
Abstract
Introduction
Health habits like type 2 diabetes self-care may be influenced by masculinity. Nevertheless, there is limited evidence from research that quantitatively assesses the relationship between masculinity and self-care among Mexican adult men with type 2 diabetes.
Objective
The purpose of this study was to investigate the association between masculinity and self-care behaviors in Mexican adult men with type 2 diabetes.
Methods
A cross-sectional, correlational study was conducted with adult men previously diagnosed with type 2 diabetes at five primary healthcare centers. Data was gathered between February and June of 2019. The Conformity to Masculine Norms Inventory and Summary of Diabetes Self-Care Activities questionnaire were employed. SPSS v.26 was used to conduct correlations and multiple linear regression analysis.
Results
A total of 221 adult males participated (mean age = 52.4 years, SD = 9.8; time of diabetes evolution = 8.9 years, SD = 5.8). Alcohol consumption was reported by 42.5%, 25.3% reported smoking, and 17.6% stated having previously been diagnosed with hypertension. Masculinity was negatively correlated with self-care behaviors, including diet (r = −.200, p = .003), self-monitoring of blood glucose (r = −.133, p = .038), foot care (r = −.268, p = .001), and oral hygiene (r = −.283, p = .001). Homophobia, self-reliance, risk-taking, violence, and control over women were aspects of masculinity that were negatively associated with self-care. In regression analyses, total masculinity predicted lower diabetes self-care, with homophobia and violence emerging as significant negative predictors.
Conclusions
Masculinity was negatively associated with self-care in Mexican adult men with type 2 diabetes, particularly in the dimensions of diet, self-monitoring of blood glucose, foot care, and oral hygiene. In order to increase self-care adherence, improve glycemic control, avoid complications, and lower premature mortality, future interventions should address these features of masculinity.
Introduction
Type 2 diabetes (T2D) is the most prevalent form of diabetes worldwide, with a higher burden in low- and middle-income countries (International Diabetes Federation [IDF], 2025). Globally and in North America, men exhibit higher prevalence and mortality rates. However in Mexico, women are more likely than men to have T2D, whereas males are more likely than women to die young from diabetes between the ages of 25 and 64 (Montoya et al., 2023; Vega-López & González-Pérez, 2021). Oaxaca is one among the top ten states in Mexico for diabetes-related mortality (Instituto Nacional de Estadística y Geografía [INEGI], 2024).
Furthermore, poor glycemic control (HbA1c > 7%) is reported by 69.6% of Mexican diabetics (Rojas-Martínez et al., 2023). In order to maintain glycemic control, avoid complications, and lower mortality, people with diabetes must participate in a range of self-care activities after being diagnosed (Ahmad & Joshi, 2023). Maintaining a nutritious diet, using prescription drugs or insulin, and participating in regular aerobic or anaerobic physical activity are important self-care practices (American Diabetes Association Professional Practice Committee, 2025). Oral hygiene practices should be regarded as crucial self-care activities in the management of T2D since current research has demonstrated that they enhance glucose control and lower mortality (Lipman et al., 2023; Zhang et al., 2023).
Nonetheless, adherence to self-care practices among diabetics in Mexico is still below ideal (Cortés-Hernández et al., 2025; Mendoza-Catalán et al., 2022). While adherence to lifestyle changes, such as diet and exercise, is rather poor, the majority of patients take their medications more regularly (da Rocha et al., 2020). Men are disadvantaged when it comes to diabetic self-care because factors including age, education level, and female gender are linked to higher adherence to these recommendations (Baroni et al., 2022; Villalobos et al., 2020). Adherence to conventional masculine norms may have an impact on poor self-care among Mexican adult men with T2D, which could lead to increased morbidity and mortality.
Review of Literature
A collection of societal standards, beliefs, and attitudes that specify the anticipated actions of men in society are collectively referred to as masculinity. These standards frequently place an emphasis on strength, independence, taking risks, and emotional control, according to hegemonic masculinity (Connell & Messerschmidt, 2005; Evans et al., 2011). According to Courtenay (2000), men's health behaviors might be adversely affected by adhering to these conventional masculine ideals. Men may resist getting medical attention, disregard preventive measures, or take risks in order to project an image of toughness and independence. Adult Mexican men with T2D may find it especially difficult to live up to these expectations. Men who exhibit higher levels of traditional masculinity are less likely to accept their diagnosis, according to a number of studies (Mendoza-Catalán et al., 2021). Many males are reluctant to publicly admit they have diabetes because they feel ashamed of the condition (Testerman & Chase, 2018). Because diabetes is seen as undermining independence and dignity (Bhattacharya, 2024), males frequently conceal their disease at work and ignore self-care activities out of fear of being stigmatized (Dale et al., 2015). According to Hawkins et al. (2017), some men think they can handle their disease on their own and that medical visits are not necessary. Others go for alternative therapies because they believe that medical advice is ineffective (Idris et al., 2019).
