
Abstract
Background
Burnout syndrome refers to a state of physical or extreme emotional exhaustion, a negative and cynical attitude toward patients, a diminished sense of personal achievement, and depersonalization, often resulting from prolonged and unmanaged workplace stress.
Objective
This study aimed to investigate the magnitude and associated factors of burnout syndrome among healthcare professionals working in intensive care units.
Methods
A multicenter, institution-based, cross-sectional study was conducted from July 1, 2023 to August 30, 2023, involving 529 healthcare professionals. A systematic random sampling method was used to select participants. The standardized Maslach Burnout Inventory questionnaire was employed to collect the data. The data were reviewed, coded, and entered into Epi Info version 7.0, then transferred to SPSS version 26 for analysis. Bivariate and multivariable logistic regression models were used to identify factors associated with burnout syndrome. A p-value <0.05 was considered statistically significant.
Results
The prevalence of burnout syndrome among healthcare workers in the intensive care unit was 28.7% (95% confidence interval [CI]: 25.1–33.1). Factors such as being over 40 years old (adjusted odds ratio [AOR]: 2.82; 95% CI: 1.23–6.46), having 5 to 10 years of work experience (AOR: 4.81; 95% CI: 2.92–7.92), exceeding 10 years of work experience (AOR: 3.96; 95% CI: 1.67–9.39), working more than 8 h per day (AOR: 2.51; 95% CI: 1.34–2.71), and substance use (AOR: 2.52; 95% CI: 1.08–5.86) showed statistically significant associations with burnout syndrome in a binary logistic regression model.
Conclusion and Recommendations
Burnout syndrome is very common among healthcare workers in intensive care units. Therefore, healthcare facilities and policymakers need to recognize its impact on their staff's wellbeing. Implementing measures like regular mental health support, staff rotation, and efficient workload management can significantly reduce burnout and enhance the overall quality of patient care in these high-stress environments.
Introduction
Burnout syndrome (BOS) is a psychological condition that results from prolonged negative stress. It is a response to chronic work-related stressors and is characterized by emotional exhaustion (EE), depersonalization (DP), and low personal accomplishment (LPA). This syndrome can occur among individuals who work with people for extended periods without adequate time for physical or emotional recovery (Das et al., 2015; Gan et al., 2019).
Burnout among healthcare professionals is one of the key challenges affecting healthcare practice and the quality of care (Bridgeman et al., 2018; Dubale et al., 2019a). Burnout among healthcare providers has been linked to increased self-reported errors, reduced time devoted to providing clinical care, and higher mortality rates in low- and middle-income countries (Fentie et al., 2021). The consequences of BOS can be serious for professionals, clients, and organizations in general. Burnout is an occupational phenomenon in the 11th Revision of the International Classification of Diseases (ICD-11). Burnout is associated with physical health issues, psychiatric disorders, brain changes, and career dissatisfaction (Guo et al., 2021).
During the COVID-19 pandemic, healthcare workers will face longer work hours, a heavier workload, insufficient time for rest and recuperation, inadequate availability of personal protective equipment, and prolonged use of PPE. This situation will increase the risk of burnout in an already vulnerable professional environment. Additionally, inadequate knowledge about the diagnosis, transmission, and management of novel viruses will worsen the risk of burnout syndrome (Abdelhafiz et al., 2020; Embriaco et al., 2007; Galanis et al., 2021).
Healthcare providers are recognized as a high-risk population for experiencing burnout, and the incidence of burnout among them has been increasing in recent years. Reports indicate that the prevalence of burnout in high-income countries within the general working population ranges from 13% to 58% (Jalili et al., 2021).
The study would enhance the existing body of knowledge by providing specific data and insights into the extent of burnout experienced by healthcare professionals in intensive care units (ICUs), offering a baseline understanding of the issue, and identifying the demographic and work environment factors that influence burnout levels among healthcare workers inICUs.
Review of Literature
BOS is defined by Maslach et al. as the presence of increased feelings of emotional exhaustion, the development of a negative and cynical attitude toward clients (depersonalization), and a negative sense of personal accomplishment (Maslach & Jackson, 1981). It is a complex syndrome characterized by a combination of internal personal characteristics and occupational stressors that lead to behaviors, attitudes, feelings, and strategies (Maslach & Jackson, 1981; Schutte et al., 2000).
The connection between stressors and inputs results in outcomes such as unmet expectations, robotic behavior, poor operational management, demotivation, and neglect of service recipients. This multifaceted issue naturally leads to burnout, which affects service quality and the wellbeing of those involved. The extent and depth of interactions between these factors depend on the individual's personal and professional experiences (Manzano-García & Ayala-Calvo, 2013).
