
Abstract
Background
Burnout is a growing occupational health issue among nurses, particularly those working in emotionally demanding units such as oncology and hematology. In Palestine, limited resources, high workloads, and political instability further exacerbate this challenge. Shift work, a necessity in hospital settings, has been linked to disrupted sleep patterns, emotional exhaustion, and burnout. However, limited evidence exists on its specific impact among Palestinian oncology nurses.
Objective
To examine the association between shift work and burnout among oncology/hematology nurses in Palestinian hospitals, and to explore gender-specific differences.
Methods
This cross-sectional study included 214 registered nurses working in oncology/hematology units across public, private, and nongovernmental hospitals in the West Bank and Gaza. Data were collected using a validated Arabic version of the Maslach Burnout Inventory–Health Services Survey (MBI-HSS). Burnout was assessed across three dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment. Statistical analysis included t-tests, ANOVA, and multivariate linear regression.
Results
More than half of participants (57.2%) reported moderate levels of burnout. Emotional exhaustion was the most prevalent subscale (69.4%), followed by reduced personal accomplishment (53.3%) and depersonalization (45%). Shift workers demonstrated higher burnout scores, particularly among males. Younger age and fewer years of oncology experience were associated with greater burnout. Gender differences in subscale patterns were observed but not statistically significant.
Conclusion
Shift work contributes to increased burnout among Palestinian oncology nurses. Age and experience play moderating roles. Policy reforms are needed to address scheduling practices and improve mental health support for nursing staff.
Introduction
Burnout has emerged as a pervasive occupational health issue in nursing, characterized by emotional exhaustion, depersonalization, and diminished personal accomplishment (Maslach & Leiter, 2016). Globally, between 40% and 50% of nurses experience moderate to severe burnout, a phenomenon that undermines psychological well-being, patient safety, and the overall quality of healthcare delivery (Dall’Ora et al., 2020; Woo et al., 2020). Burnout among nurses leads to higher absenteeism, reduced work engagement, and increased turnover intentions, posing a significant challenge to the sustainability of health systems across both high- and low-income countries (Boamah & Laschinger, 2016; Reith, 2018).
Nurses working in oncology and hematology units are particularly vulnerable to burnout due to their continuous exposure to suffering, death, and ethical complexity. Caring for patients with life-threatening illnesses demands sustained emotional engagement, empathy, and psychological resilience (Barbosa et al., 2024; Lee et al., 2025). The cumulative exposure to terminal care, moral distress, and compassion fatigue increases emotional exhaustion and depersonalization (Gómez-Urquiza et al., 2021). In addition, high patient acuity, staffing shortages, and emotionally intense environments amplify professional strain, making oncology nurses among the most at-risk healthcare providers for burnout (Barbosa et al., 2024; Tuna & Baykal, 2014).
A substantial body of evidence has identified shift work as a key occupational determinant of burnout. Rotating, night, or extended shifts disrupt circadian rhythms, impair sleep quality, and induce chronic fatigue, which collectively diminish cognitive performance and emotional regulation (Booker et al., 2020; Tanaka et al., 2024). Recent integrative reviews indicate that nurses working irregular schedules exhibit significantly higher rates of emotional exhaustion and depersonalization compared with those on fixed day schedules (Alzahrani et al., 2025; Simons et al., 2024). These effects are particularly pronounced in high-intensity settings such as oncology, where emotional demands compound the physiological consequences of disrupted sleep and fatigue.
Within the Palestinian context, the risk of burnout is intensified by systemic and sociopolitical challenges. The Palestinian health sector faces chronic shortages of nursing staff, limited financial resources, overcrowded hospital wards, and ongoing political instability, all of which heighten psychological distress among healthcare workers (Abukhader et al., 2020; Hamdan & Hamra, 2017). Studies have reported that more than 60% of Palestinian nurses experience moderate to severe levels of emotional exhaustion, reflecting both occupational and contextual pressures (Hallaq & Jondi, 2017). Moreover, nurses working in oncology and hematology departments face additional emotional demands related to end-of-life care and resource scarcity, compounding the effects of shift work and institutional stressors (Jaradat & Qtait, 2025).
