
Abstract
Introduction
Nurses frequently encounter high incidences of Burnout Syndrome precipitated by excessive workloads, taxing emotional demands, and the inherent strain of prolonged patient interactions. Furthermore, female nurses often experience compounded stress arising from the dual burden of professional obligations and domestic responsibilities. Consequently, the implementation of a caring-based QNWL intervention is imperative; by integrating carative principles, healthcare institutions can fortify emotional resilience, mitigate occupational stress, and ultimately optimize the standard of clinical care.
Objective
To evaluate the efficacy of the Caring-Based QNWL Program in mitigating burnout syndrome and enhancing professional performance.
Methods
This quasi-experimental study employed a pretest–posttest design to evaluate outcomes among sixty-six female nurses (n = 66), who were equally distributed into intervention and control groups (n = 33 each). The intervention group underwent an 8-week Caring-Based QNWL program, whereas the control group received standard institutional care. To assess the primary variables, the Maslach Burnout Inventory was utilized to measure burnout levels, while nursing performance was evaluated across five distinct dimensions. Data analysis was conducted using the Wilcoxon Signed-Rank and Mann–Whitney U tests.
Results
The implementation of the program significantly reduced Burnout Syndrome, with mean scores decreasing from 43.21 ± 9.688 (pretest) to 38.82 ± 6.729 (posttest), p = .003. Nurse professional performance improved significantly, with scores rising from 66.85 ± 6.95 to 70.88 ± 4.03, p < .001. In contrast, the control group showed no significant changes (Burnout: p = .203; performance: p = .301). Between-group comparison confirmed significant differences in burnout (p = .009) and performance (p = .001) after the program.
Conclusions
The Caring-Based Quality of Nursing Work Life (QNWL) program is an effective approach for reducing burnout syndrome and improving professional performance among nurses. Through the systematic integration of carative values into routine clinical practice, this program supports psychological well-being and individual productivity and can be adapted for sustainable implementation across diverse healthcare settings.
Introduction
Nurses are highly susceptible to burnout syndrome, primarily driven by excessive workloads and the emotional strain of prolonged patient interactions. Globally, the nursing profession exhibits some of the highest rates of occupational burnout; prevalence estimates range from 30% to 60% across OECD countries. Notably, with females comprising up to 79% of the nursing workforce, evidence suggests that female nurses experience significantly higher burnout levels than their male counterparts. This disparity is often attributed to a complex interplay of biological factors, occupational demands, and family stressors (Alsharari, 2019) Work–family conflict is consistently identified as a major contributor to psychological distress, reduced job satisfaction, and impaired performance among female nurses (Rosyida et al., 2024). Nevertheless, recent evidence suggests that work–family conflict does not function as a standalone predictor of Quality of Nursing Work Life (QNWL) unless it interacts with job stress, indicating a multifactorial mechanism influencing emotional well-being (Roberts et al., 2024). In this context, QNWL encompasses multidimensional factors such as job satisfaction, occupational stress, and work-life balance—all of which collectively determine nurses’ emotional resilience and productivity.
In Indonesia, burnout remains a substantial concern within the healthcare sector; approximately 58.3% of nurses report symptoms, predominantly ranging from mild to moderate stress. Recent research indicates that female nurses, in particular, may exhibit lower levels of caring behavior, which poses a potential risk to patient satisfaction and the overall quality of care (Juanamasta et al., 2024). This is further supported by a 2021 hospital-based survey, which revealed that while general patient satisfaction was relatively high at 79%, instances of dissatisfaction were frequently linked to a perceived lack of empathy and clinical compassion from nursing staff.
Empirical studies indicate that high workload, aggressive client behavior, role ambiguity, and limited resources compounded by demographic factors such as gender, age, and salary contribute significantly to burnout among nurses and support workers (Chireh et al., 2025; Putra, Andayani et al., 2021; Putra, Sutadi et al., 2021). In line with these findings, a consistent body of literature suggests that poor QNWL and high work–family conflict are intrinsically linked to increased burnout and diminished care quality (Widayati et al., 2020). As a multidimensional construct, QNWL encompasses structural aspects including work design, job control, and the physical workplace environment (Nursalam et al., 2020). Consequently, interventions aimed at enhancing QNWL—such as workload adjustments, increased autonomy, and caring-based reward systems—are essential to strengthening emotional resilience among healthcare professionals (Putra, Andayani et al., 2021; Putra, Sutadi et al., 2021).
Theoretical foundations rooted in Watson's Theory of Human Caring emphasize that meaningful nurse–patient interactions promote emotional strength, compassion, and healing (Babaei et al., 2025). In alignment with this, QNWL has been found to significantly influence nurse performance (Nursalam et al., 2020), while multiple studies document a negative correlation between QNWL and burnout (Jarzynkowski et al., 2021). Burnout, in turn, is known to reduce care quality and threaten patient safety (Pujiyanto & Hapsari, 2021), particularly when emotional exhaustion diminishes the caring behaviors essential to nursing (Rohita, 2022). If unaddressed, burnout compromises psychological well-being, clinical performance, and organizational outcomes (Dall’Ora et al., 2020). Despite this evidence, most existing interventions remain generic, failing to incorporate gender-sensitive components that address the unique vulnerabilities of female nurses.
This study evaluates the effectiveness of a Caring-Based QNWL intervention, which integrates Watson's ten carative factors to mitigate Burnout Syndrome and enhance nursing performance. Focusing on female nurses is justified by their representation of over 90% of the workforce in the surveyed hospitals and their documented susceptibility to emotional strain. This vulnerability often stems from the interplay between work-family conflict and occupational stress (Roberts et al., 2024). Consequently, by addressing this specific demographic, the study seeks to develop targeted and equitable workforce interventions.
Beyond its local relevance, a caring-based QNWL framework holds potential for broader application across diverse healthcare settings. By grounding the intervention in universally applicable caring principles such as emotional support, reflective practice, and work-life integration, this model allows contextual adaptation while preserving its core theoretical foundation. Such adaptability is particularly important in healthcare systems facing increasing workforce strain and gender related work family pressures.
