
Abstract
Introduction
More than a third of diabetes patients undergo surgery at least once in their lifetime. However, there is limited research on managing the needs of these patients after hospital discharge.
Objective
This study aimed to determine the effect of home care on glycosylated hemoglobin (HbA1C) and quality of life in type 2 diabetes patients discharged from hospitals.
Methods
This study was a randomized clinical trial. About 69 type 2 diabetes patients undergoing surgery were assigned to intervention and control groups after discharge orders. Home care was provided for three months with an interprofessional approach. Data collection tools included diabetes-related quality of life questionnaire and laboratory tests. Data were analyzed using SPSS version 23 with parametric and non-parametric tests.
Results
HbA1C levels decreased significantly in the intervention group over the three-month period (P < 0.05), whereas this decrease was not significant in the control group (P > 0.05). The mean quality of life scores improved in satisfaction and future concern domains in the intervention group and in the social concern domain in the control group (P < 0.05). The mean changes in total quality of life scores over three months post-discharge were not significant in both groups (P > 0.05).
Conclusions
The findings of this study indicate that structured home care delivered through a team-based approach contributes not only to improved glycemic control but also to enhancing specific dimensions of quality of life—particularly satisfaction with life despite diabetes and reduced concerns about the future—in post-surgical diabetic patients. These results emphasize the importance of incorporating such services into post-discharge care plans to support patient well-being and recovery.
Introduction
Diabetes is a global, multifactorial, and complex public health challenge that has seen a rising impact on social and economic fronts akin to an epidemic. The prevalence of diabetes worldwide has doubled over the past 20 years and constitutes a significant portion of non-communicable diseases (NCDs) (Organization, 2021, Esteghamati et al., 2017). The increasing prevalence and longer lifespan of individuals with diabetes, particularly in developing countries, have escalated the need for surgical interventions among these patients. It is estimated that approximately 25% to 50% of these individuals will require surgery during their lifetime, and currently, around 25% of all hospitalized patients are people with diabetes (Ostling et al., 2017, Crowley et al., 2023). Anesthesia and surgical procedures induce metabolic changes that complicate blood glucose control in patients with diabetes. There is a direct correlation between postoperative complications and blood glucose levels in patients with diabetes, indicating the detrimental impact of elevated blood sugar on exacerbating complications and disease progression (Rollins et al., 2016, Parish et al., 2017, Zhang et al., 2022).
Hospitalization of individuals with diabetes significantly impacts their quality of life. Recent studies on the post-discharge quality of life in patients with chronic diseases such as diabetes have shown that recurrent hospitalizations are directly associated with decreased quality of life and increased patient mortality. Patients’ inability to manage post-discharge stresses and consequently the lack or ineffective implementation of post-discharge care plans are among the reasons for recurrent hospitalizations (Tamornpark et al., 2022, Wróblewska et al., 2023). The aspect of quality of life is crucial because neglecting it can lead to despair, lack of motivation for any effort, and reduced social, economic, cultural, and health activities, ultimately affecting social and economic development of communities in profound ways. In other words, improving physical health for individuals, disregarding quality of life, is particularly challenging for those with chronic diseases such as diabetes (Zhang et al., 2022, Tamornpark et al., 2022, Wróblewska et al., 2023). Moreover, the level of HbA1C, as an indicator of blood glucose control in different individuals, varies based on treatment expectations, duration of diabetes, life expectancy, and the presence or absence of different support systems. Nonetheless, achieving and maintaining optimal levels of HbA1C has been shown to significantly reduce the risk of diabetes-related complications. Therefore, providing strategies for better HbA1C control in hospitalized and post-discharge patients with diabetes can potentially enhance their quality of life in various dimensions (Boye et al., 2022, American Diabetes Association. Standards of Care in Diabetes-2023.Diabetes Care).
When an individual requires post-discharge care and prefers to remain at home, but continuous care cannot be easily or effectively provided by family and friends, effective healthcare team communication with the patient and continuity of post-discharge care have had a positive impact on patient recovery (Rubin et al., 2022, Caraballo et al., 2019, Moro and Caliri, 2016). Indeed, creating awareness, attitudes, and patient skills in managing their illness is crucial to facilitating post-discharge situations, reducing the gap between post-discharge needs and patient functional capacity, thus increasing the patient's sense of independence (Bellier-Teichmann et al., 2022, Low et al., 2015). Home care is a solution that fosters coordination between healthcare service providers and patients, ensuring patient safety with continuous care. Numerous studies, including systematic reviews, have confirmed the effectiveness of home care in reducing mortality, preventing rehospitalization, improving patient functional capacity, and enhancing quality of life in patients with congestive heart failure, elderly patients with fractures, and patients with cardiovascular, respiratory, and neurological diseases (Finlayson et al., 2018, Mikhael et al., 2020, He et al., 2023).