It is crucial for nurses to comprehend the specific elements that lead to poor adherence to self-care, including the impact of masculinity on the self-care behaviors of men with diabetes. In the context of secondary prevention, nursing practice focuses on health education and attempts to avoid consequences related to chronic illnesses. This knowledge may help create more successful treatments to enhance men's diabetes self-care. This study sought to quantitatively investigate how masculinity affects self-care in males with diabetes, in contrast to earlier research, which has mostly been qualitative. It specifically examined the connection between self-care practices and masculinity in Mexican adult men with T2D.
Methods
A correlational, cross-sectional investigation was carried out. In order to quantitatively investigate the relationship between diabetes self-care practices and masculinity, this approach was selected. Adult men with a diagnosis of T2D between the ages of 20 and 79 who were treated at five primary health facilities along the coast of Oaxaca, in southwest Mexico, made up the target population. The requirements for inclusion were living in the state of Oaxaca, being between the ages of 20 and 79, and having a prior diagnosis of T2D for at least a year. Men who self-reported having major surgery within the previous six months that restricted their capacity to engage in self-care activities, had been diagnosed with mental health conditions (such as dementia or schizophrenia), or had acute symptoms that prevented them from completing the questionnaires on the day of their clinic visit were not allowed to participate. For a multiple linear regression analysis, the sample size was determined using G*Power version 3.1.9.2, assuming a 95% confidence level, statistical power of 0.90, and an effect size of 0.20 (Mendoza-Catalán et al., 2018). Sampling was conducted by convenience.
Questionnaires
Diabetes Self-Care
Diabetes self-care was assessed using the Summary of Diabetes Self-Care Activities questionnaire (Toobert et al., 2000). Oral hygiene activities have been identified as essential daily practices for individuals with T2D, as they contribute to better glycemic control, prevent gingival recession and tooth loss, and reduce cardiovascular risk (Lipman et al., 2023; Zhang et al., 2023). Two essential behaviors (brushing and interdental cleaning) were chosen in order to determine the most pertinent oral hygiene practices associated with glycemic control. Four questions were then modified to conform to the original SDSCA's structure and response format. The oral hygiene subscale demonstrated acceptable internal consistency (α = 0.72). The final version included 14 items across five domains: diet, exercise, self-monitoring of blood glucose (SMBG), foot care, and oral hygiene behaviors. Each item assessed the frequency of behaviors over the past seven days (scored 0–7), with higher scores indicating greater self-care adherence. The questionnaire demonstrated adequate reliability, with Cronbach's Alpha = 0.76 and McDonald's Omega = 0.79.
Masculinity
The 22-item Conformity to Masculine Norms Inventory (Mahalik et al., 2003), modified for the Mexican context, was used to assess masculinity (Mendoza, 2017). Eleven aspects of masculinity are measured by this inventory: the importance of work, the desire for status, risk-taking, emotional control, dominance over others, violence, winning, power over women, playboy, independence, and homophobia. A 4-point Likert scale, with 0 representing “strongly disagree” and 3 representing “strongly agree,” is used to score each topic. Higher scores indicate better adherence to masculine norms; scores can also be provided per dimension. The responses are added together to produce a total score. With McDonald's Omega = 0.80 and Cronbach's Alpha = 0.75, the instrument showed adequate reliability.
Covariates
Age, marital status, years of schooling, number of working days per week, average daily working hours, alcohol use, smoking, hypertension, antihypertensive medication, waist circumference, body mass index (BMI), and systolic and diastolic blood pressure were also recorded.
Data Collection
Face-to-face interviews in a confidential setting offered by the health center were used to gather data. On the day of their scheduled medical appointment, participants were contacted in the waiting area. By evaluating the exclusion criteria and inquiring about a previous T2D diagnosis, eligibility was verified. Informed consent was read aloud, study objectives were presented, and eligible males were requested to participate. A copy of the consent form was given to each participant for their records after they signed it. Participants were then led to a secluded space to fill out questionnaires and take anthropometric measures. In 2019, information was gathered from February to June. The study was approved by the Research Ethics Committees of the Faculty of Nursing at the Autonomous University of Baja California (approval number 0191084).
