproductive and obstetric history, medical conditions and personal habits, the modified WHO MNM tool, and perinatal outcomes. Information on MNM events and adverse perinatal outcomes was extracted from maternal and neonatal medical records using the modified WHO MNM tool (Tura et al., 2017). Women in both the exposed and unexposed groups were also interviewed using the pretested structured questionnaire to collect data on potential confounders of adverse perinatal outcomes. Interviews were conducted when participants were stable, near the time of hospital discharge (Figure 1).

Flowchart of study participant selection and follow up in maternal near-miss cohort study among exposed and nonexposed groups of women admitted in Gurage Zone Hospitals, southwest Ethiopia 2022 (n = 1032).
Measurement of Variables
The primary outcome of interest was the composite adverse perinatal outcome. The presence of adverse perinatal outcomes was generated by summing up individual perinatal outcomes: stillbirth, low birth weight, preterm birth, early neonatal death, perinatal mortality, admission to NICU, and birth asphyxia.
Stillbirth: Refers to a newborn delivered without signs of life at or after 28 completed weeks of gestation.
Preterm: Refers to a live newborn after 28 completed weeks of gestation but before 37 completed weeks.
Low birth weight: Refers to a newborn weight of less than 2500 g.
Birth asphyxia: Refers to the fifth minute Apgar score below 7.
Early neonatal mortality: Refers to the loss of a newborn within seven days of life (Jaleta et al., 2021; Liyew et al., 2018).
Gestational age was determined using the last normal menstrual period or early ultrasound estimations.
Maternal near-miss: Refers to a woman admitted to the selected hospitals during pregnancy and childbirth who fulfilled at least one of the MNM conditions per the Modified WHO MNM criteria.
Maternal Near-Miss
Diagnosis of events of MNM was a two-step process: first, all women were screened for the presence of any of the potentially life-threatening conditions such as severe postpartum hemorrhage, severe preeclampsia, eclampsia, uterine rupture, a severe complication of abortion and sepsis/ severe systemic infection, and received critical interventions (use of blood products and laparotomy other than cesarean section); admitted to the ICU. After that, women with potentially life-threatening conditions were further assessed for life-threatening complications (MNM events). A woman who had one or more potential life-threatening complications was classified as having MNM events. The identified MNM by data collectors was evaluated and confirmed by the first author (Table 1).
Modified WHO Maternal Near-Miss Criteria (Tura et al., 2017).

Note. ICU=intensive care unit; WBC=white blood cell; WHO=World Health Organization.
Acute cyanosis is the blue or purple coloration of the skin or mucous membranes due to low oxygen saturation.
Gasping is a terminal respiratory pattern, and the breath is convulsively and audibly caught.
Shock is persistent severe hypotension, defined as a systolic blood pressure <90 mmHg for ≥60 min with a pulse rate of at least 120 despite aggressive fluid replacement (>2 L).
Oliguria is urinary output <30 mL/h for 4 h or <400 mL/24 h.
Failure to form clots can be assessed by the bedside clotting test or absence of clotting from the IV site after 7 to 10 min.
Loss of consciousness lasting >12 h is a profound alteration of mental state that involves complete or near-complete lack of responsiveness to external stimuli. It is defined as a Glasgow Coma Scale <10 (moderate or severe coma).
g Stroke is a neurological deficit of cerebrovascular cause that persists beyond 24 h or is interrupted by death within 24 h.
Uncontrolled fits/total paralysis is refractory, persistent convulsions or status epilepticus.
Preeclampsia is defined as the presence of hypertension associated with proteinuria. Hypertension is defined as a blood pressure of at least 140/90 mmHg on at least two occasions and at least 4 to 6 h apart after the 20th week of gestation in women known to be normotensive beforehand. Proteinuria is defined as the excretion of 300 mg or more of protein every 24 h. If 24h urine samples are not available, proteinuria is defined as a protein concentration of 300 mg/L or more (≥1 on dipstick) in at least two random urine samples taken at least 4 to 6 h apart.
Eclampsia is diastolic blood pressure ≥90 mmHg or proteinuria +3 and convulsion or coma.
Uterine rupture is a complete rupture of the uterus during labor and/or confirmed later by laparotomy.
Sepsis or severe systemic infection is defined as a clinical sign of infection and 3 of the following: temp >38˚C or <36˚C, respiration rate >20/min, pulse rate >90/min, WBC >12,000.
