
Abstract
Background
Self-care management (SCM) is a cornerstone in the management of diabetes mellitus (DM), as it has a positive impact on glycemic control.
Aims
To investigate the level, specific practices, correlates, and predictors of SCM practices among Jordanian adult patients with type 1 diabetes (DM1).
Methodology
Using an online self-report questionnaire, a convenience sample of 127 DM type 1 patients were recruited who agreed to complete the questionnaire. The questionnaire had four sections; demographics, the diabetes self-efficacy scale (DSES), the appraisal of self-care agency scale-revised (ASAR-R), and the Diabetes Self-Management Scale (DSMS).
Results
The mean score of the total Diabetes Self-Management Scale (DSMS) of patients was 204.16 (SD = 40.35, range = 97–299). We found that SCM practices differed between patients according to their characteristics; the SCM-Activity and SCM-Food differed according to gender, educational level, and income. Furthermore, there were significant negative relationships between the duration of being diagnosed with DM and SCM-activity, and between BMI and each of SCM-Blood glucose monitoring and SCM-adherence to the medication regimen. Lastly, sequential regression showed that income, self-efficacy (SE), and self-care agency (SCA) were significant predictors of SCM.
Conclusions
Patients with DM type 1 exhibit different levels of SCM according to their personal and clinical characteristics. Tailored health education plans should be provided to patients according to their risk factors for low SCM practices.
Background
Diabetes mellitus (DM) is one of the most common chronic diseases that causes serious complications in many organs (WHO, 2021). According to the International Diabetes Federation Report, 8.75 million people were diagnosed with type 1 diabetes (DM1). In 2022, the Middle East and North Africa region was ranked as the third largest region having the highest number of cases of DM1. In Jordan, there were 6,344 people diagnosed with DM1 in 2022; around three-fourths of them aged between 20 and 59 years (Ogle et al., 2022).
To overcome the distress caused by chronic disease (Darawad et al., 2017), patients with DM type 1 and 2 need to accept it as part of their daily lives (Ait-Taleb Lahsen et al., 2023), that is, Normalizing (Babler and Strickland, 2015). Self-care management (SCM) is considered a cornerstone in managing DM for both type 1 and 2, as it has a positive impact on glycemic control (Al-Khawaldeh et al., 2012; Chupradit et al., 2021; D'Souza et al., 2017; Gao et al., 2013; Hammad et al., 2015; King et al., 2010; Rawlins et al., 2017). SCM includes seven practices that are healthy eating, being active, taking medications, self-monitoring, problem solving, coping, and reducing risks (American Association of Diabetes Educators, 2009).
All self-care practices are affected by the patient's beliefs about his own ability to do these practices, in other words, patient's self-efficacy (Al-Khawaldeh et al., 2012; Albargawi et al., 2017; Gao et al., 2013; Gharaibeh et al., 2016; Masoompour et al., 2017; Walker et al., 2014). Health care professionals should focus on improving patient self-efficacy to improve their performing of self-care practices (Mohebi et al., 2013). Self-efficacy is a very important factor for performing self-management activities for DM (D'Souza et al., 2017; Gao et al., 2013; Gharaibeh et al., 2016; Kav et al., 2017; King et al., 2010; Masoompour et al., 2017; Walker et al., 2014). Self-efficacy determines one's achievement and, as a result, his quality of life, Bandura claims that self-efficacy is a very important determinant for ones’ agency (Bandura, 1997).
Self-care agency (SCA) is one of the main concepts of self-care theory, and can be reflected in the abilities and limitations of the patient in performing self- care practices (Alligood, 2014; Eddings, 2012). If SCA is inadequate, self-care deficit or dependent care agency is indicated to be present (Alligood, 2014). Patients with DM who had higher levels of self-efficacy and SCA committed more to SCM, and thus improved clinical outcomes (Eddings, 2012; Sousa et al., 2005).
Patients’ adherence to perform self-management varies and is affected by many factors. Self-management of diabetes was associated with age, gender, level of education, and duration of DM (Alrahbi, 2014). Ishak et al. (2017) found that having a family caregiver, social support (especially family), knowledge of the disease, and having nephropathy had a positive impact on SCM, while having neuropathy had a negative one on self-care.
In Jordan, DM affected about 13.1% of adults, and its prevalence is increasing (World Health Organization, 2016). It was responsible of 7% of deaths among all ages and considered the sixth leading cause of death in Jordan based on WHO report in 2016 (World Health Organization, 2016).