The home care approach is a team effort where nurses assess the patient's needs and problems in the home environment, provide consultation by contacting physicians if necessary, and this process potentially impacts glycemic control in adults with diabetes as a preventive measure to delay diabetes-related complications (Fernández-Medina et al., 2021). Home care nursing does not solely focus on the patient but also includes addressing the needs of family members and other individuals interacting with the patient for maximum health outcomes (Barker et al., 2017).
Review of Literature
Numerous studies have investigated the effects of surgery and anesthesia on glycemic control in patients with diabetes. M. Vasantha Kumar and B. Ravi (2019) conducted a retrospective study on 100 patients with diabetes undergoing surgery to compare changes in blood pressure (BP), blood glucose levels, heart rate (HR), and visual analog scale (VAS) scores under general versus regional anesthesia. The findings indicated higher post-operative blood glucose levels and significant fluctuations in glucose, BP, and HR with both types of anesthesia (KUMAR and Ravi, 2019). Similarly, Lingala et al. (2024) carried out a one-year prospective cohort study evaluating the role of postoperative glycemic control in reducing surgical site infections (SSIs) in 75 patients undergoing abdominal surgeries. SSIs were assessed on days 7, 14, and 30 post-operations. The study found a significant reduction in both HbA1C levels and SSI incidence among patients who maintained blood glucose within the target range(Lingala et al., 2024).
Given that one of the most important expected outcomes of glycemic control is the improvement and maintenance of quality of life in individuals with diabetes, several studies have explored this aspect as well. Haririan et al. (2007) conducted a descriptive cross-sectional study in Iran assessing the quality of life in 150 patients with diabetes selected through simple random sampling. The results revealed poor quality of life, particularly in the physical and social domains (Hamidreza Haririan et al., 2007). Wróblewska et al. (2023) studied the quality of life of 294 elderly patients with diabetes in Poland using a researcher-developed questionnaire including clinical and sociodemographic information, the WHOQOL-Bref, the Acceptance of Illness Scale (AIS), the Self-Care of Diabetes Inventory (SCODI), and the Geriatric Depression Scale (GDS). Findings demonstrated significant associations between quality of life and body mass index (BMI), education level, and place of residence. Higher depression levels were linked to poorer perceived quality of life, while self-care maintenance was the only significant predictor of quality of life (Wróblewska et al., 2023). AbuAlhommos et al. (2022) conducted a study aimed at evaluating the quality of life in 321 patients with type 2 diabetes in Saudi Arabia. The most commonly reported diabetes-related issues affecting patients’ quality of life were pain/discomfort, followed by mobility problems and symptoms of depression and anxiety (AbuAlhommos et al., 2022).
Several studies have also examined the impact of follow-up care interventions, including patient and family education and home care, on glycemic control in patients with diabetes. Khodaveisi et al. (2018) conducted a randomized controlled trial (RCT) to determine the effect of home care education on blood glucose control in patients with type 2 diabetes. Patients and their families received three training sessions over three weeks, and follow-up evaluations three months later revealed significant reductions in BMI and fasting blood glucose levels (Khodaveisi et al., 2018). Lee et al. (2023), in a pilot retrospective cohort study, evaluated the impact of a home care program for patients with type 1 diabetes. In this study, a multidisciplinary team consisting of physicians, nurses, and nutritionists provided specialized education to 196 patients in the intervention group and conducted regular health assessments through phone calls or text messages. Over a 9-month follow-up period, the findings demonstrated a significant reduction in HbA1c levels and a higher proportion of patients in the intervention group achieving the target HbA1c level (<7.0%) compared to the control group (Lee et al., 2023). Sertbas et al. (2020), in a retrospective study, analyzed biomedical data from 256 patients with diabetes who were being followed by a home health care team. The patients were undergoing various treatment regimens, including oral antidiabetic medications, insulin therapy, or no pharmacological treatment. The findings highlighted the benefits of home care through regular visit programs and individualized treatment plans (Sertbas et al., 2020).