Sociodemographic variables such as age, gender, and professional experience further influence burnout patterns. Younger nurses tend to exhibit higher emotional exhaustion and depersonalization due to limited coping mechanisms and less professional resilience (Tuna & Baykal, 2014; Van Bogaert et al., 2009). Gendered expectations, especially in patriarchal and collectivist cultures, may increase burnout risk among women who shoulder both professional and domestic responsibilities (Hussein & Faraj, 2024; Rahman et al., 2024). Conversely, male nurses may adopt emotional detachment as a coping strategy, resulting in elevated depersonalization scores (Mudallal et al., 2017; Purvanova & Muros, 2010). Such gendered patterns are rarely examined in Middle Eastern contexts, where sociocultural dynamics profoundly shape professional stress experiences.
Despite growing international research, empirical data on burnout among Palestinian oncology and hematology nurses remain scarce. Their work context combines high emotional intensity, resource constraints, and sociopolitical adversity, creating a uniquely high-risk environment for psychological distress. Understanding how shift work interacts with demographic and professional variables to influence burnout within this context is essential for developing evidence-based interventions and workforce policies (Hammad & Qassas, 2025; Tannous & Daher, 2025).
Therefore, this study aims to examine the relationship between shift work and burnout among oncology and hematology nurses in Palestinian hospitals and to explore the moderating effects of age, gender, and professional experience. Addressing this gap will provide contextually grounded evidence to guide organizational reforms, promote nurse well-being, and improve the sustainability and quality of cancer care within Palestine's constrained healthcare system.
Review of Literature
Burnout among nurses is widely recognized as a major occupational health concern that adversely affects individuals, institutions, and healthcare outcomes. The World Health Organization has identified burnout as an occupational phenomenon arising from chronic workplace stress that has not been effectively managed. Globally, the prevalence of moderate to severe burnout among nurses exceeds 40%, with emotional exhaustion identified as the most prominent dimension (Dall’Ora et al., 2020; Woo et al., 2020). The COVID-19 pandemic further exacerbated these challenges by intensifying workload, moral distress, and emotional fatigue across clinical settings (Nguyen et al., 2024).
Nurses working in oncology and hematology departments are particularly vulnerable to burnout due to the sustained emotional labor required in caring for patients with life-threatening illnesses. Prolonged exposure to patient suffering, ethical dilemmas, and end-of-life care frequently results in compassion fatigue, moral distress, and diminished professional engagement (Barbosa et al., 2024; Gómez-Urquiza et al., 2021). Lee et al. (2025) reported that oncology nurses exhibit significantly higher levels of depersonalization and emotional exhaustion compared with those in general medical units, largely due to cumulative emotional strain and the need to balance empathy with professional detachment. These findings are consistent with earlier studies linking oncology nursing with high psychological burden and reduced personal accomplishment (Tuna & Baykal, 2014).
Shift work a defining characteristic of hospital-based nursing—is a well-documented occupational stressor. It encompasses rotating, evening, and night schedules that disrupt circadian rhythms, impair sleep quality, and trigger chronic fatigue (Tanaka et al., 2024). Physiological disturbances associated with disrupted sleep cycles have been shown to exacerbate cognitive fatigue and emotional instability, contributing to elevated burnout risk (Booker et al., 2020; Simons et al., 2024). A recent integrative review by Alzahrani et al. (2025) demonstrated that nurses working irregular or extended shifts exhibit significantly higher emotional exhaustion and depersonalization compared with those on fixed schedules. Similarly, Tanaka et al. (2024) emphasized that chronic circadian misalignment compromises psychological well-being and work performance. Collectively, these findings underscore the intricate interplay between biological, psychological, and organizational factors in the development of burnout among shift-working nurses.