Diabetes as a non-communicable disease has many complications, which needs management as well. SCM plays an essential role in managing diabetes and its complications. Performing self-management activities depends on many factors like psychosocial factors, family and social support. In addition, it depends on patient's capability to perform SCM activities, and his/her beliefs in owns’ ability to perform these activities (American Diabetes Association, 2017). In other words, SCA and self-efficacy are important factors in adaptation to and performing self-management in DM and other non-communicable diseases.
The level of SCM was investigated and was evident to be low among Jordanian patients with diabetes, especially doing exercises (Darawad et al., 2017). However, SCM and specific practices performed by Jordanian patients with DM1 were not investigated. Additionally, predictors of practicing such practices were not studied. Therefore, this study aims to investigate the level, specific practices, and correlates of SCM practices among Jordanian patients with DM1. Specifically, this study answered the following research questions:
What is the level of self-care management among Jordanian patients with DM1? Which of the self-care management practices do Jordanian patients with DM1 perform the most and least? Based on categorical demographics, what are the differences in self- care management practices among Jordanian patients with DM1? What are the predictors of self-care management among Jordanian patients with DM1?
Literature Review
Type 1 DM (T1DM) results from autoimmune pancreatic Beta cells destruction leading to complete insulin deficiency, and thus totally depending on insulin. Therefore, it is called insulin dependent DM or Juvenile diabetes, but T2DM can occur in children too. There is another type of T1DM, which is the idiopathic T1DM. The pathophysiology of T1DM is much more developed than in T2DM. Based on clinical studies, the presence of two or more autoantibodies is considered a predictor of T1DM. The progress rate depends on many factors like the time of first detection of these antibodies, number of antibodies, antibodies’ specificity and titer (American Diabetes Association, 2017).
Patients with chronic diseases such as DM need to depend on their selves to manage their disease; they have to accept it as part of their daily lives. In other words, Normalizing, or accepting DM as part of their selves (Babler & Strickland, 2015). Self-management is considered a cornerstone in managing DM, as it has a positive impact on glycemic control (Al-Khawaldeh et al., 2012; D'Souza et al., 2017; Gao et al., 2013; King et al., 2010). Self-management includes seven behaviors which are healthy eating, being active, taking medications, self-monitoring, problem-solving, coping, and reducing risks (American Association of Diabetes Educators, 2009). In addition, the American Diabetes Association includes smoking cessation and DSME/S as aspects of lifestyle management for patients with DM (American Diabetes Association, 2017).
Patients’ adherence to self-management varies and is affected by many factors. An Omani study investigated self-management status among 266 Omani patients with DM. Results revealed that 77% had their medication regularly, 26% performed problem-solving regularly, 18% had a healthy diet, 13.5% assessed and cared for their feet regularly, 9.5% exercised regularly, 3% performed specific activities to reduce DM risk and complications, and only 1% were performing self-monitoring of blood glucose (SMBG). Diabetes self-management was associated with age (younger patients committed to performing exercises and foot care more), gender (male patients tend to exercise more and female patients committed to taking their medications more), level of education (those with higher education committed to self-management more), and duration of DM (those who diagnosed with DM for 6 years or more were performing problem-solving more than those who diagnosed 5 years or less) (Alrahbi, 2014).
Subjects, Materials, and Methods
In the current study, a nonexperimental cross-sectional descriptive design was used, as part of a larger research project, using an online self-report questionnaire uploaded to Google Forms in the period November 2023 to February 2024. This study was conducted in two large hospitals in the main cities of Jordan; Amman (the capital) and Irbid as those referral hospitals had the largest bed capacity.
Sampling
Non-probability, a convenience sample was used to select the study sample. The inclusion criteria were to be 18 to 30 years old, had a medical diagnosis of DM1 for more than 6 months and were able to use a smartphone or computer to complete the online questionnaire. Critically ill patients and those with mental or physical disabilities were excluded from the study.
Sample size was determined based on Cohen power primer (Cohen, 1992). Using conventional power of .8, medium effect size of 0.25 and level of significance of .05 and analysis of variance (ANOVA), the minimum sample size would be 64 for each group of intervention and control groups. Using G-power 3.1.9.2, and using power of .8, medium effect size (0.25), and level of significance of .05 and ANCOVA, the minimum total sample size would be 128 (Faul, 2014).