Review of Literature
QNWL and Burnout
The Quality of Nursing Work Life (QNWL) is a multidimensional concept reflecting nurses’ job satisfaction and their ability to function effectively in the workplace while maintaining personal well-being. According to Brooks and Anderson (2005), QNWL encompasses four primary dimensions: work-life/home-life balance, work design, work context, and work world. These dimensions are crucial in shaping nurses’ overall professional experiences and performance in clinical settings. Consequently, a high QNWL has been linked to enhanced job satisfaction, reduced turnover rates, and improved quality of care (Nursalam et al., 2020). Conversely, global evidence demonstrates that burnout—characterized by emotional exhaustion, depersonalization, and reduced personal accomplishment—remains highly prevalent across healthcare systems (Al Maqbali et al., 2021; Dubale et al., 2019). This phenomenon adversely affects nurse well-being, patient safety, and clinical outcomes (Dall’Ora et al., 2020), further highlighting the critical need for supportive work environments and structured interventions.
Gender Differences and Work–Family Pressures
Female nurses often face heightened vulnerability to burnout due to overlapping professional demands and family responsibilities, which intensify work–family conflict (Hwang & Yu, 2021). This dual burden contributes to emotional strain and diminished resilience compared with their male counterparts (Kelly et al., 2021). Consequently, despite their overrepresentation in the nursing workforce, interventions specifically addressing the gendered nature of burnout remain limited (Hwang & Yu, 2021). Furthermore, research consistently indicates that work–family pressures are a major predictor of psychological fatigue, job disengagement, and poor performance among female nurses (Zhang et al., 2018), underscoring the critical need for gender-sensitive institutional programs.
Caring-Based Interventions
One of the most promising approaches to addressing burnout is the integration of caring behavior into the work environment. Watson's Human Caring Theory offers a comprehensive model grounded in ten caritas processes—including love, hope, sensitivity, and spiritual growth—which align with the interpersonal and emotional demands of nursing. These factors provide a robust foundation for developing holistic interventions. Within this framework, nurse managers play a central role in fostering environments that mitigate emotional exhaustion and enhance personal accomplishment (Shen et al., 2020). Complementing this, Swanson's Caring Theory highlights five essential processes: knowing, being with, doing for, enabling, and maintaining belief (Gürsoy & Yeşildere Sağlam, 2021). These dimensions promote empathetic nurse-patient interactions, which are linked to reduced stress and increased job engagement. However, while many interventions draw upon these frameworks, they often remain generic, failing to account for the unique pressures faced by female nurses, such as the dual burden of professional and domestic roles.
Several large-scale, cross-cultural studies have investigated the QNWL. For instance, research across OECD countries and WHO data highlight burnout as a critical global issue (Dall’Ora et al., 2020; Li et al., 2022). Specifically, a study among critical care nurses in Jordan revealed moderate QNWL levels, which were significantly influenced by environmental and physiological factors such as noise and sleep quality (Alzoubi et al., 2024). Furthermore, systematic reviews and meta-analyses demonstrate that interventions—particularly mindfulness and caring-based programs—effectively reduce burnout while enhancing nurse well-being and performance (Kang & Myung, 2022). Consequently, these findings underscore the necessity for culturally adapted, sustainable interventions, such as the Caring-Based QNWL Program developed in this study.
The integration of Watson's carative factors with the four dimensions of QNWL presents a novel and holistic intervention framework. Female nurses, who constitute the majority of the nursing workforce, are particularly susceptible to burnout syndrome due to the competing demands of professional and domestic responsibilities (Hwang & Yu, 2021). Nevertheless, few interventions have been specifically tailored for this demographic using a caring-based QNWL approach. The present study addresses this gap by developing and evaluating a ‘Caring-Based QNWL Program’ that synthesizes QNWL theory with Watson's Human Caring principles. This program aims to enhance all dimensions of QNWL while simultaneously mitigating burnout symptoms and optimizing clinical performance. By prioritizing female nurses, this study acknowledges their unique professional challenges and provides a gender-sensitive, evidence-based intervention to improve both nurse well-being and patient outcomes (Figure 1).

Research framework.
Methods
Study Design and Setting
A quasi-experimental design was employed, utilizing a non-randomized cluster-based allocation with pre- and posttest assessments administered to both intervention and control groups. This cluster approach was specifically selected to mitigate the risk of contamination bias, which often occurs when individual randomization within the same ward leads to intervention spillover. Consequently, this method better reflects real-world clinical conditions while maintaining a robust framework for evaluating the intervention's effectiveness. The study was conducted from September 27 to November 22, 2023, within the general medical and surgical wards of two public hospitals. Specialized units, such as intensive care and emergency departments, were intentionally excluded to minimize variability in work intensity and clinical demands. To address potential intra-cluster bias, the study selected wards with comparable baseline characteristics, specifically regarding workload patterns, patient volume, and staffing distribution. Finally, the study adhered to the Transparent Reporting of Evaluations with Nonrandomized Designs (TREND) guidelines to ensure comprehensive, structured, and transparent reporting (asu, 2004).
Participants
Of the 213 nurses screened, 66 met the inclusion criteria and provided written informed consent to participate voluntarily. In alignment with the study's gender-specific parameters, all participants were female. This recruitment strategy was grounded in empirical evidence suggesting that female nurses exhibit a higher vulnerability to emotional exhaustion and burnout, often exacerbated by the dual pressures of professional and domestic roles (Johnson et al., 2020). Consequently, narrowing the scope to female nurses was both contextually relevant and theoretically justified (Figure 2).

The TREND flow chart (asu, 2004).
The specific inclusion criteria required participants to be female nurses currently assigned to general inpatient wards, married, and having children. Furthermore, participants had to demonstrate mild to moderate burnout levels, as defined by the Maslach Burnout Inventory (MBI) threshold scores: Emotional Exhaustion (17–26), Depersonalization (7–12), and Personal Accomplishment (31–36). Professional requirements included a minimum of one year of clinical experience and at least a Diploma in Nursing (D3). Conversely, the exclusion criteria accounted for nurses presenting no burnout symptoms, those stationed in intensive care, emergency, or outpatient units, and individuals currently receiving psychological intervention for stress-related conditions.
While outcome assessors were not blinded due to the reliance on self-reported questionnaires, the implementation of standardized instruments served to mitigate potential assessment bias. This rigorous selection process ensured that the intervention was directed toward the population most likely to benefit, thereby enhancing the study's internal validity.