Several other studies conducted in various countries—including clinical trials, systematic reviews, cohort studies, and descriptive studies—have highlighted the benefits of home care for various diseases, including diabetes (Torki-Harchegani et al., 2020, Garg et al., 2017). However, none of these studies have specifically examined the effect of home care in patients with diabetes undergoing surgery and in terms of both glycemic control and quality of life simultaneously. The present study aimed to determine the impact of home care on HbA1C levels and quality of life in patients with type 2 diabetes following surgery, starting from the time of hospital discharge. At the time the study was conducted, although home care was officially recognized within the healthcare system as a component of chronic disease management, there were no mandatory policies or specific clinical protocols for guiding post-surgical home care in patients with diabetes. Accordingly, the care approach used in this study extended beyond existing guidelines, aiming to explore whether structured home care could improve clinical outcomes, promote healing, and reduce recovery time. The study also sought to generate evidence to support the potential development of future care protocols and inform policy decisions in the healthcare system.
Methods
Study Design and Participant
The present study is a randomized clinical trial registered under the code IRCT20190730044386N1. The target population consisted of patients with type 2 diabetes undergoing surgery hospitalized in general and specialized surgery departments across three educational hospitals.
Research Sample
A total of 35 patients were included in each of the intervention and control groups from the research community who met the inclusion criteria.
Inclusion and Exclusion Criteria
Inclusion criteria for the study participants were:
Being diagnosed with type 2 diabetes. Residing in the geographical area of the study setting during the research period. Having the ability to communicate verbally. Having undergone surgery during the sampling period, with a discharge order documented in the medical file. Being 45 years of age or older. Providing informed consent to participate in the study. For illiterate participants, the consent form was read aloud using clear, simple, and easily understandable language, and their verbal consent was obtained in the presence of a witness. For participants in the intervention group, in addition to the patient's consent, informed consent was also obtained from a first-degree family member, as the home care activities required the involvement of such a family member. To ensure continuity and data integrity, the same first-degree relative was involved throughout the entire study, with no changes during the study period.
In cases where the patient in either the intervention or control group is illiterate, informed consent was obtained from a literate first-degree family member who assisted the patient in completing the quality-of-life questionnaire.
The exclusion criteria for both the intervention and control groups were as follows:
Withdrawal of consent to continue participation at any point during the study period. Relocation of the patient's residence outside the geographical boundaries of Isfahan for any reason during the study.
By implementing these criteria, the study aims to maintain methodological consistency while addressing potential literacy and language barriers, ultimately ensuring reliable participation and high-quality data.
By implementing these criteria, the study aimed to maintain methodological consistency while addressing potential literacy and language barriers, thereby ensuring reliable participation and high-quality data.
Sampling Method
In this study, considering the study type, sampling was of the convenient type. The researcher identified eligible patients in the surgical departments throughout the week during morning and afternoon shifts. Patients meeting the inclusion criteria were randomly allocated using block randomization method into either the intervention or control groups. Subsequently, consent was obtained from the patient in the control group and both the patient and a first-degree family member (usually the spouse) in the intervention group. Convenient sampling and random allocation of samples continued until the required sample size was achieved in each of the intervention and control groups.
Random allocation using block randomization was conducted as follows: The total sample size was divided into smaller groups called blocks, with each block containing four individuals. The placement of individuals (four individuals) within each block was as follows: (ACAC, ACCA, CCAA, CAAC, AACC, CACA). Each arrangement was assigned a number (ACAC = 1, ACCA = 2, CCAA = 3, CAAC = 4, AACC = 5, CACA = 6). Numbers were written on uniform-sized spherical beads and placed inside a bag. A preschooler was asked to randomly draw beads from the bag, repeating the process until the required number of blocks was achieved. The number on the bead corresponded to the allocation sequence for sampling.
Data Collection Tools and Their Reliability and Validity
Each question was answered using a five-point Likert scale (ranging from very satisfied to very dissatisfied). Therefore, the average score for each questionnaire item ranged from one to five, where a lower score indicated better quality of life. The score for each domain was calculated by dividing the total score of that domain by the number of items.
The Diabetes Quality of Life Questionnaire (DQOL) was developed in 1988 by Jacobson in English, and its validity and reliability were confirmed in a study titled “Normalization of the Diabetes Quality of Life Questionnaire among Type 2 Diabetes Patients in Isfahan in 2007 by Mousavi and colleagues. The overall reliability of this questionnaire was confirmed with a Cronbach's alpha of 0.89. The estimated time required to complete this questionnaire was 20 min.
