
Abstract
Background
Anemia is characterized by reduced hemoglobin, hematocrit, or red blood cell counts below normal levels for age, sex, and race. In 2019, globally, the prevalence of anemia in children aged 6 to 59 months was 39.8%, with the highest rate in the African Region at 60.2%. In Ethiopia, this rate reached 52.1%. This study aimed to assess the prevalence and associated factors of anemia in children under five in Ethiopia.
Method
A quantitative cross-sectional study was conducted at Wolkite Health Center and Hospital in March 2024. Participants were selected through systematic sampling, and data were collected via structured interviews and venous blood samples. Data analysis was performed using SPSS version 25, focusing on descriptive statistics and multivariable analysis to identify significant associations, with a significance level set at P ≤ .05.
Results
The overall prevalence of anemia among 164 participants was 39.0%, with 22.6% classified as mild, 13.8% as moderate, and 2.6% as severe. Anemia was significantly associated with inadequate dietary diversity (adjusted odds ratio [AOR] = 2.218, 95% confidence interval [CI] = 1.253–3.925) and underweight status (AOR = 2.835, 95% CI = 1.151–6.982).
Conclusion
Childhood anemia is a moderate public health issue in the study area, with significant links to recent malaria infections, inadequate dietary diversity, and underweight status. Addressing these factors is essential for improving child health outcomes.
Introduction
Anemia is defined as a reduction in hemoglobin, hematocrit, or red blood cells below the normal range for age, sex, and race. According to the World Health Organization, children under five are anemic if their hemoglobin level is below 110 g/L, with severity categories for mild, moderate, and severe anemia. Globally, anemia remains a major public health issue, contributing to high morbidity and mortality in children. In 2019, 39.8% of children aged 6 to 59 months around 269 million were anemic (WHO, 2021), with the highest prevalence in Africa (60.2%) and in Ethiopia at 52.1% (Hailu et al., 2024). Although there has been a gradual global decline in childhood anemia since 2000, rates have remained stagnant since 2010. A hospital-based study in the Harari region (Eastern Ethiopia) found an anemia prevalence of 33% among under-five children, with 58.7% mild, 34.9%, moderate, and 6.4% severe cases (Gemechu et al., 2024).
Iron deficiency is estimated to cause about half of all anemia cases, particularly in low-income settings with poor dietary intake (Gedfie et al., 2022; WHO, 2021). Recent evidences show that in addition to iron deficiency, infections, genetic conditions, and micronutrient deficiencies (e.g., B12, folate, and vitamin A) are major contributors to anemia across populations (Armah-Ansah et al., 2023; WHO, 2025). The etiology of anemia is multifactorial, involving biological, nutritional, socioeconomic, and environmental factors (Aliyo & Jibril, 2022; Gebreweld et al., 2019; Kebede et al., 2021; Sahiledengle et al., 2024). Risk factors in Ethiopia include stunting, wasting (a low weight-for-height), low maternal education, poor dietary diversity, and limited prenatal care (Belachew & Tewabe, 2020; Orsango et al., 2021).
Anemia can be classified by a red blood cell size and color, and common types include iron deficiency, sickle cell, vitamin deficiency, and anemia of chronic disease (Kebede et al., 2021; Niss & Quinn, 2022). In children anemia impairs cognitive, physical, and immune development (Fentaw et al., 2023; Orsango et al., 2021). WHO guidelines recommend screening for palmar pallor and hemoglobin testing (Gebereselassie et al., 2020; WHO, 2021).
Despite many national studies, no prior research has found on anemia among children under five in Wolkite town in Gurage zone, an area with high malaria burden and limited diagnostic resources (Solomon et al., 2020). This study aims to assess the prevalence and associated factors of anemia among under-five children in Wolkite's public health facilities
Review of Literature
Anemia defined by low hemoglobin or red blood cell levels, is major global health issue affecting nearly 40% of children under five, with the higher prevalence in Africa (60.2%) and Ethiopia (52.1%) (Hailu et al., 2024; WHO, 2021). A hospital-based study in eastern Ethiopia in 2022 revealed that 33% of under-five children were anemic (Gemechu et al., 2024). Anemia commonly arise from nutrient deficiencies, genetic blood disorders, parasitic infections, and other acute or chronic illnesses. Risk factors include stunting, wasting, low maternal education, poor dietary diversity, and limited prenatal care (Belachew & Tewabe, 2020).
