
Abstract
Background
The code of ethics identifies the moral and ethical obligations inherent in the midwife's professional role. The practice of a code of ethics for midwives is important for the quality of care.
Objective
To assess the level of practice of the professional code of ethics, identify associated factors, and explore barriers to its practice among midwives in referral hospitals of the Amhara regional state, Ethiopia.
Method
An institutional-based cross-sectional study with concurrent triangulation of a qualitative component was conducted from December 1, 2023 to January 30, 2024. A simple random sampling technique was used to select 423 study participants. Qualitative participants were selected purposively until saturated information was obtained. The P-value <.05 was used to assert statistical significance in multivariable analysis. For the qualitative component, participants were selected purposively, and data were collected through in-depth interviews using semistructured questions. The data were analyzed using thematic analysis.
Results
This study revealed that 222 (53.5%) (95% confidence interval [CI]; 48.6%, 58.4%) midwives had good practice of the code of ethics. Training on the code of ethics (adjusted odds ratio [AOR] = 2.12, 95% CI: 1.10, 4.09), good knowledge about the code of ethics (AOR = 4.97, 95% CI: 2.89, 8.56), favorable attitude toward the code of ethics (AOR = 2.63, 95% CI: 1.58, 4.39) and job satisfaction (AOR = 1.83, 95% CI: 1.12, 2.98) were significantly associated with the practice of the code of ethics. Individual factors, institutional factors, patient-related factors, and current political instability emerged as themes representing barriers to the practice of the code of ethics.
Conclusions
According to the findings of this study, the practice of the code of ethics was lower than national expectations, as every healthcare provider had a responsibility to work in line with the professional code of ethics. Strengthening training programs, enhancing knowledge development, and fostering job satisfaction are also crucial for improving the practice of a code of ethics.
Introduction
Ethics refers to the principles and standards that guide professional behavior in determining what is right and wrong in human action (Beauchamp & Childress, 2019; Ethiopian Medical Association, 2017). It is concerned with questions about right versus wrong conduct (WHO, 2015). Within healthcare, ethical practice is commonly framed by the biomedical ethics model proposed by Beauchamp and Childress, which articulates four foundational principles: autonomy, beneficence, nonmaleficence, and justice that support morally sound clinical decision making (Beauchamp & Childress, 2019). These principles are directly relevant to midwifery practice, where practitioners must balance respecting women's choices, promoting wellbeing, preventing harm, and fairly allocating resources in maternity care.
A code of ethics serves as a public statement reflecting the beliefs and values upheld by a profession and its practitioners. In addition to biomedical ethics, midwifery practice is guided by a profession-specific ethical framework. The International Confederation of Midwives (ICM) code of ethics provides globally recognized standards that articulate midwives’ responsibilities to uphold human dignity, respect women's autonomy, ensure informed decision making, advocate for equitable care, and maintain professional integrity. It supports the ethical mandate to promote the health and wellbeing of women and newborns within their families and communities (ICM, 2014). The code of ethics helps midwives regulate their own practice, reinforces professional identity, and serves as a framework to assess ethical behavior (Simbar et al., 2023). Grounding midwifery practice in these ethical frameworks is essential, as midwives frequently encounter complex clinical situations that require moral judgment and ethical reasoning.
Midwives should be mindful not only of their practice but also of the moral and ethical challenges that may arise from it. They need to know how to effectively navigate the ethical dilemmas that can occur while providing care (Organisation, 2014). In all circumstances, midwives are expected to uphold human dignity, provide respectful care, and support women and their families in making informed decisions (Oelhafen et al., 2017).
Review of the Literature
Currently, professional codes of ethics have gained priority and focus due to increased public knowledge and development in science and technology (Deo et al., 2017). As a result, midwives were expected to adhere to the professional code of ethics to ensure safe, respectful, dignified maternity care, and to protect themselves from medicolegal issues. In Ethiopia, the code of ethics for health professionals has been established and approved under Regulation No. 299/2013, following the guidelines of the Food, Medicine, and Healthcare Administration and Control Proclamation No. 661/2009. This initiative aims to uphold ethical standards among health professionals for the protection of patients and clients (Federal Democratice Republic of Ethiopia, 2014). The Ethiopian Midwives Association (EMwA) also developed a code of ethics guidelines to update the emerging professional code of practice, enhance midwifery practice, and protect both the community and the profession from medicolegal issues (Association, 2021).
Globally, adherence to the professional code of ethics among healthcare providers varies from country to country. Evidence showed in Ghana (91%) (Asare et al., 2022), Iran (80%) (Abdishahshahan, 2018), Nepal (76.4%) (Timilsina, 2017), Saud Arabia 26% (Al-Shehri et al., 2020), and other evidence Nepal 50% (Shrestha & Jose, 2014) healthcare providers were adhere to their code of ethics. Even if every healthcare provider in Ethiopia had a responsibility to work in line with their professional code of ethics (Federal Democratice Republic of Ethiopia, 2014), most of them do not practice well. Previous findings in Ethiopia reported a low level of ethical practice among health workers in various regions: 30% in Addis Ababa, 24% in Ambo, 32.7% in a national study, and 46.7% in Gondar (Mulu et al., 2018; Tafesse et al., 2022; Tiruneh & Ayele, 2018; Yeshineh et al., 2022). This poor practice compromised the quality of care and contributed to the increase in complaints against the health professional. In Ethiopia, between 2011 and 2017, a total of 125 complaints were submitted to the Federal Health Professionals’ Ethics Committee of Ethiopia against 146 health professionals (Wamisho et al., 2019).