Data Analysis
The current study used a questionnaire consisting of four sections, including (a) demographics, comorbidities, and health education on diabetes, (b) the diabetes self-efficacy scale (DSES), (c) the appraisal of self-care agency scale-revised (ASAR-R), and (d) the Diabetes Self-Management Scale (DSMS). The questionnaire was translated into Arabic according to WHO guidelines of translation (World Health Organization, 2018). Then, piloting was done to develop the final version of the questionnaire.
The second section was the Diabetes Self-Efficacy Scale (DSES), which measures the patient's confidence in performing specific practices to manage their disease (Sousa et al., 2009). This scale consisted of 60 items with seven subscales including eating healthy foods (15 items), his activity (6 items), blood glucose monitoring (7 items), adherence to the medication regimen (specifically insulin) (6 items), foot care (7 items), problem solving (4 items), and reducing risks (15 items). The scale is rating self-efficacy on a six-point Likert scale (0-Strongly Disagree to 5-Strongly Agree). The possible total score ranges from 0 to 300, with a higher score indicating a higher level of self-efficacy in performing self-care practices. According to Sousa et al. (2009), the Scale Level Content Validity of the DSES was 0.97, and the Item Level Content Validity ranged from 0.8 to 1.0 for item level (Sousa et al., 2009).
The third section was the ASAR-R that measures whether the participant is capable to perform self-care practices in managing diabetes (Sousa et al., 2010). It consists of 15 items with three subscales that include having (six items), developing (five items), and lacking power (three items) for self-care. The scale is rating SCA on the Five-Point Likert scale (1-Totally Disagree to 5-Totally Agree), and the scores of four items must be reversed. The possible total score ranges from 15 to 75, and the higher score indicates a better level of SCA. Sousa et al. (2009) reported that the scale is valid and reliable, and has a very good fit and good internal consistency with Chronbach's alpha of 0.89 (Sousa et al., 2009).
The fourth section was the Diabetes Self-Management Scale (DSMS), which was developed based on Orem's theory of self-care. This scale consisted of the same 60 items, subscales, and ratings as those in DSES, but DSMS measures the patient's performance of specific practices to manage their disease instead of confidence (Sousa et al., 2009). The higher score indicates better adherence to self-care practices, with a possible score (0–300). According to Sousa et al. (2009), the content validity for item level was higher than 0.78, except for one item, it was 0.7, while the content validity for the scale level was 0.96 (Sousa et al., 2009).
This study protocol was ethically reviewed and approved by the Institutional Review Board (IRB) of the Scientific Research Committee of the Faculty of Nursing of the University of Jordan and the Ministry of Health. After obtaining the ethical approvals from the University of Jordan and the Ministry of Health, one of the research team approached the nurses’ managers of the diabetes clinic in selected hospitals, to explain the purpose, procedure of the study, and to obtain permission to meet eligible participants. Then, they were invited to participate in the study by asking them to sign the informed consent that explained the purpose of the study and the rights of the participants. Subsequently, the online questionnaire link was sent to the provided phone numbers and asked to fill it out during the waiting time at the clinic. The estimated time to complete the questionnaire was approximately 15 to 20 minutes. During that time, the research team member was available to respond to any concerns or questions.
Statistical Analysis
Statistical Package for Social Science (SPSS) for windows (version 25) was used for data analysis (IBM Corporation, 2017). Based on the level of measurement, descriptive values (means, SDs, and frequencies) were used to describe the variables of interest, with a level of significance < .05. Data were checked for missing data and outliers, and were managed using the most appropriate procedure. Furthermore, t-test and ANOVA were performed to assess differences in self- care management practices based on categorical demographic variables. Also, hierarchical multiple linear regression analysis was performed to calculate the amount of variance in the SCM level that could be explained by continuous demographics, self-efficacy, and SCA.
Results
The sample consisted of 127 participants; their age ranged from 18 to 30 years (M = 23.47, SD = 4.13), 58.3% of them were females (n = 74), and three-quarters of them were single (n = 96) (See Figure 1).

Flow diagram for participants.
Based on BMI, their mean weight was within normal limits (M = 24.16 ± 4.32). About one third of them reported being smokers (n = 39), and most of them received health education about DM (91.3%, n = 116). For further details, see Table 1.