The magnitude of burnout syndrome varies in different studies. A meta-analysis report of 31.81% of frontline healthcare professionals working during the severe acute respiratory syndrome, the Ebola, and COVID-19 pandemics (Busch et al., 2022). The prevalence of burnout in high-income countries among the general working population has been reported to range from 13% to 27%. However, healthcare providers have been described as a high-risk population for experiencing burnout, and the prevalence of burnout among healthcare providers has been increasing in recent years (Moukarzel et al., 2019). Studies conducted in the United States have shown that 54% of physicians, 35% of hospital nurses, and 35.2% of medical students reported experiencing burnout. Similar rates of burnout among healthcare providers have been reported in other high-income countries (Dubale et al., 2019b).
A Systematic Review of 927 records on the Burden of Burnout among Healthcare Professionals in intensive care units and emergency departments during the COVID-19 pandemic shows that the prevalence of overall burnout ranged from 49.3% to 58% (Gualano et al., 2021). Based on a specific profession, a meta-analysis of 16 studies reported that the overall prevalence of emotional exhaustion was 34.1%, depersonalization was 12.6%, and lack of personal accomplishment was 15.2% among nurses working during the COVID-19 pandemic. An overall pooled prevalence of burnout symptoms among global nurses was 11.23% (Galanis et al., 2021; Woo et al., 2020).
In a study conducted among Egyptian physicians during the COVID-19 pandemic, the frequency of BOS among the research group was 36.36% (Abdelhafiz et al., 2020). The prevalence of BOS among nurses was 34% in a study done among Nurses in Public Hospitals in Southwest Ethiopia (Hailay et al., 2020). In a study conducted among 412 nurses working in public hospitals of Harari regional state and Dire Dawa administration, eastern Ethiopia, from February 1 to29, 2020, 44.4% of nurses experienced burnout (Dechasa et al., 2021). In a study done in Gondar University Hospital, burnout among healthcare professionals, the overall prevalence of burnout was 13.7%, and the majority of the respondents experienced debility (52.8%), self-criticism (56%), and depressive symptoms (46%) (Bhagavathula et al., 2017).
A study conducted in the Addis Ababa public hospital in 2019 shows that the overall prevalence of burnout syndrome among healthcare workers was 31.6%. Sociodemographic factors, age, marital status, long night shift work, job satisfaction, and educational level were factors significantly associated with burnout syndrome (Fentie et al., 2021).
A study in Ethiopia found that educational status, job title, work experience, and social support are strong predictors of burnout syndrome among nurses. Females and those with fewer years of experience were more likely to experience burnout (Jalili et al., 2021).
The possible explanation for the difference in prevalence may be attributed to variations in study setting, study population, tools, and methodological differences. In addition to this, the majority of health care workers from developed countries like Italy might be with good educational status, job title, and strong social support, whereas, in other studies conducted in Africa, there were respondents with low social support, fatigue syndrome, psychological distress, and major sleeping problems, which could contribute to the development of burnout syndrome (Figure 1; Pisanti et al., 2011).

Conceptual Framework for the Magnitude and Associated Factors of Burnout Syndrome Among Healthcare Workers Att Public Hospitals Intensive Care Units in Ethiopia.
Methods
Study Design and Period
An institution-based, multicenter, cross-sectional study was conducted from July 1, 2023 to August 30, 2023. The study took place in Addis Ababa, the capital city of the country. According to data from PHEOC (Public Health Emergency Operations Center), there are 284 mechanical ventilators and 414 ICU bed capacities in public hospitals nationwide. Of these, 96 MVs and 124 ICU bed capacities are located in Addis Ababa.
Research Questions
This research investigated the following research questions:
What is the prevalence of burnout syndrome among healthcare workers in ICUs in Addis Ababa? How do demographic and work environment factors affect the levels of burnout among healthcare workers in ICUs in Addis Ababa?
Source Population and Study Population
The source population for this study consisted of healthcare workers in ICUs at public hospitals in Addis Ababa. The study population included all selected healthcare workers in the ICUs during the data collection period.
Sample Size Determination
The sample size for the prevalence of burnout syndrome among healthcare workers in ICUs was calculated using a single population proportion formula, based on the following assumption: a proportion level of 31.6% was taken from a study conducted at Addis Ababa Public Hospital in 2019 (Fentie et al., 2021).
95% Confidence level and 5% degree of precision; Margin of error (0.05); Z±α/2 is the standard normal value at a 95% confidence level (1.96).
