
Abstract
Introduction
This study examined alexithymia, illness-related stigma, and self-esteem among patients with lymphedema to provide evidence for improving self-esteem, enhancing emotional expression, and reducing stigma.
Objectives
To describe levels of alexithymia, illness-related stigma, and self-esteem in patients with lymphedema; examine demographic differences; and test prespecified associations among these variables.
Methods
This was a cross-sectional, questionnaire-based study. A convenience sample of 195 patients with lymphedema receiving treatment at a tertiary oncology hospital in southern China completed questionnaires between October 2020 and February 2021. Instruments included the Toronto Alexithymia Scale, Social Impact Scale, and Rosenberg Self-Esteem Scale. Descriptive statistics summarized patient characteristics and scores. Group differences were tested with t-tests, analysis of variance, and rank-sum tests.
Results
The mean alexithymia score was 56.53 ± 8.43, with externally oriented thinking highest and difficulty describing emotions lowest. Alexithymia differed by education, marital status, residence, income, and activity after onset (p < .05). The mean stigma score was 60.36 ± 11.08, highest for social exclusion and lowest for internalized shame, differing by income, personality, and family relationships (p < .05). The mean self-esteem score was 27.84 ± 4.07, differing by education, employment, residence, income, personality, activity, and family relationships (p < .05). Alexithymia correlated positively with stigma (r = .51, p < .01) and negatively with self-esteem (r = −.65, p < .01). Stigma correlated negatively with self-esteem (r = –.60, p < .01).
Conclusion
Economic discrimination was the strongest correlate of stigma, and income and family relationships were key associated factors. Interventions targeting emotional expression and self-esteem may be relevant for psychosocial support in this population.
Introduction
Lymphedema is one of the most common postoperative complications of malignant tumors. Previous studies have reported that the incidence of secondary lower-limb lymphedema following gynecological cancer surgery ranges from 0% to 69% (Bona et al., 2020), while the incidence after breast cancer surgery is 4.4% to 32.5% (Ahn et al., 2024; Zou et al., 2018). Although lymphedema in oncology settings is most commonly discussed as a postoperative complication of breast and gynecological cancers, lymphedema is a chronic condition with diverse etiologies. In non-oncological contexts, particularly in endemic regions, lymphatic filariasis represents a major cause of chronic lymphedema and has been shown to impose a substantial psychosocial and emotional burden. A recent systematic review highlighted that individuals affected by lymphatic filariasis frequently experience stigma, social isolation, impaired body image, and reduced quality of life (Vasconez-Gonzalez et al., 2025). Considering evidence across different etiologies helps situate illness-related stigma and self-esteem within a broader framework of chronic swelling conditions, while the present study specifically focuses on cancer-related lymphedema in a tertiary oncology center.
Review of Literature
Lymphedema is a chronic condition that may cause physical dysfunction and altered physical appearance. It can impair patients’ daily functioning and social interactions, increase psychological and social barriers, and ultimately reduce quality of life (Anbari et al., 2021; Huang & Wu, 2022).
Alexithymia refers to a deficit in the ability to identify, distinguish, describe emotions, as well as difficulties in expressing inner thoughts and feelings. It is considered a psychological construct associated with emotional dysregulation. Patients with lymphedema often face long-term treatment, and changes in body image may expose them to social scrutiny or discrimination. These experiences can foster illness-related stigma and negatively impact self-esteem. Illness-related stigma refers to the internalized sense of stigma or embarrassment arising from one's disease. Self-esteem, in contrast, reflects an individual's sense of self-worth, and is a key determinant of overall health and mental wellbeing. Picco et al. (2016) demonstrated that illness-related stigma significantly influences self-esteem among patients with mental illness, with higher levels of stigma associated with lower self-esteem, pessimism, and feelings of inferiority.
To date, research on lymphedema has primarily focused on its prevention and management. However, few studies have examined the interrelationships among alexithymia, illness-related stigma, and self-esteem in patients with lymphedema. Therefore, the purpose of this study was to examine levels of alexithymia, illness-related stigma, and self-esteem among patients with lymphedema, to explore demographic differences, and to test the prespecified associations among these variables. We prespecified that alexithymia would be positively associated with stigma and negatively associated with self-esteem, and that stigma would be negatively associated with self-esteem.
