
Abstract
Introduction
Children with Type 1 diabetes face complex medical and psychosocial challenges in school settings, often requiring support from educators, yet Jordanian teachers often lack sufficient training to support these students effectively.
Objectives
To evaluate the effectiveness of a structured, theory-based educational intervention in enhancing primary school teachers’ knowledge, attitudes, and self-efficacy for managing Type 1 diabetes.
Methods
Quasi-experimental, non-equivalent control group, pre-test/post-test design. Eight public primary schools in Amman, Jordan, were purposively selected. A total of 139 teachers (intervention n = 78; control n = 61) completed validated Arabic questionnaires assessing Type 1 diabetes knowledge, attitudes, and self-efficacy before and after a single 3-h session grounded in Bandura's social cognitive theory. The session included presentations, group discussions, videos, and printed materials—repeated measures analysis of variance was used to evaluate the outcomes.
Results
The main effects of time, group, and their interaction were statistically significant (p < .001). In the intervention group, significant improvements from pre- to post-test in all outcome domains: knowledge (M = 56.11 to M = 77.15), attitudes (M = 94.23 to M = 102.87), and self-efficacy (M = 25.54 to M = 33.78) (p < .001). No significant changes were observed in the control group. Prior experience with students with Type 1 diabetes did not moderate any outcome.
Conclusions
A brief, structured, theory-driven educational session significantly enhanced teachers’ preparedness to manage Type 1 diabetes in the classroom, supporting the integration of standardized diabetes education programs to foster safer, more inclusive school environments.
Keywords
Introduction/Background
Type 1 diabetes (T1D) is a common childhood illness worldwide, affecting 8.75 million people, including 1.52 million children and adolescents (International Diabetes Federation, 2022). T1D requires complex daily management of insulin, blood glucose levels, and lifestyle choices, posing serious health risks such as severe hypoglycemia, which can lead to convulsions, coma, and death (Issa, 2022; Puckett et al., 2023).
In Jordan, the prevalence of T1D is 6,340 cases, and the incidence is rising by 4.9% annually. With peak onset occurring between ages 6–8, 40.7% of cases present with diabetic ketoacidosis at diagnosis (Alassaf et al., 2019). This places a significant burden on the education system, as management responsibility often extends to school staff. However, school personnel are often unprepared to address the complex medical and psychosocial needs of students with T1D. Studies consistently reveal a persistent gap in teachers’ knowledge and confidence in responding to diabetes-related issues, particularly in emergency situations (Armas Junco & Fernández-Hawrylak, 2022; Issa, 2022; Haridi & Alshammari, 2021).
Literature Review
Evidence from the region underscores the gap in teachers’ knowledge and confidence in addressing diabetes-related issues. For instance, in Saudi Arabia, despite a high incidence rate, studies found that only 34.4% of male teachers knew the normal blood sugar levels, merely 3.1% reported having a school nurse, and only 10.8% of teachers had received training to support students with T1D (Issa, 2022; Haridi & Alshammari, 2021). This lack of appropriate support puts children with T1D at increased risk for school absenteeism, social exclusion, and emotional distress (de Wit et al., 2022; Fried et al., 2020).
International guidelines recommend ongoing staff education in diabetes care (Cogen et al., 2024; Lawrence et al., 2022). Despite this consensus, formal diabetes education for teachers is rare in many countries, including Jordan. Research suggests that Jordanian educators already exhibit notable knowledge and self-efficacy gaps in T1D management (Al-Shorman et al., 2023), a gap that is compounded by the lack of training programs.
Although previous studies in Jordan have focused on children and parents or descriptive adherence (Al-Shorman et al., 2023; Sabbah et al., 2024; Salem et al., 2025), no studies have assessed the effectiveness of structured educational interventions for teachers. This study addresses a critical gap by providing evidence of the impact of structured, theory-based education.
Therefore, this study aimed to assess the effectiveness of educational interventions in improving school teachers’ knowledge, attitudes, and self-efficacy in managing students with T1D. The results will guide policymakers in Jordan's Ministry of Education and Ministry of Health in using this evidence-based approach to empower teachers and foster safer school environments.