Anemia impairs children's cognitive and physical development and weakens immunity (Fentaw et al., 2023). WHO recommends screening using hemoglobin tests and clinical signs. Despite national data, no prior studies have assessed anemia in Wolkite town, a high-risk area with malaria and limited resources (Solomon et al., 2020).
Methods and Materials
Study Area and Period
A quantitative cross-sectional study was conducted from March 1 to 30, 2024, in Wolkite town, situated in the Gurage Zone of Central Ethiopia, approximately 159 km southwest of the capital, Addis Ababa. Wolkite serves as the capital of Gurage Zone, with an average annual temperature of 18.6°C and an average rainfall of 1,244 mm. The town is located at an elevation between 1,910 and 1,935 m above sea level. The Central Statistical Agency of Ethiopia reported data from the 2007 Census, and based on projections from City Population (2023), the population of Wolkite city is expected to reach 103,000 (City Population, 2023). The town is served by three government health facilities: one specialized hospital and two health centers. Wolkite Health Center, located in Bekur Sub-city, provides healthcare services to the local population and surrounding areas such as Kebena and Abeshge. Wolkite University Specialized and Referral Hospital, situated in Gubre Sub-city, is 172 km away and functions as a teaching hospital for medical and nursing students of Wolkite University. Established in 2019, the hospital offers a range of services, including medical, surgical, maternal and child health, and pediatric care.
Population
All children aged between 6 months and 59 months who attended care and treatment at Wolkite Health center and Wolkite University Specialized and Referral Hospital during the data collection period were included, and those under-five children who were treated with iron supplements and/or blood transfusion in the past 3 months were excluded.
Inclusion and Exclusion Criteria
All children aged 6 to 59 months who attended care and treatment at Wolkite Health Center and Wolkite University Specialized and Referral Hospital during the data collection period were included. Children who had received iron supplementation or a blood transfusion within the previous 3 months were excluded.
Sampling
The sample size was determined by using single population proportion formula with 95% confidence interval (CI), and 5% margin of error with prevalence of 52.2% from a study in Kombollcha (Fentaw et al., 2023).

Thus, adding 10% nonresponse rate, the final sample size was 421.
The participants in the study were chosen through a systematic random sampling technique. The first child was selected randomly using a lottery method, and subsequently, every 12th child was selected according to the sequence of their visits.
Data Collection Tool and Procedure
Data collection was conducted using a structured, interviewer-administered questionnaire adapted from existing literature (Aliyo & Jibril, 2022), the WHO guidelines for measuring dietary diversity and meal frequency, and the Food and Nutrition Technical Assistance (FANTA) guidelines for assessing household food insecurity (FANTA, 2007). The questionnaire was initially prepared in English, then translated into Amharic, and subsequently back-translated into English by language experts to ensure consistency. The instrument was pretested on 5% of the sample size at another health center in the city. The pretest demonstrated content validity with a score of 0.79. Data collection was performed by two trained nurses using face-to-face, interviewer-administered structured questionnaires. Prior to the interviews, participants were provided with a clear explanation of the study's purpose. To prevent double sampling of participants who were referred to the hospital, a marker was applied to their middle finger.
Blood Sample Collection
Blood samples were collected in strict adherence to the standard operating procedures (SOPs), with a 3 mL venous blood sample to determine the hemoglobin levels of the children, and no other laboratory tests other than hemoglobin were involved. Two experienced laboratory technicians were responsible for collecting the samples in tubes containing ethylenediaminetetraacetic acid (EDTA). The materials used for the blood collection included syringes with needles and EDTA-containing blood collection tubes. The procedure was conducted using strict aseptic techniques.
