
Abstract
Introduction
Shift workers follow nonstandard schedules that encompass overnight duty, rotational timetables, or permanent night work which can lead to misaligned core circadian physiology. Shift work has been associated with sleep deprivation, burnout, and metabolic syndrome among healthcare workers.
Objective
We aimed to examine if shift nurses working in Malaysian public hospitals are more predisposed to burnout and to determine the predictors of burnout in this profession.
Method
This national-level cross-sectional study was conducted among nurses in public hospitals in Malaysia between July and November 2019 using self-administered questionnaires. Maslach Burnout Inventory-Human Service Survey was used to determine burnout. Multistage stratified sampling was used to recruit nurses from 32 hospitals. A complex sampling analysis was performed.
Results
Among the 1,491 hospital nurses, more than half (70.8%) of them followed shift work schedules. Shift nurses were mostly below 40 years old (80.9%), diploma holders (87.2%), and of lower professional grades (64.2%). The prevalence of overall burnout, as well as the domains of emotional exhaustion and depersonalization, was higher among shift nurses (27.1%) as compared to their counterparts (22.4%). Nurses who performed more than six night shifts per month were 2.6 times more predisposed to burnout.
Conclusion
Shift work is integral to ensure round-the-clock nursing care for patients. However, nurses are increasingly faced with more shift duties due to heavy patient loads and staff shortages. Modified work schedules must be implemented to provide sufficient rest time for shift nurses to mitigate burnout. Additionally, proper human resource projection and distribution are imperative to prevent worsening burnout.
Introduction
Burnout is defined in ICD-11 as an occupational-related syndrome resulting from chronic workplace stress that has not been successfully managed. It is characterized by three dimensions, that is, emotional exhaustion (EE): feelings of energy depletion or exhaustion; depersonalization (DP): increased mental distance from one's job or feelings of negativism or cynicism related to one's job; and lack of personal accomplishment (PA): reduced professional efficacy (Maslach et al., 2001). Certain professions are more vulnerable to burnout than others, such as those in the fields of education and health care (Salyers et al., 2017). For both professions, the pressure of deadlines, lack of job clarity, unsupportive superiors, and poor working environment are often the predisposing factors of burnout (Kader et al., 2021a).
In recent decades, healthcare systems have experienced significant changes, leading to more complex and intense patient care. Patients in hospitals today have more severe medical conditions, and healthcare workers (HCWs) often work long hours and face high workloads, juggling multiple responsibilities to manage patient care with greater precision and expertise. In addition, they have to deal with additional stressors such as exposure to death and dying, demanding patients and family members, long working hours, and shift work, making them highly susceptible to burnout (Dall'Ora et al., 2020). As the major backbone of healthcare service providers, nurses are not spared the same burnout epidemic since they constitute one of the biggest groups of HCWs (Boniol et al., 2022). As a result, prolonged exposure to workplace stress or frustration can subsequently manifest as a depletion of physical and emotional strength, leading to burnout.
Burnout among nurses has far-reaching and negative effects. They frequently experience decreased job satisfaction, higher absenteeism, as well as increased resignation and turnover rates (Dyrbye et al., 2019; Labrague et al., 2020). Furthermore, burnout can impact patient outcomes negatively because physically exhausted and emotionally depleted nurses may have reduced attention-to-detail and decision-making abilities, potentially leading to medical errors, reduced quality of patient care, and ultimately compromising the efficacy of healthcare services (Tawfik et al., 2019). On a systemic level, many healthcare systems suffer from nursing staffing shortages due to budget constraints or inadequate workforce planning. High patient-to-nurse ratios can worsen the workload and stress for individual nurses, increasing their vulnerability to burnout. High burnout rates further contribute to nurse turnover, creating a vicious cycle that further exacerbates staffing challenges. Consequently, burnout-related absenteeism and turnover among nurses result in substantial healthcare costs for organizations (Muir et al., 2022). In view of the detrimental individual and organizational impacts of burnout, it is imperative to identify the at-risk group of nurses and the associated risk factors of burnout to ensure a conducive working environment.