Pulmonary edema is an accumulation of fluids in the air spaces and parenchyma of the lungs.
Severe abortion complications are defined as septic in incomplete abortion, complicated Gestational Trophoblastic Disease with anemia.
Severe malaria is defined as major signs of organ dysfunction and/or high-level parasitemia or cerebral malaria.
Covariates
Sociodemographic factors such as place of residence, age of women, educational status, and occupation; obstetrics and RH-related factors such as the party, history of abortion, history of stillbirth, previous cesarean section, and antenatal care (ANC) utilization; preexisting medical conditions such as chronic hypertension, preexisting diabetes mellitus, heart disease, and anemia; personal habits such as alcohol consumption and cigarette smoking were taken as potential covariates.
Data Quality Control
Training was provided to data collectors and supervisors for two days, covering the study objectives, the data collection tool, and proper data collection procedures. Frequent supervision was conducted by the principal investigator and supervisors throughout the data collection period. The questionnaire was pretested on 5% of the study population at Gunchire Hospital to assess its appropriateness and validity. MNM events were identified using a modified WHO near-miss criteria, which has been tested in multiple studies in Ethiopia and Namibia and has been shown to be effective for MNM research in low-resource settings (Heemelaar et al., 2019; Tura et al., 2017; Tura et al., 2018) were used to identify exposed groups. All identified MNM cases were confirmed by the principal investigator or supervisors.
Data Management and Analysis
Data entry was done using EpiData 3.1 and analyzed using Stata version 14.0. Participant characteristics were compared across the two groups and summarized as proportions for categorical variables; and mean with standard deviation (SD) for continuous variables. The incidence of adverse perinatal outcomes was compared across two groups using the Pearson chi-square test for categorical variables and the t-test for continuous variables. A Poisson regression model with robust standard errors was used to estimate the unadjusted and adjusted relative risks (ARR) with a 95% confidence interval (CI) to identify the effects of MNM on adverse perinatal outcomes. The bivariate analysis was used to select independent variables for multivariable regression analysis. Independent variables with a p-value of ≤ .25 were included in the multivariable analysis to control for confounding factors after checking for multicollinearity using variance inflation factors and standard error. A p-value <.05 was used as a cutoff point for a statistically significant association. The command “estat” followed by “gof” was used to obtain the deviance goodness of fit or Pearson goodness of fit test. The results were nonsignificant tests indicating a good-fitting model.
Ethical Approval and Informed Consent
This study took place per the Helsinki Declaration of Research involving human subjects. In addition, the Institutional Health Research Ethical Review Board of the College of Medical and Health Sciences, approved this study. A support letter has been submitted to each hospital for permission. Written informed consent was sought from women before the initiation of the study. Confidentiality and anonymity were assured by using coded identifiers instead of names, and all audio recordings.
Results
During the study period, 261 women with MNM events were identified. Of these, 258 women were included in the exposed group and were matched with 774 women in the unexposed group. Three women with MNM events were excluded because they were discharged before delivery. In total, 1,032 women completed follow up, yielding a response rate of 98.85%.
Sociodemographic Characteristics
The mean age of participants was 26.90 years (SD = 5.07), ranging from 18 to 45 years. The mean ages in the exposed and unexposed groups were 27.93 years (SD = 5.52) and 26.56 years (SD = 4.87), respectively. Regarding residence, 588 women (56.98%) were urban dwellers, including 52.71% of the exposed group and 58.40% of the unexposed group. The majority of participants (n = 1,005; 97.38%) were married, with 93.80% in the exposed group and 98.58% in the unexposed group (Table 2).
Distribution of Sociodemographic Variables Among Exposed and Nonexposed Groups of Women Admitted in Gurage Zone Hospitals, Southwest Ethiopia 2022 (n = 1032).