Participant Recruitment and Baseline Assessment
The researcher obtained permission to work in surgical departments by obtaining an introduction letter and visiting research environments, introducing herself to surgical department officials, and receiving approval to start work. In the morning and afternoon shifts, patients with type 2 diabetes undergoing surgery who met the inclusion criteria were selected. They were assigned to intervention and control groups using block randomization after explaining the study's objectives and obtaining written consent. Detailed postal addresses and contact numbers of each sample (intervention and control groups) were recorded. Subsequently, quality of life questionnaires and background information were completed by patients in both groups, and blood samples were collected for HbA1C testing.
The blood sampling technique for measuring HbA1C involved collecting a venous blood sample and transferring it to the laboratory within a maximum of one hour, while maintaining the cold chain. In the laboratory, the blood samples could be stored at a temperature of 4 to 8°C for up to three days. However, in this study, all samples were analyzed on the same day they were collected.
During the sampling period, the researcher explained the Diabetes Quality of Life Questionnaire in detail to all participants in both the intervention and control groups. For literate patients, the questionnaire was presented directly to them. In cases where the patient was illiterate, the explanation was provided to a first-degree family member who was responsible for the patient's care. The questionnaire was administered at two time points: once before the intervention and again three months after the intervention. The researcher also addressed and clarified any questions or ambiguities related to the questionnaire items. Accordingly, for illiterate patients, the designated family member read each question aloud to the patient and recorded the patient's responses in the questionnaire.
Patients in the control group were informed that they would be contacted separately three months later for blood sampling for HbA1C testing and to complete the quality-of-life questionnaire again.
Intervention
Initiation of Home Care and Needs Assessment
In the intervention group, the date and time of the first meeting (arranged with the patient and family) were scheduled within the first 24 h after discharge. During this initial meeting, based on the self-management and case management tool, educational, care, therapeutic, and supportive needs were determined and prioritized. According to each patient's needs, an educational and care plan was devised. The implementation of intervention programs such as dressing changes, blood sugar monitoring, dietary recommendations (considering frequent reminders of the target range for blood sugar control and diabetes control indicators) was carried out with the involvement of the family and patient cooperation.
Coordination with Healthcare Professionals and Nutritional Support
Throughout each patient's home care sessions, any medical issues concerning the patient's medication were communicated to the responsible physician at the Endocrine Research Center via WhatsApp, telephone calls, or face-to-face meetings. If additional information about the patient's condition was required, further data were collected under the physician's guidance and communicated to her. If necessary, the patient would be visited by the physician; necessary arrangements regarding the appointment time and day would be scheduled, and with the assistance of the family, the patient would attend the center for visit by the physician and receive necessary orders. The researcher would be informed of any new treatment plans, and if needed, educational and care plans would be revised. If dietary regimen modification was part of the planning, coordination with the nutrition unit of the Endocrine Research Center would be conducted, and based on the nutritionist's recommendations, necessary education and dietary modification advice would be provided to the patient and family during the home care session.
Individualized Follow-Up and Frequency of Home Visits
The researcher closely observed the individual educational and skill needs of patients, such as the need to review medication administration methods, adhere to dietary and medication regimens, monitor physical activity levels, foot care techniques, post-operative care, glucometer usage methods, fluctuations in blood sugar levels, and how to record fasting and postprandial blood glucose levels, blood pressure control, and wound healing progress. Considering that patients or their caregivers used both glucometers and insulin delivery devices (such as syringes or insulin pens) at home, several measures were implemented to ensure safety and accuracy. Prior to initiating the study, patients and caregivers were trained on the correct use of glucometers, including appropriate sampling techniques and interpretation of results. They also received instructions on the safe and personal use of insulin syringes or pens, with emphasis on avoiding device sharing. Additional guidance was provided on hand hygiene, proper handling of blood samples, prevention of bloodborne pathogen exposure, and disposal of used lancets and needles in puncture-resistant sharps containers. Safe storage practices for insulin and injection devices were also discussed.