Sampling and Sample Sizes
The study employed a probability sampling design, specifically utilizing a cluster random sampling approach. This method involves the randomization of collective units rather than individual subjects, with groupings defined by the geographic or administrative locations of the population. In this study, participants were allocated to either the intervention or control groups through the cluster randomization of inpatient wards. From a total of 15 available wards, eight were randomly selected for inclusion. Subsequently, these eight wards were equally distributed: four were assigned to the intervention group, where the Caring-Based QNWL Program was administered, while the remaining four served as the control group, receiving conventional administrative care.
Given that the data scale employed in Stage 3 of this study was an interval scale, the sample size was determined using the hypothesis testing formula for the difference between two means (Lemeshow et al., 1994). The calculation was established based on the following parameters:

N = required sample size per group
μ₁ − μ₂ = clinically meaningful difference in mean scores before and after the intervention
σ = estimated standard deviation of the mean difference
α = significance level (5%)
β = statistical power (80%)
By inputting these parameters into the sample size formula via statistical software, the minimum required sample size was determined to be 29.68 participants per group. Consequently, this figure was rounded up to 30 participants to ensure statistical adequacy. To account for potential attrition or participant dropout, a 10% adjustment was applied using the following formula:

Consequently, the final required sample size was adjusted to 33 participants per group. To satisfy this requirement, the study enrolled 33 nurses in the intervention group and 33 in the control group, ensuring that the sample met both the criteria for statistical power and the constraints of practical implementation.
Operationally, cluster random sampling was conducted by randomly selecting 8 inpatient wards from a total of 15 wards. The selected wards were then randomly assigned into intervention and control clusters. The intervention group consisted of Wijaya Kusuma 1, Bugenvile 1, Bugenvile 2, and Hasan Sobari 1 wards, while the control group consisted of Hasan Sobari 2, Dahlia 1, Dahlia 2, and Mawar wards. Within each selected ward, eligible nurses were recruited until the required sample size of 33 participants per group was achieved. This approach ensured methodological rigor, reduced selection bias, and enhanced internal validity by maintaining randomization at the cluster level.
Instruments
To ensure the empirical accuracy and validity of the study variables, the research employed three psychometrically validated instruments:
General Characteristics Questionnaire A structured questionnaire was employed to assess the participants’ demographic and educational backgrounds. Specifically, the instrument evaluated variables such as age, satisfaction with the nursing major and clinical practice, and prior exposure to undergraduate education concerning patient safety. Furthermore, it documented observations of safety-related incidents involving clinical staff, as well as personal experiences with adverse safety events during clinical rotations. While gender was included in the standard demographic form, the cohort consisted entirely of female respondents, a distribution consistent with the specific nursing education setting of this study. Burnout Syndrome Instrument Burnout syndrome was evaluated using a 22-item questionnaire adapted from the Maslach Burnout Inventory (MBI). This psychometric instrument measures burnout across three distinct subscales: Emotional Exhaustion (9 items), Depersonalization (5 items), and Personal Accomplishment (8 items). For the purpose of analysis, scores were stratified into low, moderate, and high categories as follows:
Emotional Exhaustion:
Low: 9–26 Moderate: 27–33 High: 34–45. Depersonalization:
Low: 5–15 Moderate: 15–18 High: 19–25 Personal Accomplishment:
Low: 30–40 Moderate: 24–29 High: 8–23 The MBI demonstrated robust psychometric properties within the context of this study. Specifically, validity testing yielded item-total correlation coefficients ranging from 0.356 to 0.717, thereby establishing satisfactory construct validity. Furthermore, reliability analysis resulted in a Cronbach's alpha of 0.902, confirming high internal consistency for assessing burnout levels among the nursing workforce. Nurse Performance Instrument Nursing performance was evaluated using a proprietary instrument developed specifically for this study, grounded in Gibson's (Gibson et al., 1997) Theory of Performance. To ensure a comprehensive assessment, the instrument operationalizes performance across the following five distinct dimensions:
Quality (three items) Quantity (three items) Timeliness (four items) Effectiveness (three items) Independence (three items) Each item was evaluated using a 5-point Likert scale, ranging from 1 (very poor) to 5 (very good), to facilitate the quantification of behavioral and task-related performance outcomes within the clinical nursing context. Subsequent psychometric evaluation established that the instrument possessed high levels of reliability and validity. Specifically, item-total correlations ranged from 0.512 to 0.853, while Cronbach's alpha coefficient was calculated at 0.980. These statistical indices demonstrate excellent internal consistency, thereby validating the instrument's suitability for evaluating clinical performance among nursing staff.
Data Collection
The data collection process was systematically organized into three sequential phases:
Preintervention Phase Baseline (pretest) measurements were conducted for both the intervention and control groups to evaluate initial levels of burnout syndrome, professional performance, and QNWL. These assessments were critical to ensure the comparability of starting conditions across clusters and served as a rigorous benchmark for evaluating the subsequent effectiveness of the intervention. Intervention Phase The study participants, consisting of 66 female nurses, were bifurcated into experimental and control groups (n = 33 per group). The intervention group was subjected to a comprehensive Caring-Based QNWL Program, which utilized standardized materials compiled in a formal manual to facilitate future replicability. The program comprised two primary components:
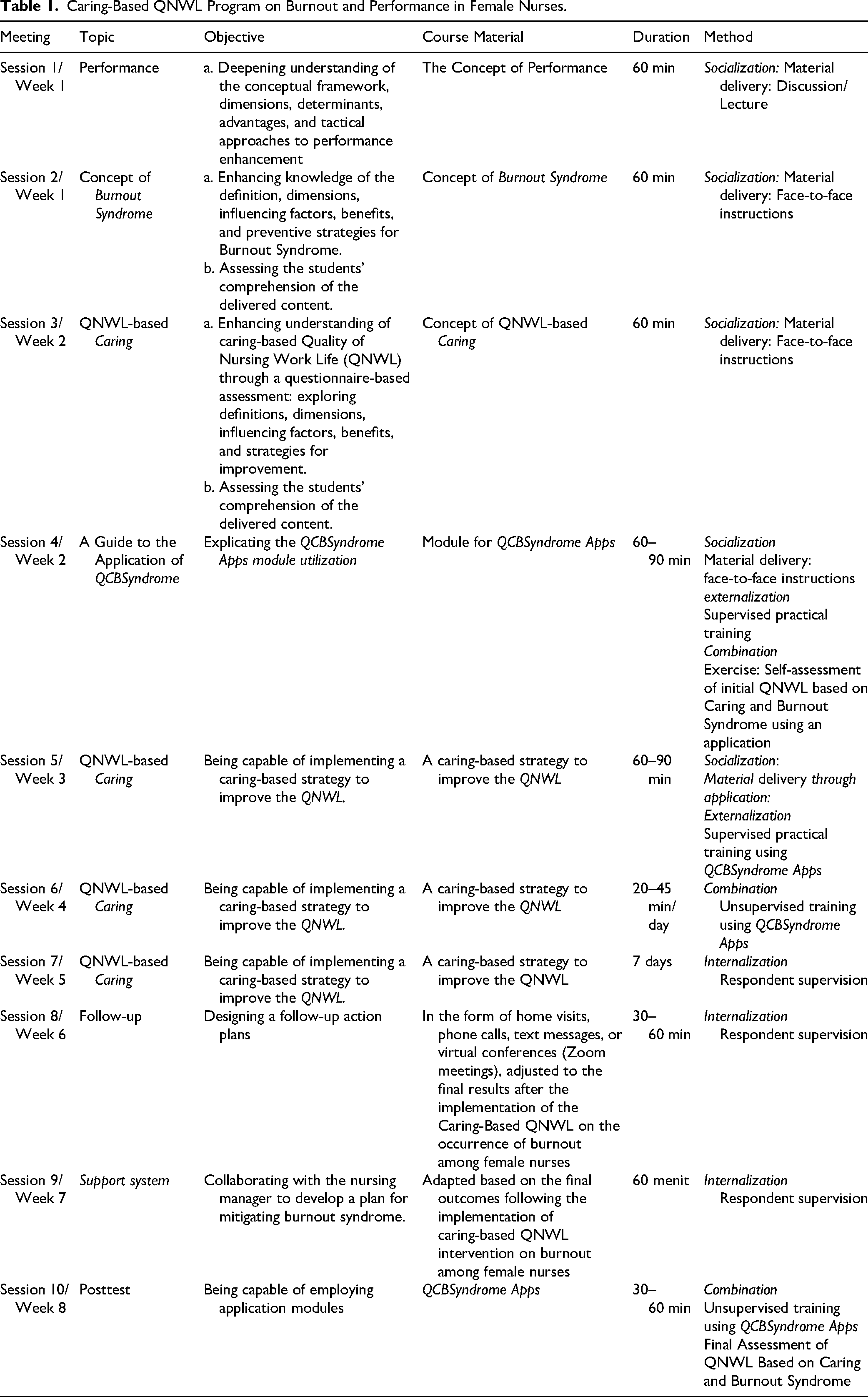
Educational Sessions: This component involved didactic lectures and structured group discussions centered on carative nursing approaches, mindfulness strategies, and reflective practices. To maintain internal validity, all instructional materials, worksheets, and reflective guides were standardized to ensure uniformity in delivery. Supervised Practical Training: Following the theoretical phase, participants applied the integrated caring principles during routine clinical activities. This application was conducted under the direct supervision of clinical mentors and head nurses. To ensure the quality of facilitation, instructors were required to possess a minimum of five years (≥5) of clinical experience and specialized prior training in caring-based The program was conducted over an 8-week period, comprising ten in-person sessions with durations ranging from 30 to 90 min. Complementing these sessions, participants utilized the QCBSyndrome App, a scientifically validated digital platform designed for daily burnout self-monitoring. This application facilitates sustained engagement through guided mindfulness audio, reflective prompts rooted in Watson's Carative Factors, weekly performance assessments, and automated adherence reminders to reinforce continuous learning. To ensure the integrity of the intervention, fidelity monitoring was rigorously maintained through weekly observation checklists, attendance logs, and periodic audits by the research team. These measures were implemented to verify the consistency of session content, duration, and delivery standards. Furthermore, participant adherence was evaluated based on session attendance, the completion of reflective assignments, and app-generated usage analytics, with a threshold of ≥80% established as the criterion for acceptable adherence. A comprehensive summary detailing the intervention structure, objectives, and delivery modalities is provided in Table 1. The control group did not receive any additional training or intervention and continued their standard professional duties based on the hospital's routine operational procedures. Postintervention Phase Following the conclusion of the intervention period, a posttest evaluation was performed for both the experimental and control groups. To ensure consistency in measurement, the identical instruments utilized during the pretest phase were re-administered to assess postintervention outcomes—specifically burnout syndrome, nursing performance, and QNWL. This methodological consistency facilitated a rigorous comparative analysis, enabling the evaluation of the program's impact both between the groups and within each group over time.
Caring-Based QNWL Program on Burnout and Performance in Female Nurses.
Data Analysis
All collected data were processed and analyzed using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were utilized to summarize the participants’ demographic characteristics and to illustrate the distribution of scores across all study variables.
To determine the appropriate statistical approach, the normality of continuous variables in both the intervention and control groups was evaluated using the Kolmogorov–Smirnov test. Additionally, Levene's test was employed to assess the homogeneity of variances between the groups. Since the data violated the assumption of normality, non-parametric tests were selected for inferential analysis. Specifically, the Wilcoxon signed-rank test was used to examine intra-group differences (pre- and postintervention), while the Mann–Whitney U test was applied to compare outcomes between the intervention and control groups. Although non-parametric analyses typically necessitate the reporting of medians and interquartile ranges (IQR), this study presents results as mean ± standard deviation (SD), as the original raw data were inaccessible and only summarized datasets were available for final reporting.
A significance level (α) of 0.05 was used for all statistical tests, with 95% confidence intervals reported. Findings were interpreted based on the observed p-values in relation to the significance threshold, in order to determine the impact of the Caring-Based QNWL Program on burnout and nurse performance.
Ethics Approval and Consent to Participate
This study received ethical approval from the Ethics Committee of the Faculty of Nursing, Universitas Airlangga, with approval number 2769-KEPK. To ensure the protection of human subjects, participant confidentiality was strictly maintained throughout all stages of the research process. Furthermore, prior to the commencement of data collection, all participants were thoroughly briefed on the study's objectives, and documented informed consent was voluntarily obtained from each individual.
Results
This section elucidates the empirical findings derived from pretest and posttest assessments, conducted via structured questionnaires. Each participant's response was systematically categorized and analyzed in strict accordance with predefined operational definitions. These outcomes demonstrate the significant impact of the Caring-Based Quality of Nursing Work Life (QNWL) Program in mitigating burnout syndrome and enhancing professional performance among female nurses.