Understanding biomedical ethics concepts and acting consistently with professional ethics is a fundamental component of midwifery care and a required core competency (Megregian, 2016; Oelhafen et al., 2017). If midwives do not practice according to a code of ethics, it not only weakens the patient-healthcare provider relationship but also compromises the quality of care and leads to potentially high incidences of violence (Damayanti et al., 2020). Violations of the code of ethics in clinical practice can lead to serious consequences, including unnecessary healthcare costs, patient harm, disability, or even death. Furthermore, ethical breaches undermine public trust in healthcare providers and institutions, while also adversely affecting the psychological and physical wellbeing of healthcare workers (Giacalone et al., 2016; Wamisho et al., 2015). In addition, healthcare providers may also face blame, litigation, and damage to their professional identity and dignity as a result of such violation (Ethiopian Medical Association, 2017; Peyman, 2017). Despite these consequences, evidence regarding the practice of the code of ethics among midwives in Ethiopia remains limited, according to an extensive literature search. Therefore, this study employed a mixed-methods approach to assess the level of adherence to the professional code of ethics, identify associated factors, and explore barriers to its practice among midwifery healthcare providers. Understanding current practices is crucial for guiding training, supervision, and policy interventions aimed at promoting ethical midwifery practice.
Methods
Study Design and Setting
An institution-based cross-sectional study with concurrent triangulation of a qualitative component was conducted from December 1, 2023 to January 30, 2024, to assess the level of practice of the professional code of ethics, identify associated factors, and explore barriers to its practice among midwives in referral hospitals of the Amhara regional state, Ethiopia. The Amhara Regional State is located in the northwestern and north-central parts of Ethiopia, and comprises 108 hospitals, including eight referral hospitals, and 885 health centers. Of the total 4,935 midwives in the region, 548 were employed in referral hospitals (Ethiopia Ministery of Health, 2021). The concurrent triangulation design enabled quantitative assessment of prevalence and determinants, while simultaneously exploring contextual barriers qualitatively.
Study Population
All midwives working in Amhara Regional State referral hospitals and available during the data collection period were included in the study. For the qualitative component, key informants or midwives were purposively selected based on their experience and willingness to provide in-depth insights until data saturation was achieved. However, midwives on annual or maternity leave, as well as those attending long-term training, were excluded from the study. Participants were approached in their workplace during duty hours, after requesting the collaboration of each hospital's midwife ward heads. Midwives were provided with information sheets, and written informed consent was obtained before participation.
Sample Size and Sampling Procedures
The sample size was calculated using a single population proportion formula based on the following assumptions: a 95% confidence interval, a 5% margin of error, and an assumed proportion of 50% due to the lack of similar studies in Ethiopia. An additional 10% was added to account for the potential nonresponse.
Variables and Measurements of the Study
The practice of the code of ethics among midwives was the dependent variable and was measured using 13 practice-related item questions rated on a five-point Likert scale response ranging from 1 (never) to 5 (always). A total possible score ranges from 13 to 65, and participants who scored 49 or higher out of 65 (≥ 75%) on the practice-based items were classified as having good practice (Tiruneh & Ayele, 2018; Yeshineh et al., 2022).
Knowledge of the code of ethics: Measured using nine yes-or-no questions related to the midwifery code of ethics. Participants who correctly answered 75% or more (at least 7 out of 9 questions) were considered to have good knowledge of the code of ethics (Ayele & Michael, 2019; Yeshineh et al., 2022).
Attitude to the code of ethics: Measured by 10-item questions with a five-point Likert scale response, and participants who answered ≥ 75% (38 or more out of 50) on attitude questions were considered to have favorable attitudes (Ayele & Michael, 2019; Yeshineh et al., 2022).
For Knowledge, Attitude, and Practice (KAP) assessment, the widely adopted Bloom's cutoff points categorize scores as follows: 80% to 100% for high knowledge, positive attitude, and good practice; 60% to 79% for moderate knowledge, neutral attitude, and fair practice; and less than 60% for low knowledge, negative attitude, and poor practice (Olum & Bongomin, 2020; Tafesse et al., 2022). In this study, however, the scores for KAP were dichotomized using a ≥ 75% threshold representing a modification of the original Bloom cutoff points (Basheer, 2020; Okello et al., 2020; Wahidiyat et al., 2021). This approach is consistent with prior Ethiopian studies on professional ethics and KAP among health workers (Ayele & Michael, 2019; Tiruneh & Ayele, 2018; Yeshineh et al., 2022), where the 75% threshold has been commonly applied to define “good” or “favorable” responses.
The selection of the 75% cutoff is methodologically justified by its alignment with previous Ethiopian KAP studies, facilitating direct comparability of findings across similar health professional populations. In addition, the use of this threshold reflects a broadly accepted practice in KAP research, where modified Bloom's criteria are commonly applied to identify participants with adequate understanding or favorable attitudes. This approach ensures that the measurement captures meaningful differentiation between participants with sufficient versus insufficient KAP levels while maintaining consistency with locally validated instruments. By explicitly referencing prior studies and explaining the rationale for adaptation, the use of the ≥75% cutoff is justified for the present study context.
Sociodemographic variables (age, sex, marital status, level of education, ethnicity, income, and work experience), individual factors (attitude, interest toward profession, autonomy, and job satisfaction), and institutional factors (ethical committee, training, working ward, and supportive supervision) were considered as explanatory variables.
Job satisfaction: Assessed by nine-item questions with a five-point Likert scale response; participants who answered ≥ 50% on satisfaction questions were satisfied (Temesgen et al., 2018; Yeshineh et al., 2022).
Data Collection Tool and Procedure
The quantitative data collection tool was a structured self-administered questionnaire adapted from the peer-reviewed studies (Ayele & Michael, 2019; Haile, 2022; Tiruneh & Ayele, 2018; Yeshineh et al., 2022). The tool was not entirely self-designed nor globally standardized, but rather a contextually adapted version of a scientifically established measure relevant to the code of ethics in midwifery care. To ensure the validity of the adapted tool, content validity was assessed through expert review, including a senior midwifery educator, a senior midwife working in a clinical setting, and a senior researcher to determine whether the tool addressed all necessary dimensions of the topic and to evaluate its clarity, simplicity, and relevance. Face validity was also confirmed through a pilot study conducted on 5% of the sample size (21) to assess clarity, relevance, cultural appropriateness, and the overall acceptability. Feedback from this pilot test was used to refine ambiguous or unclear items. The reliability of the practice tool was assessed using Cronbach's alpha, which was 0.785, indicating acceptable internal consistency. The tool was initially developed in English and translated into the local Amharic language, and then back-translated into English to ensure conceptual equivalence. A semistructured interview guide was developed based on the literature review for a qualitative data collection tool (Supplemental File 1).