Review of Literature
In the clinical setting, shift work is integral to ensure round-the-clock nursing care for patients. Therefore, nurses are commonly subjected to nonstandard working schedules that encompass on-call/overnight duty, rotational timetables, or permanent night work that can lead to misaligned core circadian physiology (Dall'Ora & Dahlgren, 2020). The negative impact of shift work among nurses has been widely reported, encompassing physical (interruption of the circadian rhythm and sleep quality, fatigue, as well as gastrointestinal, neuropsychological, cardiovascular, and musculoskeletal disorders), mental (DP, cynicism, aggression, and frustration), and social (deterioration of family relationships and social life) dimensions (Ferri et al., 2016; Giorgi et al., 2018). Apart from affecting the health and well-being of individual staff, burnout can also result in suboptimal healthcare delivery performance and efficiency. In a recent systematic review, moderate to high levels of burnout were associated with medical errors and compromised patient safety (Hall et al., 2016). Even though many studies have been published on burnout among nurses, it remains an important topic in health care research due to the evolving clinical demands and changing landscape in health human resources.
Approximately 15%–33% of the global workforce is involved in shift schedules, whereby the prevalence is likely to be higher among healthcare staff in view of the nature of clinical care (Brown et al., 2020). In many countries, nurses are facing more shift duties because of heavy patient load and staff shortages. Therefore, the prevalence of burnout among nurses is likely to be higher. For instance, high-risk nurses with shift work disorders were at a much higher risk of mental health problems and burnout in China (Cheng et al., 2023). To date, very few studies have been conducted in low- and middle-income countries on this issue. The association between shift work and burnout may differ in different countries given the underlying healthcare structure, work contexts, and social environments.
Therefore, we aim to assess if shift-working nurses are more predisposed to burnout compared to their counterparts. By analyzing the association between shift work and burnout, we also set out to identify the predisposing factors of burnout among nurses working in public hospitals in Malaysia. These findings will be beneficial for the stakeholders to implement the necessary steps to mitigate burnout and its impact on shift-working nurses.
Method
Design
This was part of a national-level cross-sectional study that evaluated the level of burnout among hospital and primary care nurses in the Ministry of Health (MOH) Malaysia (Zakaria et al., 2022). The results are reported based on the “Strengthening of the Reporting of Observational Studies in Epidemiology” statement.
Research Questions
What is the prevalence of burnout among shift-working nurses?
Is there any difference in the prevalence of burnout between shift-working nurses and their non-shift-working counterparts?
Among the factors associated with burnout, what are the significant predictors of burnout among shift-working nurses?
Sample
The sample size calculation was based on a 27.3% estimated prevalence of burnout in a previous local study of burnout (Siau et al., 2018), a design effect of 2.5, and a nonresponse rate of 20%. The minimum sample size required from all the hospitals was 953.
The required sample size was calculated according to the following formula.

z = confidence level at 95% (standard value of 1.96)
p = estimated prevalence of burnout (27.3%; Siau et al., 2018)
d = margin of error at 5% (standard value of 0.05)

n = 305.2 ∼ 305
To ensure optimum sample size, a few adjustments were made:
Adjusted for the design effect (deff) of 2.5 N (complex) = n × deff Adjusted the n, taking into account an expected 20% nonresponse rate n (adjusted) = n × deff × (1 − nonresponse rate) The sample size was then adjusted according to the analysis based on hospital and primary care settings, and the proportion of nurses in both places. Considering two strata (hospital and primary care), the final sample size was multiplied by 2. Taking the proportion of nurses working in hospital and primary care as 82% to 18% based on the data from the Malaysian Nursing Board, the sample size required for hospital nurses was calculated as below:




Upon calculation of the final sample size, complex sampling was applied to obtain a nationally representative population of nurses. To recruit the participants, two-stage stratified cluster sampling was performed, beginning with the random selection of one state from each of the six zones (Northern, Central, Eastern, Southern, Sabah, and Sarawak) of Malaysia. Next, based on the population of nurses in each of the selected states, a total of 32 hospitals were proportionately selected from the six states. More hospitals would be included from states that recorded a higher number of nurses to contribute to the final sample size of nurses in this study. The selection of hospitals in each state was performed using computer-generated simple random sampling sequence. In the last stage, the participants were chosen randomly from a list of nurses provided by the liaison officers at the hospitals. Nursing matrons or sisters from the respective hospitals were appointed as liaison officers.