Fitting into the formula, the final sample size was


Since the populations used for the study are heterogeneous design effect was used. Therefore, interclass correlation: 1.5,

Adding 10% for the nonresponse rate, the final sample size became 498 + 50 = 548. So, the final sample size for the study is 548.
Inclusion and Exclusion Criteria
All healthcare workers in the ICU with at least 6 months of experience who were available during the data collection period were included. Those in the ICU who did not wish to participate in the study were excluded.
Variables of the Study
Dependent Variable
Burnout syndrome (Yes, No).
Independent Variables
Sociodemographic factors: age, sex, marital status, educational level, number of children, and monthly salary. Age in years.
Personal risk factors: satisfaction with work, conflict with colleagues, smoking, drinking alcohol, khat-chewing, and lack of appreciation of ethnicity.
Work-related characteristics include job title, workload, service delivery unit, hospital type, duty hours, years of experience, training, recognition, support from family and organization, intention to leave work within the next 6 months, sleeping hours, and working hours.
Sampling Procedure
Health institutions providing ICU services were classified under the Federal Ministry of Health, the Ministry of Education, and the Addis Ababa City Administration Health Bureau. Two hospitals from the Federal Ministry of Health and two from the Addis Ababa City Administration Health Bureau were selected using a lottery method. The allocation of study subjects to each hospital was determined based on the proportion of healthcare workers in ICUs during the same period at each health facility. Systematic sampling was employed to select study participants at each health facility. The first sample was chosen through the lottery method. A systematic random sampling technique was used to select subsequent samples, and the recruitment of healthcare providers continued until the desired sample size was achieved.
Data Collection Instruments and Procedures
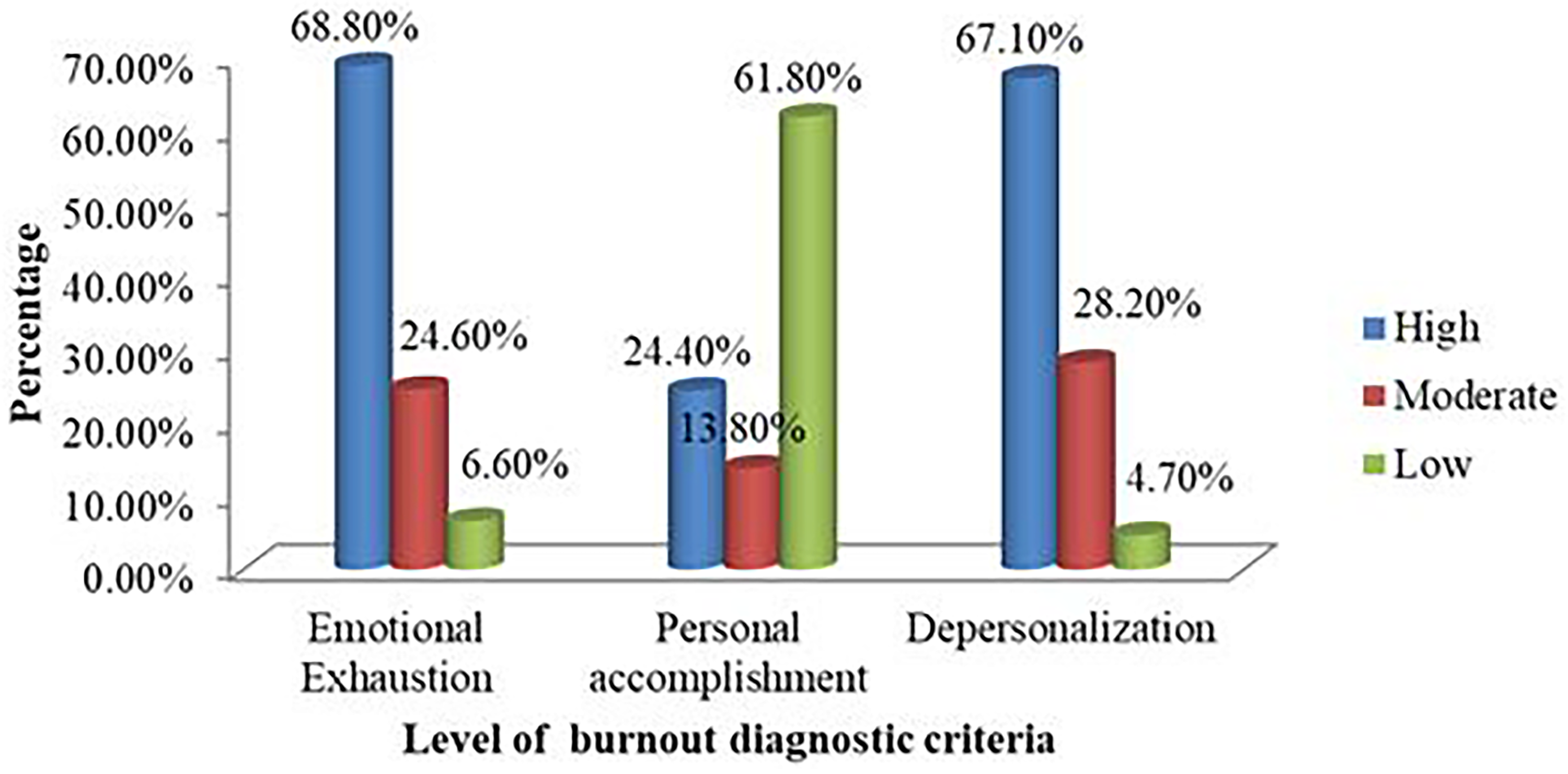
The data were collected using a self-administered, standardized questionnaire adapted from previous literature (Campos & Maroco, 2012; Cañadas-De la Fuente et al., 2015; Ebling & Carlotto, 2012). Four BSc nursing professionals conducted data collection. The questionnaire included sociodemographic characteristics and job-related details, and it also contained the Maslach Burnout Inventory (MBI), which is the most commonly used 22-item measuring tool for self-assessing the risk of burnout. It is a validated tool that evaluates three syndrome subscales: emotional exhaustion (9 items), depersonalization (5 items), and lack of personal accomplishment (8 items). The questionnaires were distributed to all participants to complete during their free time after explaining the contents, objectives, and anonymity of the study. There were no identifiers for any personal responses, and the participants were unaware of the scoring system.
Data Quality and Management