Two diploma holders and six bachelor's degree midwives were recruited as data collectors, while eight master's degree midwives were selected as supervisors. After obtaining consent, each study participant received an Amharic version of a self-administered questionnaire for quantitative data collection. However, qualitative data were collected by the principal investigator through audiorecorded, semistructured interviews. The in-depth individual interviews took place in a quiet room suitable for audio recording and lasted between 25 and 30 min. In addition to audio recording, the researcher took detailed field notes to document nonverbal cues and contextual observations. Data collection and probing of ideas continued until data saturation was reached.
Data Quality Assurances
One day of training was provided to the data collectors and supervisors. The data collection tool was pretested on 5% of the sample size (n = 21) at Nigst Eleni Mohamed Memorial Comprehensive Specialized Hospital prior to the actual data collection period, to ensure the consistency and completeness of the questionnaires. The interviews were conducted privately, with assurances of confidentiality to minimize social desirability bias. The qualitative data were transcribed, and the principal investigator checked the consistency of the information. The trustworthiness of data can be established through credibility, transferability, dependability, and confirmability (Guba, 1985). Accordingly, the credibility of the study findings was enhanced by spending sufficient time on data collection and analysis. Interview data were triangulated with field notes, and a member check was conducted to validate the findings. Additionally, researcher triangulation was conducted during the data coding and analysis process to ensure credibility and transferability. To enhance transferability, thick descriptions of the study setting and participant demographics were also provided. Dependability was achieved by the code-recode method of analysis, where data were coded over an extended period to ensure consistency in coding. A peer review of the coding framework and emerging themes was conducted to verify the dependability of the analysis process. Confirmability was ensured by documenting direct quotations of participants.
Data Processing and Analysis
The collected data were entered into the EpiData version 4.6 computer program and then exported to SPSS version 25 for cleaning, coding, computing, and analyzing. After being exported to SPSS data were checked for completeness and consistency, and the dataset was prepared for statistical analysis. Missing items in the dataset were minimal, and missing data were handled using listwise deletion. All predictor variables with a P-value <.2 in the bivariable logistic regression analysis were considered as candidates for inclusion in the multivariable logistic regression model. The adequacy of the final multiple binary logistic regression model for practice was assessed using the Hosmer and Lemeshow goodness-of-fit test, and the results indicated a good fit to the data (P-value = .158).
Finally, after adjusting for confounding, a P-value <.05 was used to declare statistical significance. The PI listened to audio recordings, transcribed the interviews verbatim, and translated them into English. After data familiarization, the translated data were coded by using ATLAS.ti version 23 qualitative data management software, and then codes with similar meanings were arranged into subcategories and main categories. The main themes were identified using a thematic analysis approach. Qualitative data were analyzed using Braun and Clark's six-phase thematic analysis: (1) familiarizing yourself with the data, (2) generating initial codes, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing the report (Clarke & Braun, 2017; Kiger & Varpio, 2020). A total of 19 codes were generated from the in-depth interview. These codes were grouped into nine subthemes and subsequently organized into four major themes following thematic analysis.
Results
Sociodemographic Characteristics