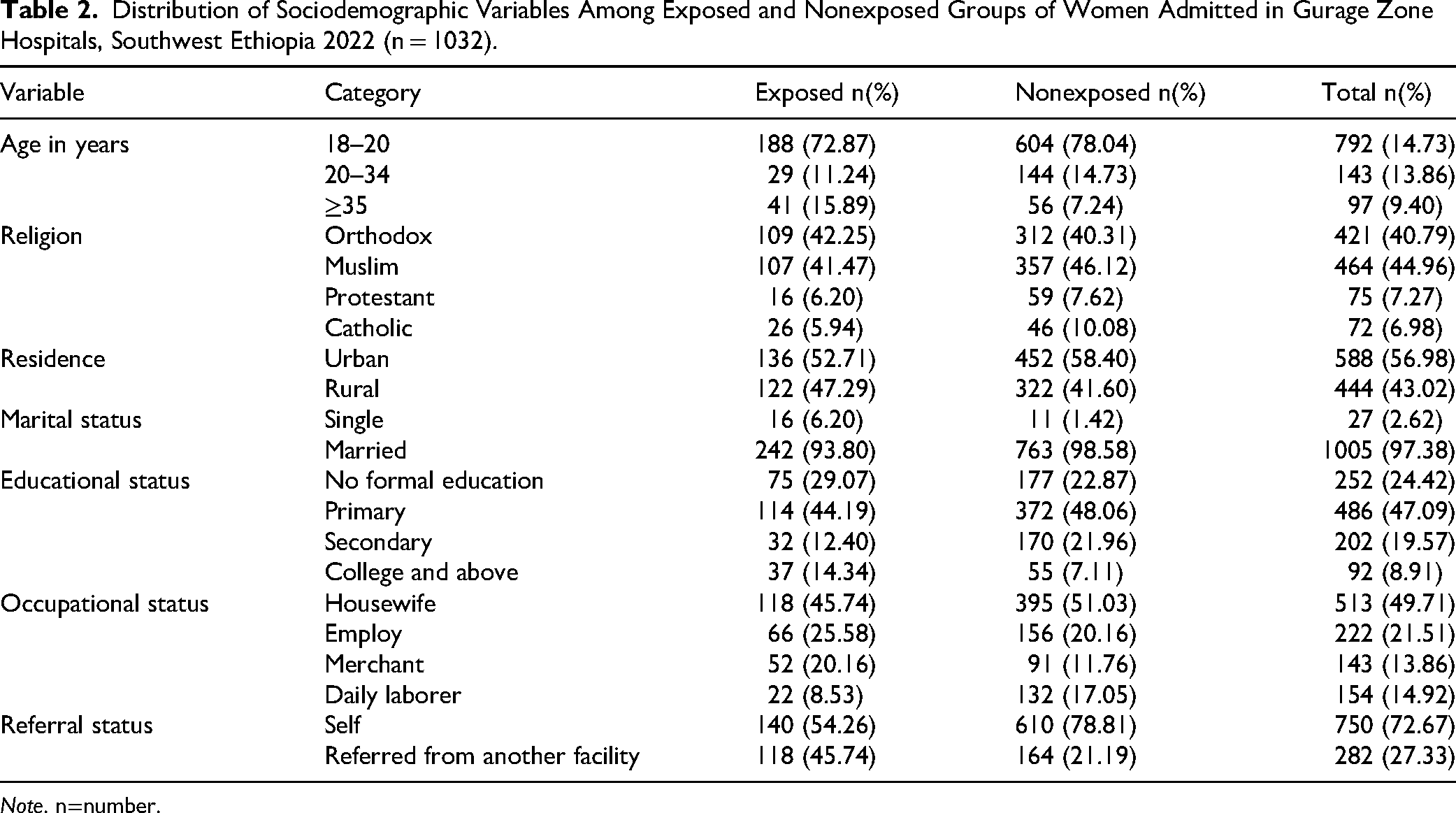
Note. n=number.
Obstetrics, Personal, and Medical History of Participants
The majority of women (n = 919; 89.05%) attended ANC during their current pregnancy, with similar rates observed in the exposed (87.60%) and nonexposed groups (89.53%). Regarding the mode of delivery, 728 women (70.54%) delivered vaginally, with a lower proportion in the exposed group (61.63%) compared with the nonexposed group (73.51%). In terms of parity, 562 women (54.46%) were multiparous, including 60.47% in the exposed group and 52.45% in the nonexposed group. Concerning medical history, 58 women (5.62%) had chronic hypertension (13.18% exposed vs. 3.10% nonexposed), and 13 women (1.26%) had a history of diabetes mellitus (1.16% exposed vs. 1.29% nonexposed) (Table 3).
Distribution of Selected Variables among Exposed and Unexposed Groups of Women Admitted in Gurage Zone Hospitals, Southwest Ethiopia 2022 (n = 1032).

Note. ANC= antenatal care; CS=cesarean section; n=number.