Participants’ Characteristics (N = 127).

Participants’ Diabetes Self-Care Management
The total DSMS mean score of the participants was 204.16 (SD = 40.35, Range = 97–299). For detailed reported responses to DSMS scale and subscales, see Table 2. The highest scores in SCM practices were related to “Problem Solving” (M = 4.36 ± 0.80), followed by “Adherence to Medication Regimen” (M = 4.11 ± 0.79). While the lowest scores were related to “Eating Healthy Foods” (M = 2.96 ± 0.77) and “Activity” (M = 3.08 ± 1.17).
Participants’ Diabetes Self-Care Management Scores.

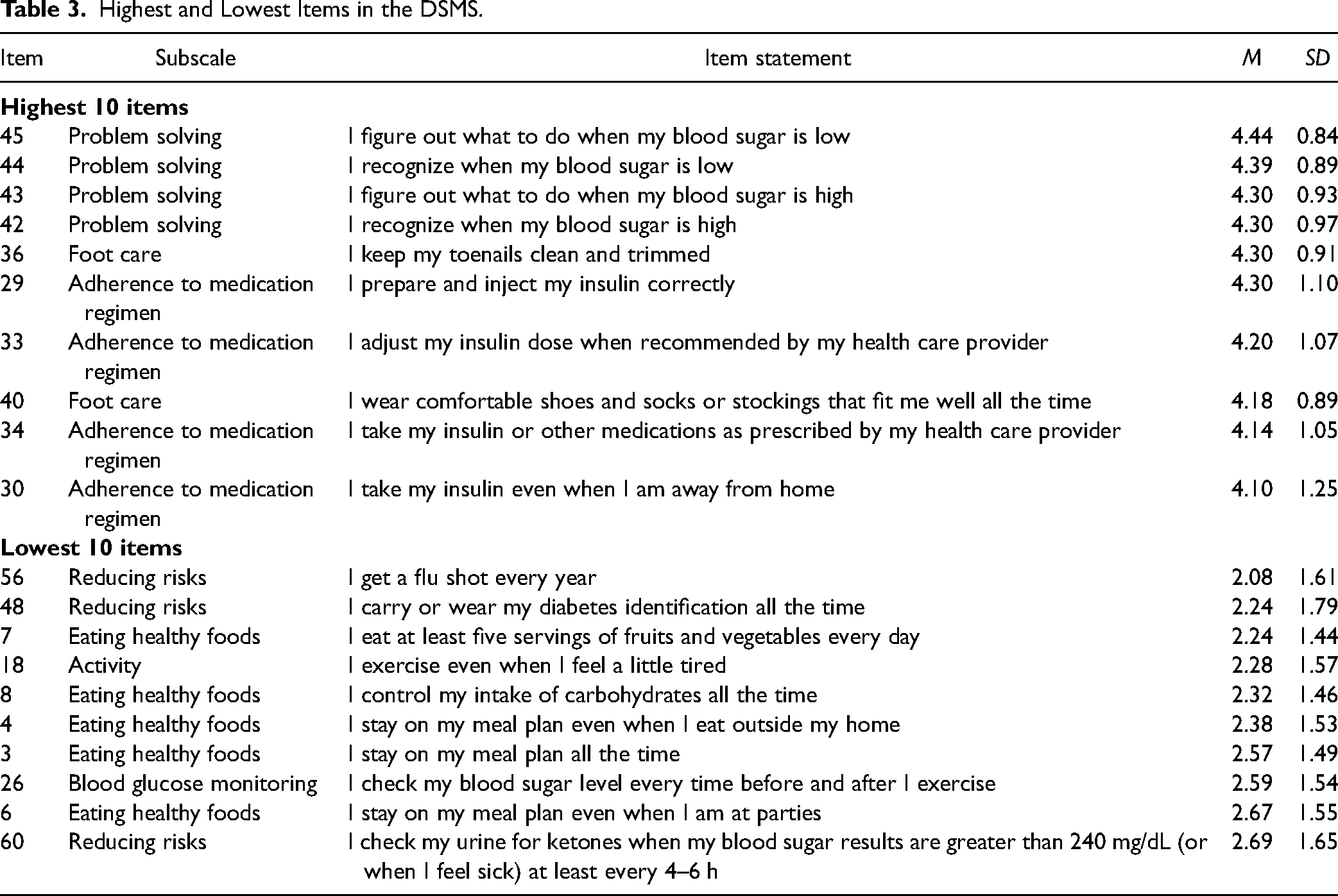
Furthermore, high or low DSMS items’ scores were detected by calculating responses of the participants to each single item, see Table 3. The highest scores were related to “Problem Solving”, “Adherence to medication regimen” and “Foot Care” subscales. The highest mean was for item 45: ‘I can figure out what to do when my blood sugar is low” (M = 4.44 ± 0.84) followed by item 44: “I recognize when my blood sugar is low” (M = 4.39 ± 0.89). On the other hand, the lowest scores were related to “Reducing Risks”, “Eating Healthy Foods”, “Activity” and “Blood Glucose Monitoring”. The lowest mean was for item 56: “I get a flu shot every year” (M = 2.08 ± 1.61) preceded by item 48: “I carry or wear my diabetes identification all the time” (M = 2.24 ± 1.79).