To ensure data quality, a pretest of the questionnaire was conducted with 55 health professionals (10% of the sample size) from hospitals excluded from the main study, verifying the information's accuracy, completeness, and clarity. Corrections were made based on feedback received from the questionnaire for the main study. Training and orientation were provided to data collectors regarding the study's objectives and relevance, as well as clarification on each item involved in the study. All questionnaires were reviewed for missing or inconsistent responses, with follow-up conducted as needed. Cronbach's alpha was calculated during piloting and after data collection to assess internal consistency. The completeness and consistency of the collected data were regularly checked, and incomplete data were excluded.
Data Entry, Analysis, and Interpretation
Data were checked for completeness before entering Epi Info version 7.0. The dataset was cleaned using Epi Info 7.0 before being transferred to SPSS version 26.0 for analysis. Descriptive statistics were presented in the form of frequency tables, graphs, and charts.
After cleaning and checking were completed, the data were summarized for sociodemographic variables using proportions, means, and medians. The summary was presented in tables and graphs. The data were then analyzed for the proportion of burnout syndrome based on the MBI classification.
Binary logistic regression was used to assess the degree of association between independent variables and the dependent variable (burnout syndrome). A bivariate analysis will be conducted to calculate an unadjusted odds ratio (OR) and screen for potentially significant independent variables at a 25% level of significance for inclusion in the multivariable binary logistic regression model. The OR, p-value, and 95% CI for adjusted OR (AOR) were used to test the significance and interpret results. Variables with a p-value ≤ .05 were considered statistically associated with the outcome variable. The assumption of multicollinearity was evaluated using VIF, and the adequacy of the final model was verified using the Hosmer and Lemeshow goodness of fit test, where a value > 0.05 indicates that the model fits the data well.
Operational Definition
BOS is a physical and psychological outcome that results from long-term exposure to job-related stress. Which is a mental state characterized by psychological weariness to provide human service, it is characterized by EE, DP, and LPA (Ahmed et al., 2022; Hailay et al., 2020).
EE is described as “wearing out, loss of energy, depletion, debilitation, and fatigue.” In this study, EE refers to feeling exhausted and no longer able to cope emotionally with stressors related to work, with a score of low (<13), moderate (14–26), and high (≥27). Corresponding to symptoms experienced a few times per month, as per the MBI tool (Ang et al., 2016; Odonkor & Frimpong, 2020).
DP is defined as emotional apathy and dehumanization of those who receive one's services, care, treatment, or instruction, with a score of low (<2), moderate (3–9), and high (≥10) corresponding to symptoms experienced once per month or less (AbdAllah & El-Hawy, 2019; Cañadas-De la Fuente et al., 2015).