Inclusion/Exclusion Criteria
All nurses working in the 32 hospitals were included. However, the liaison officers were reminded to exclude any nurses with conditions requiring formal psychiatric follow-up from the list. This group of nurses may have a lower threshold toward the precipitating factors of burnout because of their underlying psychiatric conditions. Furthermore, they might also be given light duties or put on sick leave, thus affecting their perception and answers toward certain items in the study instrument. Similarly, nurses who were absent from work for more than three months were also excluded because their responses to the questionnaire items might not be reflective of their most recent experience at work. In this study, nonshift nurses referred to those who followed the standard office hour schedule (8.00 a.m. to 5.00 p.m.). In contrast, shift nurses included those who worked on a rotational work schedule that combined day, evening, and/ or night shifts.
Data Collection Process
Data collection was performed between July and November 2019. All selected nurses were invited to the face-to-face data collection session. They were briefed about the study objectives and assured that strict confidentiality would be upheld by not using any personal identifier in the questionnaire. A written informed consent was attached to the questionnaire and all participation would be voluntary. Those who agreed to participate were asked to complete the questionnaires before returning them during the same session.
Study Instrument
A dual-language questionnaire in English and Malay was prepared to extract the participants’ sociodemographic and professional information including age, gender, marital status, number of children, household income, and sleeping hours. Professional characteristics surveyed included education level, years of service, professional grades, types and frequency of shift words, and experience of traumatic events at work. Traumatic events were defined as any previous exposure to harassment/aggression/life-threatening event/litigation/medical error/mass disaster at the workplace based on a relevant publication (Morganstein et al., 2017). In addition, the participants were asked to fill in the average hours of daily sleep duration in the past month. Sleep deprivation was defined as having less than 6 hr of sleep per day in this study based on the National Sleep Foundation consensus report (Cirelli et al., 2017).
As for burnout, the Maslach Burnout Inventory for Human Services (MBI-HSS) was adopted. It comprised 22 items to be rated on a 7-point Likert scale from 0 (never), 1 (few times a year), 2 (once a month), 3 (a few times a month), 4 (once a week), 5 (a few times a week), to 6 (every day). The Malay version of MBI-HSS shares the same cutoff scores for the total values of the three domains as the original version, that is, > 27, > 13, and <32 for EE, DP, and PA, respectively. For this research, burnout is defined as having EE and/ or DP (Maslach et al., 1997). The Malay version of MBI-HSS reported a good internal consistency with Cronbach's alpha value of 0.803, thus suitable to be applied in Malaysia (Chen et al., 2014).
Statistical Analysis
Following data cleaning, data analysis was performed using complex sampling analysis procedures in Statistical Package for the Social Science (SPSS V.22). The prevalence of burnout was determined using sample weights and reported as numbers and percentages. Sample weightage was necessary in this case so that unbiased estimates could be obtained as not all nurses in the population would have the same probability of being selected. The odds ratios (ORs) and 95% confidence intervals (CIs) of all categorical variables were calculated to determine the associated factors of burnout among shift nurses. Significant factors with a p-value < .25 (Bursac et al., 2008; Ughade, 2013) at the univariate level were entered into the multivariate logistic regression to identify independent predictors of burnout.
Ethical Statement
This study involved human participants and was approved by the Medical Research and Ethics Committee of the MOH Malaysia, NMRR-18-3590-45274 (IIR). Permission was also obtained from the hospital directors of the involved study sites before data collection. Written informed consent was sought from each participating nurse at the beginning of the study before they answered the questionnaire.
Results
Sample Characteristics
A total of 1,491 hospital nurses were included in the final analysis after data cleaning. More than half of them (n = 1,056, 70.8%) were involved in shift work schedules. Tables 1 and 2 show the comparison of the baseline characteristics between shift nurses and nonshift nurses. There were significant differences in the sociodemographic and professional characteristics of the two groups of nurses. The majority of the hospital nurses were married with at least one child. In terms of age, there was a bigger proportion of shift nurses in the younger age groups (< 40 years old) whereas more than half (60.5%) of the nonshift nurses were more than 40 years old. For both groups of nurses, the majority of them were diploma holders and of M40 household income. In addition, more than half of the respondents (51.9%) had a diploma and had worked for more than 10 years (55.3%). Among the nonshift nurses, as high as 79.9% of them had worked for more than 10 years. The prevalence of sleep deprivation was high in both groups, that is, 89.7% among shift-working nurses and 87.2% among nonshift nurses. One-third of shift-working nurses (33.8%) experienced traumatic events at work before, compared to only one-fifth of nonshift nurses (20.8%). In terms of the nature of shift work, slightly more than half (50.05%) undertook more than 24 shifts per month. Furthermore, more than one-third (36.6%) performed more than six night shifts per month, and another 27.0% of them had to perform more than five double shifts in a month.