Highest and Lowest Items in the DSMS.
Differences in Self-Care Management Levels of Patients with DM1
t-Test and ANOVA were used to assess the differences in participants’ scores of DSMS based on their demographics and other characteristics; only significant results were reported. The actual performance of the participants in “exercises and activities” (SCM-Activity) differed significantly according to their gender (t (125) = 2.614, p = .01). The mean of SCM-Activity for male participants (M = 20.34, SD = 6.82) was higher than that for female participants (M = 17.11, SD = 6.91). Furthermore, the SCM activity of the participants differed significantly according to their education (t (125) = 2.015, p = .046). Participants who have less than a BSc degree (M = 19.54, SD = 6.26) exercise more than those who have a higher BSc degree (M = 17.04, SD = 7.75). Furthermore, the SCM-Activity significantly differed based on their income (t (125) = 3.175, p = .002). Those with an income ≤ 500 JD (M = 19.61, SD = 6.66) exercise more than those with higher income (M = 15.29, SD = 7.13).
Furthermore, participants’ management and control of their food (SCM-Food) significantly differed according to their education (t (125) = 2.275, p = .025) and income (t (125) = 2.128, p = .035). Those who hold less than BSc degree (M = 46.60, SD = 11.76) control their food more than those who hold a higher degree of BSc (M = 41.40, SD = 13.96). As well, those with lower income (M = 45.81, SD = 12.62) control their food more than those with higher income (M = 40.35, SD = 13.25). Finally, participants’ total DSMS differed significantly based on their income (t (125) = 2.07, p = .041). Those with lower income (M = 208.58, SD = 40.81) performed SCM activities more frequently than those with higher income (M = 192.06, SD = 36.99).
Pearson coefficient was used to detect any relationship between demographics, clinical variables and total scores of DSMS and each subscale, based on their level of measurement (Table 4). There were significant negative relationships between the duration of being diagnosed with DM (r = −.23, p = .05) and SCM-Activity. More specifically, those who had being diagnosed with DM for a shorter period of time exercised more frequently than those who had been diagnosed with DM for a longer period of time. Furthermore, there were significant negative relationships between BMI and each SCM-Blood glucose monitoring (r = −.20, p = .05) and SCM-Adherence to medication regimen (r = −.25, p = .01). This indicates that participants with lower BMI monitor their blood glucose and adhere to their medication more than those with lower BMI.
Correlations Between T1DM Patients’ Related Factors and DSMS and Subscales.

Correlation is significant at P = .05.
Correlation is significant at P = .01.