Method
Design
This cross-sectional, questionnaire-based study was conducted between October 2020 and February 2021 at the Department of Breast Surgery of a tertiary oncology hospital in southern China.
Patients were recruited from the lymphedema treatment service (outpatient clinic and/or inpatient wards). Eligible patients were approached during routine visits by trained research staff; because convenience sampling was used, selection bias cannot be excluded.
Research Questions
This study addressed the following research questions:
What are the levels of alexithymia, illness-related stigma, and self-esteem among patients with lymphedema? Do alexithymia, illness-related stigma, and self-esteem differ according to demographic and clinical characteristics? What are the associations among alexithymia, illness-related stigma, and self-esteem in patients with lymphedema?
Sample and Eligibility Criteria
Sample
Sample size was determined a priori for the primary correlational analyses. Assuming a small-to-moderate correlation (r = 0.20), a two-sided α of 0.05, and statistical power of 0.80, the required sample size was approximately 194 participants. To allow for incomplete questionnaires, 210 questionnaires were distributed.
A total of 195 participants were included in the final analysis. Fifteen questionnaires were excluded due to inability to complete the questionnaire or substantial missing data. The participant flow is shown in Figure 1.

Flow diagram of participant recruitment and inclusion. Of the 210 questionnaires distributed, 15 were excluded due to inability to complete the questionnaire because of advanced age (n = 5) or substantial missing data (>10% of items missing; n = 10). A total of 195 participants were included in the final analysis.
Inclusion and Exclusion Criteria
Inclusion criteria were as follows:
diagnosis and stage of lymphedema determined by the treating surgeon and lymphedema therapist based on clinical examination (e.g., limb swelling and skin changes) and medical record documentation, consistent with referenced criteria (Bona et al., 2020); age ≥ 18 years; sufficient cognitive and communication abilities to complete the questionnaire; and provision of written informed consent.
Exclusion criteria included:
diagnosis of other systemic malignancies or severe hepatic or renal dysfunction; tumor recurrence or distant metastasis; comorbid ascites, generalized edema, or serous effusion; and history of psychiatric illness or personality disorders.
Instruments
General Information Questionnaire
Based on a review of the literature, the research team developed a self-designed questionnaire to collect demographic and disease-related information. Clinical characteristics (e.g., lymphedema site, duration, and clinical stage) were obtained from medical records and confirmed by the treating team. Lymphedema stage was recorded according to routine clinical staging documented in the medical chart.
Toronto Alexithymia Scale
The Toronto Alexithymia Scale-20 (TAS-20), revised by Bagby and Taylor, is a widely used and reliable measure of alexithymia (Bagby et al., 1994). The scale comprises 20 items across three dimensions: difficulty identifying feelings (items 1, 3, 6, 7, 9, 13, and 14), difficulty describing feelings (items 2, 4, 11, 12, and 17), and externally oriented thinking (items 5, 8, 10, 15, 16, and 18–20). Items are rated on a five-point Likert scale, with items 4, 5, 10, 18, and 19 reverse scored. Higher scores indicate greater alexithymia.
A total score ≥ 61 indicates alexithymia, ≤ 51 indicates non-alexithymia, and scores between 52 and 60 indicate a tendency toward alexithymia. In this study, Cronbach's α coefficient for the total scale was 0.816. The validated Chinese version of the TAS-20 was used (Zhu et al., 2007).
Social Impact Scale
The Social Impact Scale (SIS), developed by Fife and Wright (2000), assesses illness-related stigma in patients with cancer and AIDS. It consists of 24 items across four dimensions: social exclusion, economic discrimination, internalized shame, and social isolation. Items are rated on a four-point Likert scale, with higher scores indicating greater perceived stigma. The total possible score is 96.
Cronbach's α coefficients in previous studies ranged from 0.85 to 0.90; in the present study, Cronbach's α was 0.945. A validated Chinese version of the SIS (C-SIS) was used (Qin et al., 2019).