The Aim and Hypotheses
The purpose of this study was to evaluate whether a structured educational intervention improves teachers’ knowledge, attitudes, and self-efficacy in managing T1D.
Theoretical Framework
This study is grounded in Bandura's social cognitive theory (SCT), a widely accepted framework for understanding learning and behavioral change in educational and health contexts. It posits that people learn through interactions among personal factors, behavior, and environmental influences (Bandura, 1986). Central to SCT is self-efficacy, an individual's belief in their ability to perform a behavior successfully (Bandura, 1977).
SCT provides a framework for developing interventions that enhance teachers’ knowledge, attitudes, and self-efficacy in supporting students with T1D. Bandura (1997) emphasizes that strong self-efficacy beliefs increase the likelihood of adopting and maintaining new behaviors. Therefore, empowering teachers to enhance their self-efficacy is crucial for delivering effective diabetes care in schools.
In addition to self-efficacy, SCT encompasses cognitive and affective learning. As teachers’ knowledge and positive attitudes toward students with T1D increase, so does their confidence and willingness to act (Bandura, 1986; Pajares, 2002). This reflects the reciprocal determinism inherent in SCT.
The educational intervention in this study applied SCT by creating a structured, interactive, and psychologically safe learning environment. By focusing on mastery, modeling, verbal persuasion, and emotional arousal, the program aimed to enhance teachers’ knowledge, attitudes, and self-efficacy, which are essential for supporting students with T1D effectively in schools.
Method
Study Design
A quasi-experimental, non-equivalent control group design with pre- and post-test assessments was used. The study was conducted in eight public primary schools under the Directorate of Education in the University District, Amman, Jordan.
Sample and Sampling Procedure
The target population included public primary school teachers (Grades 1–6). The inclusion criteria were full-time employment, willingness to participate, and no prior training in diabetes management. Exclusion criteria included having a first-degree relative with T1D and less than 6 months of teaching experience. A total of 182 teachers enrolled; 139 completed both assessments (experimental n = 78; control n = 61).
Schools were purposively selected for geographic diversity, and teachers were recruited via convenience sampling. A priori power analysis (G*Power 3.1) indicated that 100 participants would be sufficient to detect a moderate effect size (η2 = 0.04) at 80% power and α = .05. Anticipating a 50% attrition rate, the estimated total sample size was increased to 150 participants, with 75 participants in each of the two groups.
Sampling was conducted in two stages. First, eight schools (four for girls, four for boys) were purposively selected from 41 public primary schools in Amman to ensure geographic representation. Second, convenience sampling was used to recruit eligible teachers from these schools. Of approximately 270 teachers approached, 88 were excluded for failing to meet the inclusion criteria. The remaining participants were assigned to either the experimental group (n = 101) or the control group (n = 81) based on their willingness to participate and attend the intervention.
Due to the nature of the educational intervention, blinding was not feasible for participants or for those administering it. However, outcome assessors were not involved in group assignment, and data were de-identified prior to analysis to minimize potential bias.
During post-testing, 23 teachers from the experimental group and 20 from the control group were lost to follow-up, resulting in 78 and 61 teachers, respectively, included in the final analysis (see Figure 1).

Participants’ recruitment.
Measures
An Arabic self-reported questionnaire was used as a pre-test and post-test to collect teacher data. It consisted of four parts: demographic characteristics, teachers’ knowledge of T1D, teachers’ attitudes, and teachers’ self-efficacy in managing students with diabetes.
Demographic Data
Collected data included age, gender, educational level, teaching experience, prior T1D exposure, and prior training.
Teachers’ T1D Knowledge and Attitude Scale
Teachers’ knowledge and attitudes towards T1D were measured using the Arabic version of the instrument developed by Aljehany (2016). The questionnaire consisted of two sections: Knowledge of T1D in children and Attitudes towards children with T1D.