Data Analysis
Data were entered and analyzed using IBM SPSS Statistics version 26 for Windows. Categorical variables were summarized using frequencies and percentages, while continuous variables were reported as means and standard deviations. For the overall and domain-specific scores of diabetes self-care, values were averaged on a 0–7 scale, to facilitate comparisons. Spearman's correlation was used to examine the relationships between masculinity and diabetes self-care, both overall and by questionnaire domains. Sociodemographic characteristics and anthropometric measurements were also included in the analysis. Finally, multiple linear regression analyses were conducted with diabetes self-care as the dependent variable. In the first model, the total masculinity score was included, and in the second model, the individual masculinity dimensions were entered separately. Both models were adjusted for covariates, and all regression assumptions were verified and met prior to analysis. Statistical significance was set at p < .05.
Results
The study included 221 adult men with T2D and the majority were married and had finished primary school, with a mean age of 52.4 years (SD = 9.8). The participants reported working 8.1 h a day, 5.4 days a week, and sleeping 6.3 h a night on average. The average time since being diagnosed with diabetes was 8.9 years. In terms of lifestyle and health factors, 17.6% had previously been diagnosed with hypertension, 25.3% were current smokers, and 42.5% reported drinking alcohol. In all, 62.9% of participants’ waist circumferences were larger than 94 cm. Although slightly raised, the systolic and diastolic blood pressure readings were also within normal levels (see Table 1).
Sociodemographic and Clinical Characteristics of the Participants.

Note. M = mean; SD = standard deviation; n = frequency; % = percentage; WC = waist circumference; BMI = body mass index.
Overall, there was a lack of diabetes self-care, and the masculinity scores were within the average range of the entire survey. In terms of self-care domains, participants indicated that they adhered to their diet the most frequently, followed by exercise, oral hygiene, foot care, and SMBG (see Table 2). Power over women, playboy conduct, and aggression were found to have the lowest ratings among the masculine aspects, whereas winning, pursuing status, and prioritizing work were found to have the greatest scores.
Description of Masculinity and Diabetes.

Note. M = mean; SD = standard deviation; SMBG = self-monitoring of blood glucose.
Correlations Between Masculinity and Diabetes Self-Care
Masculinity was associated with lower overall diabetes self-care, as well as with lower educational level, fewer hours of sleep, alcohol consumption, smoking, and a previous diagnosis of hypertension. Conversely, participants with higher self-care scores were associated with lower waist circumference, work hours, BMI, alcohol consumption and smoking (see Table 3).
Correlation Analysis Between Masculinity, Self-Care, and Participant Characteristics.
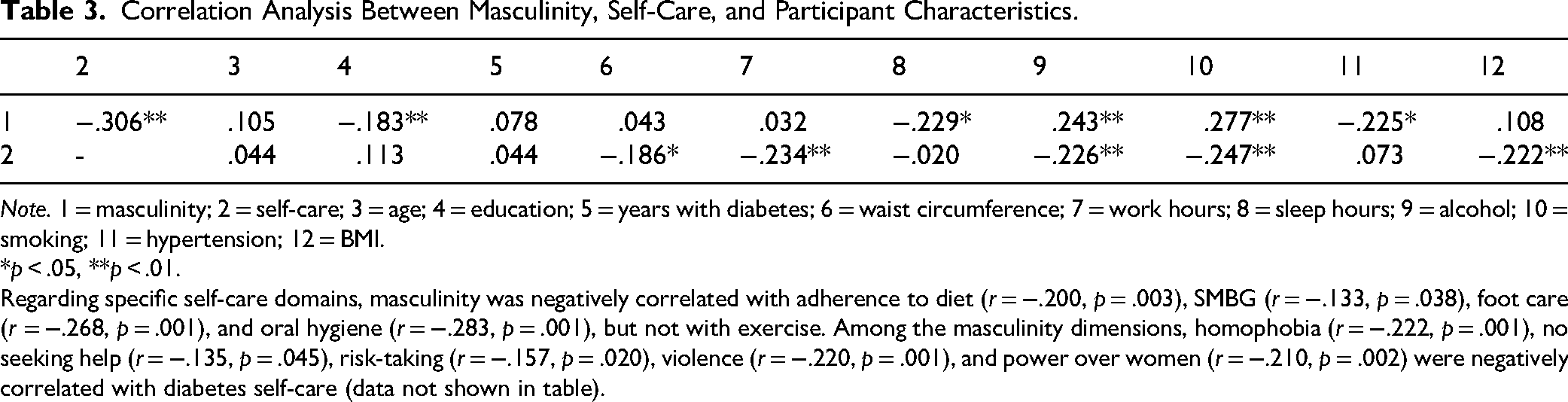
Note. 1 = masculinity; 2 = self-care; 3 = age; 4 = education; 5 = years with diabetes; 6 = waist circumference; 7 = work hours; 8 = sleep hours; 9 = alcohol; 10 = smoking; 11 = hypertension; 12 = BMI.