Anthropometric Measurement
Anthropometric assessments, including height-for-age, weight-for-height, and weight-for-age, were conducted following the WHO guidelines (World Health Organization, 2006). Each of the three measurements was expressed as standard deviation (SD) units in terms of Z-scores compared to the median of the WHO 2006 standard population.
Operational Definitions
Anemic: Under-five children with blood hemoglobin levels of <11 g/dL were declared anemic, and those under-five children with blood hemoglobin levels of ≥ 11 g/dL were not anemic (WHO, 2025).
Household Food Insecurity Assessment
Food and Nutrition Technical Assistance prepare questionnaire contain nine questions for the assessment of household food insecurity (Foodand NutritionTechnicalAssistance [FANTA], 2007). Children whose height-for-age Z-score ≤ 2 SD from the median of the reference population were considered Stunted, children whose weight-for-height Z-score
Data Analysis and Presentation
Data entry was performed using Epi-Data version 4.6 and subsequently exported to Statistical Package for the Social Sciences (SPSS) version 25 for analysis. Descriptive statistics were used to summarize the sociodemographic characteristics of the participants. A binary logistic regression model was employed to identify factors associated with anemia. Variables that showed a P-value of ≤ .25 in the bivariate analysis were considered candidates for inclusion in the multivariable analysis. Multivariable logistic regression was conducted to control for potential confounding factors and determine the true effects of the selected predictor variables. The strength of association between various factors and anemia was assessed using adjusted odds ratios (AOR) with 95% CI, with a P-value of ≤ .05 regarded as statistically significant.
Results
Sociodemographic Characteristics of Participants
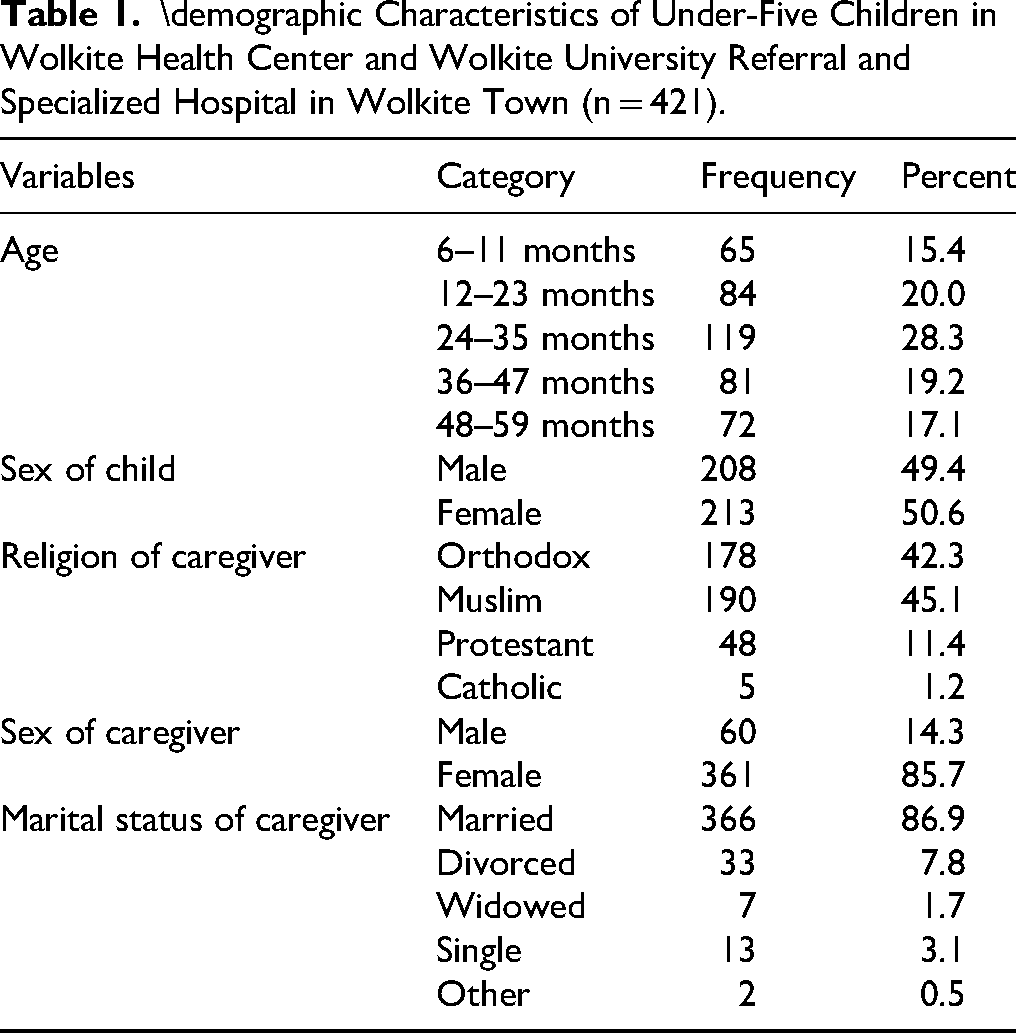
In this study 421 under-five children were enrolled. The participants’ ages ranged from 6 to 59 months, with a mean (SD) age of 30.21(±15.294) months. Among 421 children under the age of five, 213(50.6%) were female, and the majority 196 (46.6%) of children's mothers/caregivers were house wives. Three hundred and twenty-one (76.2%) had male household head, 366 (86.9%) were married and 361 (85.7%) of caregivers were female. More than half, 238(56.5%) were