The knowledge and Attitude scales were validated by four endocrinologists and two diabetes educators from hospitals in the UK and the KSA. The scale was tested on 540 teachers, and Cronbach's α was .953 (Aljehany, 2016)
Self-Efficacy Scale
Adapted from Atiyeh (2020), this eight-item scale assesses teachers’ confidence in supporting students with T1D. The scale is a 5-point Likert-type scale ranging from 1 = not able at all to 5 = very able. The total score ranges from 21 to 105, with higher scores indicating greater self-efficacy. The scale was modified to include items applicable only to school teachers. The final version of the questionnaire contained eight questions; thus, the total score ranged from 8 to 40. The scale was validated by a panel of expert teams using the Universal Agreement Method (S-CVI/UA), yielding a score of 0.9. Alpha Cronbach was used to assess the reliability of the self-efficacy scale, yielding an α of .852 (Atiyeh, 2020). The Cronbach's α for the scale in the current study was .877.
Data Collection Procedure
Principals of the participating schools were contacted after Institutional Review Board (IRB) approval was obtained. Participant recruitment and data collection took place from September 11, 2024, to October 26, 2024. The study's aim and procedures were explained, and approval was obtained from school principals to meet with teachers at an appropriate time. The availability of each school's resources was assessed, including the lecturing room, computer, and data. During the first visit in both groups, the teachers were introduced to the study, its aim, and the process.
All teachers willing to participate in the study and meet the inclusion criteria (experimental and control groups) were asked to sign the consent form and complete the pre-test questionnaire.. The researcher was available to answer any questions that may arise. During the second visit, the Intervention group received only the educational intervention.
During the third visit, all participants completed the post-test questionnaire. Finally, the Control group received the same training as the post-test group to ensure ethical equity. All sessions were conducted by the principal investigator, a certified educator in clinical health training.
The Interventions
The intervention was based on the IDF's Kids and Diabetes in Schools (KiDS) Toolkit (IDF, 2022) and American Diabetes Association (ADA) recommendations (Helping the Student with Diabetes Succeed: A Guide for School Personnel, 2022). It included a 3-h training session with presentations, videos, discussion, and printed materials.
Participants were trained to Level 2 competency per ADA classification, with an emphasis on both theoretical understanding and emergency preparedness. The content covered diabetes basics, emergency response, nutrition, and communication with students and families. Training was delivered by the principal investigator, a certified educator.
The intervention was explicitly guided by Bandura's SCT, which emphasizes self-efficacy, observational learning, and reciprocal determinism. These principles were operationalized by incorporating interactive teaching strategies, such as modeling appropriate responses to diabetic emergencies, mastery experiences through practice and role-play, and verbal persuasion to boost confidence. Emotional engagement was fostered through discussion and supportive group activities. The learning environment was structured to be psychologically safe, encouraging active participation and cognitive engagement.
By aligning with SCT principles, the intervention aimed to increase teachers’ perceived self-efficacy, improve their knowledge and attitudes toward students with T1D, and foster sustained behavioral change in school-based diabetes support.
Ethical Considerations
Ethical approval was obtained from the authors’ institution and the Ministry of Education. Informed consent was obtained from all participants. Participants reported no adverse events or unintended effects during or after the intervention sessions. The educational nature of the intervention posed minimal risk, and all training was delivered in a supportive and psychologically safe environment.
Data Analysis
Data were analyzed using IBM SPSS Statistics Version 26. Descriptive statistics were used to summarize participants’ sociodemographic characteristics. Means and standard deviations were calculated for continuous variables (e.g., age, years of teaching experience). At the same time, frequencies and percentages were used for categorical variables (e.g., gender, education level, prior experience with students with T1D).
To evaluate the intervention's effectiveness, a repeated measures analysis of variance (ANOVA) was conducted to assess within- and between-group differences over time for the primary outcome variables: knowledge, attitudes, and self-efficacy. The group (intervention vs. control), time (pre-test vs. post-test), and their interaction (Group × Time) were analyzed to determine the impact of the intervention. Effect sizes were reported using partial eta squared (η2).