This study was completed with 415 participants, yielding a response rate of 97.9%. Among the study participants, 58.6% were males. The age of the participants ranged from 22 to 41 years, with a mean age of 30.23 years (SD ± 3.44). The majority (91.1%) of the study participants were Amhara in ethnicity, and 362 (87.2%) were Orthodox religious followers. Nearly three-fourths (73%) of the respondents held a bachelor's degree (Table 1).
Sociodemographic Characteristics of the Study Participants in Amhara Regional State Referral Hospitals, Ethiopia, 2024 (n = 415).

*key: Argobba, Tigray, Gurage, Kimant; NGO = None Governmental Organization.
Individual and Professional-Related Factors
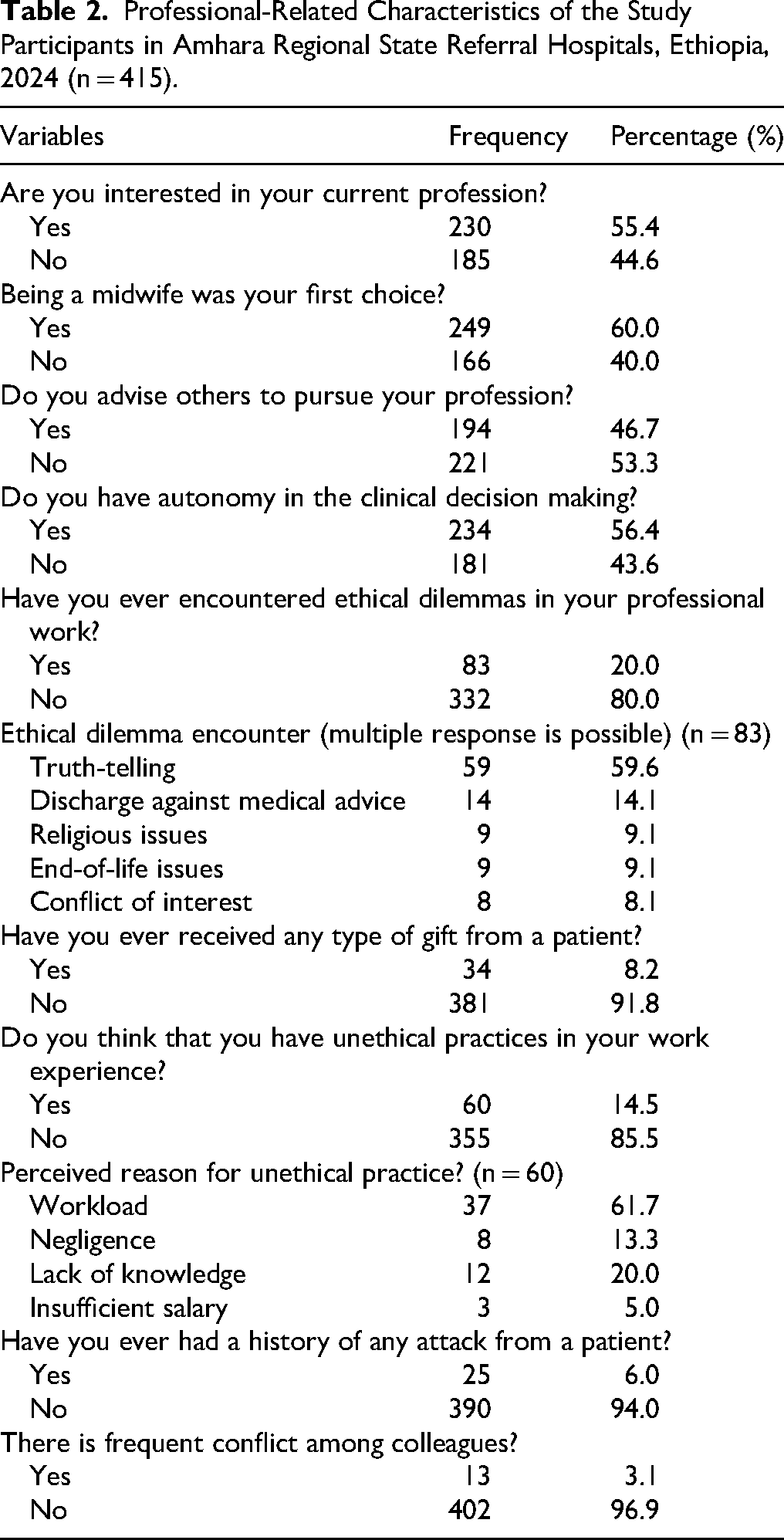
Three in seven participants (43.6%) reported having no autonomy in clinical decision making. One-fifth (20%) of the study participants reported encountering ethical dilemmas in their professional work, with truth-telling being the most frequently encountered dilemma (Table 2).
Professional-Related Characteristics of the Study Participants in Amhara Regional State Referral Hospitals, Ethiopia, 2024 (n = 415).
Knowledge and Attitudes of Study Participants Toward the Code of Ethics
Quantitatively, 267 (64.3%) (95% confidence interval [CI]: 59.5, 68.9) of the study participants demonstrated good knowledge of the professional code of ethics. Qualitative interviews confirmed this general awareness: most midwives were aware of the code of ethics, having received some basic training during college or university; however, significant gaps persisted, particularly in understanding their professional scope. One 29-year-old midwife emphasized “poor knowledge of midwives about code of ethics, even about their professional scope, was one contributing factors for unethical practice.”
Less than half, 195 (47%) of the participants had favorable attitudes toward the code of ethics (95% CI; 42.1%, 51.9%). Qualitative data reinforced this, revealing instances of disrespectful communication and weak professional relationships. A 29-year-old midwife commented: “Midwives may not develop respectful partnerships with clients or colleagues, and some fail to consult when women's needs exceed their competencies.”
Institutional Factors
Three-fifths (61.2%) of participants perceived that there was supportive supervision within the working environment. More than one-fifth (23.9%) of midwives were trained in the professional code of ethics. However, the majority of participants (83.6%) reported that an ethical committee existed in their institution.
Practice of the Study Participants Toward the Code of Ethics
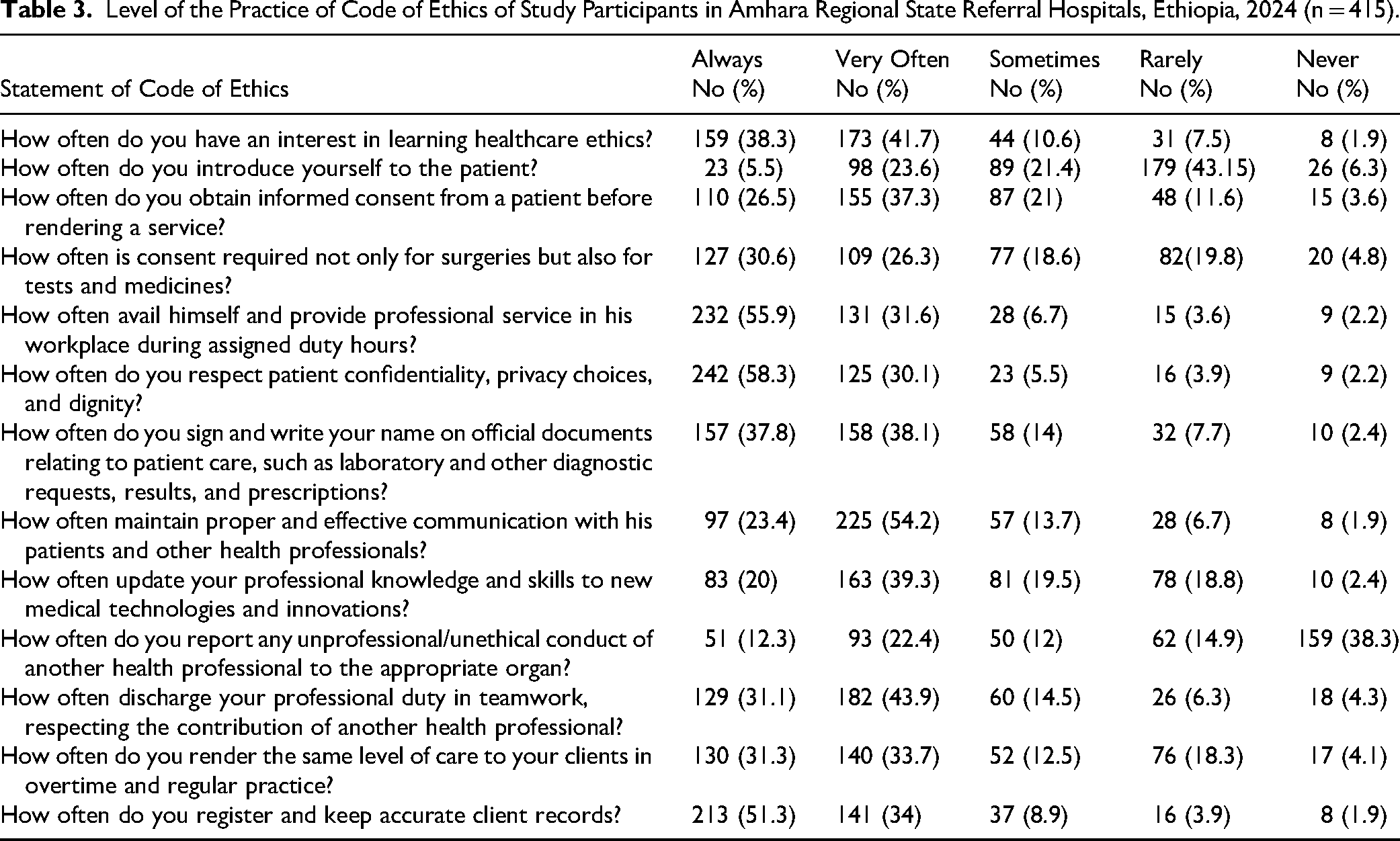
Of the total study participants, only just more than half, 222 (53.5%) of midwives had good practice of the code of ethics (95% CI: 48.6%, 58.4%) (Table 3). The qualitative respondents indicated that though midwives were aware of the professional code of ethics, gaps remained in its practice. Most of them reported a gap in obtaining informed consent consistently across the procedure, confidentiality, privacy, and communication.
One 32-year-old respondent said, “……. Informed consent was procedure-dependent: In procedures like cesarean section, all midwives might obtain the patient's informed consent and explain the benefits and side effects of the procedure. However, for other procedures like instrumental delivery and administration of medication, midwives might not inform the client about the benefits, side effects, or the right of refusal of the service.”
One 36-year-old KI said, “…. Laboring mother privacy is not consistently maintained by every midwife due to the absence of private rooms for each woman and even the absence of proper screening in the labor ward, and pelvic examination was often conducted in the labor ward in the presence of eight or more women in a single room without the use of privacy screens.”
Level of the Practice of Code of Ethics of Study Participants in Amhara Regional State Referral Hospitals, Ethiopia, 2024 (n = 415).
Factors Associated With the Practice of the Code of Ethics