Sociodemographic Characteristics of Shift Nurses (n = 1,056) and Non-Shift Nurses (n = 435).

† Household incomes were categorized according to the Malaysian Department of Statistics (DOSM) Household Income and Basic Amenities Survey 2019, that is, B40: bottom 40% (less than MYR 4,360), M40: middle 40% (MYR 4,361-MYR 9,619), and T20: top 20% of income earners (more than MYR 9,620).
Professional Characteristics of Shift Nurses (n = 1,056) and Nonshift Nurses (n = 435).

Prevalence of Burnout Among Shift-Working Nurses
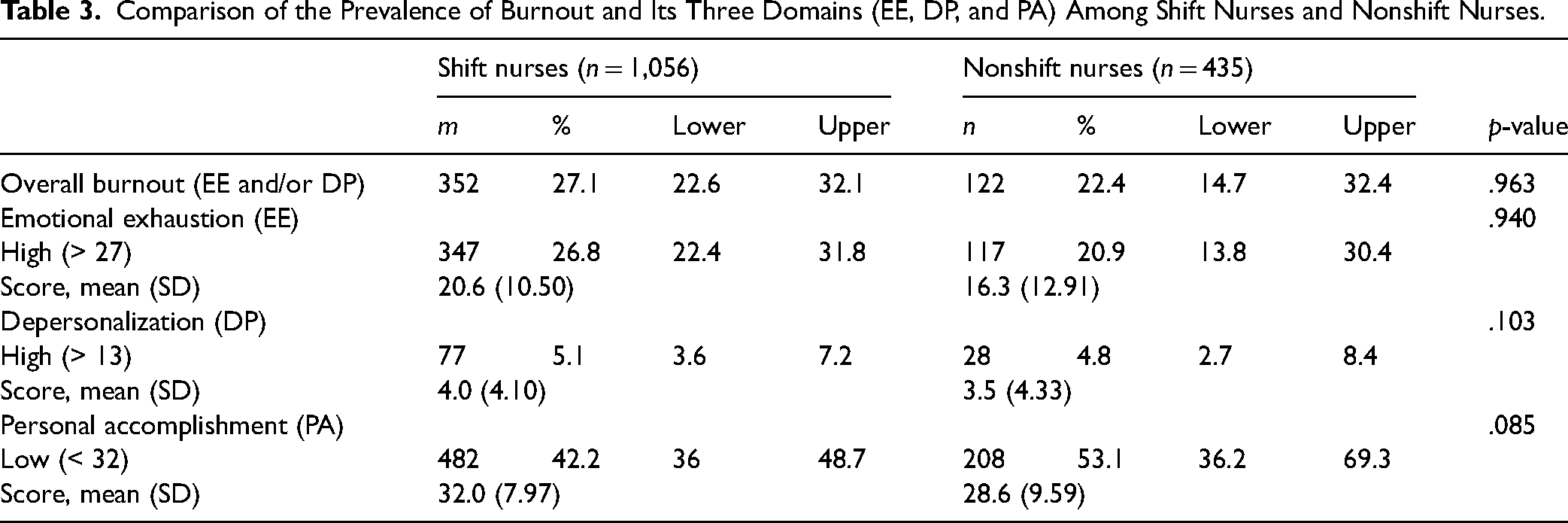
Based on Table 3, the prevalence of overall burnout was higher among shift nurses (27.1%) as compared to their counterparts (22.4%). With regard to the three domains of burnout, a higher proportion of both groups of nurses experienced low PA, followed by high EE and high DP. Shift nurses reported a higher prevalence of high EE and high DP. Even though the prevalence of low PA was higher among nonshift nurses (53.1%) than shift nurses (42.2%), the difference was not statistically significant.
Comparison of the Prevalence of Burnout and Its Three Domains (EE, DP, and PA) Among Shift Nurses and Nonshift Nurses.