*p < .05, **p < .01.
Regarding specific self-care domains, masculinity was negatively correlated with adherence to diet (r = −.200, p = .003), SMBG (r = −.133, p = .038), foot care (r = −.268, p = .001), and oral hygiene (r = −.283, p = .001), but not with exercise. Among the masculinity dimensions, homophobia (r = −.222, p = .001), no seeking help (r = −.135, p = .045), risk-taking (r = −.157, p = .020), violence (r = −.220, p = .001), and power over women (r = −.210, p = .002) were negatively correlated with diabetes self-care (data not shown in table).
Multiple Linear Regression Analysis
In the multiple linear regression model, the total masculinity score was found to have a negative effect on diabetes self-care activities (R2a = 0.153, F = 5.499, p = .001). When the individual masculinity dimensions were included in the second model, only homophobia and violence retained a significant negative effect on self-care (R2a = 0.203, F = 6.280, p = .001) (see Table 4).
Multiple Linear Regression Model for Diabetes Self-Care.

Note. βa = standardized beta, b = adjusted model: age, education, years with diabetes, waist circumference, work hours, sleep hours, alcohol consumption, smoking, hypertension, BMI.
Discussion
This study looked at the relationship between self-care and masculinity in Mexican adult men with T2D. The results showed a correlation between lesser adherence to diabetes self-care and greater masculinity scores. This correlation was especially clear when it came to the aspects of violence and homophobia.
In line with other research in Mexican populations (Mendoza-Catalán et al., 2018), the participants’ masculinity scores were close to the middle of the scale, indicating that men do not fully embrace all traits of traditional masculinity. Power over women, playboy behavior, and aggression were the least common attributes in this survey, whereas winning, pursuing social status, and prioritizing work were the most prevalent. According to Mahalik et al. (2003), these characteristics are a reflection of what society expects from a man in both his private and public life. Therefore, men recognize that maintaining their health is important to fulfill their roles as economic providers and caregivers. Remaining active at work is often perceived as a sign of health. Seeking medical care may be considered unnecessary as long as they can continue working (Bhattacharya, 2024; Idris et al., 2019). Workplace competitiveness, as a hierarchical expression of masculinity, is associated with health-related behaviors. Men may prioritize work over health to maintain both professional and masculine status (Dale et al., 2015).
The findings also demonstrate that men with T2D, especially in SMBG, had inadequate self-care, which is consistent with findings from low- and middle-income nations (Mogre et al., 2019). SMBG is linked to a significant decrease in glycated hemoglobin and is crucial for people who are at high risk of hypoglycemia (Ajjan et al., 2023). According to earlier research, Mexican-American men are less likely than non-Hispanic whites and non-Hispanic blacks to have SMBG, which is associated with worse glycemic control (Harris et al., 1999). Access to SMBG may be restricted by a number of factors, such as individual resources, knowledge of SMBG, and opinions regarding its value for controlling blood sugar (Cuevas et al., 2015). The men with T2D in the sample under analysis were from southern Mexico, where there are significant differences in the usage of preventive care services. Because it is frequently regarded as an out-of-pocket payment, it constitutes a substantial financial burden for patients (Ewen et al., 2025). Furthermore, patients may have to make the tough decision of buying prescriptions or self-monitoring supplies (glucometer and test strips) due to shortages of antihyperglycemic drugs in healthcare institutions (Vértiz-Ramírez et al., 2024).