Among candidates with a P-value <.2 for inclusion in the multivariable analysis, training on the professional code of ethics, knowledge of the code of ethics, attitude, and job satisfaction were significantly associated with the practice of the code of ethics in multivariable logistic regression analyses (P < .05).
This study showed that midwives who received training on the professional code of ethics were 2.12 times more likely to have good practice of the code of ethics compared to participants who had never received training (adjusted odds ratio [AOR] = 2.12, 95% CI: 1.10, 4.09). Qualitative results supported this finding. One 36-year-old KI said, “……Absence of training about the code of ethics was one barrier for unethical practices.” This highlights how institutional investment in continuous professional development shapes the quality of care and ethical conduct.
In addition, participants with good knowledge of the code of ethics were nearly five times more likely to have good practice of the code of ethics compared to their counterparts (AOR = 4.97, 95% CI: 2.89, 8.56). The qualitative result also identified that knowledge was one barrier to the practice of the code of ethics. One 29-year-old KI said, “……. Poor knowledge of midwives about the code of ethics, even about his/her professional scope, was one contributing factor for unethical practice.” This alignment suggests that knowledge is not merely informational but foundational to ethical decision-making and professional accountability.
Similarly, study participants who had a good attitude toward the code of ethics were 2.63 times more likely to have good practice of the code of ethics compared to participants who had a poor attitude (AOR = 2.63, 95% CI: 1.58, 4.39).
Furthermore, participants who were satisfied with their job were 1.83 times more likely to practice a code of ethics than those who were unsatisfied (AOR = 1.83, 95% CI: 1.12, 2.98) (Table 4). This finding was in line with the qualitative result. One 30-year-old KI said, “…Dissatisfaction with the profession, largely due to inadequate income that fails to cover monthly expenses, was identified as a contributing factor to the poor adherence to the code of ethics.” These experiences suggest that ethical practice cannot be separated from the socioeconomic realities of midwifery. This highlights how systemic and financial challenges affect midwives’ ability to uphold ethical standards, potentially compromising both the quality of care and professional integrity.
Bivariable and Multivariable Logistic Regression Analysis of Factors Associated With the Practice of the Code of Ethics of Midwives in Amhara Regional State Referral Hospitals, Ethiopia, 2024 (n = 415).

Note: *Significant at P-value <.05, **statistically significant at P-value <.001. AOR=adjusted odd ratio; CI=confidence interval; COR=crude odd ratio.
The qualitative study identified four main themes as below.
Theme 1: Individual-Related Factors
Under this theme, participants identified poor communication, job dissatisfaction, negligence, limited knowledge, and lack of autonomy among midwives.
Theme 2: Institutional-Related Factors
Under this theme, the shortage of drugs and equipment, the absence of structured support systems, the high patient-to-midwife ratio, and low monthly salary were stated.
Theme 3: Instability and Conflict
An emerging subtheme of workplace instability stemming from political or security challenges was identified as a significant barrier to midwifery ethical practice. Participants reported that such instability undermines the ability of midwives to deliver quality care and adhere to professional ethical standards. One 30-year-old KI said, “…Instability negatively affects healthcare providers’ ability to utilize their skills and deliver quality care. It contributed to the midwives’ absence in the workplace and negatively influenced the practice of the code of ethics.” This reflects how external forces, such as political instability, not only disrupt the personal sense of safety and peace for midwives but also deeply impact their ability to maintain ethical standards and deliver quality care.