Predictors of SCM among Jordanian Patients with T1DM
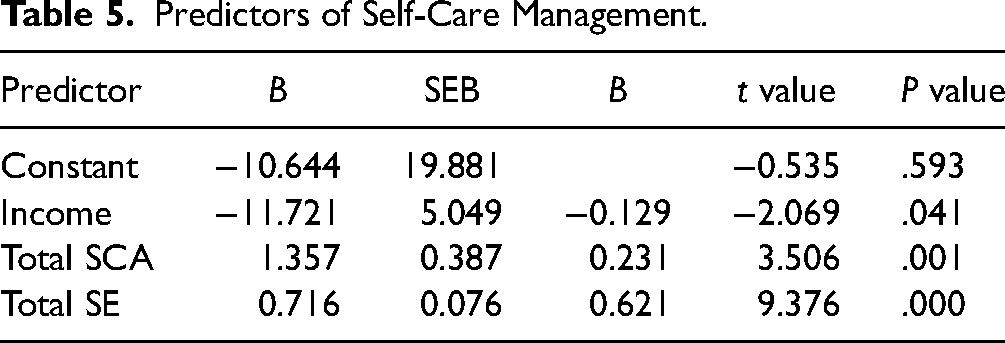
To investigate the predictors of SCM, sequential regression was carried out. Initially, based on the results of bivariate correlations between demographics, clinical variables, Total SE, Total SCA and Total DSMS, only significant variables were entered in the model. Only income, among all variables, was significantly correlated with total DSMS. Additionally, Total SE and Total SCA were significantly correlated with total DSMS. Therefore, income, Total SE and Total SCA were entered into the sequential regression models in 2 blocks. Income was entered into the first block and Total SE and Total SCA were entered into the second block. The results showed that income, Total SE and Total SCA were significant predictors of SCM. Besides, the overall prediction model, including three predictors, was statistically significant and represented 63% of the variance in SCM (R = .8, R2 = .63, adjusted R2 = .62, F(3, 123) = 68.36, P < .001). To assess the contribution of individual predictors, the t ratios for the individual regression slopes were examined for each variable in the step when it first entered the analysis. In Step 1, income was statistically significant, t(124) = -2.069, P = .041, R2increment was .033. This indicates that those with a lower income exhibited better SCM. Likewise, Total SE and Total SCA significantly increased the R2 when it was entered in Step 2, Total SCA: t(124) = 3.506, P = .001. Total SE: t(124) = 9.376, P < .001. R2increment in Step 2 was .59. This indicates that those with higher SCA and SE exhibited better SCM. Total SE was the strongest predictor (β = .621, P < .001), followed by Total SCA (β = .231, P = .001), and income (β = −.129, P = .022) (Table 5).
Predictors of Self-Care Management.
Discussion
The objectives of the study were to investigate the levels, practices, predictors of self- care management among DM1 patients. The highest score of self- care management among Jordanian patients withDM1 were related to “Problem Solving”,” Adherence to medication rigmen”, and “Foot Care” subscales. Where the lowest scores were related to “Reducing Risks”, “Eating healthy Food”, “Activity”, and “Blood Glucose Monitoring”. Self- care management varies among DM1 patients based on their gender, education level, and income. The current study revealed that income, SE, and SCA levels are the main predictors of SCM among DM1 patients.
Diabetes SCM is not solely dependent on glycemic blood level; it also includes modifications in all aspects of patient life, such as healthy diet choices, regular exercise, and adherence to medication regimens. When comparing the level of SCM in the current study with a previously published Jordanian survey of diabetes patients (Darawad et al., 2017), the current study's level of SCM is considered accepted. Another study of Chinese patients with DM1 found that they had poor practice of SCM activities (Lin et al., 2016), and that for young Chinese patients with DM2, which were considered below acceptable levels (34.29 (SD = 16.70, Range = 0–77) (Yang et al., 2020). While the level of SCM was considered good among a few Italian patients with T1DM (34.8%, 63) (Caruso et al., 2019). However, the level of SCM in the current study was lower than that of Spanish patients with DM1 (41.6 (SD = 7.9, Range = 11–55) (Alvarado-Martel et al., 2019).
The patients in the current study participated in “problem solving” and “adherence to the medication regimen” more than any other activity. However, many studies reported non-adherent to medication among DM type 2 patients (Alatawi et al., 2016; Babazadeh et al., 2022; Ranjbaran et al., 2020b). In contrast to other activities, they did fewer activities related to “activity” and “eating healthy foods”. This reflected the highest and lowest item scores. The lowest item scores were “I get flu shot every year” preceded by “I carry or wear my diabetes identification all the time”. Many Jordanians, whether they are sick or not, choose not to get vaccinated, because they doubt the efficacy of the vaccines and base their opinions on the experiences of others (Darawad et al., 2017). In addition, Jordanian patients rarely carry any type of identification for any disease, including diabetes identification. According to a Jordanian study of 341 diabetes patients, diet was the practice that was reported the most frequently, while exercise was the least one (Darawad et al., 2017). In the opposite to Iranian study (2020a), where non-adherent to diet is the main issue among patients with DM type 2 (Ranjbaran et al., 2020b). According to a Chinese study of patients with DM1, ‘adherence to treatment’ and “healthy diet” received the highest scores in SCM practices, while ‘foot care’ and “self-monitoring of blood glucose (SMBG)” received the lowest values (Lin et al., 2016).