from urban areas. Approximately, 112 (26.6%) of children's caregivers had higher than high school education. Out of 421 children under the age of 5, approximately 190 (45.1%) were Muslims. One hundred and seventy-five (41.6%) were living in a household with four family members, and the majority of households, 360 (85.5%) had incomes greater than 1500 Ethiopian birr (Table 1).
\demographic Characteristics of Under-Five Children in Wolkite Health Center and Wolkite University Referral and Specialized Hospital in Wolkite Town (n = 421).
Child Feeding History
Among 421 under-five children, 311 (73.9%) had adequate dietary diversity practice, 266 (63.2%) introduction of complementary food less than or at 6 months, 243 (57.7%) mothers/caregivers have nutritional information, 315 (74.6%) had used animal products, 150 (35.6%) face mild food insecurity within 4 weeks, 392 (93.1%) had adequate meal frequency per day of their age, while majority 184 (43.7%) breastfeeding practice continued at 6 to 12 months (Table 2).
Child Feeding-Related Factors Among Under-Five Children in Wolkite Health Center and Wolkite University Referral and Specialized Hospital in Wolkite Town (n = 421).

Note. DD=dietary diversity; MF=meal frequency.
Birth History and Maternal Comorbid Condition
Of the 421 under-five children, 315 (74.8%) were delivered by spontaneous vaginal delivery (SVD), 233 (55.3%) had no history of maternal anemia, majority of the children, 364 (86.5%) had no history of birth asphyxia, and 410 (97.4%) took immunization of their age. Among 421 under-five children, 43 (10.2%) were underweight, 6(1.4%) stunted, and 5(1.2%) wasted.
Out of 421 under-five children enrolled in the study, 402 (95.5%) had no history of blood loss, 414 (98.3%) had no history of surgery, and 417 (99.0%) had no history of blood loss due to injuries. One hundred and eighty-seven (44.4%) had recent history of fever followed by recent history of diarrhea 164 (39.0%), and 88 (20.9%) had intestinal protozoa followed by malaria infection 74 (17.6%), 401 (95.2%) had no chronic disease and 15 (3.6%) soil-transmitted helminthic infection (Table 3).
Birth History and Maternal Comorbid Illness Among Under-Five Children in Wolkite Health Center and Wolkite University Referral and Specialized Hospital in Wolkite Town (n = 421).

Note. CS=caesarean section; SVD=spontaneous vaginal delivery.