Theme 4: Patient-Related Factors
In this theme patient knowledge gap subtheme has emerged. Patients who were not aware of their rights became more vulnerable to unethical or disrespectful practices by healthcare providers. The 30-year-old man said, “…Usually, the client's decision is not respected, especially if the client doesn’t know her rights and duties.” This implies that inadequate patient education contributes to power imbalances in clinical interactions and increases the risk of unethical behavior from providers.
Integration of Quantitative and Qualitative Findings
A joint display was developed to show how quantitative and qualitative findings converged, complemented, or expanded one another (Table 5).
Joint Display Table to Show the Integration of Quantitative and Qualitative Findings.

Note: AOR=adjusted odd ratio.
Discussion
The findings of this study showed that slightly more than half (53.5%) (95% CI: 48.6%, 58.4%) of the study participants had good practice of the code of ethics. The qualitative findings corroborated these results and highlighted recurring gaps such as ineffective communication, inconsistent informed consent procedures, and limited maintenance of patient privacy. Those shortcomings directly contradict the ICM code of ethics, which identifies respect for autonomy, confidentiality, human dignity, and collaborative partnership as foundational ethical obligations of midwives (ICM, 2014).
When interpreted through Beauchamp and Childress’ ethical principles, the observed deficiencies reflect threats to autonomy due to failure to provide adequate information, violation of nonmaleficence as a result of compromised care under system-level constrains, challenges to beneficence through inability to consistently promote wellbeing, and breach of justice when high workload limits equitable access to care (Beauchamp & Childress, 2019). In addition, the ethics of care theory emphasizes the relational and contextual nature of midwifery ethics, illustrating how poor communication, weak midwife–patient partnerships, and disrespectful interactions with colleagues undermine trust and ethical sensitivity (Buchanan et al., 2025; Thompson & Thompson, 2002). The findings of this study align with an Ethiopian qualitative study of midwives lived experience, which documented ethical dilemmas arising from cultural and religious constraints on women's autonomy, confidentiality conflicts, resource scarcity, and institutional barriers affecting ethical decision making (Getu et al., 2025). This concordance underscores that ethical practice cannot be understood solely as a matter of individual knowledge or attitude, but must also be examined in light of institutional, cultural, and systemic realities.
The current finding is consistent with studies done in Gurage (53%) (Haile, 2022), in Addis Ababa 48.8% (Tolosa et al., 2024), and Nepal (50%) (Shrestha & Jose, 2014). However, the current study finding was higher than studies conducted in a country-based study in Ethiopia (32.7%) (Tafesse et al., 2022), Addis Ababa (30%) (Tiruneh & Ayele, 2018), Ambo (24%) (Mulu et al., 2018), Bale (45.6%) (Sciences et al., 2019), and Saudi Arabia (26%) (Al-Shehri et al., 2020). This might be due to the difference in the level of knowledge of study participants, the study period, and the study population. The previous country-based finding in Ethiopia showed that only one-third had an adequate understanding of professional ethics; however, the current study finding showed that nearly two-thirds of participants had sufficient knowledge. Good knowledge of the code of ethics was significantly associated with better adherence to ethical practice, as evidenced by different findings (Nayak et al., 2016; Tiruneh & Ayele, 2018; Yeshineh et al., 2022). Likewise, the discrepancy from the findings in Ambo might be due to a variation in the study period, which was conducted in 2016, and subsequent national training initiatives. Since 2016, the Ethiopian Ministry of Health has implemented various interventions, including training on Compassionate and Respectful Care (CRC), development of the midwife code of ethics by EMwA, and Ethics and Medicolegal basic training for healthcare professionals, also developed by the Ethiopian Medical Association (Association, 2021; Ethiopian Medical Association, 2017; Training & Manual, 2017). These interventions reinforce beneficence and respect for persons by equipping midwives with structured ethical guidance.
However, this finding is lower than the study findings in Ghana (91%) (Asare et al., 2022), Iran (80%) (Abdishahshahan, 2018), and Nepal (76.4%) (Timilsina, 2017). This inconsistency might be due to the differences in the study participants’ knowledge of the code of ethics, measurement, and educational systems. The previous finding in Ghana showed that more than three-fourths had adequate knowledge, whereas this study showed that nearly two-thirds of participants had good knowledge. Additionally, the findings of this study are lower than those reported in Iran, which might be due to the difference in educational systems, since Iran's midwifery curriculum includes the International Code of Ethics for midwives (Abdolalipour et al., 2023). Curricula that embed ethical principles more robustly are likely to reinforce autonomy, justice, and beneficence as routine components of clinical reasoning.
Receipt of training on the professional code of ethics was significantly associated with better-reported practice of the code of ethics. Study participants, who received training in the professional code of ethics, were 2.12 times more likely to apply the code of ethics into practice. This agreed with a study conducted in Gurage, Ethiopia (Haile, 2022), Nigeria (Funmilola & Aina, 2020; Yohanna & Afonne, 2016), Sri Lanka (Ranasinghe et al., 2020), and Iran (Shahabnia1 et al., 2020). This result was supported by qualitative findings of this study, in which training toward the code of ethics was one barrier to the practice of the code of ethics. This finding was in line with a study done in Iran (Mobasher, 2017). This association may reflect that midwives who receive training are more likely to have higher knowledge, attitude, and skill regarding CRC (Training & Manual, 2017). From an ethical-theory perspective, training strengthens midwives’ ability to respect autonomy, prevent harm (nonmaleficence), and promote the wellbeing of women and newborns (beneficence).