All statistical tests were two-tailed, with a significance level set at p < .05.
Analyses were conducted on a per-protocol basis, including only participants who completed both pre-test and post-test assessments. An intention-to-treat (ITT) approach was not used, as the aim was to assess the intervention's effect among participants who received the full training and completed the outcome measures. Future studies may consider ITT strategies to mitigate attrition bias.
Results
Participants’ Characteristics by Experimental and Control Groups
Table 1 presents the demographic characteristics of the 139 participants who completed the study, including the experimental group (n = 78) and the control group (n = 61). Gender distribution was similar across groups, with males comprising 44.9% of the experimental group and 47% of the control group. The mean age was slightly lower in the experimental group (M = 39.38, SD = 9.40) than in the control group (M = 42.74, SD = 7.26).
Descriptive Statistics of Participants’ Characteristics by Intervention and Control Group (N = 139).

Note. M = mean; SD = standard deviation.
Control group participants had more teaching experience on average (M = 15.41 years, SD = 7.75) than those in the experimental group (M = 12.25 years, SD = 8.34), with similar ranges across groups (1–31 years). Most participants held a bachelor's degree, although the proportion was higher in the experimental group (82.1% vs. 67.2%). In contrast, postgraduate qualifications were more common in the control group (31.1% vs. 14.1%), and only a few individuals in either group held diplomas. Experience teaching students with T1D was more prevalent in the control group (44.3%) than in the experimental group (35.9%).
Educational Interventions
A series of 2 (Time: Pre vs. Post) × 2 (T1D Experience: Yes vs. No) mixed ANOVAs were conducted to examine the effects of prior experience with students with T1D on teachers’ outcomes over time across three domains: knowledge, attitudes, and self-efficacy.
Knowledge