In the intervention group, the frequency of patient visits and the hours spent at home varied during the first, second, and third months. Patients who maintained their blood sugar within target ranges and could self-manage their blood glucose levels did not require regular home visits but were followed up regularly via telephone calls to monitor their condition. However, in some cases, due to urgent or unforeseen circumstances, unplanned visits or phone calls to families were made within less than four hours of receiving patient status updates. Such situations included sudden fluctuations in blood glucose levels, acute pain, signs of wound infection, or general deterioration in the patient's condition. In these instances, the issue was immediately reported to the research nurse, who maintained continuous communication with the patient and their family via phone or video call until reaching the patient's home, providing guidance on immediate actions they could take. Upon arrival, if necessary, the nurse coordinated with other members of the treatment team, and in critical cases, the patient was promptly referred to specialized medical centers. The number of home visits within three months varied from a minimum of three times during the three months to up to three times a week. In the control group, monthly telephone calls were made to remind patients of the date for HbA1C testing three months after discharge and the date for completing the quality-of-life questionnaire three months post-discharge.
The necessary authorization to conduct the study was obtained from the Ethics Committee of Isfahan University of Medical Sciences, under the code IR.MUI. RESEARCH.REC.1398.210. The researcher then obtained informed consent from all participants in the hospital by introducing herself and explaining the study's objectives. She completed an informed consent form for each participant. Participants were free to withdraw from the study at any stage, and there were no negative consequences for them.
Statistical Methods
Statistical analyses were performed using both descriptive and inferential methods. Depending on data characteristics and distribution, appropriate parametric (e.g., paired and independent t-tests) and non-parametric (e.g., Chi-square test) tests were applied to assess differences between the intervention and control groups.
More than fifty percent (52.8%) of all patients participating in the study were women. Over eighty percent of patients in the intervention group (89.2%) and the control group (83%) had a history of surgery. In both groups, more than 60% of patients were illiterate, and over 90% had health insurance. The chi-square test did not show a significant difference (p > 0.05) in the distribution of gender, health insurance status, education level, and history of surgery between the two groups. Similarly, the t-test did not reveal any difference (p > 0.05) in the mean age and duration of hospital stay between the intervention group (age: 59.26 ± 13.90 years, hospital stay: 10.05 ± 14.82 days) and the control group (age: 64.47 ± 13.78 years, hospital stay: 10.52 ± 9.66 days). The chi-square test did not indicate any difference between the two groups in terms of the duration of diabetes (Table 1).
Frequency Distribution of the Duration of Diabetes in Patients from Two Intervention and Control Groups.

The significance level is p ≤ 0.05.
Regarding the association with HbA1C levels, the paired t-test with a p-value of 0.410 indicated no significant change in this indicator in the control group and a significant decrease (p = 0.001) in the intervention group three months after discharge (see Table 2).
Comparison of the Mean HbA1C Levels at the Time of Discharge and Three Months Later in Patients from Both the Intervention and Control Groups.

apaired t-test.
The significance level is p ≤ 0.05, and statistically significant results are bolded.
Although the independent t-test did not show a significant difference in the mean change in HbA1C from discharge to three months later in both the intervention and control groups (p = 0.094), it did indicate a significant difference in the mean percentage change in HbA1C between the two groups (p = 0.020) (see Table 3).
Comparison of Mean HbA1C Changes at Discharge and Three Months Later Between Patients in the Intervention and Control Group.

aindependent t-test.
The significance level is p ≤ 0.05, and statistically significant results are bolded.
In terms of comparing the scores of quality-of-life domains, the paired t-test indicated an improvement in quality of life in terms of satisfaction with life (p = 0.002) and concern about the future (p = 0.007) in patients of the intervention group three months after discharge. However, there was no statistical difference in these domains in the control group post-discharge.
Regarding the domain of diabetes impact on quality of life, despite a slight apparent decrease in the mean score of this domain in both groups over the three-month period, the paired t-test did not show any statistically significant difference in either group (p > 0.05).The paired t-test with a p-value > 0.05 did not show a significant difference in the mean score of the social concerns domain in the intervention group, but this difference was significant in the control group (p = 0.045) (see Table 4).
Comparison of Mean Quality of Life Domains at the Time of Discharge and Three Months Later for Patients in the Intervention and Control Groups.

apaired t-test.
The significance level is p ≤ 0.05, and statistically significant results are bolded.