Prevalence of Anemia
Based on the hemoglobin cutoff value, less than 11 g/dL was categorized as anemic, and Hgb values of 10 to 10.9, 7 to 9.9, and less than 7 g/dL were determined to be mild, moderate, and severe, respectively (WHO, 2021). The overall prevalence of anemia was 164 (39.0%; Figure 1). Among children with anemia under 5 years of age, 95 (22.6%) were mild, 58 (13.8%) moderate, and 11 (2.6%) severe. Children with anemia scores hemoglobin values of mild anemia = 10 to 10.9 g/dL, moderate anemia = 7 to 9.9 g/dL, and severe anemia = less than 7 g/dL (WHO, 2021; Figure 2).

The Anemia Among Under-Five Children Attended Wolkite Health Center and Wolkite University Referral and Specialized Hospital in Wolkite Town 2024.

Anemia Level Among Under-Five Children Attended Wolkite Health Center and Wolkite University Referral and specialized Hospital in Wolkite Town 2024.
Factor Associated With Anemia in Under-Five Children
In bivariate analysis, child sex, educational level of care giver, place of residence, monthly income of caregiver, dietary diversity practice, nutritional information, meal frequency, history of maternal anemia, recent history of fever, recent malaria infection, recent history of diarrhea, household food insecurity, and underweight had a P-value of <.25 and were considered candidates for multivariable analysis.
In multivariable analysis, the chance of having anemia was approximately seven times higher among children under the age of 5 who's sex was male (AOR = 7.252, 95% CI = 4.176–12.592) than being female. Additionally, children who had lived in rural areas had four times more likely to have anemia (AOR = 4.295, 95% CI = 2.499–7.382) than lived in urban areas. Under-five children with history of recent fever had two times higher chance to have anemia (AOR = 2.183, 95% CI = 1.203–3.960) than their counterparts. Similarly, the children who had recent malaria infection were four times more likely to have anemia (AOR = 4.387, 95% CI = 2.097–9.179) than those who did not have recent malaria infection. Additionally, children who had inadequate dietary diversity had two times more likely to have anemia (AOR = 2.218, 95% CI = 1.253–3.925) than children with adequate dietary diversity practice. Similarly, under-five children with underweight had nearly three times higher chance to have anemia (AOR = 2.835, 95% CI = 1.151–6.982; Table 4).
Factors Associated With Anemia in Among Under-Five Children in Wolkite Health Center and Wolkite University Referral and Specialized Hospital in Wolkite Town, Ethiopia.