Demographic Characteristics
The table below presents the demographic characteristics of the respondents, providing an overview of their background, including factors such as age, education, and other relevant variables. These characteristics are essential to understanding the context of the study population and their potential influence on the outcomes of the Caring-Based QNWL Program implementation.
Regarding the recruitment process, 213 nurses were initially assessed for eligibility. Of this total, 137 individuals did not meet the predefined inclusion criteria, while an additional 10 declined to participate. Consequently, 66 nurses satisfied the requirements and consented to participate. Following ward-based cluster randomization, all 66 participants (comprising 33 in the intervention group and 33 in the control group) successfully completed the study and were included in the final analysis. Notably, there were no missing data or losses to follow-up, a factor explicitly documented to ensure data integrity and analytical validity.
Furthermore, baseline demographic variables were relatively balanced between the intervention and control groups. The absence of statistically significant differences at baseline supports the assumption of initial group equivalence. Moreover, the study maintained a zero-attrition rate, thereby preserving the integrity of pre- and posttest group comparisons.
Table 2 delineates the demographic and professional characteristics of the study participants. In this research, variables such as age, educational background, parity (number of children), tenure, and income levels were not identified as significant confounding factors. The majority of respondents were within the late adulthood developmental stage (36–45 years), accounting for 54.6% of the intervention group and 36.4% of the control group. In terms of academic qualifications, the Ners professional degree predominated in both cohorts, representing 69.7% of each group.
Demographic Characteristics of Female Nurses (n = 66).

With respect to family structure, most participants had ≤2 children, comprising 60.6% and 57.6% of the intervention and control groups, respectively. Regarding professional experience, the largest proportion of respondents had a tenure of 6–10 years (63.6% intervention; 69.7% control). Furthermore, the financial profiles indicated that most participants earned ≥ the regional minimum wage (≥ Rp 1,900,000), representing 51.5% of the intervention group and 69.7% of the control group.
Ultimately, all participants enrolled and assigned to their respective groups completed the study and were included in the final analysis. Consequently, a per-protocol analysis approach was adopted, as the study encountered no attrition or protocol deviations.
Implementation of Caring-Based QNWL Program on Burnout Syndrome and Performance in Female Nurses
The subsequent tables delineate the empirical results of the Caring-Based QNWL Program's implementation, specifically focusing on burnout syndrome and professional performance among female nurses. Table 3 illustrates the distribution of pretest and posttest scores across the three dimensions of burnout syndrome and performance levels for both the intervention and control groups. Furthermore, Table 4 provides a comprehensive summary of the statistical analyses regarding the disparities between pretest and posttest outcomes, thereby elucidating the program's significant impact on mitigating burnout and enhancing nursing performance.
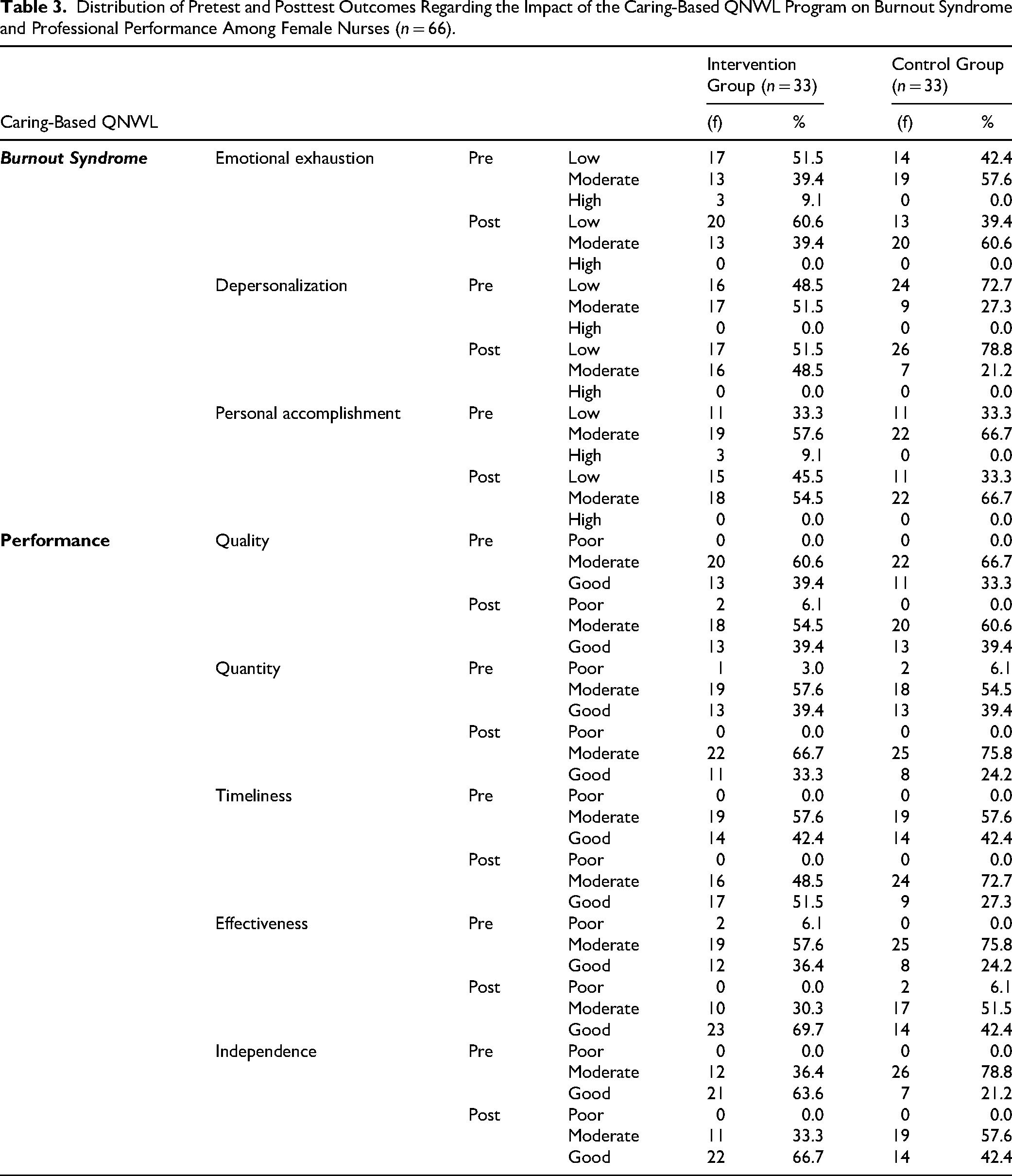
Distribution of Pretest and Posttest Outcomes Regarding the Impact of the Caring-Based QNWL Program on Burnout Syndrome and Professional Performance Among Female Nurses (n = 66).