In this study, we use the term “stigma” to refer to the overall construct measured by the SIS total score, whereas “internalized shame” refers specifically to the name of one SIS subscale.
Rosenberg Self-Esteem Scale
The Rosenberg Self-Esteem Scale (RSES), developed by Rosenberg in 1965 (Rosenberg, 1965), is a 10-item instrument comprising five positively worded and five negatively worded items. Items are rated on a four-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). Total scores range from 10 to 40, with higher scores indicating higher self-esteem.
In this study, Cronbach's α coefficient was 0.847. The validated Chinese version of the RSES was used (Jiang et al., 2023).
Ethical Considerations
This study was approved by the ethics committee of a tertiary university-affiliated oncology hospital. All participants provided written informed consent prior to participation. Data were collected anonymously using a structured, self-administered questionnaire under the guidance of the lymphedema treatment team.
Participants received standardized instructions, and the purpose, significance, and confidentiality of the study were explained in detail. Research staff received standardized training and followed scripted procedures. Assistance was limited to clarification of item meanings without suggesting responses to minimize information bias. Questionnaires were distributed and collected on-site, with immediate verification for completeness. Data entry was performed independently by two researchers and cross-checked for accuracy. The questionnaires and scales used in this study are provided as Supplemental materials S4–S6.
Statistical Analysis
All statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Categorical variables were summarized as frequencies and percentages, and continuous variables as means and standard deviations. Normality was assessed using the Shapiro–Wilk test and graphical inspection, and homogeneity of variance was assessed using Levene's test. Group differences were examined using independent-samples t-tests or one-way analysis of variance (ANOVA) for approximately normally distributed variables, and rank-sum tests for non-normally distributed variables, as appropriate.
Pearson correlation analysis was used to examine associations among alexithymia, illness-related stigma, and self-esteem for approximately normally distributed scale totals; otherwise, Spearman’s correlation was considered. Multiple stepwise regression analyses were conducted for exploratory purposes to identify factors associated with alexithymia, stigma, and self-esteem. Entry and removal criteria were set at p < .05 and p > .10, respectively. Multicollinearity was assessed using variance inflation factors, and residual diagnostics were examined.
Given the number of comparisons performed, subgroup analyses were considered exploratory and interpreted with caution. Missing data were handled using listwise deletion for analyses involving the respective variables. All statistical tests were two-sided, and p < .05 was considered statistically significant. Where applicable, post hoc comparisons were performed using the least significant difference (LSD) test; these subgroup comparisons were considered exploratory.
Results
General Characteristics of Patients (Sample Characteristics)
A total of 195 patients with lymphedema were included in this study. Given the clinical context of a tertiary oncology center, the sample was predominantly female, and the mean age was 55.60 ± 11.32 years. The general demographic, sociological, and clinical characteristics of the patients are summarized in Table 1. The distributions of alexithymia, stigma, and self-esteem scores are illustrated in Figure 2. Given the highly imbalanced sex distribution and the small cell sizes in certain subgroups (e.g., male participants and those aged >70 years), all subgroup comparisons are considered exploratory and should be interpreted with caution. The following sections present results addressing the study research questions.

Box plots showing the distributions of alexithymia (TAS-20 total score), illness-related stigma (SIS total score), and self-esteem (RSES total score) among patients with lymphedema. The boxes represent the IQR, the horizontal line within each box indicates the median, and whiskers extend to 1.5 × IQR. Circles denote individual outliers. IQR=interquartile range; RSES= Rosenberg Self-Esteem Scale; SIS= Social Impact Scale; TAS-20=Toronto Alexithymia Scale-20.
General Characteristics of Patients With Lymphedema (n = 195).

Current Status and Univariate Analysis of Alexithymia in Patients With Lymphedema
Current Status of Alexithymia
The mean total alexithymia score was 56.53 ± 8.43. Among the subscales, externally oriented thinking had the highest score (22.71 ± 3.03), followed by difficulty identifying feelings (20.02 ± 4.57), while difficulty describing feelings had the lowest score (13.80 ± 2.55). Details are shown in Table 2.
Scores of Alexithymia in Patients With Lymphedema (n = 195, mean ± SD).