Burnout experiences among nurses are also shaped by sociodemographic variables such as age, gender, and professional experience. Younger nurses tend to report higher emotional exhaustion and depersonalization due to lower resilience and fewer coping mechanisms (Tuna & Baykal, 2014; Van Bogaert et al., 2009). Gender differences have been consistently reported in the literature, with female nurses showing higher emotional exhaustion and male nurses exhibiting greater depersonalization (Hussein & Faraj, 2024; Purvanova & Muros, 2010). Rahman et al. (2024) found that women in patriarchal healthcare systems often experience dual burdens of professional and domestic responsibilities, intensifying emotional fatigue. Conversely, male nurses, particularly in female-dominated professions, may rely on emotional detachment as a coping strategy (Mudallal et al., 2017). These gendered coping mechanisms highlight the importance of culturally sensitive interventions tailored to diverse professional and social contexts.
In regions affected by conflict and resource scarcity, such as Palestine, burnout among nurses is further aggravated by systemic instability, occupational insecurity, and chronic under-resourcing. The Palestinian healthcare system faces persistent shortages of personnel and medical supplies, high patient-to-nurse ratios, and prolonged exposure to political and economic stressors (Abukhader et al., 2020; Hamdan & Hamra, 2017). Hallaq and Jondi (2017) reported that over 60% of nurses in Hebron's hospitals experience moderate to severe burnout, primarily driven by excessive workloads and emotional strain. Jaradat and Qtait (2025) similarly documented that occupational stress among Palestinian nurses is significantly associated with workload, shift rotation, and limited institutional support. Comparative studies from other conflict-affected countries, including Lebanon and Syria, reveal analogous patterns of psychological distress, emphasizing that organizational instability amplifies burnout risk (Hammad & Qassas, 2025; Tannous & Daher, 2025).
Despite the high prevalence of burnout, several organizational factors can buffer its effects. Supportive leadership, fair workload distribution, and access to mental health resources are repeatedly identified as protective factors that reduce emotional exhaustion and foster resilience (Chien et al., 2025; Mudallal et al., 2017). Alzahrani et al. (2025) emphasized that restorative scheduling practices and institutional recognition contribute to job satisfaction and reduce turnover intentions. Similarly, Qtait (2023) highlighted that transformational leadership and effective communication between head nurses and staff can mitigate burnout and improve nurse performance. These findings align with global recommendations from the World Health Organization and nursing bodies, advocating for organizational well-being strategies that prioritize staff mental health and sustainable scheduling policies.
Although burnout has been extensively studied globally, empirical research focusing on Palestinian oncology and hematology nurses remains limited. Most regional studies have examined general hospital nurses or intensive care units without disaggregating findings by specialty or shift type. Moreover, few studies have explored the interaction between shift work and demographic variables such as age, gender, and years of experience within politically unstable healthcare systems. Addressing these gaps is crucial for developing evidence-based interventions and policy reforms tailored to the Palestinian context.
The present study, therefore, investigates the relationship between shift work and burnout among oncology and hematology nurses in Palestinian hospitals, with attention to sociodemographic moderators. Understanding these associations will contribute to designing targeted strategies that enhance nurse well-being, improve retention, and strengthen the resilience of the Palestinian healthcare workforce.
Aim of the Study
This study aimed to examine the relationship between shift work and burnout among oncology and hematology nurses in Palestinian hospitals. It explored how age, gender, and professional experience influence burnout dimensions—emotional exhaustion, depersonalization, and reduced personal accomplishment. The findings provide evidence to guide interventions that enhance nurse well-being, job satisfaction, and patient care quality within the Palestinian healthcare system.
Methods
Study Design and Setting
This study employed a cross-sectional, descriptive-analytical design to examine the relationship between shift work and burnout among oncology and hematology nurses in Palestine. Data collection was conducted between January 2023 and May 2023 in government, nongovernmental, and private hospitals located in both the West Bank and the Gaza Strip.
Research Question
“What is the relationship between shift work and burnout among oncology and hematology nurses in Palestinian hospitals, and how do demographic factors such as age, gender, and professional experience influence this relationship?”