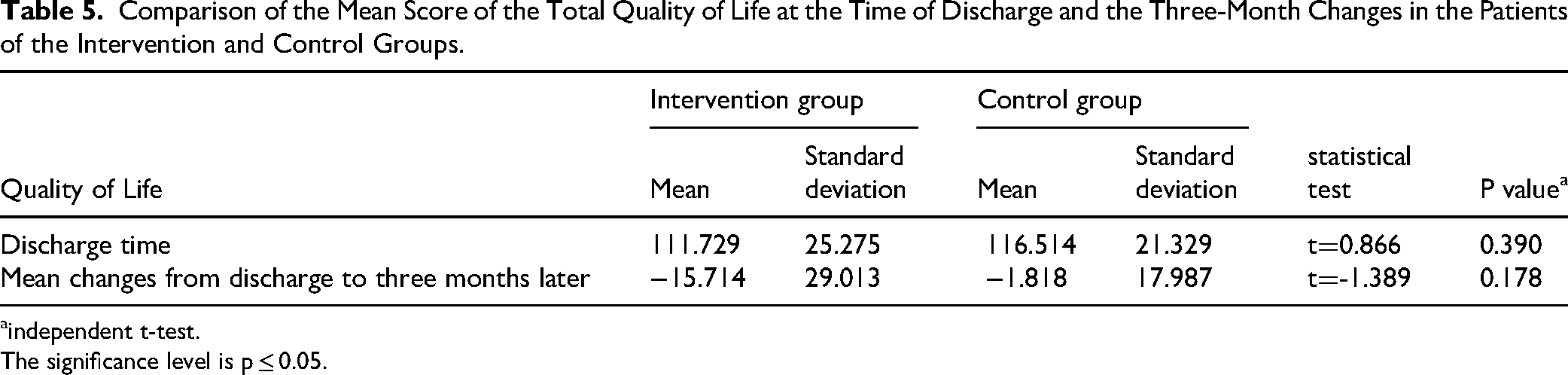
The independent t-test with a p-value > 0.05 did not show a significant difference in the mean total quality of life score between the intervention and control groups three months after discharge (see Table 5).
Comparison of the Mean Score of the Total Quality of Life at the Time of Discharge and the Three-Month Changes in the Patients of the Intervention and Control Groups.
aindependent t-test.
The significance level is p ≤ 0.05.
Discussion
Diabetes mellitus (DM) is one of the most important non-communicable diseases worldwide and a major contributor to poor quality of life. Quality of life (QOL) is an important aspect of human life that is influenced by culture, values system, goals, and individual expectations from life (Tamornpark et al., 2022, Wang et al., 2020). In the current study, patients from two groups did not differ significantly in baseline characteristics, HbA1C, and quality of life scores before the intervention, indicating proper randomization of patients into the intervention and control groups. Within-group comparisons showed no statistically significant reduction in HbA1C levels over the three-month period in patients of the control group. However, this reduction was statistically significant in patients of the intervention group. Despite the lack of a significant difference in the mean change in HbA1C levels between the two groups over the three-month period, the mean percentage change in this parameter was significant. It could be argued that the non-significance in the mean change in HbA1C levels, despite the significant percentage change, may be due to the short intervention duration and the sample size. However, in a study by Garg et al. (2017), which investigated the effect of a hospital diabetes care provider team follow-up on diabetes control in patients one year after discharge, despite a decrease in hemoglobin A1C levels in both intervention and control groups, the degree of reduction did not differ significantly between the two groups. The findings of Garg et al. suggest that continued home care for more than three months to even a year after discharge does not necessarily lead to improvements in hemoglobin A1C (Garg et al., 2017). On the other hand, although in the present study one significant reason for the lack of meaningful difference in the average changes of HbA1C could be the small sample size, in the study by Garg et al., more than twice the sample size of the current study, i.e., 150 participants, was involved (Garg et al., 2017). Furthermore, in the present study, the significant mean percentage change indicates that home care was associated with a reduction in HbA1C levels over the three-month period. Wang et al. (2020) found that continuous nursing intervention leads to a decrease in blood sugar and hemoglobin A1C levels (Wang et al., 2020). The results of Torki et al. (2020) also indicated that home visits after three months were associated with a decrease in hemoglobin A1C levels (Torki-Harchegani et al., 2020).