Higher masculinity levels were linked to poorer food, SMBG, dental hygiene, and foot care compliance. Self-care is frequently seen unfavorably from a masculine perspective (Allen, 2024). In order to avoid criticism, humiliation, or feelings of inferiority, men with diabetes may forgo self-care activities in social situations or while other men are around since they are stigmatized as being weak or feminine (Whittemore et al., 2019). Inadequate diet compliance may also be a reflection of societal perceptions about food. Meat consumption is considered a sign of masculinity and energy for men. In the workplace, diets that prioritize vegetables or limit red meat may result in mockery and views of diminished masculinity (Rodríguez et al., 2020). Body size and strength are frequently viewed as indicators of masculinity and are crucial for recreation, sports, and professional performance, even though dietary changes can aid in weight loss and improve diabetes control (Fidolini, 2022). Men eat what is most easily accessible due to cultural eating customs and financial limitations that further restrict access to healthful meals (Bhattacharya, 2024). Men's sense of autonomy and dignity may also be threatened by daily glucose self-monitoring since they worry about coming across as weak (Bhattacharya, 2024).
According to earlier studies (Rossaneis et al., 2016; Thomas et al., 2012), men who used tobacco and alcohol reported decreased adherence to self-care. Tobacco and alcohol consumption are socially acceptable habits that support a man's identity (Merdassa, 2024). Diabetes frequently necessitates lifestyle modifications, such as cutting back on drinking and giving up smoking, which can cause social difficulties and feelings of alienation (Chan & Corvin, 2016). The risk of early complications in diabetes is increased by alcohol and tobacco use (Ramírez-García et al., 2024; Trichia et al., 2024). Men's sense of purpose and male identity may be further threatened by disease-related health decline, which could jeopardize employment (Chan & Corvin, 2016). When diabetic self-care is neglected, alcohol drinking may be used as a coping strategy to handle stress (Montesi, 2018). On the other hand, abstaining from alcohol might result in social marginalization, which can reinforce risky behaviors including overeating, drinking again, and being sedentary (Smith-Miller et al., 2022; Testerman & Chase, 2018). Increased alcohol use may be linked to diabetes-related health decline. Diabetes and depression, which are associated with worse health outcomes, may co-occur with this (Strand & Warne, 2019).
The masculine traits that were found to be adversely correlated with self-care using Spearman correlation and linear regression analysis included homophobia and violence, which is a novel discovery. Nevertheless, there is still a dearth of research on T2D self-care in relation to homophobia. One explanation could be that men with diabetes are perceived as having feminine traits when they try to take care of themselves and don’t live up to the manly ideals of bravery and strength (Connell & Messerschmidt, 2005). Guys may be reluctant to ask for assistance in order to avoid coming out as weak or less manly because this is frequently linked to teasing from other guys. This can be mirrored in homophobic attitudes (Testerman & Chase, 2018). According to Courtenay (2000), men may be reluctant to participate in health-promoting activities when they are ill because other men may see such actions adversely. Because of this, they frequently try to uphold their feeling of masculinity in accordance with social norms. It has been demonstrated that machismo causes Latino males to put off seeking medical attention until diabetes issues become apparent (Hawkins et al., 2017). This may imply that men are more likely to experience problems due to their homophobic views toward self-care.
On the other side, males may use violence to express their feelings and anxieties in an attempt to avoid appearing vulnerable. Violence is frequently seen as a valid form of control and authority from the standpoint of hegemonic or toxic masculinity (Corvo & Golding, 2022). According to Hawkins et al. (2017), Quaglia (2020), and Ramírez-Morros et al. (2024), men may also engage in self-directed violence in this setting by displaying stoicism, downplaying their sickness, and postponing self-care. Additionally, when family members witness self-care neglect, their attempts to provide support may be received with hostility, which ultimately results in a decrease in family involvement to prevent conflict (Mendoza-Catalán et al., 2018). In some educational, familial, and social environments, violence is seen from an early age as a means of establishing control, authority, and power. In the Mexican sociocultural framework, these actions are socially acknowledged and supported by other men as manifestations of machismo (Núñez Noriega, 2016). According to research, Mexican men who use violence frequently do so in order to resolve conflicts or defend themselves (Meneses Reyes, 2020). As a result, it is crucial to establish specific scales to assess violence. These scales should be carefully created and validated to capture how men perceive and express this complicated dimension, which will eventually influence customized approaches to their treatment.