Incidence of Adverse Perinatal Outcomes
Of the 1,032 women included in this study, 201 (19.48%; 95% CI [17.17, 22.01]) experienced a composite adverse perinatal outcome. The incidence of adverse composite perinatal outcomes was significantly higher among women with MNM events compared with those without (37.98% vs. 13.31%, p < .001). Specifically, the incidence of birth asphyxia was greater among newborns of women with near-miss events than among those without (10.47% vs. 2.20%, p < .001). Perinatal mortality was also elevated among women with near-miss events compared with those without (8.53% vs. 2.84%) (Table 4).
Incidence of Adverse Perinatal Outcomes Among Women With Near-Misses and Without Near-Misses Among Women Admitted in Gurage Zone Hospitals, Southwest Ethiopia 2022 (n = 1032).

Note. N=number; NICU=neonatal intensive care unit.
Association b/n Type of Adverse Perinatal Outcomes and Maternal Near-Miss
Admission to the NICU, five-minute birth asphyxia, low birth weight, and early neonatal death were the perinatal outcomes most frequently associated with MNM events. Newborns of women who experienced MNM events had a 10.5-fold higher risk of NICU admission. Similarly, the risk of five-minute birth asphyxia was 4.76 times higher among infants born to these women. The risks of low birth weight and early neonatal death were also elevated, at 4.50 and 4.20 times higher, respectively, among MNM cases (Table 5).
Maternal Near-Miss and Risks of Types of Adverse Perinatal Outcome Among Women Admitted in Gurage Zone Hospitals, Southwest Ethiopia 2022 (n = 1032).
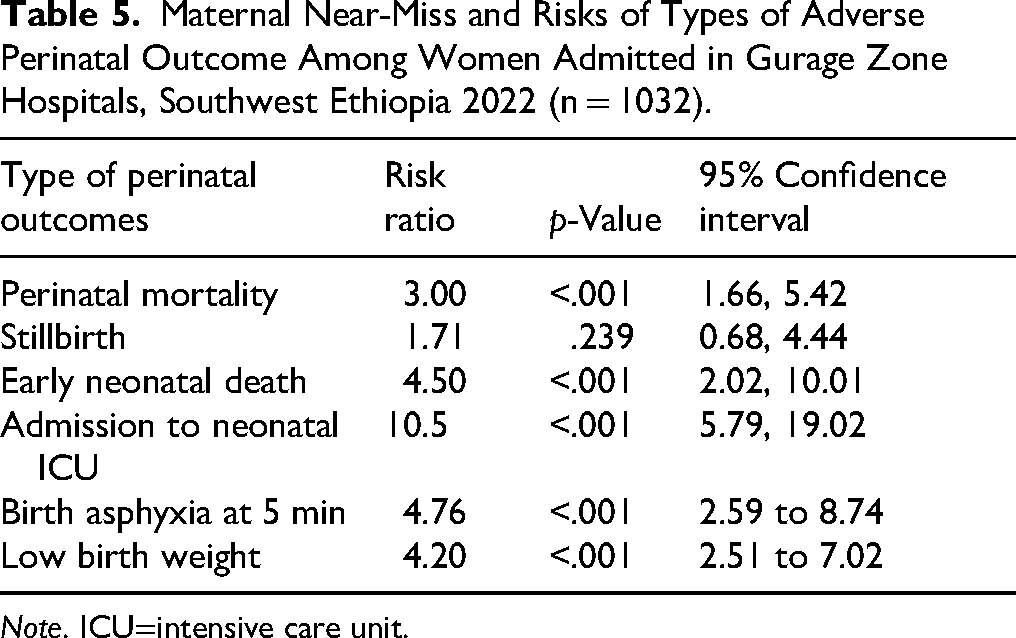
Note. ICU=intensive care unit.
Risk Factors of Composite Adverse Perinatal Outcome
After adjustment for potential covariates, including residence, alcohol consumption, maternal age, history of abortion, history of stillbirth, previous cesarean section, mode of delivery in the index pregnancy, chronic hypertension, and anemia during the index pregnancy, the risk of adverse perinatal outcomes remained significantly higher among women who experienced MNM events (ARR = 2.36, 95% CI [1.74, 3.18]). Additionally, the risk of adverse perinatal outcomes was significantly increased among rural residents (ARR = 1.52, 95% CI [1.14, 2.03]), women with chronic hypertension (ARR = 1.66, 95% CI [1.05, 2.62]), and women with anemia during the index pregnancy (ARR = 1.60, 95% CI [1.10, 2.31]) (Table 6).