One reason why the findings of Garg et al. differ from those of the current study could be the intervention method. In the study by Garg et al., all patients underwent assessment, education, and care planning from admission and were then randomized into intervention and control groups. Whereas in the current study, patients were enrolled from discharge, and the control group did not receive additional care beyond routine care provided to all surgical patients, as mandated by the study protocol. Nonetheless, given that a one percent reduction in hemoglobin A1C levels reduces the risk of complications by 45% in patients with type 2 diabetes, the significant reduction in this parameter over three months in the group receiving home care in the current study may indicate the usefulness of this approach in patients with diabetes undergoing surgery to sustain postoperative care.
Regarding the impact of home care on dimensions of quality of life, in patients in the intervention group, unlike the control group, there was a statistically significant improvement in satisfaction-related aspects of quality of life (items: time spent managing and controlling diabetes, time spent on blood glucose testing, current diabetes treatment, diabetes awareness) three months after discharge. In other words, the quality of life of patients in the intervention group had improved in the satisfaction domain within the three-month period, which could indicate the impact of the home care program in addressing all these aspects. Additionally, HbA1C levels in patients in the intervention group had significantly decreased compared to the control group. Al-Maskari et al. (2011) concluded in their study that reducing hemoglobin A1C to less than 8% improves the quality of life in individuals with diabetes (Al-Maskari et al., 2011).
In the future concern domain, there was no significant difference in the level of future concern three months after discharge in the control group compared to the discharge time. In other words, the level of future concern in the control group did not decrease over the three-month period, whereas a significant reduction in future concern levels was observed in patients of the intervention group, meaning that the level of future concern in patients with diabetes undergoing home care had decreased over the three-month period. In Khalili et al.'s study (2016), which was an observational study, the future concern score did not differ significantly between the study groups (Khalili et al., 2016). It seems that the implementation of a home care program in the intervention group led to these patients feeling more secure in living with diabetes compared to the control group, resulting in a reduction in concerns about the future life with diabetes.
These findings are particularly meaningful given the high rate of illiteracy among participants. Individuals with limited literacy often face challenges in understanding medical information, adhering to treatment plans, and engaging in effective self-care. The success of the home care intervention in this study indicates that tailored, home-based support can overcome some of these barriers. This aligns with previous research highlighting that simplified education and consistent home follow-up can improve glycemic control and health outcomes in low-literacy populations (Butayeva et al., 2023). Therefore, home care should be considered a key component in post-discharge planning, especially for vulnerable groups.
Regarding the domain of magnitude of diabetes impacts on quality of life, despite a nominal decrease in the average score of this domain over the three-month period in both groups, there was no statistically significant difference between these two groups. Therefore, in the intervention group receiving home care and the control group receiving standard treatment and care, the negative effects of diabetes on quality of life were not alleviated over the three-month period. Thus, the negative effects of diabetes on quality of life were not mitigated in the intervention group receiving home care compared to those in the control group receiving usual treatment and care.
In the domain of social concerns, there was no significant improvement in the QOL scores in the intervention group. However, in the control group, there was an improvement in QOL scores in this area. Considering the items in this domain, including fear of hypoglycemia, mortality, or diabetes-related complications, the reduction of these concerns in the control group three months post-discharge is noteworthy, despite the fact that hypoglycemia was the reason for rehospitalization in 2 out of 9 readmissions in the control group, while none of the patients in the intervention group experienced hypoglycemia during the 3-month period (Faridani et al., 2021).
In the present study, despite improvements in quality of life in two domains in the intervention group and one domain in the control group, there was no significant difference in the mean changes in overall quality of life score between the two groups over the three-month period. The research conducted by Amin et al. (2022). revealed that a majority of type-2 diabetes patients, specifically 54% and 51.2% respectively, reported an average assessment of their quality of life (QoL) and health. However, their QoL scores were below the average range (Amin et al., 2022). Many factors such as age, gender, marital status, occupation, economic status, education, quality of medical care, disease stage, adherence to treatment regimens and Surgical parameters are recognized as contributors to poor quality of life in patients with diabetes (Khalili et al., 2016, Amin et al., 2022, Shah et al., 2020, Gupta et al., 2021). While in the present study, the intervention focus was solely aimed at manipulating and improving one of these factors, namely the quality of medical care.
Strengths and Limitations
The use of block randomization ensured an equal distribution of participants between the intervention and control groups. This methodological strength minimized the influence of potential confounding variables, such as comorbidities, and enhanced the internal validity and generalizability of the findings. Also, the intervention was tailored to each patient's specific educational, therapeutic, and supportive needs, based on a structured assessment at the beginning of the home care process. This patient-centered approach—delivered through home visits, phone follow-ups, coordination with healthcare providers, and continuous reassessment—enhanced the relevance and potential impact of the intervention. It reflects a real-world, holistic model of care that addresses medical, educational, and psychosocial aspects of diabetes management after surgery.