PA is defined as sentiments of work stagnation, inefficiency, and underperformance, with a score of low (≥ 43), average (31–42), and a high degree of burnout (≤ 31) corresponding to symptoms experienced approximately once per week (Alvares et al., 2020; Organization, 2010).
Health professionals are individuals who study, advise on, or provide preventive, curative, rehabilitative, and promotional health services based on a substantial body of theoretical and factual knowledge in diagnosing and treating diseases and other health issues.
Substance abuse, according to DSM-5-TR criteria, is a maladaptive pattern of substance use leading to clinically significant impairment or distress, as manifested by recurrent substance use failing to fulfill major role obligations (Sadock, 2015).
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Institutional Review Committee of GAMBY Medical and Business College, with the ethical reference number V685/14/07/2023. A formal letter was submitted to the Addis Ababa Health Bureau and each selected study hospital to ensure permission and maintain confidentiality. Verbal and written informed consent were acquired from each study participant under the principles of the Helsinki Declaration. The Declaration of Helsinki was considered, and its principles and recommendations have been applied.
Results
Sociodemographic Characteristics
A sample of 529 study participants took part in this study, achieving a response rate of 96.5%. The ages of the participants ranged from 24 to 64 years, with a median age of 31 years and an interquartile range (IQR) of 28 to 35 years. Nearly half of the participants were categorized as being between 30 and 40 years old. More than half of the participants (54.3%) were male, and 259 (49.0%) were married (Table 1).
Sociodemographic Characteristics of Health Care Workers at Public Hospitals in the Intensive Care Units in Addis Ababa, 2023.

Medical and Behavioral Characteristics
Among the respondents, 44 (8.3%) of the study participants have been diagnosed with a chronic disease. Of those diagnosed with chronic diseases, 28 (63.6%) did not meet the criteria for diagnosing burnout syndrome, while 16 (36.4%) did meet the criteria. Similarly, 56 (10.6%) of the respondents reported abusing at least one type of substance. Half of the substance-abusing respondents (28, 50.0%) met the criteria for diagnosing burnout syndrome (Table 2).
Work and Related Characteristics of Health Care Workers at Public Hospitals’ Intensive Care Units in Addis Ababa, 2023.
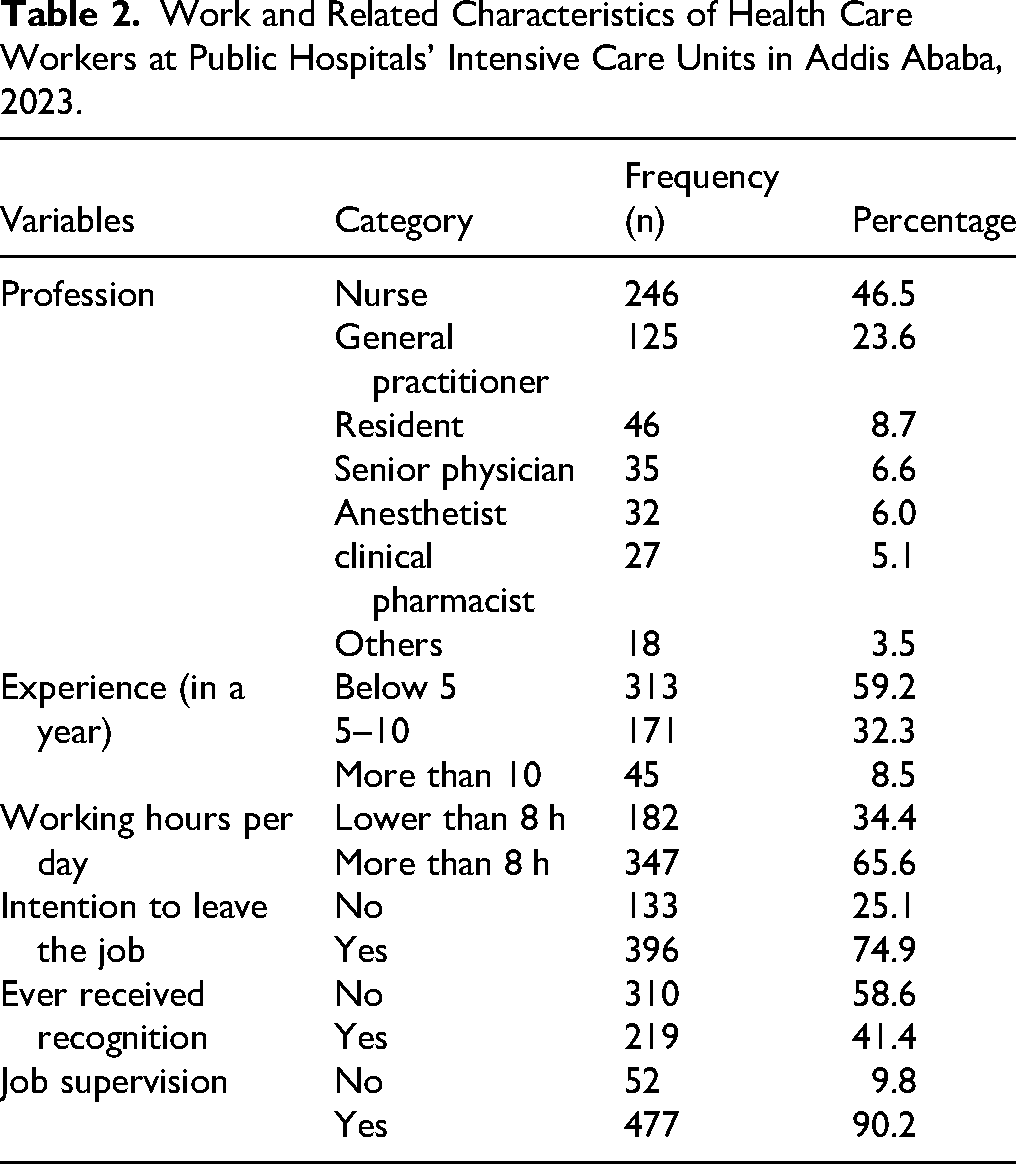
Work and Related Characteristics