There was a significant main effect of Time, F(1, 135) = 76.48, p < .001, partial η2 = .362, indicating that overall knowledge scores significantly improved from pre-test (Estimated Marginal Mean [EMM] = 59.37, SE = 0.92) to post-test (EMM = 68.92, SE = 0.70) across all participants (Table 2a and b). A significant Time × Group interaction was observed, F(1, 135) = 110.87, p < .001, partial η2 = .451. Partial η2 indicated large effect size (η2 > .14).
Main and Interaction Effects for Knowledge Scores (Pre–Post Intervention).
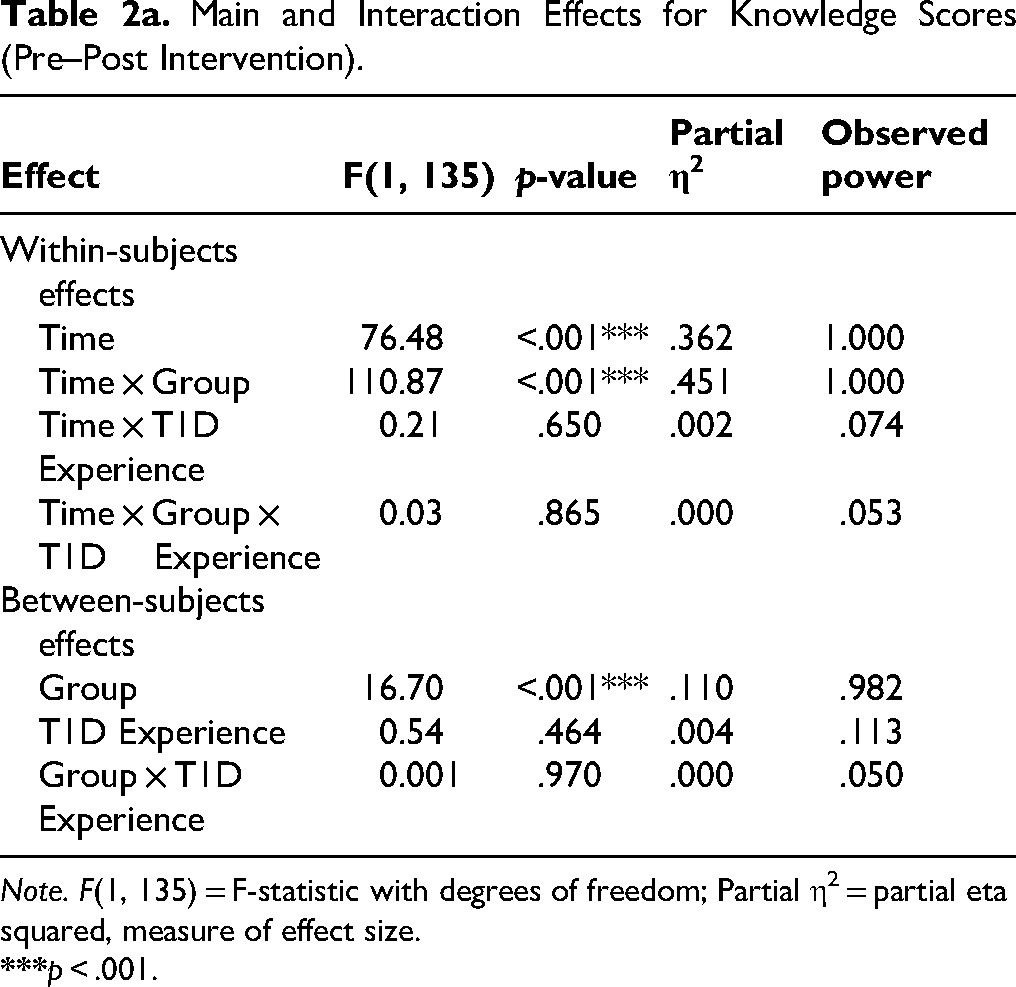
Note. F(1, 135) = F-statistic with degrees of freedom; Partial η2 = partial eta squared, measure of effect size.
EMMs and Descriptive Statistics for Knowledge.

Note. M (SD) = observed mean and standard deviation; EMM = estimated marginal mean; SE = standard error; CI = confidence interval.
Post hoc pairwise comparisons revealed that participants in the intervention group demonstrated a large and significant increase in knowledge from pre-test (EMM = 56.11, SE = 1.24, 95% CI [53.67, 58.55]) to post-test (EMM = 77.15, SE = 0.94, 95% CI [75.28, 79.01]). In contrast, the control group exhibited a slight decrease in knowledge, from pre-test (EMM = 62.63, SE = 1.36, 95% CI [59.95, 65.32]) to post-test (EMM = 60.69, SE = 1.04, 95% CI [58.63, 62.74]).
There was also a significant main effect of Group, F(1, 135) = 16.70, p < .001, partial η2 = .110, indicating that participants in the intervention group had higher knowledge scores across time points compared to those in the control group.
No significant interactions were found for Time × T1D Experience, F(1, 135) = 0.21, p = .650, or for the three-way interaction Time × Group × T1D Experience, F(1, 135) = 0.03, p = .865. This suggests that prior experience with students with T1D did not significantly influence changes in knowledge over time or across groups (Tables 2a and b).
Attitudes
There was no significant main effect of time, F(1, 135) = 3.60, p = .060, partial η2 = .026, indicating no overall change in attitudes from pre- to post-test across groups (Table 3a and b).
Main and Interaction Effects for Attitude Scores (Pre–Post Intervention).

Note. F(1, 135) = F-statistic with degrees of freedom; Partial η2 = partial eta squared, measure of effect size.
**p < .01. ***p < .001.
EMMs and Descriptive Statistics for Attitudes.