Univariate Analysis of Alexithymia in Patients With Lymphedema
One-way ANOVA was performed to assess differences in alexithymia scores according to patients’ demographic and clinical characteristics. The results showed that education level, marital status, living arrangement, place of residence, monthly household income, and main activity pattern after lymphedema onset were significantly associated with alexithymia scores (p < .05). Lower education levels and lower monthly income were associated with higher alexithymia scores. Married patients, those living with spouses or children, and patients who primarily stayed at home also had higher scores. Details are presented in Supplemental Table S1.
Current Status and Univariate Analysis of Stigma in Patients With Lymphedema
Current Status of Stigma
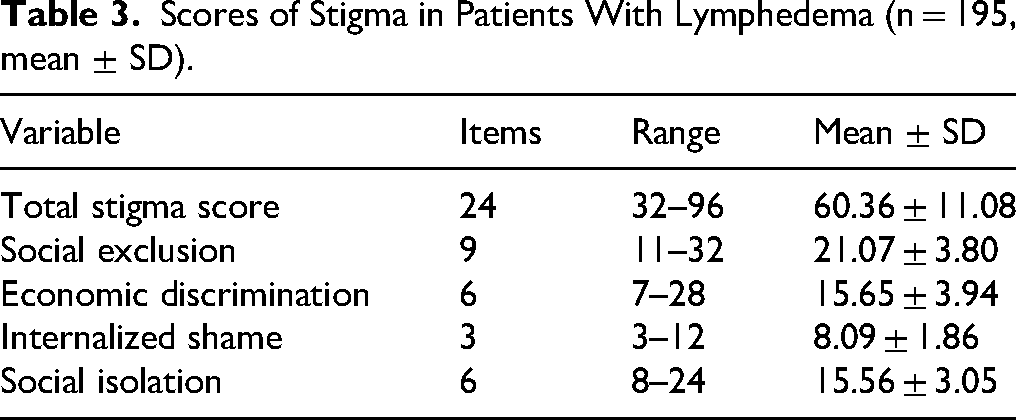
The mean total stigma score was 60.36 ± 11.08. Among the subscales, social exclusion scored the highest (21.07 ± 3.80), followed by economic discrimination (15.65 ± 3.94) and social isolation (15.56 ± 3.05), while internalized shame scored the lowest (8.09 ± 1.86). Details are shown in Table 3.
Scores of Stigma in Patients With Lymphedema (n = 195, mean ± SD).
Univariate Analysis of Stigma
One-way ANOVA was performed to evaluate the effects of demographic and clinical factors on stigma scores. The results showed that monthly household income, comorbidity with diabetes, personality type, and family relationships were associated with stigma levels (p < .05). Patients with lower monthly income, diabetes, introverted personality, and poor or moderate family relationships had significantly higher stigma scores. The results are summarized in Supplemental Table S2.
Status and Univariate Analysis of Self-Esteem in Patients With Lymphedema
Status of Self-Esteem
The mean self-esteem score was 27.84 ± 4.07. Among individual items, item 2 scored the highest (3.14 ± 0.62), followed by item 4 (3.01 ± 0.63), while item 8 scored the lowest (1.87 ± 0.53). Details are presented in Table 4.
Self-Esteem Scores and Item-Level Results in Patients With Lymphedema (n = 195, Mean ± SD).

Univariate Analysis of Self-Esteem
One-way ANOVA showed that education level, occupational status, place of residence, monthly household income, personality, main activity level after lymphedema onset, and family relationships were significantly associated with self-esteem scores (p < .05). Higher educational attainment, employment, urban residence, higher monthly income, extroverted personality, frequent outdoor activity, and good family relationships were associated with higher self-esteem. Results are summarized in Supplemental Table S3.
Correlation Between Alexithymia, Stigma, and Self-Esteem
Normality assumptions for the total scores of the study scales were assessed and met; therefore, Pearson correlation coefficients are reported. Pearson correlation analysis showed a significant positive correlation between alexithymia and stigma (r = .51, p < .01). Alexithymia was negatively correlated with self-esteem (r = −.65, p < .01), and stigma was also negatively correlated with self-esteem (r = −.60, p < .01). Results are presented in Table 5.