Study Population and Sampling
The target population consisted of registered nurses employed in oncology and hematology departments across Palestinian hospitals. Inclusion criteria were (1) having at least one year of clinical experience
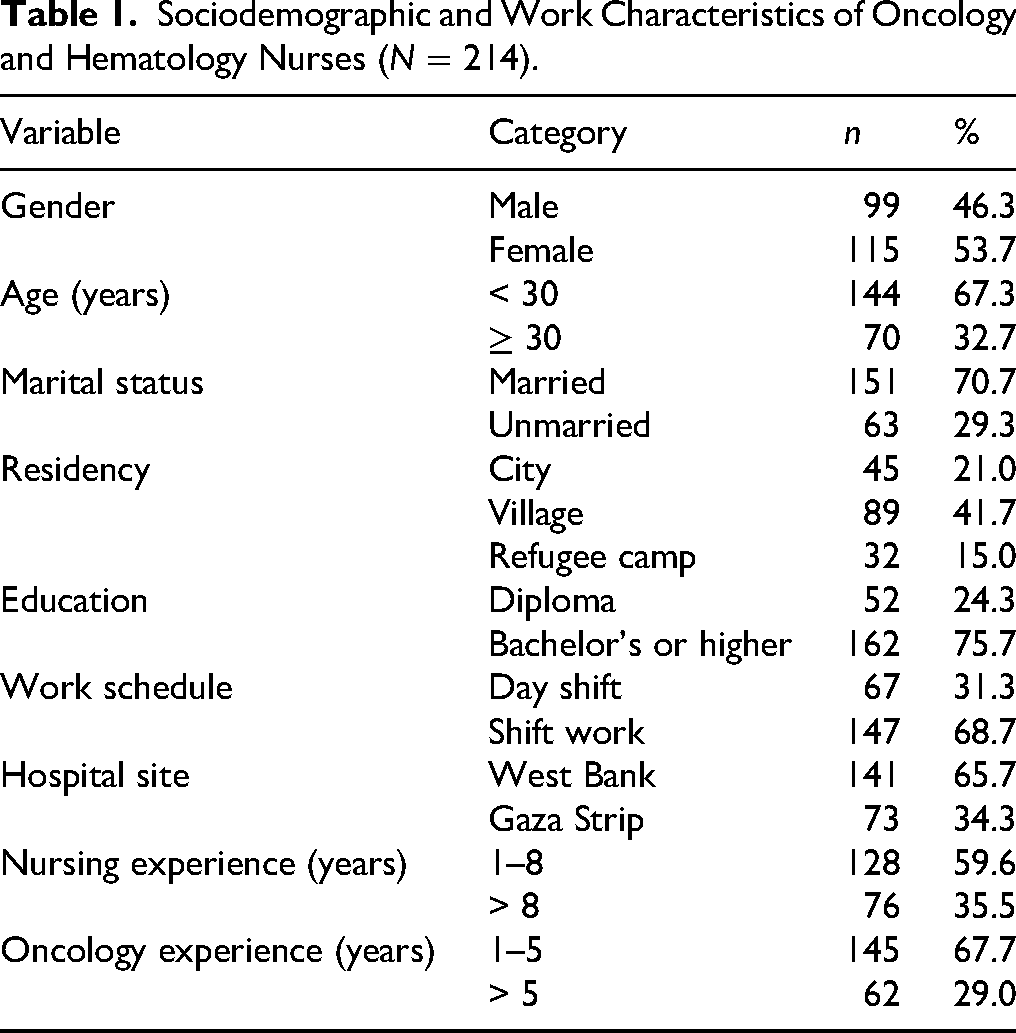
The final sample included 115 females (53.7%) and 99 males (46.3%), aged between 21 and 55 years (mean age: 30.8 years, SD: 8.1). Among them, 68.7% were shift workers and 31.3% worked regular day shifts. Participants represented a range of geographical backgrounds (urban 45.3%, rural 39.7%, and refugee camps 15%) and educational levels (24.3% diploma, 75.7% bachelor's degree or higher). Additionally, 35.5% had more than 8 years of general nursing experience, and 29% had more than 5 years of oncology/hematology-specific experience.