Among the study participants, 246 (46.5%), 125 (23.6%), and 46 (8.7%) were nurses, general practitioners, and residents, respectively. More than half of the respondents, 313 (59.2%), have work experience of <5 years. Similarly, two-thirds of the respondents, 347 (65.6%), work more than 8 h per day. Nearly three-fourths of the study participants, 396 (74.9%), intend to leave their jobs, and 477 (90.2%) of the study participants have a supervisor. Considering the working shifts of the study participants, 309 (58.4%), 204 (38.6%), and 16 (3.0%) of the healthcare workers alternate between day and night shifts, respectively (Table 2).
Prevalence of Burnout Syndrome
In this study, 152 (28.7%) of the healthcare workers met the criteria for the diagnosis of burnout. Therefore, the prevalence of burnout among healthcare workers was 28.7% (95% CI: 25.1–33.1; Figure 2).
Prevalence of Burnout Syndrome Among Halthcare Workers at Public Hospitals Intensive Care Unit in Addis Ababa 2023.
Factors Associated With Burnout Syndrome
In this study, sex, age, years of experience, working more than 8 h per day, intention to leave a job, known chronic diseases, recognition, substance abuse, job supervision, and monthly income were considered as candidate variables in the bivariate logistic regression model. Among these candidates, substance use, working more than 8 h per day, years of experience, and age demonstrated statistical significance in the multivariable binary logistic regression model (Table 3).
Factors Associated With BOS Among Healthcare Workers at Public Hospitals’ Intensive Care Units in Addis Ababa.

Note. AOR: adjusted odds ratio; BOS: burnout syndrome; CI: confidence interval; COR: Crude Odd Ratio.
*Indicates variables having a p-value <.25 in bivariate analysis, and ** indicates variables having a p-value <.05 in multivariable analysis.
Health workers over 40 years old have 2.82 times the chance of experiencing burnout compared to those under 30 years old (AOR: 2.82; 95% CI: 1.23–6.46). The odds of burnout among healthcare workers with 5 to 10 years of experience are 4.81 times higher (AOR: 4.81; 95% CI: 2.92–7.92), while those with more than 10 years of experience face 3.96 times higher odds (AOR: 3.96; 95% CI: 1.67–9.39) compared to those with <5 years of experience (Table 3).
The risk of burnout among healthcare workers who worked more than 8 h per day was 2.51 times higher than that of their counterparts who worked fewer than 8 h per day (AOR: 2.51; 95% CI: 1.34–1.71). The odds of burnout among healthcare workers who abused at least one substance were 2.52 times higher than those of their counterparts who had not abused any substances (AOR: 2.52; 95% CI: 1.08–5.86; Table 3).
Discussion
This study was conducted among healthcare workers at public Hospital ICUs in Addis Ababa, Ethiopia, to identify the prevalence of burnout syndrome and its associated factors. The findings will also significantly help overcome the problems associated with burnout syndrome among healthcare workers, including a decrease in the quality of care (McElearney et al., 2005), poor interaction with healthcare professionals (Shanafelt et al., 2002), and high turnover rates and absenteeism.