Maternal NeariMiss and Risks of Composite Adverse Perinatal Outcome With Other Confounding Variables Among Women Admitted in Gurage Zone Hospitals, Southwest Ethiopia 2022 (n = 1032).

Note. ARR=adjusted relative risk; CI=confidence interval; CRR=crude relative risk; CS=cesarean section.
p < .001;bp = .004; cp < .029; dp=0.013.
Discussion
This study examined the effect of MNM on adverse perinatal outcomes among a cohort of women admitted to hospitals in the Gurage Zone, southwest Ethiopia. Overall, a composite adverse perinatal outcome occurred in 19.48% of deliveries (95% CI = 17.17–22.01). After adjusting for potential covariates, women who experienced MNM events had a significantly higher risk of adverse perinatal outcomes compared with women without MNM.
The incidence of adverse perinatal outcomes in our study is lower than the finding from public hospitals in Addis Ababa (36%) (Liyew et al., 2018). The variation might be due to the difference in the study population and settings. Given that the majority of patients visiting tertiary/referral hospitals in the Addis Ababa study would be high-risk populations compared to our general and district hospitals, the difference is not unexpected.
Incidence of Adverse Perinatal Outcomes
At a statistically significant level, the incidence of NICU admission, early neonatal mortality, preterm birth, low birth weight, and birth asphyxia at five minutes was higher among the exposed group (women with MNM events) compared with the nonexposed group. This finding may be explained by the fact that MNM cases often involve severe obstetric complications—such as severe preeclampsia or eclampsia, obstetric hemorrhage, sepsis, or obstructed labor—which can impair placental function, reduce fetal oxygen supply, or necessitate preterm delivery to preserve maternal health.
In this study, the risks of composite adverse perinatal outcomes were two times higher among women with MNM than those without MNM. An increased risk of adverse perinatal outcomes among women with MNM has been reported in studies from central Ethiopia (Liyew et al., 2018), eastern Ethiopia (Tura et al., 2020), southwest Ethiopia (Aliyi et al., 2021), Nigeria, and Brazil (Adeoye et al., 2013; Oliveira & Costa, 2013). Given life-threatening complications in pregnancy will lead to interventions, like termination of pregnancy before term, this might result in preterm birth and low birth weight an indicator of adverse perinatal outcomes. In addition, MNM events related to (severe preeclampsia) eclampsia, uterine rupture, or obstetric hemorrhage will have a profound effect on the fetus leading to birth asphyxia, intrauterine growth restriction, low birth weight, prematurity, stillbirth, or perinatal mortality, thereby increasing the risks of adverse perinatal outcomes (Berhe et al., 2020; Ness & Sibai, 2006; Ness & Sibai, 2006). This finding indicates the importance of treating underlying maternal complications of MNM early to reduce the effect on adverse perinatal outcomes. Therefore, it is important to render evidence-based intervention for the improvement of maternal health, which leads to an improvement in perinatal outcomes.
Consistent with studies in Ethiopia, the risk of adverse perinatal outcomes was significantly higher among rural residents (Berhie & Gebresilassie, 2016; Liyew et al., 2018). Women residing in rural areas may travel a long distance to get ANC, and skilled delivery services, or will have significant delays, which will be associated with adverse perinatal outcomes (Ickovics et al., 2007).
In this study, women with anemia during the index pregnancy were twice as likely to experience adverse perinatal outcomes. Evidence from previous studies indicates that maternal anemia is associated with an increased risk of preterm birth and related neonatal complications (Beckert et al., 2019) an indicator of adverse perinatal outcomes. Nutritional intervention and iron supplementation during pregnancy may help to prevent and improve anemia during pregnancy. In addition, women with chronic hypertension were more likely to develop adverse perinatal outcomes than women without chronic hypertension. This could be explained by the fact that chronic hypertension in pregnancy increases complications such as placenta abruption and superimposed preeclampsia (Seely & Ecker, 2014), thereby increasing the risks of adverse perinatal outcomes.