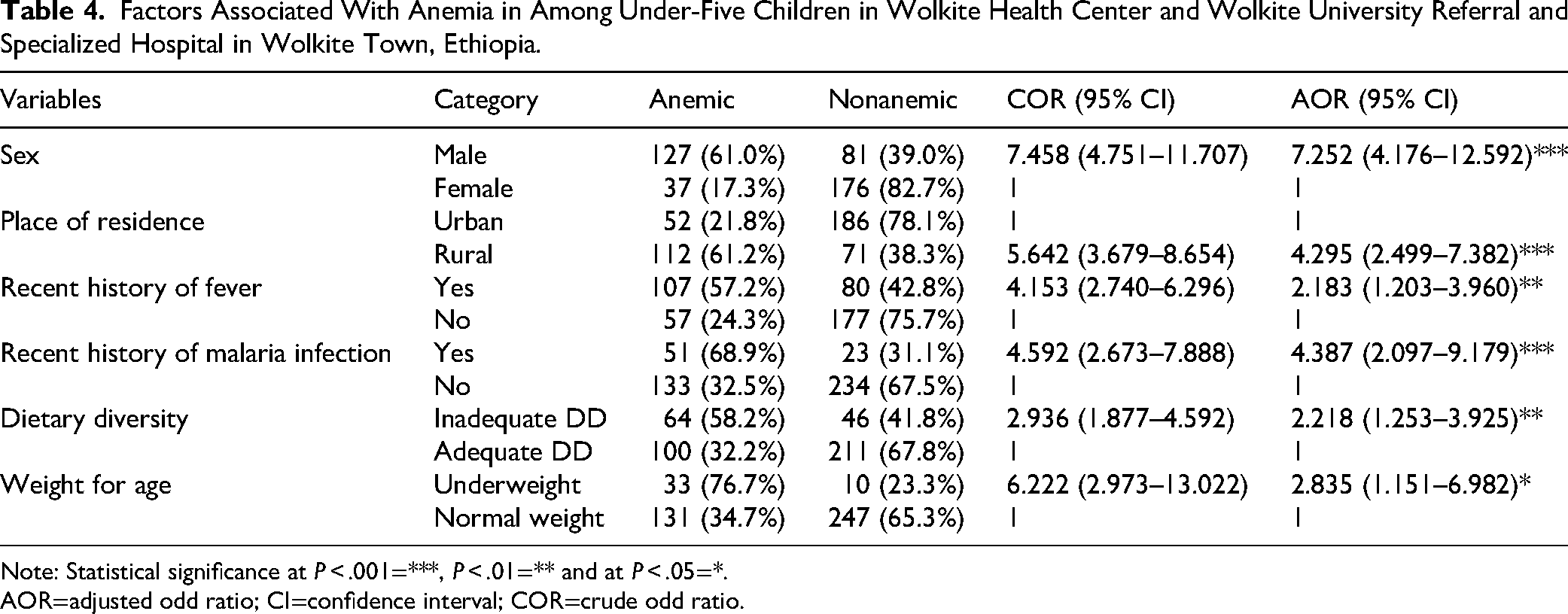
Note: Statistical significance at P < .001=***, P < .01=** and at P < .05=*.
AOR=adjusted odd ratio; CI=confidence interval; COR=crude odd ratio.
Discussion
The prevalence of anemia among children under five attending Wolkite health center and Wolkite University referral and specialized hospital was found to be 39.0%, which, according to WHO criteria, qualifies as a moderate public health concern (WHO, 2011). This finding is consistent with the global estimate reported by WHO in 2021 (39.8%), and similar to studies conducted in Northern Tamzania (37.9%; Mboya et al., 2020) and Guguftu, Northeast Ethiopia (41.1%; Gebreweld et al., 2019).
However, the prevalence observed in this study is lower than estimates from the WHO African region (60.2%) and Ethiopia nationally (52.1%; WHO, 2021), as well as data from the 2016 Ethiopian Demographic and Health Survey (EDHS) (57%). It is also lower than findings from South and Southeast Asia (57.2%; Sunuwar et al., 2023), Indonesia (76.1%; Randell et al., 2022), sub-Saharan Africa (64.1%; Tesema et al., 2021), and several Ethiopian countries. Variations in the prevalence may reflect differences in age groups studied, sample size, methodology, and regional context. For example, the Debre Brhan study included younger children (6–23 months), who are more vulnerable to anemia. Conversely, this study's prevalence was higher than in China (24.4%; Elmardi et al., 2020), Debre Markos (11.9%; Alamneh et al., 2021), Southern Ethiopia (32%; Orsango et al., 2021), and Bule Hora (13.2%; Aliyo & Jibril, 2022). These disparities may result from differences in hemoglobin cut-of-points, cultural practices, dietary patterns, and healthcare access.
Multivariable analysis revealed that male sex was significantly associated with anemia, consistent with findings from sub-Saharan Africa (65.3%; Tesema et al., 2021) and Nepal (45,65; Khanal et al., 2023). Due to faster growth, there is increase in their vulnerability. Despite son preference in some cultures, evidences suggest that girls are more likely to be neglected nutritionally (Dagne & Nigatu, 2019).
Rural residence was another significant factor, consistent with findings from china (32.8%) (Elmardi et al., 2020) and Ethiopian settings like Guguftu (49.5%) and Shaban Gibe (42.3%) (Gebreweld et al., 2019; Kebede et al., 2021). Limited healthcare access, poor sanitation, and low awareness about anemia ay contribute (Sahiledengle et al., 2024).