The prevalence of burnout among healthcare workers at public Hospitals in ICUs in Addis Ababa was 28.7% (95% CI: 25.1–33.1). This study was found to be low when compared with a study done at Jimma University Teaching Hospital (JUTH), Ethiopia (82.8%) (Biksegn et al., 2016). Public Hospitals in South West Ethiopia (Belay et al., 2021), in China (56.03%) (Zhang et al., 2020), and in Spain (69.2%) (Siguero et al., 2003). In contrast to the other study, this study was found to be higher than the studies conducted in different areas, specifically in Italian and Dutch, which had rates of 2% and 10%, respectively (Pisanti et al., 2011), and in Brazil, 12% (Gil-Monte et al., 2011).
The possible explanation for the difference in prevalence may be attributed to variations in study settings, populations, tools, and methodologies. For instance, the studies conducted in Brazil and at JUTH, Ethiopia, used the Spanish burnout inventory-educational version (SBIEd) and Copenhagen's burnout inventory tool to assess burnout syndrome, respectively, which differs from our tool (MBI-HSS). In contrast to this, the majority of healthcare workers from developed countries like Italy might have a good educational status, a job title, and strong social support. In this study, however, there were respondents with low social support, fatigue syndrome, psychological distress, and major sleeping problems, which could contribute to the development of burnout syndrome (Pisanti et al., 2011).
Age was identified as a factor related to burnout among healthcare workers. Health workers older than 40 years have a 2.82 times higher chance of experiencing burnout compared to those under 30 years (AOR: 2.82; 95% CI: 1.23–6.46). This finding aligns with the results of a study conducted in Ethiopia (Adbaru et al., 2019; Zewdu et al., 2017). This could be explained by the fact that when people remain in the same job for a long time, there is nothing new to do, rendering the position monotonous. Furthermore, because the individual has been in the same role for an extended period, there is a risk that they may overwork themselves and become exhausted.
Years of experience were identified as a factor associated with burnout among healthcare workers. The odds of experiencing burnout among healthcare workers with 5 to 10 years of work experience were 4.81 times higher (AOR: 4.81; 95% CI: 2.92–7.92), and those with more than 10 years of work experience faced odds 3.96 times higher (AOR: 3.96; 95% CI: 1.67–9.39) compared to those with less than 5 years of work experience. This finding is in line with the studies conducted in Greece (Fradelos et al., 2014). In Public Hospitals in South West Ethiopia (Belay et al., 2021), and Amhara, Ethiopia (Adbaru et al., 2019). This might be explained by that nurses who work for long durations of time in the health setting are more subject to emotional exhaustion, lack of energy, and general fatigue, which in turn leads to the development of burnout syndrome (Duli, 2016).
Longer working hours per day were identified as a factor linked to burnout among healthcare workers. The risk of burnout among healthcare workers who worked more than 8 h a day was 2.51 times higher than that of their counterparts who worked fewer than 8 h a day (AOR: 2.51; 95% CI: 1.34–1.71). This finding aligns with other studies that have demonstrated that extended working hours and increased night shifts significantly elevate the risk of burnout (Al-Dubai & Rampal, 2010; Ashkar et al., 2010). This may depend on the work organization, as daytime healthcare workers perform procedures, while at nighttime, there is minimal work to avoid disturbing patients. This results in an increased workload during the daytime (Fernandes et al., 2018).
The odds of burnout among healthcare workers who abused at least one substance were 2.52 times higher than those of their counterparts who had not used any substances (AOR: 2.52; 95% CI: 1.08–5.86). This finding is supported by a study conducted in Malawi (Jung & Baek, 2020; Lecca et al., 2020). This may be because substance abuse can lead to depression, anxiety, and dependency. Every profession requires the employee's commitment and time, and those who abuse substances may struggle to fulfill these expectations. This can result in decreased job performance and fatigue.
Strengths and Limitations of the Study
The first strength is that we included healthcare professionals from various departments in multicenter hospitals, which increases generalizability and ensures a high response rate. Our study also has some limitations that must be considered. The data were collected through self-reports from the respondents, which may lead to under- or over-reporting of the outcome variable. Furthermore, the temporality and causality of the observed associations could not be assessed due to the cross-sectional study methodology.
Implications for Practice
Investigating burnout in ICU professionals has multifaceted implications for practice, ultimately aiming to improve healthcare worker wellbeing, optimize the ICU environment, and enhance patient care. The research findings will inform the development and implementation of targeted interventions to prevent burnout and provide early identification, such as stress management training, counseling services, and peer support groups. The study can highlight the importance of self-care practices, empowering healthcare workers to adopt strategies that mitigate burnout.