Strengths and Limitations of the Study
This study employed a validated sub-Saharan African-adapted (modified WHO) MNM tool to determine exposure status. Multiple perinatal outcomes were assessed, including stillbirth, low birth weight, preterm birth, early neonatal death, perinatal mortality, NICU admission, and birth asphyxia. Although these outcomes differ in clinical severity, they were combined into a composite adverse perinatal outcome due to insufficient sample size to analyze each outcome separately. This approach increased statistical power and reduced the likelihood of chance findings. Additionally, follow up was limited to seven days postpartum or until hospital discharge, whichever occurred first, because of logistical and feasibility constraints. Consequently, early neonatal deaths occurring after discharge may not have been captured.
Implications and Recommendations
The findings of this study have significant implications for nursing practice, particularly in settings where severe maternal morbidity is associated with an increased risk of adverse neonatal outcomes. The higher incidence of adverse outcomes among rural residents highlights the need for nurses to strengthen early recognition of maternal danger signs and to promote timely care-seeking behaviors. Nurses working in peripheral and rural health facilities play a critical role in triage, stabilization, and prompt referral; therefore, improving referral pathways and communication systems may substantially reduce delays in care. Furthermore, the identification of chronic hypertension and anemia as independent predictors of adverse outcomes underscores the importance of comprehensive antenatal screening led by nurses, along with targeted follow up, patient education, and appropriate clinical management to prevent progression to MNM events.
In addition, the higher rates of adverse neonatal outcomes observed among the exposed group indicate gaps across the continuum of emergency obstetric and newborn care. Nurses play a central role in addressing these gaps by ensuring consistent maternal and neonatal monitoring, facilitating timely interventions, and coordinating referrals to higher-level facilities for advanced care. Strengthening the capacity of rural and peripheral health centers through improved diagnostic resources, reliable emergency transport systems, and increased availability of skilled nursing personnel may further enhance timely and effective care delivery. Moreover, integration of maternal and perinatal critical care services is essential, as nurses are often the first providers to assess neonates born to mothers with severe complications and must ensure prompt access to specialized support, including NICUservices.
Conclusions
The incidence of adverse perinatal outcomes was high in this study. MNM was identified as an independent risk factor, even after adjusting for potential covariates. Adverse perinatal outcomes were also significantly more common among rural residents and among women with chronic hypertension or anemia during the index pregnancy. These findings underscore the importance of addressing maternal risk factors to improve perinatal outcomes. Further research is needed to evaluate the appropriateness of interventions and the quality of care to prevent high rates of adverse perinatal outcomes in the future.
Supplemental Material
sj-docx-1-son-10.1177_23779608261444448 - Supplemental material for The Effect of Maternal Near-Miss on Adverse Perinatal Outcomes Among Women Admitted to Hospitals of Gurage Zone, Southwest Ethiopia: A Prospective Cohort Study
Supplemental material, sj-docx-1-son-10.1177_23779608261444448 for The Effect of Maternal Near-Miss on Adverse Perinatal Outcomes Among Women Admitted to Hospitals of Gurage Zone, Southwest Ethiopia: A Prospective Cohort Study by Shegaw Geze Tenaw, Bitew Tefera Zewudie, Bogale Checkole Temere and Daniel Tsega in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608261444448 - Supplemental material for The Effect of Maternal Near-Miss on Adverse Perinatal Outcomes Among Women Admitted to Hospitals of Gurage Zone, Southwest Ethiopia: A Prospective Cohort Study
Supplemental material, sj-docx-2-son-10.1177_23779608261444448 for The Effect of Maternal Near-Miss on Adverse Perinatal Outcomes Among Women Admitted to Hospitals of Gurage Zone, Southwest Ethiopia: A Prospective Cohort Study by Shegaw Geze Tenaw, Bitew Tefera Zewudie, Bogale Checkole Temere and Daniel Tsega in SAGE Open Nursing
Footnotes
Abbreviations
Acknowledgments
We would like to thanks Wolkite University College of Medicine and Health Sciences, Department of Midwifery for allowing us to enroll in this program. We want to thank the public hospitals of the Gurage zone for giving us the necessary information, data collectors, and supervisors.
Ethical Approval and Informed Consent
This study took place per the Helsinki Declaration of Research involving human subjects. In addition, the Institutional Health Research Ethical Review Board of the College of Medical and Health Sciences, Wolkite University approved this study (Ref no. RCSUIL026/14). A support letter has been submitted to each hospital for permission. Written informed consent was sought from women before the initiation of the study.
Authors’ Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Wolkite University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The dataset used or analyzed during this study is available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.