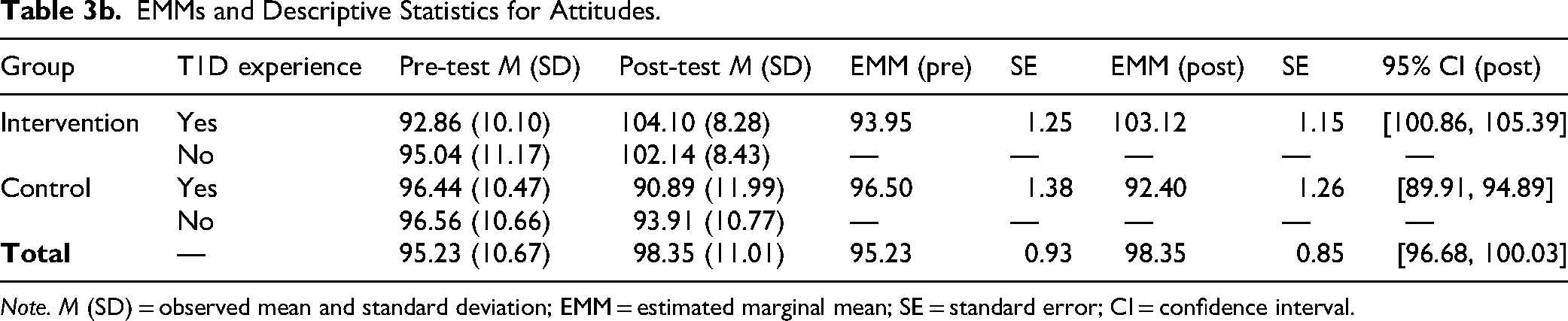
Note. M (SD) = observed mean and standard deviation; EMM = estimated marginal mean; SE = standard error; CI = confidence interval.
A significant Time × Group interaction was found, F(1, 135) = 24.69, p < .001, partial η2 = .155. Partial η2 indicated a large effect size (η2 > .14).
The intervention group improved significantly in attitudes from M = 94.23 (SD = 10.77) at pre-test to M = 102.87 (SD = 8.38) at post-test. The control group showed a decrease from M = 96.51 (SD = 10.49) at pre-test to M = 92.57 (SD = 11.33) at post-test.
A significant main effect of group was also found, F(1, 135) = 11.92, p = .001, partial η2 = .081, indicating higher attitude scores in the intervention group over time.
There were no significant interactions involving prior experience with students with T1D: Time × T1D Experience, F(1, 135) = 0.05, p = .818; and Time × Group × T1D Experience, F(1, 135) = 1.74, p = .189 (Table 3a and b).
Self-Efficacy
There was a significant main effect of time, F(1, 135) = 22.84, p < .001, partial η2 = .145, indicating a general increase in self-efficacy from pre-test to post-test across all participants (Table 4a and b). Importantly, a significant Time × Group interaction was found, F(1, 135) = 51.65, p < .001, partial η2 = .277. Partial η2 indicated a large effect size (η2 > .14).
Main and Interaction Effects for Self-Efficacy Scores (Pre–Post Intervention).

Note. F(1, 135) = F-statistic with degrees of freedom; Partial η2 = partial eta squared, measure of effect size.
***p < .001
EMMs and Descriptive Statistics for Self-Efficacy.

Note. M (SD) = observed mean and standard deviation; EMM = estimated marginal mean; SE = standard error; CI = confidence interval.
The intervention group showed a substantial improvement in self-efficacy scores, increasing from M = 25.54 (SE ≈ 0.70) to M = 33.78 (SE ≈ 0.63), while the control group declined slightly from M = 26.77 to M = 25.31.
There were no significant effects involving prior experience teaching students with T1D: Time × T1D Experience, F(1, 135) = 1.42, p = .235, and Time × Group × T1D Experience, F(1, 135) = 2.04, p = .156 (Table 4a and b).
Discussion
This study evaluated the impact of an educational intervention on teachers’ knowledge, attitudes, and self-efficacy in managing students with T1D. Findings demonstrate that a structured educational session significantly improved all three outcome variables in the intervention group compared to the control group. Along with the results of the present study, previous literature has shown the effectiveness of educational interventions in improving knowledge, attitudes, and self-efficacy regarding T1D (Aljehany, 2016; Gutierrez, 2020; Hamza et al., 2022).