Study participants who had good knowledge of the code of ethics were 4.97 times more likely to practice the code of ethics when compared to their counterparts. This agreed with studies done in Gondar (Yeshineh et al., 2022), Addis Ababa (Tiruneh & Ayele, 2018; Tolosa et al., 2024), Bale (Sciences et al., 2019), Iran (Nasiriani1 et al., 2018), and India (Nayak et al., 2016). Similarly, according to the qualitative findings, poor knowledge of the code of ethics was one of the determining factors for poor practice of the code of ethics. This aligns with a qualitative finding from Iran (Dehghani et al. 2015), which highlights that ethical knowledge is a critical aspect of nursing care. Professional ethics theory supports this finding by emphasizing that competence and knowledge are essential for ethical decision making (Johnstone, 2015). In addition, moral distress theory explained that a lack of knowledge may generate ethical uncertainty and compromise the ability to act in the patient's best interest (Morley et al., 2019). Midwives with better knowledge of the code of ethics are more likely to distinguish between ethical and unethical practices, correlated with higher adherence.
Furthermore, this study revealed that a favorable attitude toward the code of ethics was significantly associated with the practice of the code of ethics. Study participants who had favorable attitudes toward the professional code of ethics were 2.63 times more likely to take the code of ethics into practice. This is in line with a study done in Gondar (Yeshineh et al., 2022), Addis Ababa (Tiruneh & Ayele, 2018; Tolosa et al., 2024), Bale (Sciences et al., 2019), and country-based findings in Ethiopia (Tafesse et al., 2022). The possible reason might be that when midwives have favorable attitudes, they always see the best and do the right, even in difficult situations. Ethics of care and principles converge here: attitude shapes moral sensitivity, decision making, and internalization of ethical values such as respect, dignity, and advocacy (Banks, 2012; Beauchamp & Childress, 2019). Therefore, favorable attitudes strengthen the internalization of professional values such as respect, dignity, and advocacy highlighted in the ICM code, and supports the principle of beneficence and respect for persons.
Job satisfaction was another identified significant variable associated with the practice of a code of ethics. Study participants who were satisfied with their jobs were 1.83 times more likely to practice the code of ethics when compared to those dissatisfied. This finding aligns with the study conducted in Gondar (Yeshineh et al., 2022), Addis Ababa (Tolosa et al., 2024), and national-level findings in Ethiopia (Tafesse et al., 2022). Qualitative data from this study support this result. One 30-year-old KI stated, “dissatisfaction with the profession, mainly due to inadequate income, was linked to poor adherence to the code of ethics.” This reflects that midwives with higher job satisfaction are more likely to report motivation, which may be associated with greater adherence to ethical standards (Pinar et al., 2017). Moral distress theory explains how dissatisfaction, especially due to inadequate pay or support, reduces motivation, and adherence to ethical standards (Morley et al., 2019). From an ethical standpoint, dissatisfaction may be associated with compromising beneficence by reducing the caregiver's ability to act in the patient's best interests and may threaten justice when unequal workloads and demotivation affect care consistency.
The qualitative data revealed that individual-related, institutional-related, political instability, and patient-related factors were major barriers affecting the practice of the midwifery code of ethics. Midwives frequently cited poor communication, negligence, and limited autonomy as barriers to ethical practice. Participants reported that poor communication, including weak midwife-to-patient relationships and disrespectful interactions with colleagues, was linked to misunderstanding and compromised ethical care. As one 29-year-old KI stated, “……Midwives might not develop a partnership with the individual clients, and some may not work respectfully with other health professionals.” Because communication is essential for informed consent, trust-building, and respectful maternity care, these findings illustrate clear violations of autonomy and maleficence. Similar findings from Ethiopia (Tiruneh & Ayele, 2018), Iran (Dehghani et al., 2015), and Belgium (Vermeulen et al., 2020) highlight that poor communication results in unethical and disrespectful maternity care. As supported in literature, effective communication is fundamental for building trust, increasing patient satisfaction, ensuring informed consent, and enhancing respectful care (Ayudiah et al., 2024; Tiwary et al., 2019).
The study revealed that a shortage of drugs and equipment, high patient-to-midwife ratios, and a lack of support systems severely constrained the practice of the code of ethics. Such circumstances may be linked with lower adherence to justice and beneficence, as resource constraints can limit equitable access and the ability to provide optimal care. This finding is consistent with the previous studies in Gondar (Yeshineh et al., 2022), Addis Ababa (Tiruneh & Ayele, 2018), and Iran (Dehghani et al., 2015). Comparable evidence in South Africa (Mathibe-Neke & Mashego, 2022), Ghana (Boakye, 2022), and Kenya (Tallam et al., 2025) also indicated that deficiencies in materials and human resources were contributing to unethical behavior and professional malpractice. This may be due to these under-resourced environments, which were correlated with lower adherence to ethical practice, possibly reflecting challenges in providing optimal care.
In addition, clients’ limited awareness of their health rights was found to negatively affect ethical practice and the overall quality of care. Study participants reported that women often lacked understanding about informed consent, which led to the procedure being conducted without adequate communication or patient agreement. As one 30-year-old man stated, “…Usually, the client's decision is not respected, especially if the client doesn’t know her rights and duties.” This finding aligns with existing evidence showing that low levels of education and limited health literacy reduce patients’ abilities to make informed decisions, and it is associated with increased ethical violence (Hansson & Fröding, 2021). However, other studies have also shown that as women become more aware of their healthcare rights, the incidence of litigation tends to rise (Mathibe-Neke & Mashego, 2022). Furthermore, the findings of this study suggest that empowering patients through education may strengthen ethical accountability, as informed clients are more likely to question unethical practices and demand respectful care.
Political instability and conflict also emerged as a significant barrier to ethical practice among midwives. Midwives described feeling unsafe and unsupported, which was associated with higher reports of emotional exhaustion and absenteeism. Other evidence showed healthcare providers have to make a difficult choice between saving someone's life and their safety because laws regarding the immunity of healthcare providers in war are not always respected (Muhammad et al., 2024). This underscores that ethical practice might be breached due to fear for their own life. Therefore, ensuring the protection and psychological support of midwives in conflict zones is essential to uphold ethical care.