Clinical and Research Implications
Nursing professionals may encounter challenges since males with T2D often show low participation in diabetes self-care interventions or general health education programs (de Paiva Neto et al., 2020). Even when males have participated in diabetic care programs, these interventions have not consistently led to improvements in attitudes or behavior (Krag et al., 2016). Research and the creation of evidence-based solutions are challenged by this. The results of this study enable the authors to identify a number of research and instructional areas of interest. Education programs need to improve and broaden the competencies of nursing students in relation to the male population. In order to support men's commitment to their well-being, it is necessary to understand the particular health needs and difficulties they encounter, as well as to be able to effectively communicate, demonstrate empathy, and establish a therapeutic alliance (Oliveira et al., 2020; Rosu et al., 2017). In a similar vein, developing health literacy programs for men is crucial since it may promote early detection, treatment compliance, and their participation in preventative measures (Zanchetta et al., 2023). Additionally, gender-responsive assessment tools are needed to identify men's health needs (Santos et al., 2020). Last but not least, policies that enhance and modify health care to suitably address the particular needs of men must be encouraged (Sousa et al., 2021). These educational, clinical, and policy-focused initiatives may have a direct impact on nursing practice and health education programs aimed at improving involvement, adherence, and outcomes for men with T2D. Based on behavior change theories, nurses should offer individualized lifestyle-change interventions. Additionally, they ought to provide diabetes self-management education and support that is tailored to men and the local context, taking into consideration cultural customs and the ways that masculinity can affect health-related behaviors (ADA Professional Practice Committee, 2025; IDF, 2015).
The nursing professional should assess and identify characteristics of masculinity such as homophobia and violence that have been associated with low levels of self-care among men with T2D. In this regard, it is essential to incorporate men's beliefs, attitudes, and traditional masculine norms into educational and behavioral interventions, including those related to hegemonic or toxic forms of masculinity that may hinder the adoption of healthy behaviors. From this perspective, nursing interventions should aim to promote self-care in T2D as an expression of personal responsibility, autonomy, and fulfillment of the masculine role, thereby fostering the development of healthier forms of masculinity that do not conflict with health-related behaviors. Finally, the creation of community-based programs led by nursing professionals for men with T2D is recommended, providing safe spaces where participants can share experiences, fears, and concerns without feeling vulnerable or stigmatized.
Strengths and Limitations
This is one of the first quantitative studies to address the underexplored topic of masculinity and self-care in Mexican adult men with T2D. The findings contribute valuable evidence that can guide the design of strategies and programs specifically tailored to the male population with diabetes to improve glycemic control and reduce the risk of complications. As a cross-sectional study that relied on self-reported data, causal relationships cannot be inferred from the findings. Additionally, the findings should be interpreted within the specific cultural context of southern Mexico, where meanings and expressions of masculinity may differ from those in other regions of Mexico or in other countries. The use of convenience sampling highlights the need for future studies to employ randomized sampling methods. It is also important for future research to include biochemical variables such as HbA1c and lipid profiles to better understand how masculinity influences these health indicators.
Conclusions
The results showed that among Mexican adult men with T2D, the masculinity aspects of aggression and homophobia were inversely correlated with self-care. Nursing providers should see these features as new potential to enhance self-care in this population, since they represent traditional manifestations of masculinity in southern Mexico. Furthermore, this highlights the critical need to develop new, empirically supported therapies to lessen homophobia and violence so that men may take care of themselves and embrace their condition without viewing it as a threat to their masculinity. Similarly, it is crucial to improve nursing staff's capacity to promote empathy, carry out suitable evaluations, and address the unique needs of men. Future research should incorporate longitudinal designs to examine the long-term impact of traditional masculinity on self-care, the development of complications, and mortality among men with T2D. In addition, it is a priority to design and evaluate gender-sensitive nursing interventions aimed at strengthening self-care and therapeutic adherence, taking into account masculine norms and their influence on health-related behaviors.
Footnotes
Acknowledgments
The authors acknowledge the support of Universidad Autónoma del Estado Hidalgo.
ORCID iDs
Ethical Approval
The study protocol was approved by the Ethics and Research Committee of the School of Nursing, Universidad Autónoma de Baja California (approval number 019-1-084).
Informed Consent
Both written and verbal consent were obtained from the patients.
Author Contributions
GM-C: conceptualization, methodology, formal analysis, writing—original draft, supervision, approval of the final manuscript. ASJ-O: data curation, investigation, writing—review & editing, approval of the final manuscript. JA-G: methodology, validation, writing—review & editing, approval of the final manuscript. DE-L: data curation, formal analysis, visualization, writing, approval of the final manuscript. NL-G: investigation, writing—review & editing, critical revision, approval of the final manuscript. IV-G: writing—review & editing, critical revision of the manuscript, approval of the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication of this article was funded by the Universidad Autónoma del Estado Hidalgo.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.