Pretest and Posttest Analysis on the Impact of the Implementation of the Caring-Based QNWL Program on Burnout Syndrome and Performance in Female Nurses (n = 66).

Note: a = Wilcoxon signed rank test, b = Mann–Whitney.
Table 3 illustrates the pretest and posttest outcomes of the Caring-Based QNWL Program regarding burnout syndrome and nursing performance. Within the intervention group, a substantial reduction in burnout syndrome was observed across all three dimensions. Specifically, the proportion of respondents categorized with low-level symptoms improved as follows: emotional exhaustion (from 51.5% to 60.6%), depersonalization (from 48.5% to 51.5%), and personal accomplishment (from 33.3% to 45.5%). Notably, no respondents remained in the “high” burnout category for any dimension postintervention. In contrast, the control group exhibited negligible changes.
In terms of nursing performance, the intervention group demonstrated marked improvements across all five dimensions, with an increased percentage of nurses reaching the “high” performance category: quality (from 60.6% to 54.5%), quantity (from 57.6% to 33.3%), timeliness (from 57.6% to 33.3%), effectiveness (from 51.5% to 63.6%), and independence (from 36.4% to 63.6%). Conversely, performance levels within the control group remained relatively stable. Collectively, these findings indicate that the Caring-Based QNWL Program significantly mitigated Burnout Syndrome while enhancing professional performance in the intervention group.
As several variables violated the assumption of normality, a non-parametric reporting format utilizing the median and interquartile range (IQR) would have been ideal. However, since the raw data were not retained, the median and IQR could not be calculated; consequently, the study relies on summary statistics (mean and standard deviation). This lack of raw data is explicitly acknowledged as a primary methodological constraint of the current study.
Table 4 presents the pretest and posttest results of the Caring-Based QNWL Program on burnout syndrome and performance in the intervention and control groups (n = 66). In the intervention group, the pretest score (43.21 ± 9.688) significantly decreased to the posttest score (38.82 ± 6.729), with a reduction of −4.394 and p = .003, indicating a significant reduction in burnout syndrome. Conversely, the control group showed no significant change, with pretest and posttest scores of 42.3 ± 6.512 and 43.94 ± 5.556, respectively (delta = 1.636, p = .203). The Mann–Whitney test revealed no significant difference between groups before the intervention (p = .753), but a significant difference after the intervention (p = .009), with the control group showing higher Burnout Syndrome scores.
In terms of professional performance, the intervention group showed a significant improvement, with the pretest score (66.85 ± 6.95) increasing to the posttest score (70.88 ± 4.03), a difference of +4.03 and p < .001. In contrast, the control group showed a slight decrease in performance, with pretest and posttest scores of 64.61 ± 5.82 and 64.27 ± 5.15, respectively (delta = −0.70, p = .330). The Mann–Whitney test showed no significant difference between groups before the intervention (p = .147), but a significant difference after (p = .001), with the intervention group outperforming the control group. These results confirm that the Caring-Based QNWL Program effectively reduced Burnout Syndrome and improved nurse performance.
Discussion
Statistical analysis confirms that the Caring-Based Quality of Nursing Work Life (QNWL) Program significantly reduces burnout syndrome among nurses within the intervention group. This reduction was consistently observed across all three dimensions of burnout—emotional exhaustion, depersonalization, and personal accomplishment—between pre- and postintervention assessments, thereby validating the program's effectiveness in enhancing nurses’ emotional well-being. These findings align with extant literature demonstrating that structural improvements in the clinical work environment and the quality of nursing work life effectively mitigate burnout symptoms (Kutney-Lee et al., 2013; Nursalam et al., 2020; Widayati et al., 2020).
QNWL has been widely recognized as a critical determinant of nurses’ emotional resilience and professional functionality. Prior studies have reported a moderate negative correlation between QNWL and burnout, suggesting that higher occupational quality substantially contributes to decreased emotional exhaustion and depersonalization (Nursalam et al., 2020). Furthermore, burnout has been linked to a deterioration in overall quality of life and diminished empathy, particularly among practitioners experiencing a reduced sense of personal accomplishment (Kupcewicz & Jóźwik, 2020; Seo et al., 2020).
Beyond mitigating burnout, the Caring-Based QNWL program demonstrated a statistically significant positive impact on nursing performance. Most performance dimensions exhibited substantial improvement within the intervention group, reinforcing the premise that an emotionally supportive and caring-oriented work environment fosters higher levels of professional engagement and productivity. These findings align with existing literature, which posits that burnout is inextricably linked to heightened stress, sleep disturbances, psychological disengagement, and a subsequent decline in occupational (Chico-Barba et al., 2022).
Nevertheless, the specific dimension of “quality of care” did not yield a statistically significant improvement, suggesting that this facet of performance may be governed by broader organizational and systemic determinants. Factors such as staffing ratios, workload distribution, and overarching administrative policies are critical in shaping the quality of care and may necessitate more sustained, organization-wide interventions that extend beyond the 8-week duration of this program. This observation corroborates previous studies emphasizing the inherent complexity of enhancing care quality through individual-level interventions alone (Nursalam et al., 2020).
Statistical analysis confirms that the Caring-Based Quality of Nursing Work Life (QNWL) Program significantly reduces burnout syndrome among nurses within the intervention group. This reduction was consistently observed across all three dimensions of burnout—emotional exhaustion, depersonalization, and personal accomplishment—between pre- and postintervention assessments, thereby validating the program's effectiveness in enhancing nurses’ emotional well-being. These findings align with extant literature demonstrating that structural improvements in the clinical work environment and the quality of nursing work life effectively mitigate burnout symptoms (Kutney-Lee et al., 2013; Nursalam et al., 2020; Widayati et al., 2020).
QNWL has been widely recognized as a critical determinant of nurses’ emotional resilience and professional functionality. Prior studies have reported a moderate negative correlation between QNWL and burnout, suggesting that higher occupational quality substantially contributes to decreased emotional exhaustion and depersonalization (Nursalam et al., 2020). Furthermore, burnout has been linked to a deterioration in overall quality of life and diminished empathy, particularly among practitioners experiencing a reduced sense of personal accomplishment (Kupcewicz & Jóźwik, 2020; Seo et al., 2020).