Instrumentation
Data were collected using a structured, self-administered questionnaire consisting of three major sections: sociodemographic and occupational characteristics, work schedule, and burnout assessment.
Sociodemographic and Occupational Characteristics: This section captured participants’ demographic data and work-related variables, including age, gender, marital status, place of residence, educational level, hospital type, years of total nursing experience, years of oncology/hematology-specific experience, and employment status. These variables were used to explore associations between personal and professional characteristics and burnout levels. Work Schedule: Participants were asked to identify their current work pattern, categorized as either day shift or shift work. The shift work category included rotating (day–evening–night) and fixed night shifts, in accordance with definitions provided by the International Labour Organization (ILO, 2019). This classification enabled analysis of the relationship between nonstandard work hours and burnout outcomes. Burnout Assessment: Burnout was assessed using the Maslach Burnout Inventory–Human Services Survey (MBI-HSS), developed by Maslach and Jackson (1981) and widely used to measure occupational burnout among healthcare professionals. The instrument includes 22 items across three subscales:
Emotional Exhaustion (EE)—9 items reflecting feelings of being emotionally overextended by one's work. Depersonalization (DP)—5 items assessing impersonal or detached responses toward patients. Personal Accomplishment (PA)—8 items evaluating perceived competence and successful achievement at work.
Each item was rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), with higher scores indicating greater levels of the respective construct. Negatively worded items were reverse-scored to ensure consistency.
Following established scoring conventions (Maslach & Jackson, 1981; Maslach et al., 2016), subscale totals were interpreted as follows:
Emotional Exhaustion: Low (<19), Moderate (19–26), and High (>26). Depersonalization: Low (<6), Moderate (6–9), and High (>9). Personal Accomplishment: Low (< 34), Moderate (34–39), and High (> 39).
Overall burnout levels were also categorized according to standardized guidelines:
Low burnout: total score < 33. Moderate burnout: total score 34–66. High burnout: total score ≥ 67 (Maslach & Jackson, 1981; Schaufeli et al., 2019).
In this study, the mean total burnout score of 54.4 (SD = 7.2) corresponded to moderate burnout, aligning with prior international findings among oncology nurses (Gómez-Urquiza et al., 2021; Lee et al., 2025).
Translation and Validation: The original English version of the MBI-HSS was translated into Arabic using a rigorous forward–backward translation procedure performed by bilingual nursing researchers. Content validity was reviewed by an expert panel of five nurse educators specializing in oncology and psychometrics. A pilot study with 20 oncology nurses was conducted to test clarity, cultural relevance, and internal consistency.
The Arabic version demonstrated strong reliability and construct validity:
Overall scale: Cronbach's α = .88. Emotional Exhaustion: α = .87. Depersonalization: α = .80. Personal Accomplishment: α = .79.
Exploratory factor analysis (EFA) confirmed the expected three-factor structure, with factor loadings exceeding 0.55 for all items, consistent with previous validations in Middle Eastern nursing populations (Abukhader et al., 2020; Mudallal et al., 2017).
Data Collection Procedure
The research team distributed printed copies of the Arabic and English versions of the questionnaire to the participants during working hours. Written informed consent was obtained prior to participation. Nurses were given one week to complete and return the anonymous questionnaires, which were placed in sealed envelopes and returned to a secure collection box. Hospital administrators were informed of the study in advance and facilitated the distribution process.
Ethical Considerations
Ethical approval for this study was obtained from the Research and Ethics Committee at Al-Quds University (Ref. No. 07/2023). Additional administrative permissions were secured from the Palestinian Ministry of Health and from relevant nongovernmental and private healthcare institutions. All participants received clear and comprehensive information about the purpose and procedures of the study, and informed written consent was obtained prior to data collection. Participation was entirely voluntary, with assurances that individuals could withdraw at any stage without penalty.