Correlation Analysis Among Alexithymia, Stigma, and Self-Esteem in Patients With Lymphedema (n = 195).

Note. *p* < .05. **p** < .01 (two-tailed).
DIF = difficulty identifying feelings; DDF = difficulty describing feelings; EOT = externally oriented thinking.
Influencing Factors of Stigma in Patients With Lymphedema
Multiple linear regression analyses were conducted for exploratory purposes to identify factors associated with alexithymia, illness-related stigma, and self-esteem. Only the model for illness-related stigma yielded a stable solution and is therefore reported in detail. The total stigma score was used as the dependent variable, with monthly household income and family relationships (significant in univariate analysis) entered as independent variables. Monthly household income and family relationships entered the final model. The regression model was statistically significant (F(2, 192) = 9.22, p < .001), explaining 13.5% of the variance in stigma scores. Results are shown in Table 6.
Multiple Regression Analysis of Stigma in Patients With Lymphedema (n = 195).

Model summary: R2 = 0.135.
Discussion
General Characteristics of Patients
In this study, 195 patients with lymphedema were included, the majority of whom were female and middle-aged. Most patients were married and living with a spouse, suggesting relatively stable family circumstances. A total of 139 patients resided in urban areas, and the majority had attained a college-level education or higher. The largest occupational group was employed individuals (40.82%). More than half of the patients reported a monthly household income of ≥ 5,000 RMB, indicating relatively favorable socioeconomic and educational backgrounds.
The anatomical sites of lymphedema in this cohort were diverse, including 118 cases of upper-limb lymphedema, 50 cases of lower-limb lymphedema, 21 cases of lower-limb lymphedema combined with perineal involvement, three cases of breast lymphedema, and one case of abdominal lymphedema. Most patients were classified as stage I or II lymphedema, with 109 cases having a disease duration of > 6 months. Personality traits were predominantly extroverted (n = 74) or introverted (n = 41), with 80 patients classified as neutral. Following the onset of lymphedema, most patients primarily stayed at home or occasionally went out. Approximately 75% were able to manage daily living independently, and 83.16% reported good family relationships.
Current Status and Univariate Analysis of Alexithymia in Patients With Lymphedema
Current Status of Alexithymia
Alexithymia can seriously compromise treatment adherence, mental health, and quality of life among patients with cancer and is often expressed through somatic symptoms. Lymphedema is a common postoperative complication after treatment for malignant tumors and remains incurable, imposing substantial psychological stress and trauma. In clinical practice, however, the role of alexithymia in the onset, progression, treatment response, and prognosis of lymphedema has been partly overlooked.
In the present study, the mean total alexithymia score was 56.53 ± 8.43. Among subscales, externally oriented thinking had the highest mean score (22.71 ± 3.03), followed by difficulty identifying feelings (20.02 ± 4.57), whereas difficulty describing feelings had the lowest mean score (13.80 ± 2.55). The total score was slightly higher than that reported by Xu et al. (2017) among patients with cancer (55.37 ± 10.97), suggesting a moderately high level of alexithymia in this population. These findings may reflect multiple stressors: the physical and psychological burden of cancer and surgery; postoperative lymphedema with visible swelling; changes in daily routines; fear of negative social evaluation; and concerns regarding self-esteem and discrimination. Such factors may foster social withdrawal and emotional suppression. In addition, adjuvant radiotherapy and chemotherapy can further heighten both physical and psychological stress, blurring patients’ ability to differentiate somatic discomfort from emotional distress and hindering authentic emotional expression.
Given the long-term nature of lymphedema management and the need for comprehensive postoperative care, timely recognition and intervention for alexithymia are warranted to mitigate negative affect and promote overall health and quality of life.