Beyond mitigating burnout, the Caring-Based QNWL program demonstrated a statistically significant positive impact on nursing performance. Most performance dimensions exhibited substantial improvement within the intervention group, reinforcing the premise that an emotionally supportive and caring-oriented work environment fosters higher levels of professional engagement and productivity. These findings align with existing literature, which posits that burnout is inextricably linked to heightened stress, sleep disturbances, psychological disengagement, and a subsequent decline in occupational (Chico-Barba et al., 2022).
Nevertheless, the specific dimension of “quality of care” did not yield a statistically significant improvement, suggesting that this facet of performance may be governed by broader organizational and systemic determinants. Factors such as staffing ratios, workload distribution, and overarching administrative policies are critical in shaping the quality of care and may necessitate more sustained, organization-wide interventions that extend beyond the 8-week duration of this program. This observation corroborates previous studies emphasizing the inherent complexity of enhancing care quality through individual-level interventions alone (Nursalam et al., 2020).
Several methodological limitations must be considered when interpreting these findings. First, the observed performance improvements may be partially attributed to the Hawthorne effect, given that participants in the intervention group were cognizant of being monitored. Furthermore, despite the implementation of cluster-based allocation, the risk of contamination bias—specifically through inter-ward information exchange—could not be entirely eliminated. Such lateral communication may have attenuated the variance between groups, thereby potentially diminishing the perceived magnitude of the intervention's impact.
From a global perspective, the current findings align with existing empirical evidence demonstrating the efficacy of caring- and mindfulness-based interventions in mitigating burnout and enhancing the quality of nursing work life (QNWL) across diverse clinical settings. For instance, longitudinal studies conducted in China and Spain have reported significant reductions in emotional exhaustion alongside marked improvements in resilience, collaborative teamwork, and psychological well-being (Ruiz-Fernández et al., 2020). Such consistency underscores the cross-cultural relevance and adaptability of caring-based QNWL frameworks within international healthcare systems.
The Indonesian cultural landscape further reinforces the applicability of this intervention. Nursing practice in Indonesia is deeply embedded in collectivist values, hierarchical organizational structures, and high societal expectations regarding empathy and interpersonal harmony. Furthermore, female nurses frequently navigate compounded work–family obligations, which significantly heightens their vulnerability to occupational burnout. The observed efficacy of the Caring-Based QNWL Program suggests that caring-oriented values resonate profoundly within this specific cultural milieu, bridging the gap between professional requirements and cultural identity.
From a practical standpoint, these findings imply that hospital administrators should prioritize the integration of caring-based and mindfulness-oriented programs into professional development and staff well-being initiatives. Such interventions represent sustainable strategies for reducing attrition and enhancing clinical performance, particularly for female nurses managing dual-role demands. Academically, this study enriches the burgeoning body of literature on integrative interventions that simultaneously address emotional health and professional excellence in nursing.
To build upon these findings, future research should investigate the long-term sustainability of these effects through longitudinal follow-up periods. Additionally, incorporating patient-level outcomes would provide a more comprehensive assessment of the impact of QNWL interventions on the quality of care. Finally, expanding the research scope to include male nurses and a broader range of clinical environments would enhance the generalizability of the results and deepen the understanding of burnout dynamics across the entire nursing workforce.
From a theoretical standpoint, the mediating role of job satisfaction within the Caring-Based QNWL framework can be interpreted through the lens of the Job Demands–Resources (JD–R) model, which posits that organizational resources such as supportive leadership, professional recognition, and a caring work climate buffer the impact of job demands and foster engagement and well-being (Bakker & Demerouti, 2007). Within this framework, improvements in QNWL function as structural job resources that enhance intrinsic motivation and emotional regulation, thereby indirectly reducing burnout and strengthening performance outcomes. Although the R2 values observed in the structural model were modest, this finding is theoretically coherent given the multifactorial nature of burnout and performance in healthcare settings. Burnout is shaped not only by organizational climate but also by individual coping capacity, personality traits, workload intensity, leadership style, and broader systemic constraints (Maslach & Leiter, 2016). Consequently, the explained variance should not be interpreted as a weakness of the model but rather as an indication of the inherent complexity of occupational health phenomena in clinical environments. These results support the notion that caring-based organizational interventions represent a meaningful, albeit partial, mechanism within a broader ecological system influencing nurse well-being and professional functioning.
Several methodological limitations must be considered when interpreting these findings. First, the observed performance improvements may be partially attributed to the Hawthorne effect, given that participants in the intervention group were cognizant of being monitored. Furthermore, despite the implementation of cluster-based allocation, the risk of contamination bias—specifically through inter-ward information exchange—could not be entirely eliminated. Such lateral communication may have attenuated the variance between groups, thereby potentially diminishing the perceived magnitude of the intervention's impact.
From a global perspective, the current findings align with existing empirical evidence demonstrating the efficacy of caring- and mindfulness-based interventions in mitigating burnout and enhancing the quality of nursing work life (QNWL) across diverse clinical settings. For instance, longitudinal studies conducted in China and Spain have reported significant reductions in emotional exhaustion alongside marked improvements in resilience, collaborative teamwork, and psychological well-being (Ruiz-Fernández et al., 2020). Such consistency underscores the cross-cultural relevance and adaptability of caring-based QNWL frameworks within international healthcare systems.
The Indonesian cultural landscape further reinforces the applicability of this intervention. Nursing practice in Indonesia is deeply embedded in collectivist values, hierarchical organizational structures, and high societal expectations regarding empathy and interpersonal harmony. Furthermore, female nurses frequently navigate compounded work–family obligations, which significantly heighten their vulnerability to occupational burnout. The observed efficacy of the Caring-Based QNWL Program suggests that caring-oriented values resonate profoundly within this specific cultural milieu, bridging the gap between professional requirements and cultural identity.
From a practical standpoint, these findings imply that hospital administrators should prioritize the integration of caring-based and mindfulness-oriented programs into professional development and staff well-being initiatives. Such interventions represent sustainable strategies for reducing attrition and enhancing clinical performance, particularly for female nurses managing dual-role demands. Academically, this study enriches the burgeoning body of literature on integrative interventions that simultaneously address emotional health and professional excellence in nursing.