Predictors of Burnout Among Shift-Working Nurses
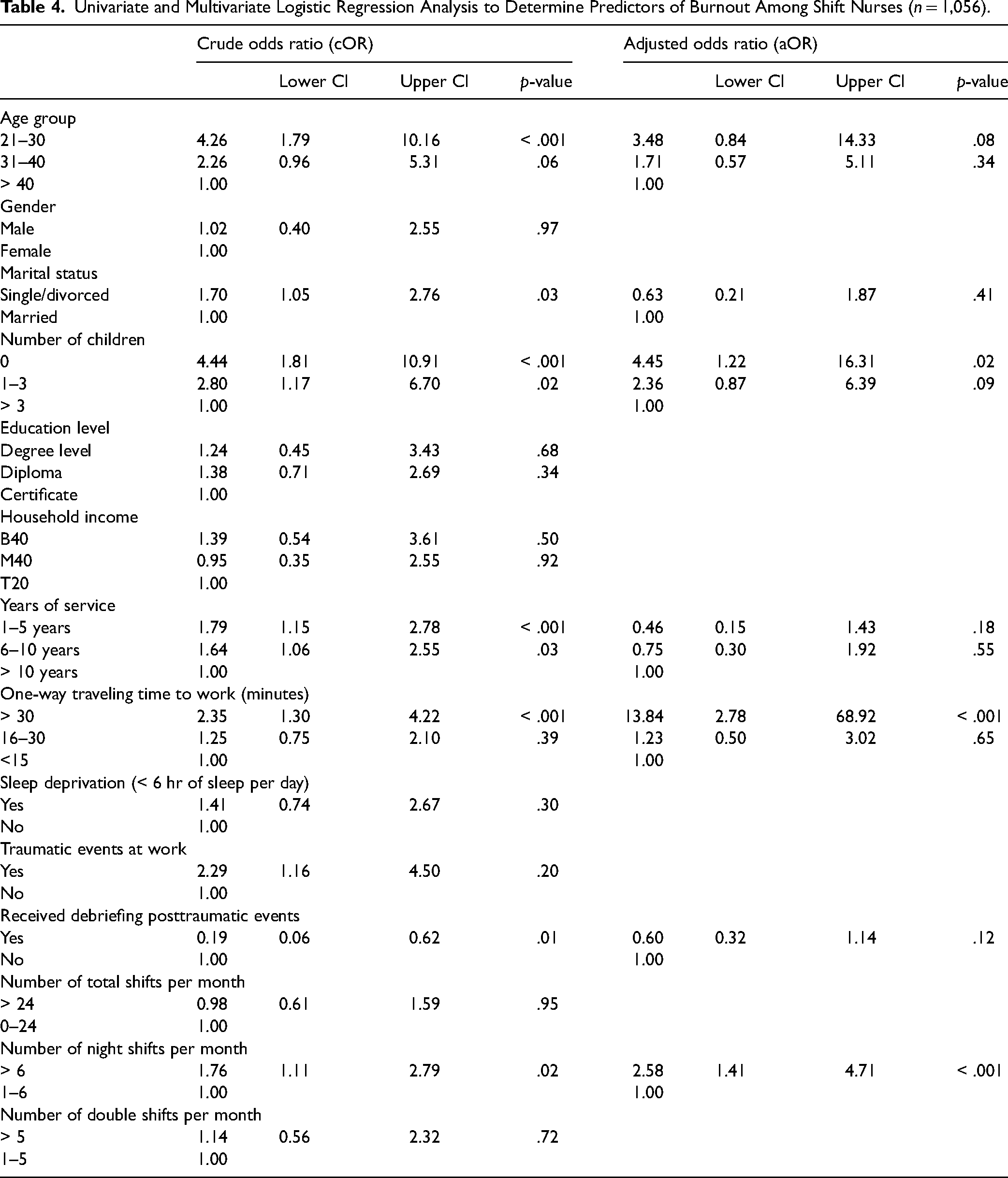
In Table 4, univariate logistic regression showed that age group, marital status, number of children, years of service, traveling time to work, and receiving debriefing posttraumatic events at work were significantly associated with the development of burnout among shift-working nurses (p < .05). Based on the adjusted odds ratio from multivariate logistic regression, those who were childless were 4.5 times more likely to experience burnout (p < .05). In addition, traveling time to work was a significant predictor of burnout whereby those who took more than 30 min per way to work reported a 13.8 times higher prevalence of burnout (p < .001). In terms of shift schedule, the number of total shifts and double shifts per month did not affect the development of burnout. However, nurses who performed more than six night shifts per month were found to be 2.6 times more predisposed to burnout (p < .001).