Investigating burnout syndrome can provide evidence to support the allocation of resources toward interventions that address burnout, such as increasing staffing levels and providing mental health support, and implementing workload management strategies. The study can inform the development of policies at the hospital, regional, or national level that address the systemic factors contributing to burnout among healthcare workers in ICUs. This includes policies related to working hours, mandatory breaks, and access to mental health services. In addition, it can provide evidence to advocate for greater recognition of the importance of healthcare worker’ wellbeing and the need for systemic changes to support their mental and physical health.
Conclusion
This study provides valuable insights into the factors contributing to burnout syndrome among healthcare workers in ICUs. It suggests that factors such as age, years of experience, daily working hours, and substance use may increase the likelihood of experiencing burnout.
The significant association of burnout with regretting career choice and other factors underscores the urgent need for stakeholders such as mentors, policymakers, healthcare leaders, and facility in-charges to implement targeted interventions aimed at reducing burnout and its adverse effects.
These interventions may include actions like expanding access to mental health services for healthcare providers, strategies to better distribute workload by implementing efficient staffing schedules, hiring enough healthcare providers, and promoting work–life balance through flexible scheduling and adequate rest periods.
Recommendations
Based on the results of this study, we recommend us follow.
♦ Hospital management should provide trainings that focus on stress inoculation, relaxation, time management, and assertiveness programs. ♦ Health facilities to improve remuneration strategies to enhance job satisfaction, reduce financial stress, and increase a sense of being valued at work. ♦ Government and other nongovernmental organizations to increase the number of healthcare providers at peripheral facilities to reduce the patient load per healthcare provider. ♦ Since we found a higher prevalence of burnout, we recommend further studies of qualitative studies to get a deeper understanding of burnout on overall patient outcomes and patient satisfaction concerning burnout among healthcare providers.
Overall, healthcare facilities and policymakers need to recognize the effects of burnout on their staff's well-being. Implementing measures like regular mental health support services, staff rotation, and workload management can significantly reduce burnout and improve the overall quality of patient care in these high-stress environments.
Supplemental Material
sj-docx-1-son-10.1177_23779608251366384 - Supplemental material for Magnitude and Associated Factors of Burnout Syndrome Among Healthcare Professionals Workers in Intensive Care Units, Addis Ababa, Ethiopia, 2023
Supplemental material, sj-docx-1-son-10.1177_23779608251366384 for Magnitude and Associated Factors of Burnout Syndrome Among Healthcare Professionals Workers in Intensive Care Units, Addis Ababa, Ethiopia, 2023 by Mustofa Hassen Yesuf, Zewdie Aderaw Alemu, Abdurehman Seid Mohammed, Natnael Fekadu Tekle, Solyana Haileselassie Admassie and Getachew Mekete Deress in SAGE Open Nursing
Supplemental Material
sj-doc-2-son-10.1177_23779608251366384 - Supplemental material for Magnitude and Associated Factors of Burnout Syndrome Among Healthcare Professionals Workers in Intensive Care Units, Addis Ababa, Ethiopia, 2023
Supplemental material, sj-doc-2-son-10.1177_23779608251366384 for Magnitude and Associated Factors of Burnout Syndrome Among Healthcare Professionals Workers in Intensive Care Units, Addis Ababa, Ethiopia, 2023 by Mustofa Hassen Yesuf, Zewdie Aderaw Alemu, Abdurehman Seid Mohammed, Natnael Fekadu Tekle, Solyana Haileselassie Admassie and Getachew Mekete Deress in SAGE Open Nursing
Footnotes
Abbreviations
Acknowledgments
The authors thank GAMBY Medical and Business College for its support. The authors extend their gratitude to the hospital managers and unit team leaders for their cooperation during the data collection process. The authors would like to express their heartfelt thanks to their data collectors and friends who supported them in this research work.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Institutional Review Committee of GAMBY Medical and Business College, with the ethical reference number V685/14/07/2023. A formal letter was submitted to the Addis Ababa Health Bureau and each selected study hospital, ensuring permission to maintain confidentiality. Verbal and written informed consent were presented and obtained from each study participant under the principles of the Helsinki Declaration. The Declaration of Helsinki was considered, and its principles and recommendations were utilized.
Authors’ Contributions
MHF, ZDL, ASM, NFT, SHD, and GMD have contributed to the conceptualization, data curation, formal analysis, investigation, methodology, resources, software, supervision, validation, visualization, writing—original draft, and writing—review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest in the research, authorship, and/or publication of this article.
Availability of Data and Material
The data of this study will be available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.