To build upon these findings, future research should investigate the long-term sustainability of these effects through longitudinal follow-up periods. Additionally, incorporating patient-level outcomes would provide a more comprehensive assessment of the impact of QNWL interventions on the quality of care. Finally, expanding the research scope to include male nurses and a broader range of clinical environments would enhance the generalizability of the results and deepen the understanding of burnout dynamics across the entire nursing workforce.
The replicability of the Caring-Based QNWL Program represents a key strength of this study. Although the intervention was implemented in Indonesian public hospitals, its core components namely Watson's carative factors, structured reflective practices, and work–life balance support are grounded in universal caring principles and are not bound to specific cultural norms. These components can be adapted across diverse healthcare contexts by aligning implementation strategies with local cultural values, organizational policies, and workforce characteristics. In addition, the program has the potential to be integrated into routine professional development activities, sustainable staff well-being initiatives, and digital self-monitoring systems. Although the present study did not include long-term follow-up evaluations, future research is recommended to conduct longitudinal assessments to examine the sustainability of the intervention's effects on burnout reduction and improvements in nurses’ professional performance.
Strengths and Limitations
This study presents a novel integration of Watson's Human Caring Theory within the QNWL framework, specifically tailored to address the needs of female nurses—a demographic significantly predisposed to Burnout Syndrome. The intervention was systematically developed and rigorously evaluated through a quasi-experimental design featuring pretest and posttest measures alongside a control group comparison, thereby enhancing the empirical validity of the findings. Furthermore, the employment of validated instruments and structured mentoring protocols reinforces the program's methodological rigor and its practical applicability within authentic clinical environments.
This study has several limitations that warrant acknowledgment. First, the quasi-experimental, non-randomized design precludes the establishment of definitive causal relationships between the intervention and the observed outcomes. Second, the generalizability of the findings to broader nursing populations or diverse healthcare settings is constrained by the relatively small sample size, the exclusive inclusion of female nurses, and the limitation of data collection to only two hospitals. To validate and extend these results, future research should employ larger, randomized, and more diverse samples across multiple sites.
Third, the absence of a long-term follow-up stage leaves the sustainability of the intervention's effects uncertain; consequently, subsequent studies should incorporate longitudinal measurements to evaluate the persistence of improvements over time. Fourth, although the exclusive focus on female nurses reflects the gender demographics of the selected sites, it restricts the external validity across gender lines. Future inquiries should prioritize more diverse gender representation and encompass various healthcare contexts, regions, and hospital types.
Fifth, the 8-week intervention period may have been insufficient to yield significant improvements across all performance dimensions, particularly within the quality domain. This lack of marked improvement may be attributed to both the limited duration and a deficiency in managerial reinforcement, suggesting that quality-related outcomes may require more prolonged and systemic interventions. Sixth, the study did not report effect size (ES) values, thereby limiting the interpretation of the findings’ practical significance beyond mere statistical probability. Incorporating effect size analysis in future research is essential to strengthen the clinical relevance of the outcomes.
Seventh, the study relied solely on quantitative metrics, such as burnout scores and task performance, leaving qualitative dimensions—including nurse satisfaction, perceived self-efficacy, and the nuance of nurse–patient relationships—unexplored. Adopting a mixed-methods approach in future research would offer a more holistic understanding of how caring-based QNWL interventions influence nurses’ lived experiences. Finally, the unavailability of raw data hindered the reporting of Median–IQR values for nonparametric analyses, which is noted as a further methodological constraint.
Implications for Nursing Practice
The Caring-Based Quality of Nursing Work Life (QNWL) program offers a robust framework for optimizing nursing well-being and professional performance by integrating carative values, systematic stress management, and comprehensive work-life balance support. Through the promotion of emotional resilience and the reinforcement of mindfulness practices, this initiative fosters a psychologically safe clinical environment.
From an organizational standpoint, the program serves as a strategic intervention to mitigate absenteeism, reduce turnover rates, and alleviate the economic burden associated with clinician burnout. Furthermore, it cultivates an institutional culture rooted in compassion and professional engagement, which subsequently enhances interpersonal communication, collaborative teamwork, and the delivery of patient-centered care. Embedding these interventions into professional development frameworks constitutes a sustainable strategy for strengthening workforce retention and elevating clinical outcomes.
In terms of long-term implications, the program's design facilitates institutional sustainability through its potential adoption as a core component of continuous professional development and wellness initiatives. Systematic integration into hospital policies and ongoing training modules ensures that the benefits remain durable and adaptable to the evolving complexities of the healthcare landscape.
From a broader policy perspective, the findings of this study underscore the necessity of incorporating caring principles and QNWL metrics into national nursing workforce strategies and hospital accreditation standards. Integrating mindfulness-based caring protocols into quality improvement frameworks provides a viable solution to the challenges of nursing workforce sustainability. Consequently, healthcare administrators and policymakers are encouraged to formulate institutional policies that prioritize a culture of care, ensure psychological safety, and implement equitable workload distribution to preserve nursing excellence.
Furthermore, although this study primarily focused on female nurses, the foundational pillars of the program—caring values, stress management, and work-life balance—remain highly transferable. Adapting the curriculum to address gender-specific and role-specific nuances would enhance its relevance and efficacy across diverse, multidisciplinary healthcare teams.
Conclusion
This study demonstrates that the Caring-Based Quality of Nursing Work Life (QNWL) Program effectively mitigates Burnout Syndrome and optimizes professional performance among female nurses. By integrating structured educational interventions with the utilization of the QCB Syndrome application, the program fosters emotional resilience and reinforces carative behaviors within clinical practice. Furthermore, the synthesis of Watson's caring principles with digital support tools cultivates a more empathetic and robust work culture.
Beyond individual outcomes, these findings offer significant implications for hospital administration and healthcare policy. Specifically, the incorporation of caring-based and gender-sensitive strategies into workforce development frameworks can reduce occupational burnout, bolster job satisfaction, and elevate the quality of care at the institutional level. Consequently, broader implementation and rigorous evaluation across diverse healthcare settings are recommended to ensure the sustainability and scalability of this model, With appropriate contextual adaptation, this program may serve as a scalable framework for promoting nurse well-being and performance across diverse healthcare systems.
Use of AI Software
No generative AI software was used in the writing of this manuscript. Where applicable, AI tools were used only for language editing and have been appropriately acknowledged.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.