Confidentiality and anonymity were rigorously maintained; datasets were coded using numerical identifiers, and no personal information was recorded or disclosed. All electronic files were stored in secure, password-protected systems accessible only to the research team. The study adhered to the ethical principles of the Declaration of Helsinki, ensuring respect for autonomy, beneficence, nonmaleficence, and justice throughout the research process.
Statistical Analysis
Data analysis was performed using STATA version 10. Normality of continuous variables was assessed using kernel density plots. Descriptive statistics (means, standard deviations, frequencies, and percentages) were calculated for all demographic and professional variables.
Group differences in burnout levels were examined using t-tests and ANOVA. To investigate the associations between shift work and burnout, linear regression analyses were conducted. Three sets of models were estimated:
Crude (unadjusted). Adjusted for age and years of oncology experience. Stratified by gender.
Burnout scores and subscale scores (emotional exhaustion, depersonalization, and reduced personal accomplishment) were treated as continuous dependent variables. Results were reported as β coefficients with 95% confidence intervals (CIs). Statistical significance was set at p
Result
Sample Characteristics
Table 1 shows that most participants were female (53.7%), under 30 years old (67.3%), and married (70.7%). The majority held a bachelor's degree (75.7%) and worked rotating or night shifts (68.7%). Overall, the sample represented a young, well-educated, and moderately experienced nursing workforce across Palestinian hospitals.
Sociodemographic and Work Characteristics of Oncology and Hematology Nurses (N = 214).
Burnout Levels by Demographic and Occupational Variables
The overall mean burnout score was 54.4 (SD = 7.2), reflecting moderate burnout among oncology and hematology nurses. Subscale scores were Emotional Exhaustion (M = 24.4, SD = 5.8), Depersonalization (M = 11.3, SD = 3.1), and Reduced Personal Accomplishment (M = 18.7, SD = 4.2).
As presented in Table 2, a clear pattern emerged linking shift work and burnout dimensions among Palestinian oncology and hematology nurses. Nurses engaged in rotating or night shifts demonstrated significantly higher overall burnout scores (p = .03) and depersonalization levels (p < .01) compared with their counterparts working fixed day schedules. These findings suggest that irregular work hours may intensify emotional fatigue and emotional detachment, likely due to disrupted sleep cycles and limited recovery time between shifts.
Burnout Scores by Gender, Work Schedule, Age, and Oncology Experience.

Age also exhibited a meaningful influence on burnout. Younger nurses (< 30 years) reported significantly higher overall burnout and lower personal accomplishment (p = .02) compared with older nurses. This pattern indicates that early career professionals may possess less-developed coping strategies and professional resilience when confronted with the emotional and cognitive demands of oncology care.
A similar trend was observed regarding professional experience. Nurses with five or fewer years of oncology experience reported greater depersonalization and emotional exhaustion (p = .03), underscoring the cumulative protective effect of clinical exposure and professional maturity against burnout.
Regarding gender, male nurses exhibited higher depersonalization scores (p = .003), reflecting a greater tendency toward emotional withdrawal or cynicism, although their overall burnout scores did not differ significantly from those of female nurses. This finding aligns with prior research indicating that male nurses often display depersonalization as a coping mechanism to manage stress in emotionally demanding specialties.
The Cohen's d values ranging from 0.24 to 0.45 indicate small to moderate effect sizes, suggesting that while the observed group differences are not large in magnitude, they are both statistically and practically meaningful within the clinical and organizational context of nursing practice. Collectively, these results emphasize that shift work, limited experience, and younger age substantially contribute to burnout vulnerability among Palestinian oncology and hematology nurses, with nuanced gender-based variations in coping patterns.
The study revealed moderate levels of burnout among oncology and hematology nurses in Palestinian hospitals, with emotional exhaustion and depersonalization as the most prominent dimensions. Results from Table 2 demonstrated that shift work was significantly associated with higher overall burnout and depersonalization, indicating that irregular or night schedules contribute to emotional strain and reduced engagement. Younger nurses (<30 years) and those with ≤ 5 years of oncology experience exhibited greater vulnerability to burnout, reflecting limited coping capacity and professional resilience. Male nurses reported higher depersonalization, suggesting gendered differences in emotional regulation and coping strategies.