Univariate and Multivariate Logistic Regression Analysis to Determine Predictors of Burnout Among Shift Nurses (n = 1,056).
Discussion
Shift work is an integral part of the nursing profession in the hospital setting to ensure round-the-clock quality care for patients. Previous studies have shown that shift work can be potentially detrimental to nurses’ physical and mental well-being (Dahlgren et al., 2016; Dall'Ora et al., 2016). Burnout is one of the most pressing concerns in the nursing workforce because of its adverse impact on patient care and job satisfaction (Han et al., 2014; Niu et al., 2013; Van Bogaert et al., 2013). While many studies have been conducted to determine the association between shift work and burnout (Vidotti et al., 2018; Wisetborisut et al., 2014; Yestiana et al., 2019), the evidence remains scarce in certain countries, such as Malaysia. Shift work-related risk factors of burnout may vary in different healthcare settings and populations. Therefore, this study compared the prevalence of burnout among nurses who performed shift duties and their counterparts, as well as identifying the significant predictors of burnout among shift nurses.
In this study, the prevalence of burnout and its two main domains of EE and DP were significantly higher among nurses who performed shift duty. This is consistent with another study in which nurses working shifts of 12 hr or more were more likely than nurses working shorter hours (≤8) to experience burnout in all three domains (Dall'Ora et al., 2015). Similarly, burnout was 1.5 times more frequent among shift workers than nonshift workers in a university hospital in Thailand (Wisetborisut et al., 2014). In Singapore, a study by Tan et al. reported a higher level of burnout among healthcare staff who undertook shifts longer than 8 hr during the COVID-19 pandemic (Tan et al., 2020). In terms of the types of shift work, the number of night shifts was a significant predictor of burnout among shift nurses in our study. Those who performed more than six night shifts per month were 2.6 times more likely to develop burnout. Moreover, shift nurses reported a higher level of sleep deprivation as compared to their counterparts.
The close relationship between shift work, sleep deprivation, and burnout has been the subject of many researchers. To begin with, shift work rotation can lead to a disruption in the circadian rhythm and sleeping patterns. Physiologically, shift workers, especially those undertaking night shifts, commonly exhibit an increased level of stress hormones such as adrenaline and cortisol. Similarly, the level of serum cortisol is also higher among sleep-deprived individuals (Brum et al., 2022). In a 2020 report (Chellappa et al., 2020), circadian misalignment was established as an important biological component that determines mood vulnerability, thus shift workers are commonly predisposed to sleep deprivation and subsequent undesirable mood effects, all of which serve as important precursors to burnout. This finding is parallel to studies involving HCW from other countries, including France (Poncet et al., 2007) and Nigeria (Lasebikan & Oyetunde, 2012). Nevertheless, due to the cross-sectional nature of our study, it remains debatable if sleep deprivation caused by shift schedules predisposes to burnout is a unidirectional linear relationship. From our results, we cannot ascertain if the relationship can be bidirectional whereby EE from burnout at work can in turn be the culprit of sleep problems, especially since nonshift nurses in our study also experienced a relatively high level of sleep deprivation. Traditionally, long shifts have been implemented as a strategy to counteract staff shortages in the face of heavy healthcare demands. However, as more evidence points toward the harmful impact of extreme working hours, innovative solutions in the rotational work schedule as discussed in the subsequent section on implications for practice are necessary for staff welfare while ensuring the minimum disruption to clinical care.