The current study's findings demonstrated a significant difference between the actual performance of the “exercises and activities” of the participants according to gender, with male patients exercising more. This was anticipated; while male patients can work out anywhere, female patients require specific locations to ensure their privacy. This was consistent with a Chinese study (Xie et al., 2020) and Malaysian study (Hui et al., 2014) of patients with T2DM, where female patients were less likely to exercise regularly. Similar findings were found in Jordanian patients having other chronic diseases (Darawad et al., 2017). Additionally, the results showed that patients who hold less than BSc and those with lower income exercise more than those who hold higher than BSc. Higher earners are more likely to live a sedentary lifestyle, own cars, and work a full-time job with long hours, so they exercise less. Also, because of their lifestyle, they rely on others to prepare their meals or eat junk food, which leads them to make unhealthy decisions. The results were contradictory to a Finnish and Dutch study of the general population, which found that those with higher education exercise more (Droomers et al., 2001; Kari et al., 2020).
Similarly, the results revealed that patients with higher income and educational level control their diet less than those with lower income and educational level. This was contradictory to an Egyptian study that found that higher educational levels were positively correlated with diabetes SCM (El-Radad et al., 2023). These results could be attributed to the fact that people with lower incomes are accustomed to living in particular situations and have learned to modify their needs in light of scarce resources. As a result, they might be better able to control their disease. Based on the literature search, no studies have examined the connections between particular SCM subscales and any of the demographics among patients with DM1. Finally, the results showed a significant difference in the level of SCM based on income; those with higher income performed SCM practices less than those with lower income. This also contradicted what was found in a Jordanian study of patients with DM, mostly T2DM (Adwan and Najjar, 2013), and a Saudi study of patients with T2DM (Al Johani et al., 2015); patients’ levels of SCM improve as their income increases.
We found that self-efficacy and SCA were significant predictors of SCM, consistent with previous research studies’ results. For example, self-efficacy was reported to explain 8% of the variation in self-management among diabetic participants (Abubakari et al., 2016). This result indicates that improvements in self-efficacy lead to improved self-care activities scores (Juarez et al., 2022). In addition, 223 patients with DM2 who reported higher levels of self-efficacy were found to commit more to self-care activities, including diet, exercise, blood glucose monitoring, and medication (Al-Khawaldeh et al., 2012). Furthermore, a study found that patients with DM2 who reported a higher level of SCA perform self-care activities better than those with a lower level of SCA (Eddings, 2012).
Implications and Recommendations
Patients with DM1 exhibit different levels of SCM according to their personal and clinical characteristics. It has been evident that diabetes education and is associated with better SCM; therefore, tailored health education plans should be delivered to patients according to their risk factors for having low SCM practices. Nurses taking care of patients with DM need to be educated about the various aspects of diabetes care. In addition, both self-efficacy and SCA could be used as a framework to guide behavior change and diabetes control interventions among DM1.
Limitations
It is important to note that this study has limitations. Convenience sampling and a narrow age range (18–30 years) are the first two factors that limit the generalizability of the results to this age group of patients with DM1 alone. Still, it is the most effective way to find a sample that fits certain criteria. Another drawback was the use of a self-report questionnaire, which compromises the reliability and validity of the data supplied. Nevertheless, given the geographic dispersion of the population, it was the most effective technique for collecting data. The length of the questionnaire was another area that should be considered; it is possible that participants felt bored while filling out the questionnaire, which led to them providing imprecise information.
Conclusion
SCM practices differed between patients according to their personal and clinical characteristics. Consequently, healthcare providers need to understand the patient demographics, lifestyle habits, and practices that can improve diabetes SCM. This study identifies the constructs of SCM among DM type 1 patients that can help health educators develop personalized health education for patients according to demographics of patients with low SCM.
Footnotes
Acknowledgments
The authors acknowledge the support from the University of Jordan and Applied Science Private University.
Authors' Contribution
All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The ethical approvals from the University of Scientific Research Committee of the Faculty of Nursing of the University of Jordan and the Ministry of Health (10/7/2019- No number) and the Ministry of Health (MOH REC 1800138, 9/10/2019).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.