The regression analyses in Table 3 further showed that, after adjusting for age and experience, shift work remained a positive but nonsignificant predictor of total burnout. However, depersonalization was strongly influenced by both shift work and younger age, explaining 15% of the variance (R² = .15). The overall model fit statistics (R² = .08–.15) indicated moderate explanatory power, implying that other organizational factors—such as workload, staffing ratios, and managerial support—also contribute meaningfully to burnout risk.
Crude and Adjusted Regression Models Predicting Burnout Dimensions (N = 214).

Effect sizes ranging from Cohen's d = 0.24–0.45 and η² = .06–.11 confirmed small-to-moderate practical significance, signifying that these effects, while not large, hold substantial clinical and managerial implications. Collectively, the findings highlight the need for context-sensitive interventions that address shift scheduling, enhance mentorship for younger nurses, and provide psychological and organizational support to mitigate burnout within the Palestinian oncology nursing workforce.
Discussion
This study examined the association between shift work and burnout among oncology and hematology nurses in Palestinian hospitals, with a focus on gender and sociodemographic differences. The findings revealed that more than half of the nurses (57.2%) experienced moderate levels of burnout, with high prevalence rates of emotional exhaustion (69.4%), reduced personal accomplishment (53.3%), and depersonalization (45%). These outcomes are consistent with international trends indicating that nurses in emotionally demanding specialties, such as oncology, frequently encounter high levels of emotional exhaustion due to prolonged exposure to critically ill patients and the emotional challenges of end-of-life care (Barbosa et al., 2024; Lee et al., 2025).
Shift work was positively associated with increased burnout scores, particularly among male nurses. Although the association did not remain statistically significant after adjustment, this pattern aligns with mounting evidence suggesting that rotating and night shifts exacerbate psychological stress, disrupt circadian rhythms, and impair emotional regulation—factors that cumulatively contribute to burnout (Qtait, 2025; Simons et al., 2024; Tanaka et al., 2024). The physiological and cognitive consequences of shift work are well documented, especially among nurses under 40 years of age who may simultaneously navigate professional development and family responsibilities (Alzahrani et al., 2025).
While female nurses in this study demonstrated slightly higher burnout scores during shift work, the interaction between gender and shift type was not statistically significant. This aligns with regional evidence indicating that women often experience greater emotional exhaustion due to social and familial expectations, whereas male nurses tend to exhibit higher depersonalization and diminished professional fulfillment (Hussein & Faraj, 2024; Rahman et al., 2024). These gender-related disparities emphasize the need for tailored mental health interventions that account for the sociocultural norms shaping nurses’ experiences in Middle Eastern healthcare settings.
Age and professional experience were also influential in determining burnout severity. Younger nurses and those with limited professional experience reported higher emotional exhaustion and depersonalization levels. Similar findings have been reported internationally, where early career nurses often lack the coping strategies and emotional resilience needed to manage the psychological demands of oncology care (Di Muzio et al., 2019; Jaradat & Qtait, 2025; Nguyen et al., 2024). In contrast, senior nurses generally benefit from accumulated clinical experience and greater emotional adaptability, which can buffer against fatigue and compassion strain.
One notable finding of this study was the association between depersonalization and shift work among younger nurses. Depersonalization, a form of emotional withdrawal, poses particular challenges in oncology settings, where empathy and compassion are essential for high-quality, patient-centered care. Evidence from conflict-affected regions indicates that depersonalization may function as a self-protective response to chronic exposure to trauma, yet it undermines care quality and professional engagement (Chirico & Magnavita, 2021; Tannous & Daher, 2025).