On the other hand, our results showed that younger nurses with fewer years of working experience were more likely to be performing shift duties in their hospitals. This group of shift-working nurses was also more predisposed to burnout, as shown by the result of the univariate logistic regression. This early stage of their nursing careers often coincides with the initial establishment of marriage and family, not to mention the need to care for their aging parents. In Malaysia, likewise in other parts of the world, nurses are predominantly female. Thus, it is challenging for them to juggle irregular working hours with various domestic duties expected of them as a wife, mother, and daughter. In countries with patriarchal-imposed roles and family demands on women, female shift workers have been shown to have a lower tolerance to shift work due to greater difficulties in coordinating irregular working schedules with domestic duties (Blanch & Aluja, 2012; Maglalang et al., 2021). Studies show that HCWs are conflicted in balancing care between patients and their families which can at times lead to a deficit in both situations (Maher, 2014). It is not surprising that shift work schedules can be a stressor in their private lives. For instance, they may suffer from reduced family and leisure time, as well as failure to meet the expectations of their spouses or family members, thus resulting in family–work conflict and subsequently burnout (Jia & Li, 2022). Therefore, this group of nurses deserves to be given greater attention and organizational support, such as access to training on positive coping strategies, stress reduction, time management, and work–life balance measures.
Despite so, our findings showed that regardless of age or marital status, nurses without children were more likely to experience burnout. A similar observation was reported in a meta-analysis in which being childless was linked to higher levels of EE and DP (Cañadas-De la Fuente et al., 2018). In other words, having children protects nurses from increased levels of these burnout dimensions to a certain extent. One of the postulated reasons is that childless nurses may face accentuated emotional overload and sensations of overwork from their clinical work when they do not have alternative distractions to divert their attention at home. However, this part of the study finding requires further validation to determine the reasons for childlessness, especially among nurses who are married. Difficulty with conceiving or infertility has been observed among shift workers as a result of circadian misalignment (Gamble et al., 2013) and oxidative stress (Faraut et al., 2013) that impair ovulation. Furthermore, poor tolerance of night shift work and/or lack of autonomy about shift options may further affect their reproductive capacity (Fernandez et al., 2020). Therefore, future research that centralizes childlessness and shift work is warranted to delineate a clearer relationship between shift nurses and burnout.
The relationship between repetitive professional exposure to traumatic events, such as dealing with severe injuries and mortalities, aggression, and suffering from burnout has been reported in a systematic review (Adriaenssens et al., 2015). However, little is known in the literature if shift work adds complexity to this relationship. In this study, exposure to traumatic events was found to be associated with burnout among shift nurses, even though it was not statistically significant in the multivariate analysis. A more comprehensive list of specific traumatic events in the healthcare environment can be considered in future evaluation to better delineate the difference between shift and nonshift nurses. In addition, traveling time to work also emerged as a significant predictor of burnout whereby nurses who took more than 30 min per way to work were more likely to experience burnout. Besides rendering the shift nurses more exhausted on top of their long working hours that may or may not involve night or double shifts, the long traveling time can further deplete their available time for personal, social, and leisure activities. A longer commute time leads to a decreased time spent with their spouses and children as well as friends. Often, the time spent traveling to and from the workplace is an important determinant of individuals’ satisfaction level with their work–life balance (Chatterjee et al., 2020). On top of that, nurses also face the pressure of arriving on time for a smooth transition of shift handover, or in certain instances, to fetch their children after school hours. Thus, any delays due to traffic jams or public transportation disruption further predispose them to stress and burnout. There is no quick fix to this issue as the solution lies within concerted systemic efforts from institutional and community levels. Apart from addressing shift-related causes, social support can be provided in terms of accommodation nearer to the workplace (quarters) or 24-hr childcare service in the healthcare centers, especially for families with two working parents with no other family support.
Strengths and Limitations
This national-level study with a large sample size provided a good representation of nurses working in Malaysian public hospitals. We highlighted the types of shift work that predisposed to the development of burnout among hospital nurses. In the postpandemic era, this becomes an even more pressing issue in view of the increasing workload, hygienic precautions, and patient demand. Our findings can be used as the baseline data for the comparison of any health or intervention indicators in this area between the pre- and post-COVID pandemic. In addition, early recognition of the predisposing factors of burnout among the high-risk population is the first critical step to garner sufficient buy-ins from internal and external stakeholders to emphasize positive motivational factors such as recognition, promotions, and wage improvement that have been proven to be protective against burnout (Kader et al., 2021b). Therefore, the risk factor profile of burnout-susceptible nurses presented in this study can be incorporated by policymakers and hospital managers in the design and implementation of such preventive initiatives.