Univariate Analysis of Alexithymia
Univariate analyses indicated that education level, marital status, place of residence, monthly household income, and primary activity pattern after the onset of lymphedema were significantly associated with alexithymia scores (p < .05). Lower educational attainment was associated with higher alexithymia, consistent with findings in breast cancer reported by Eskelinen and Ollonen (2011) and evidence that education enhances cognitive and descriptive abilities relevant to emotional processing (Nardelli et al., 2013). Married patients and those living with spouses and children had higher alexithymia scores than unmarried or single individuals, possibly due to perceived family burden and inhibited emotional disclosure within family roles. Lower monthly household income was associated with higher alexithymia, aligning with Peters and Lumley (2007); financial strain from surgery and long-term treatment may intensify stress and impede accurate recognition of emotional versus physical sensations. Patients who primarily stayed at home had the highest alexithymia scores compared with those who went out sometimes or frequently, suggesting self-concealment of the affected limb and avoidance behaviors linked to fear of stigmatizing attention.
Current Status and Univariate Analysis of Stigma in Patients With Lymphedema
Current Status of Stigma
The mean total stigma score was 60.36 ± 11.08. Among the subscales, social exclusion showed the highest mean score (21.07 ± 3.80), followed by economic discrimination (15.65 ± 3.94) and social isolation (15.56 ± 3.05), with internalized shame scoring the lowest (8.09 ± 1.86). The predominance of social exclusion may relate to the demographic composition of the sample (predominantly female and employed) and heightened salience of body image. Compression bandaging—a core component of lymphedema management—is visible and difficult to conceal, potentially disrupting social and occupational functioning. Daily self-management can feel relentless; repeated exposure to visible bandages may elicit anxiety, hypervigilance to perceived social labeling, and reduced social participation, thereby reinforcing social isolation. Economic discrimination may be driven by the long-term out-of-pocket costs of materials and treatment not covered by health insurance, increasing financial pressure and negative affect.
Univariate Analysis of Stigma
Univariate analyses showed that monthly household income, personality type, and family relationships were significantly associated with stigma scores (p < .05). Patients with lower monthly income reported higher stigma, consistent with Dey et al. (2016) and Kaur (2015), who noted that economic disadvantage is linked to poorer disease understanding, greater exposure to discrimination, and heightened stigma. In this study, the need for persistent daily management may further amplify perceived stigma under financial strain. Personality also mattered: patients with introverted traits reported higher stigma than those with extroverted or neutral traits, suggesting greater social distance, less emotional disclosure, and increased vulnerability to anxiety and pessimism. Poor or moderate family relationships were associated with higher stigma, whereas good family relationships were protective, echoing findings by Witt (Witt & DeLeire, 2009) and Repetti (Repetti et al., 2011) that supportive family environments facilitate adaptive appraisal and better psychological adjustment.
Current Status and Univariate Analysis of Self-Esteem in Patients With Lymphedema
Current Status of Self-Esteem
Self-esteem reflects an individual's evaluative judgment of self-worth and self-acceptance. In this study, the mean self-esteem score was 27.84 ± 4.07, indicating a moderate level overall. Item 2 (“I feel that I have a number of good qualities”) had the highest mean score (3.14 ± 0.62), followed by item 4 (3.01 ± 0.63), whereas item 8 (“I wish I could have more respect for myself”) had the lowest (1.87 ± 0.53). Long-term adherence to treatment can engender fear, denial, and inferiority; concerns about visible bandaging during social encounters may trigger embarrassment, avoidance (e.g., wearing loose or long clothing to hide swelling/bandages), and reduced social interaction—factors likely to undermine self-esteem.
Univariate Analysis of Self-Esteem
Education level, occupational status, place of residence, monthly household income, personality, primary activity level after lymphedema onset, and family relationships were significantly associated with self-esteem (p < .05). Higher education was associated with higher self-esteem, likely reflecting better access to disease-related knowledge and coping strategies. Employed patients reported higher self-esteem than unemployed patients, and urban residents scored higher than those living in towns or the countryside. Higher monthly household income was linked to higher self-esteem, whereas low-income patients may experience guilt or perceived family burden. Extroverted personality, frequent outdoor activity, and good family relationships were all associated with higher self-esteem. Given that lymphedema requires long-term, largely self-funded management in many settings, these findings underscore the cumulative psychosocial burden and its potential to lower self-esteem through social avoidance and recurrent symptom distress.