Children with a history of fever in the previous 2 weeks had higher anemia rates, aligning with studies from South and Southeast Asia (Sunuwar et al., 2023), sub-Saharan Africa (Tesema et al., 2021), and EDHS analysis (Asresie et al., 2020). Fever may signal infections like malaria or pneumonia. Which impair red blood cell production or increase destruction (Asresie et al., 2020). Recent malaria infection was also a significant factor, consistent with findings from Bule Hora (Aliyo & Jibril, 2022). Malaria contributes to anemia, with significant blood cell loss occurring after treatment and hemoglobin levels often dropping to their lowest between 3- and 7-day post-therapy (Chambrion et al., 2022).
Inadequate dietary diversity was significantly associated with anemia, as supported by studies in India (69.2%; Kathuria et al., 2023), Ghana (52.9%; Parbey et al., 2019), and other parts of Ethiopia. Poor diet leads to deficiencies in iron, folate, vitamin B12, and other nutrients vital for red blood cell production (Belachew & Tewabe, 2020).
Lastly, underweight status was linked to a higher anemia risk. Similar associations were found in Egypt (6.6%; Fouad et al., 2023), Ethiopia (50.2% in Guguftu, 62.4% in Debre Brhan; Gebreweld et al., 2019; Molla et al., 2020), and sub-Sharan Africa (Tesema et al., 2021). Malnutrition impairs nutrient absorption and weakens immunity, exacerbating malnutrition impairs nutrient absorption and weakens immunity, exacerbating anemia risk (Chambrion et al., 2022).
Strengths and Limitations
This study applied validated tools and WHO guidelines to assess anemia and its related factors, confirmed anemia through lab-based hemoglobin testing, and used multivariate regression to identify significant predictors, all while adhering to ethical standards. The findings offer valuable insights for targeted public health interventions. However, the study did not differentiate between the various classifications of anemia. Additionally, due to budget constraints, stool examinations for the assessment of protozoan and helminth infections could not be conducted. Another key limitation is that other blood parameters, such as serum ferritin and peripheral smear, were not assessed, limiting the ability to determine the specific cause and types of anemia
Implications for Nursing Practice
The study highlights key implications for nursing practice, emphasizing the need for early anemia screening, especially in high-risk group such as male children, those in rural areas, and those with recent infections or poor nutrition. Nurses should prioritize caregiver education on dietary diversity and iron-rich foods, conduct regular nutritional assessment, and support infection prevention efforts, particularly for malaria. Community outreach, timely referrals, and collaboration with other healthcare providers are also essential to effectively manage and reduce anemia in under-five children.
Conclusion
Childhood anemia represents a significant public health issue in the study area. Factors such as being male, living in rural areas, having a history of recent fever, recent malaria infection, inadequate dietary diversity, and underweight were found to be strongly associated with childhood anemia. To address this issue, it is recommended to implement effective preventive strategies, including the use of bed nets, timely diagnosis and treatment of malaria and other infections, and improving dietary diversity to reduce the risk of childhood anemia.
Footnotes
Abbreviations
Acknowledgements
The authors would like to express their deepest appreciation to participating hospital, data collectors, supervisors and the study participants for their kind invaluable contributions, without them this study wouldn’t be realized.
Ethical Consideration
Ethical approval for the study, including procedures involving blood sample collection was obtained from the College of Health Science, Addis Ababa University, Ethical Review Committee (Ref: CHS/NSG/008.017/24). Formal support letter was written to Wolkite Health center and Wolkite University Specialized Referral Hospital. Participants were informed about the study objectives prior to the data collection. Informed consent was obtained from participants parents/significant others. The study adhered to the principles outlined in the Declaration of Helsinki. Participation to the study was absolutely voluntary. Confidentiality of the data was ensured by anonymizing identifiers. And use of unique ID numbers. Anemic children were linked to the respective health center or hospital OPDs for care and treatment.
Consent for Publication
All authors in the list have read the manuscript and agreed for the publication of the article in the journal.
Authors’ Contributions
BM, AH, and NT were involved in the conceptualization. BM participated in the investigation; BM, AH, NT, and TG were involved in data curation, formal analysis, methodology, resources, project administration, original draft writing; and AH, TG, and NT were involved in supervision, validation, and visualization; TG and AH prepared the manuscript. All authors reviewed, read, and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed are available from the corresponding author on reasonable request.