The intervention group demonstrated substantial, statistically significant gains in knowledge, resulting in post-test scores markedly higher than baseline. The control group showed a slight decline in average knowledge score. This finding aligns with findings from Hamza et al. (2022) and Gutierrez (2020), who reported similar post-intervention gains among school personnel following diabetes training. Consistent with Bandura's SCT, these results suggest that providing mastery experiences and vicarious learning through interactive modules and real-life scenarios boosted teacher confidence and competence.
Attitude improvements were also observed in the intervention group, whereas the control group's attitudes declined. Although the overall time effect on attitudes was not significant, the interaction effect indicates that the intervention had a differential impact over time. Consistent with our findings, recent studies have documented significant improvements in teachers’ attitudes following targeted educational interventions. For instance, a randomized pre-post study found that a brief educational module significantly reduced stigmatizing attitudes among school teachers toward students with obsessive-compulsive disorder. However, no such change was seen in controls (Chaves et al., 2021). Similarly, broader evidence suggests that interactive, teacher-focused interventions in chronic health education lead to positive shifts in attitudes, emphasizing that a single exposure is often insufficient and that ongoing reinforcement is crucial.
Teachers’ self-efficacy in managing students with diabetes increased significantly in the intervention group. In contrast, the control group experienced a slight decline. The improvements in self-efficacy are significant, as teacher confidence is crucial for managing medical conditions in school settings. According to Bandura (1977), such gains are a direct consequence of increased perceived competence and observational learning, key mechanisms in the intervention design. Our findings confirm the effectiveness of interventions that utilize interactive, multimodal methods, including discussions, case studies, videos, and printed materials, as supported by dos Anjos Coelho Rodrigues Dixe et al. (2020). Significantly, this study extends current evidence by evaluating a population of Jordanian public school teachers, for whom few diabetes education interventions have been documented.
While the intervention group showed significant gains across all domains, the control group exhibited a slight decline in scores for knowledge, attitudes, and self-efficacy. This decline, although not statistically significant, warrants careful discussion. This outcome may be attributed to several factors. Firstly, T1D management is complex, and in the absence of a structured educational intervention, the observed decline may reflect the natural decay of initial knowledge and confidence over the study period, as no reinforcement was provided. Secondly, the control group included a notable proportion of teachers with prior experience of T1D among students (44.3%). Experiencing a challenging or acute T1D management situation between the pre-test and post-test, without adequate training, could negatively affect their perceived confidence and attitudes, resulting in a decrease in the observed score. Finally, the slight drop may also reflect regression toward the mean or the effect of being measured twice without the benefit of new information, potentially increasing awareness of existing knowledge gaps and difficulty with the post-test.
The KiDS Toolkit, endorsed by IDF and ISPAD, provided a valuable framework for the intervention. As noted by Bechara et al. (2018), such programs not only increase knowledge but also enhance willingness to act in emergencies, which is crucial for child safety in schools.
Implications for Practice
School nurses and community health nurses should play a central role in implementing and supervising diabetes education in schools. Nurses can serve as trainers, resources, and evaluators of teacher preparedness. Integrating nurse-led sessions with the KiDS Toolkit may increase teacher efficacy and student safety.
The Ministry of Education in Jordan should mandate structured diabetes training for all school personnel, particularly in public schools where access to school nurses is limited. Health policy should support intersectoral collaboration between educational institutions and healthcare providers to ensure the sustainability of programming.
Future studies should examine the long-term effects of interventions on teacher behaviors and student health outcomes (e.g., HbA1c levels). Future research could also explore the effectiveness of online or hybrid training formats compared to traditional in-person methods. Additionally, investigate how teacher self-efficacy mediates the relationship between student safety and diabetes management in schools.
Strengths and Limitations
This study possesses several strengths. It is among the first in Jordan to evaluate a structured, theory-based educational intervention for improving teachers’ preparedness to manage T1D in schools. The intervention was grounded in Bandura's SCT, which provided a robust conceptual framework for understanding behavioral change. The use of validated, reliable instruments with high internal consistency enhanced the credibility of the findings. Moreover, the inclusion of both male and female teachers from multiple schools across different districts of Amman improved the sample's representativeness and strengthened its generalizability to similar educational contexts. The study also ensured ethical rigor by offering the educational program to the control group after data collection, maintaining fairness and minimizing potential inequities.