There are several limitations to this study. Firstly, a relationship cannot be proven among the variables due to the cross-sectional nature. Future research should consider the use of longitudinal studies to confirm the temporality impact of shift work. Next, self-administered questionnaires used in the data collection could have produced social desirability bias due to self-reporting. To avoid survey fatigue, the two variables of exposure to traumatic events and sleep deprivation were assessed with only a single ad hoc item in the questionnaire. To enhance the validity of the association between these two variables with burnout among shift workers, like-minded researchers may consider a more extensive list of questionnaire items from validated tools in the future. Furthermore, the sample population included only shift-working nurses who worked in public hospitals in Malaysia. Thus, caution is required when generalizing the findings to other types of healthcare facilities or professional groups. Lastly, future studies can benefit from the inclusion of more variables related to shift work and burnout to improve the understanding of the possible relationship between different factors.
Implications for Practice
There have been increasing calls worldwide to promote healthier and safer workplace environments, especially in healthcare organizations. The significant association between the development of burnout and shift work highlighted the need for the relevant stakeholders in the hospital management and nursing division to identify and execute innovative solutions in the rotational work schedule. Self-scheduling by nurses allows individual preferences to be taken into consideration in the arrangement of shift and day-off assignments. Additionally, the application of scheduling optimization tools using AI algorithms that simultaneously consider workload fairness and individual needs is also being tested to create an efficient nurse shift-rotation schedule (Rerkjirattikal et al., 2020).
On a similar note, as sleep deprivation commonly inflicts nurses, it is important to incorporate sleep education and training with comprehensive sleep hygiene content in undergraduate nursing curricula to better prepare junior nurses who are more likely to be assigned shift schedules. Furthermore, as sleep deprivation is likely related to night shift duty and shift work in an integral component of nursing care that is almost impossible to abolish, the next best alternative would be to equip these at-risk populations with the necessary knowledge and skills to adopt regular daily naps, adjusting their personal and family rhythms to the work schedules, and if situations permit, to arrange for shift nurses to take micro-naps lasting more than 1 hr in sequence without compromising patient care, especially during the night shift. These are some of the proposed solutions in a meta-analysis published in 2022 (Membrive-Jiménez et al., 2022). These efforts are vital to prevent burnout and staff turnover, both of which can be counterproductive for healthcare organizations, especially when reviews on the negative impact of burnout on patient safety outcomes such as medical errors have been published (Hall et al., 2016; Özkan, 2022).
In view of the abovementioned study findings, modified work schedules and shift characteristics must be evaluated as potential interventions in future studies. Nurses’ preferences in their working shift schedules should be prioritized as it is linked to their well-being (Nijp et al., 2012). In an interventional study, nurses who were given more control over their shift rotations reported a lower rate of absenteeism compared to traditional scheduling systems (Turunen et al., 2020). Despite so, many proposed solutions to reduce the impact of shift work on health conditions in the literature have not been implemented in practice, often due to a lack of robust evidence in the local setting to garner higher-level commitment. Apart from interventions targeting shift patterns, proper human resource projection and distribution is imperative to cope with increasing demands on healthcare services. Appropriate staffing, work rotations, and shift schedules will go a long way in preventing a worsening of the burnout epidemic among nurses as well as minimizing negative consequences for staff and patient safety.
Conclusions
In summary, nurses who perform frequent night shift duty are highly predisposed to burnout. Our findings also evidenced the urgent need to develop interventions designed to improve the shift patterns of the nurses. Addressing burnout on an individual level is necessary but may not be sufficient. Any initiatives to improve the system of shift employment and provide amenable work environments should incorporate concerted efforts from all relevant stakeholders at the systemic and institutional levels. Collectively, these efforts could create improved working conditions and assure quality nursing services for patients.
Footnotes
Acknowledgments
We wish to thank the Director General of Health, Malaysia for his permission to publish this article. Our gratitude to all the nurses who were involved in the study and the data collection team members.
Author Contributions
N.Z. and N.H.Z. conceived the study. All authors had made substantial contributions design of the work, the acquisition, analysis, and interpretation of data and K.Y.L led the writing of this manuscript. All authors read and approved the final version of the manuscript.
Data Accessibility
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the MOH Research Grants (MRG) under the National Institutes of Health Malaysia (NMRR-18-3590-45274).
Ethical Statement
This study involved human participants and was approved by the Medical Research and Ethics Committee of the MOH Malaysia, NMRR-18-3590-45274 (IIR). Permission was also obtained from the hospital directors of the involved study sites before data collection.