Although personal accomplishment scores were not significantly influenced by shift type or gender, lower scores were observed among night-shift workers. This pattern corresponds with the findings of Chien et al. (2025), who reported that night-shift nurses often face reduced peer interaction, limited supervisory feedback, and fewer opportunities for recognition—factors that diminish professional efficacy and job satisfaction.
From a public health perspective, these findings highlight the urgent need for organizational strategies to reduce burnout among oncology and hematology nurses, particularly within low-resource and politically unstable environments such as Palestine. Recommended measures include optimizing shift rotations, offering structured psychological support, promoting mentorship for novice nurses, and establishing recognition programs to reinforce professional fulfillment (Alzahrani et al., 2025; Barbosa et al., 2024; Qtait et al., 2025).
Given the chronic instability of the Palestinian healthcare system—exacerbated by occupation, economic hardship, and staffing shortages—such interventions must be contextually feasible and culturally sensitive. As Jaradat and Qtait (2025) asserted, burnout interventions should address both individual and systemic stressors, including sociopolitical trauma and limited institutional capacity. Enhancing nurses’ well-being under these conditions is essential not only for workforce retention but also for maintaining the quality and continuity of oncology care in a fragile health system.
While this study contributes valuable evidence to an underexplored area, its cross-sectional design precludes causal inference. The reliance on self-reported measures may also introduce response bias. Nevertheless, the high response rate, the use of a validated instrument, and rigorous statistical analyses strengthen the internal validity of the findings. Future research employing longitudinal and interventional designs is warranted to confirm these relationships and develop effective, evidence-based strategies to mitigate burnout among Palestinian oncology and hematology nurses.
Strengths and Limitations
This study's strengths include its focus on an understudied, high-risk group—oncology and hematology nurses in Palestinian hospitals—and its use of validated burnout measures across multiple regions, enhancing generalizability. Robust statistical analyses, including regression and effect size estimation, strengthened result validity. However, its cross-sectional design limits causal inference, and reliance on self-reported data may introduce bias. Unmeasured factors such as leadership style and staffing levels could also affect burnout. Despite these limitations, the study provides valuable, context-specific evidence to guide strategies that reduce burnout and improve nurse well-being within resource-limited and high-stress healthcare environments.
Implications of the Study
This study underscores the urgent need for systemic and organizational interventions to mitigate burnout among oncology and hematology nurses in Palestinian hospitals. The findings highlight that shift work, younger age, and limited professional experience significantly contribute to emotional exhaustion and depersonalization, while supportive leadership and structured mentorship could serve as protective factors. To address these challenges, hospitals should implement evidence-based scheduling reforms, regular burnout screening, and resilience-building programs tailored to early career nurses. Gender-sensitive psychological support is also recommended to address differing coping mechanisms. At the policy level, integrating workforce well-being into national health strategies and aligning with WHO's Global Strategic Directions for Nursing and Midwifery (2021–2025) are essential. Ultimately, improving nurses’ mental health and working conditions will enhance job satisfaction, retention, and patient care quality, reinforcing the sustainability and resilience of the Palestinian healthcare system in resource-limited and high-stress environments.
Conclusion
This study underscores the link between shift work and burnout in Palestinian oncology/hematology nurses, revealing nuanced gender differences and emphasizing the vulnerability of younger and less experienced staff. These findings echo global concerns and reinforce the need for targeted organizational and policy-level interventions to support nurse well-being and patient care outcomes in resource-constrained healthcare environments.
Supplemental Material
sj-docx-1-son-10.1177_23779608251406676 - Supplemental material for Shift Work and Burnout Among Oncology and Hematology Nurses in Palestinian Hospitals
Supplemental material, sj-docx-1-son-10.1177_23779608251406676 for Shift Work and Burnout Among Oncology and Hematology Nurses in Palestinian Hospitals by Bilal Jawabreh, Yousef Jaradat, Mohammad Qtait and Salam Al Khatib in SAGE Open Nursing
Footnotes
Acknowledgments
We sincerely thank the participating nurses, hospital administrations, and academic colleagues whose support, cooperation, and guidance contributed significantly to the completion of this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.