Correlations Among Alexithymia, Stigma, and Self-Esteem
Correlation analyses showed that alexithymia was positively associated with stigma (r = .51, p < .01) and negatively associated with self-esteem (r = −.65, p < .01). Stigma was also negatively associated with self-esteem (r = –.60, p < .01). Compression bandaging—a key element of comprehensive decongestive therapy—reduces swelling but can affect psychosocial adaptation. Under professional guidance and with family support, structured rehabilitation, regular follow up, and psychological adjustment may help address stigma and support self-esteem. Consistent with Lysaker et al. (2008), higher stigma is linked to lower self-esteem; visible manifestations of lymphedema may worsen body-image concerns and perceived social exclusion, reinforcing low self-worth. These results suggest that comprehensive care may consider incorporating supportive strategies that address self-esteem and perceived stigma, alongside routine lymphedema management.
Factors Influencing Stigma in Patients With Lymphedema
Multiple linear regression was used to identify predictors of stigma, with the total stigma score as the dependent variable and only monthly household income and family relationships (significant in univariate analyses) entered as independent variables. Monthly household income and family relationships entered the final model and jointly explained 13.5% of the variance in stigma (model F(2, 192) = 9.22, p < .001). These findings indicate that financial resources and family dynamics are major correlates of stigma among patients with lymphedema. These relationships are summarized in the conceptual framework presented in Supplemental Figure S1.
Implications for Practice
Given the prolonged course of lymphedema, comprehensive care should address both physical rehabilitation and psychosocial adaptation. Visible bandaging can discourage social engagement; without supportive strategies and self-management skills, avoidance may worsen symptoms and reinforce stigma. Professional lymphedema therapists should provide timely psychoeducation, skills training for home-based care, and emotional regulation strategies, while encouraging peer exchange and family participation to address patients’ psychological needs and reduce illness-related stigma. In the Chinese cultural context, family relationships may be related to emotional disclosure and coping styles, and may be associated with perceived stigma and self-esteem. Supportive family environments have been reported to be associated with lower stigma, whereas strained family relationships may be linked to greater self-blame and avoidance. These associations may contribute to the internalization of negative beliefs.
Strengths and Limitations
This study has several strengths, including the use of validated instruments, a clearly defined clinical population, and a theoretically grounded examination of emotional and psychosocial factors in lymphedema. Several limitations should be acknowledged. First, this was a single-center, cross-sectional study, which limits causal inference and generalizability. Second, the sample was predominantly female. This imbalance largely reflects the clinical context of a tertiary cancer center, where most patients with lymphedema are breast cancer survivors following surgical treatment. Accordingly, the predominance of female participants is more likely attributable to disease distribution rather than sampling bias. Nevertheless, some subgroup sizes (e.g., male participants, n = 3) were very small, and sex-specific comparisons should be interpreted with caution. Future multicenter studies including patients with lymphedema of diverse etiologies are warranted to improve representativeness. Although the overall sample size was adequate for correlational analyses, the study was underpowered for some subgroup comparisons due to small cell sizes.
Conclusions
Patients with lymphedema demonstrated moderate levels of alexithymia, stigma, and self-esteem. Alexithymia was positively associated with stigma and negatively associated with self-esteem, and stigma was inversely associated with self-esteem. Primary correlates of alexithymia included activity patterns after lymphedema onset; stigma was chiefly associated with monthly household income and family relationships; and self-esteem was associated with monthly income, post-onset activity patterns, and family relationships. Long-term negative affect may be associated with reduced emotional expression, which could be linked to higher stigma and lower self-esteem. These interpretations should be viewed cautiously given the cross-sectional design. Healthcare providers may consider providing timely guidance, mobilizing family involvement and social support, and encouraging appropriate emotional expression to support self-esteem and potentially mitigate illness-related stigma.