However, given that changes in quality-of-life components typically require a longer time to manifest, a follow-up period longer than three months might have allowed for a more comprehensive evaluation of the effects of home care on all dimensions of quality of life.
Implications for Practice
The results of this study can inform health policymakers about the necessity of integrating structured home care services—particularly those involving multidisciplinary teams—into the formal post-discharge healthcare system. Aligned with national health priorities such as preventing hospital-related complications and enhancing patients’ quality of life, this integration can expand access to comprehensive and preventive care in home settings. Nurses, as the backbone of home care services and within a team-based approach, play a pivotal role in ensuring the continuity, safety, and personalization of post-discharge care for patients with diabetes. They also provide essential support to patients and families in managing blood glucose levels and improving various aspects of diabetes-related quality of life. Policymakers may utilize the study's findings to revise care transition protocols, allocate resources for training and empowering community-based nurses, and establish national guidelines that ensure nurse-led follow-up visits for individuals with chronic conditions such as diabetes. These strategies not only improve the quality and efficiency of care but also align with broader goals of the Iranian health system, including strengthening primary care, optimizing workforce utilization, and enhancing patient satisfaction through personalized, community-centered services.
Conclusion
Surgical procedures impact glycemic management in individuals with diabetes around the time of surgery. These effects stem from various physiological, psychological, economic, and social stressors, including hospital environment conditions, medications, changes in treatment regimens and diets, hemodynamic changes, and length of hospital stay. These stressors affect glycemic control and subsequently the quality of life of patients. Therefore, planning to assist patients post-discharge from the hospital to achieve good glycemic control and maintain or enhance their quality of life is essential. Poorer quality of life leads to multiple health impacts on the mental and physical health of individuals with diabetes and their families. In these circumstances, patients with diabetes undergoing surgery and their families require assistance in managing specific care needs. In the present study, home care with a team-based approach is not only beneficial in improving glycemic control but also leads to increased satisfaction with diabetes and decreased future worries as two diabetes-related dimensions of quality of life among post-surgical patients with diabetes.
Given that over 60% of the participants were illiterate, the provision of individualized, home-based education and support was instrumental in facilitating understanding, improving adherence to treatment regimens, and promoting effective self-management. The observed reductions in HbA1c levels and improvements in two dimensions of quality of life demonstrate the potential of home care not only as a supportive service, but as a critical strategy to bridge health disparities among vulnerable, low-literacy populations. Therefore, integrating such services into post-discharge care plans appears to be essential. However, home care in this study did not lead to an overall improvement in all dimensions of quality of life. Considering that multiple factors beyond glycemic control influence the quality of life of patients with diabetes and observing changes in some quality-of-life indicators require evaluation over a longer period, it is suggested that in addition to focusing on cohesive team-based care services, other modifiable factors should also be considered in home care planning.
Future studies are recommended to assess the cost-effectiveness of home care interventions for individuals living with diabetes after surgery. Such evaluations can provide critical insights for healthcare policymakers regarding the economic viability and sustainability of integrating home-based services into routine post-discharge care. It is also suggested that future research employ extended follow-up durations—ranging from six months to one year—in order to better evaluate the long-term effects and sustainability of home care on glycemic control and quality of life outcomes.
Footnotes
Acknowledgments
The authors of this article would like to acknowledge the patients who participated in the research, as well as Isfahan University of Medical Sciences for providing the platform for this study.
ORCID iDs
Ethical Considerations
The necessary authorization to conduct the study was obtained from the Ethics Committee of Isfahan University of Medical Sciences, under the code IR.MUI.RESEARCH.REC.1398.210. The researcher then obtained informed consent from all participants in the hospital by introducing herself and explaining the study's objectives. She completed an informed consent form for each participant. Participants were free to withdraw from the study at any stage, and there were no negative consequences for them.
Author Contributions
Funding
This study was financed by the Vice Chancellor for Research of Isfahan University of Medical Sciences (Project number 398234).
Parvaneh Abazari, (grant number 398234).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed Consent
Both written and verbal consent were obtained from the patients.
Availability of Data and Materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Trial Registration
The present study is a randomized clinical trial registered under the code IRCT20190730044386N1.