A growing body of literature emphasizes that midwifery ethics is distinct and relational, grounded in midwifery values, advocacy, and practical embodiment rather than abstract compliance (Buchanan et al., 2025; Buchanan et al., 2022). Ethical sensitivity arises from relationships, context-awareness, attention to power imbalance, and caring practices. These frameworks help explain why, in resource-limited and high-stress environments similar to the study setting, adherence to a code of ethics may falter despite sufficient knowledge. Ethical practice is deeply bound with emotional labor, professional identity, and moral resilience (Buchanan et al., 2022).
Strengths and Limitations of the Study
This study is strengthened by its mixed-methods design with concurrent triangulation, which enhanced the credibility of the findings by integrating quantitative results with in-depth qualitative insights. In addition, the inclusion of multiple referral hospitals improves the robustness and transferability of the findings to similar healthcare settings in Ethiopia.
However, this study also had some limitations. First, due to the cross-sectional nature of the study design, a cause-and-effect relationship could not be established. Second, reliance on self-reported data might have been influenced by social desirability bias, potentially affecting the accuracy of the response. Third, the study did not include women's perspectives or experiences, which could have provided a more comprehensive understanding of midwives’ ethical practice. Additionally, the use of purposive sampling methods for the qualitative part may introduce selection bias, as participants with strong opinions on ethical practice may have been more likely to participate. Moreover, the relatively small sample size in the qualitative part and the study's limitation to referral hospitals in the Amhara region limit generalizability and transferability of the findings to midwives in other settings or levels of care. However, the results may still reflect ethical practice challenges relevant to similar healthcare settings across Ethiopia.
Clinical Implications
The study emphasizes the need to strengthen the ethical midwifery practice in Ethiopia through multifaceted interventions. Enhancing midwives’ knowledge and attitudes through regular ethics training can significantly improve adherence to the professional code of ethics. Code of ethics and professional responsibility should be better integrated into the midwifery curriculum, drawing on international frameworks such as the International Code of Ethics for midwives. Preservice education should move beyond theoretical exposure to practical, case-based, and simulation-based ethics training. Hospital administrators should prioritize supporting the ethics committee, provide supportive supervision, address resource shortages, and ensure safe and enabling work environments. Addressing job satisfaction through fair fees and recognition could further strengthen motivation for ethical practices. Empower women to participate actively in their care by promoting effective communication and patient rights education to reduce ethical violations. Furthermore, ensuring the safety and psychological wellbeing of midwives, particularly in conflict-affected areas, is essential. Integrating the code of ethics-focused content into midwifery curricula will help prepare future professionals for real-world ethical challenges.
Conclusion
According to the findings of this study, the practice of the code of ethics was lower than national expectations, as the Ethiopian Food, Medicine, and Health Care Administration and Control Council of Ministers Regulation requires all healthcare providers to practice in accordance with their professional code of ethics.
Training on the professional code of ethics, knowledge of the code of ethics, attitude toward the code of ethics, and job satisfaction were significantly associated with the practice of the code of ethics. The qualitative findings showed that four main themes: individual-related factors that deal with, poor communication, dissatisfaction with current job, negligence, poor knowledge, and autonomy of midwives; institutional-related factors that were reflected in the shortage of drugs and equipment, high patient to midwife ratio and, lack of support systems; current political instability and patient-related factors were the barrier for practice the code of ethics.
Therefore, to enhance the practice of the midwives’ code of ethics, it might be better if the responsible bodies undertake the following steps. First, expand the code of ethics training by integrating a standardized module on professional ethics into preservice and in-service midwifery education. Secondly, establish routine supportive supervision and mentorship programs to reinforce ethical practice and to provide feedback. Additionally, promote job satisfaction by recognizing and rewarding ethical practice through institutional incentives, improving working conditions, including security in conflict-prone zones, and providing psychological support for frontline midwives. Furthermore, address resource shortage, including essential drugs, equipment, and staffing levels, to reduce moral distress and workload-induced unethical practices. Moreover, future studies should incorporate observational data and include women's perspectives to validate self-reports and provide a more comprehensive understanding of ethical practice.
Supplemental Material
sj-docx-1-son-10.1177_23779608261424662 - Supplemental material for Practice of the Professional Code of Ethics and Associated Factors Among Midwives in Amhara Regional State Referral Hospitals, Ethiopia, 2024: A Mixed-Methods Study
Supplemental material, sj-docx-1-son-10.1177_23779608261424662 for Practice of the Professional Code of Ethics and Associated Factors Among Midwives in Amhara Regional State Referral Hospitals, Ethiopia, 2024: A Mixed-Methods Study by Tadesse Getu, Getie Lake, Samrawit Abebaw, Aregash Sitot and Animut Tagele in SAGE Open Nursing
Supplemental Material
sj-doc-2-son-10.1177_23779608261424662 - Supplemental material for Practice of the Professional Code of Ethics and Associated Factors Among Midwives in Amhara Regional State Referral Hospitals, Ethiopia, 2024: A Mixed-Methods Study
Supplemental material, sj-doc-2-son-10.1177_23779608261424662 for Practice of the Professional Code of Ethics and Associated Factors Among Midwives in Amhara Regional State Referral Hospitals, Ethiopia, 2024: A Mixed-Methods Study by Tadesse Getu, Getie Lake, Samrawit Abebaw, Aregash Sitot and Animut Tagele in SAGE Open Nursing
Footnotes
Acknowledgment
We would like to thank all participants who took part in the study.
Ethics Statement
Ethical clearance was obtained from the Institutional Review Board (IRB) of the University of Gondar, College of Health Sciences, School of Midwifery, before the commencement of the study with Ref No: Mid/W.H/28/2016 E.C. Responsible officials and managers at hospitals were communicated, and permission letters were obtained. Before data collection, written informed consent was obtained from the quantitative and qualitative study participants.
Consent for Participate
The participants provided their written informed consent to participate in this study.
Author Contributions
TG developed the study's conceptualization, data curation, methodology, data analysis, and initial and final draft. GL, AT, and AS participated in conceptualization, methodology, and critical revision of the article. SA, GL, and AT participated in data curation, the methodology, and draft review and editing. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset used and analyzed during the current study is available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.