Supplemental Material
sj-docx-2-son-10.1177_23779608261442627 - Supplemental material for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study
Supplemental material, sj-docx-2-son-10.1177_23779608261442627 for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study by Qiaoling Zhong, Yuezhou Guo, Feng Liu, Qinghua Luo, Huizhen Zhang, Jinlan Li and Lijuan Zhang in SAGE Open Nursing
Supplemental Material
sj-docx-3-son-10.1177_23779608261442627 - Supplemental material for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study
Supplemental material, sj-docx-3-son-10.1177_23779608261442627 for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study by Qiaoling Zhong, Yuezhou Guo, Feng Liu, Qinghua Luo, Huizhen Zhang, Jinlan Li and Lijuan Zhang in SAGE Open Nursing
Supplemental Material
sj-docx-4-son-10.1177_23779608261442627 - Supplemental material for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study
Supplemental material, sj-docx-4-son-10.1177_23779608261442627 for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study by Qiaoling Zhong, Yuezhou Guo, Feng Liu, Qinghua Luo, Huizhen Zhang, Jinlan Li and Lijuan Zhang in SAGE Open Nursing
Supplemental Material
sj-docx-5-son-10.1177_23779608261442627 - Supplemental material for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study
Supplemental material, sj-docx-5-son-10.1177_23779608261442627 for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study by Qiaoling Zhong, Yuezhou Guo, Feng Liu, Qinghua Luo, Huizhen Zhang, Jinlan Li and Lijuan Zhang in SAGE Open Nursing
Supplemental Material
sj-docx-6-son-10.1177_23779608261442627 - Supplemental material for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study
Supplemental material, sj-docx-6-son-10.1177_23779608261442627 for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study by Qiaoling Zhong, Yuezhou Guo, Feng Liu, Qinghua Luo, Huizhen Zhang, Jinlan Li and Lijuan Zhang in SAGE Open Nursing
Supplemental Material
sj-docx-7-son-10.1177_23779608261442627 - Supplemental material for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study
Supplemental material, sj-docx-7-son-10.1177_23779608261442627 for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study by Qiaoling Zhong, Yuezhou Guo, Feng Liu, Qinghua Luo, Huizhen Zhang, Jinlan Li and Lijuan Zhang in SAGE Open Nursing
Supplemental Material
sj-docx-8-son-10.1177_23779608261442627 - Supplemental material for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study
Supplemental material, sj-docx-8-son-10.1177_23779608261442627 for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study by Qiaoling Zhong, Yuezhou Guo, Feng Liu, Qinghua Luo, Huizhen Zhang, Jinlan Li and Lijuan Zhang in SAGE Open Nursing
Supplemental Material
sj-docx-9-son-10.1177_23779608261442627 - Supplemental material for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study
Supplemental material, sj-docx-9-son-10.1177_23779608261442627 for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study by Qiaoling Zhong, Yuezhou Guo, Feng Liu, Qinghua Luo, Huizhen Zhang, Jinlan Li and Lijuan Zhang in SAGE Open Nursing
Supplemental Material
sj-docx-10-son-10.1177_23779608261442627 - Supplemental material for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study
Supplemental material, sj-docx-10-son-10.1177_23779608261442627 for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study by Qiaoling Zhong, Yuezhou Guo, Feng Liu, Qinghua Luo, Huizhen Zhang, Jinlan Li and Lijuan Zhang in SAGE Open Nursing
Supplemental Material
sj-docx-11-son-10.1177_23779608261442627 - Supplemental material for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study
Supplemental material, sj-docx-11-son-10.1177_23779608261442627 for Correlation Between Alexithymia, Illness-Related Stigma, and Self-Esteem in Patients With Lymphedema: A Cross-Sectional Study by Qiaoling Zhong, Yuezhou Guo, Feng Liu, Qinghua Luo, Huizhen Zhang, Jinlan Li and Lijuan Zhang in SAGE Open Nursing
Footnotes
Acknowledgments
The authors would like to express their gratitude to all colleagues who contributed indirectly to this work. No specific funding or institutional support was received.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Sun Yat-sen University Cancer Center (approval no.: B2025-259-01). Written informed consent was obtained from all participants prior to participation.
Author Contributions
QZ, YG, and FL conceived and designed the study, performed data analysis, and drafted the manuscript. QL and HZ contributed to data acquisition and preprocessing. JL and LZ supervised the research, provided critical revisions, and approved the final version for publication. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are not publicly available due to ethical restrictions but are available from the corresponding author on reasonable request.
Use of AI Software
The authors did not use AI-assisted technologies in the preparation of this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.