Despite these strengths, several limitations should be acknowledged. The study was conducted exclusively in public schools within Amman, which may limit the generalizability of the results to private or rural schools. The data were obtained from self-reported questionnaires, which may have introduced recall or social desirability bias. Outcomes were measured shortly after the intervention, making it unclear whether the observed improvements are sustained over time. Additionally, the quasi-experimental design without random assignment limits the ability to infer causal relationships and may introduce selection bias. Finally, the study did not include direct behavioral observations or student outcomes, which could provide richer insights into real-world application and long-term effectiveness.
Future studies should consider randomized controlled trials, longitudinal follow-up, and larger, more diverse samples across multiple regions. Incorporating qualitative components or observational measures would also help capture changes in teacher behavior and confidence in actual classroom settings.
Conclusion
This study demonstrates that structured educational interventions significantly enhance teachers’ knowledge, attitudes, and self-efficacy in managing students with T1D. Grounded in Bandura's SCT, the intervention facilitated behavioral change by enhancing self-belief, promoting observational learning, and promoting knowledge acquisition.
These results underscore the critical role of professional development in preparing school personnel to support children with chronic conditions. Enhanced teacher competence contributes to safer school environments and improved student outcomes, including glycemic control and academic success. The findings advocate for institutionalizing such interventions within public school systems, particularly in resource-limited settings like Jordan.
Supplemental Material
sj-docx-1-son-10.1177_23779608261419908 - Supplemental material for Educators’ Competence in Managing Type 1 Diabetes in Schools: A Quasi-Experimental Intervention Study
Supplemental material, sj-docx-1-son-10.1177_23779608261419908 for Educators’ Competence in Managing Type 1 Diabetes in Schools: A Quasi-Experimental Intervention Study by Nadeen Afeef Allefdawi, Nahla Al Ali and Samia Alharrasi in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608261419908 - Supplemental material for Educators’ Competence in Managing Type 1 Diabetes in Schools: A Quasi-Experimental Intervention Study
Supplemental material, sj-docx-2-son-10.1177_23779608261419908 for Educators’ Competence in Managing Type 1 Diabetes in Schools: A Quasi-Experimental Intervention Study by Nadeen Afeef Allefdawi, Nahla Al Ali and Samia Alharrasi in SAGE Open Nursing
Footnotes
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the author(s) used ChatGPT by OpenAI to assist with academic language editing, abstract and cover letter drafting, and improving clarity and conciseness of the manuscript. After using this tool, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the published article.
Acknowledgments
I sincerely acknowledge the Deanship of Research at Jordan University of Science and Technology for supporting this study. I would also like to thank all participating teachers for dedicating their time to attend the training program sessions.
Ethical Considerations
Ethical approval was obtained from Jordan University of Science and Technology's IRB (Ref: 34/170/2024) and the Jordanian Ministry of Education (Ref: 3/10/35543). Informed consent was obtained from all participants.
Authorship Contributions
Based on the journal's CRediT authorship requirements, all listed authors contributed substantially to the work as follows: Nadeen Afeef Allefdawi: conceptualization, methodology, investigation, and writing–review and editing. Nahla Al Ali: conceptualization, formal analysis, methodology, writing–original draft preparation, and writing–review and editing. Samia Alharrasi: investigation, methodology, and writing–review and editing. All authors meet the journal's requirement of contributing to at least one core research activity (conceptualization, methodology, formal analysis, or investigation) and at least one writing activity (original draft or review and editing). All authors approved the final manuscript and agree to be accountable for the work.
Submission Declaration
I hereby declare that the work described in this manuscript has not been published previously, except as an academic thesis. Furthermore, I confirm that this article is not under consideration for publication elsewhere. The publication of this article has been approved by all authors and tacitly or explicitly by the responsible authorities where the work was carried out.
Data Availability
Data will be available upon request from the editors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.